Rheumatism of the heart, a systemic disease that affects the walls of the organ or its individual layers. The pathology is characterized by the rapid progression and spread of the inflammatory process to other organs and systems, the development of complications and the deterioration of the patient’s well-being. Most often occurs in children aged 3 to 15 years.
What is rheumatism of the heart
It is necessary to consider what rheumatism of the heart is. This is a disease that develops as complications after a streptococcal infection. Heart damage is characterized by the involvement of different layers of the organ in the pathological process: the endocardium and myocardium. Damage to the valves and other anatomical parts of the heart is possible, which leads to a sharp deterioration in the patient’s well-being.
Chronic rheumatic heart disease (ICD 10 code, I05-I09), a leading cause of death in some countries, including the United States of America. CRHD develops after rheumatic fever and is characterized by predominant damage to the left ventricle of the heart.
The description of the disease includes damage not only to the endocardium or myocardium, but also to the valves of the organ.
Determining the pathology can be complicated by the lack of a direct connection between an acute rheumatic attack and the occurrence of clinical manifestations.
Symptoms of rheumatic heart disease
Symptoms of pathology can be very different.
Typically patients complain of:
- General malaise, weakness and increased fatigue.
- Shortness of breath not only during exertion, but also at complete rest.
- Cardiopalmus.
- Chest pain during exercise.
- Attacks of lack of air mainly at night, during sleep.
- Sensation of pulsation inside the chest.
- Pulsation of neck vessels.
- Dizziness.
Against the background of heart disease, the following may occur:
- symmetrical swelling of the legs and ankles;
- fainting.
When examining the patient, cyanosis of the nasolabial triangle and blush on the cheeks can be detected. With mitral stenosis in children, developmental delays occur. Patients often complain of weight loss, as well as coughing with sputum (with lesions of the mitral valve). Each symptom is not specific. Therefore, it is very important to constantly monitor the patient’s condition and conduct a comprehensive examination.
Pathological complications deserve special attention.
After a fever, mitral valve insufficiency often develops. It occurs in patients in 60-70% of cases. Isolated aortic valve insufficiency also occurs. Isolated stenosis is the least common. All these pathologies are dangerous to the life and health of the patient.
Causes of the disease
Rheumatism of the heart has various causes of development. These include the presence of the following factors:
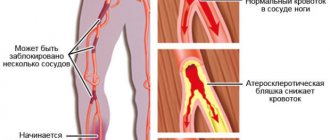
- Streptococcal infection. The etiology of the disease involves the penetration into the human body of beta-hemolytic streptococcus group A, the toxins of which have an adverse effect on the patient’s condition. In this case, damage to the valvular apparatus of the heart develops. Streptococcus becomes an antigen that accompanies rheumatism. This is possible after a sore throat or scarlet fever, especially against the background of a weakened immune system.
- Weakening of the immune system. The development of cardiac rheumatism occurs in people prone to private colds viral infections and somatic diseases.
- Genetic predisposition. Despite the fact that rheumatism of the heart in children is not inherited, there are certain risk factors that sharply increase the likelihood of developing the disease. This is possible due to the presence of a congenital predisposition to hypersensitivity reactions.
- Allergic or immune reaction. Damage to the heart and joints in children develops in response to the penetration of streptococcal infection. After all, with the blood flow, these substances quickly spread throughout the human body, most affecting the joints and heart.
You need to know why cardiac rheumatism develops. The pathogenesis and its stages continue to remain unknown. An acquired defect in the valve apparatus leads to a significant deterioration in a person’s condition. Not only physical, but also psychosomatic disorders develop.
Causes
Doctors also cannot say about them with certainty. There are several assumptions regarding the genesis of the pathological process.
An approximate list of moments that provoke a violation:
- A previous infectious disease accompanied by weakened local and general immunity.
In children, a common variant is cardiac rheumatism after tonsillitis or scarlet fever, provoked by pyogenic flora (for example, staphylococcus).
In patients of other groups, other agents, including viruses and fungi, can play a similar negative role.
- Long-term uncontrolled use of certain medications. For example, antibiotics or oral contraceptives, also cytostatics, drugs aimed at reducing the rate of division of “fast” cells (actively used in the treatment of cancer).
Among the provoking factors, several more points can be mentioned:
- Genetic predisposition. Plays a key role in determining the likelihood of getting sick. If there was at least one person in the ascending line who suffered from rheumatism (not necessarily heart disease), the chances of becoming the “owner” of an identical diagnosis are determined at 50% or even higher. In such a situation, the trigger may be hypothermia or nervous tension. Factors that seem harmless at first glance.
- The presence of chronic diseases of the oropharynx. Proven reason that increases risks.
- Peak states. Pregnancy, puberty, menopause and others, including the menstrual cycle.
The presence of hormonal dysfunctional disorders affects. Diabetes, thyroid problems and others.
Correcting these points still does not provide a 100% guarantee that the disease will not manifest itself.
What has been said is the doctors' assumptions. Until the mechanism of development is known, it will not be possible to speak precisely about risk factors and causes.
Symptoms of rheumatism
The inflammatory process in the body begins with small joints, which can be most often affected by rheumatism. The main manifestations are pain, swelling and impaired range of motion in the joint, which are of a volatile nature. Over time, the inflammatory process spreads to the bone area. The first symptoms of rheumatism of the heart appear 3-4 weeks or several months after a streptococcal infection.
In rheumatism, the heart valve (mitral) is affected, which is manifested by shortness of breath and pain in the heart.
This indicates organ failure as a result of incomplete closure of the valves or stenosis of the atrioventricular orifice. There is the appearance of noise and a change in heart rate. Arrhythmia occurs, a feeling of irregular heartbeat.
Lack of timely treatment leads to heart inflammation developing. It is accompanied by hemodynamic disturbances in the systemic and pulmonary circulation. The clinic of rheumatism in children, especially the primary attack of pathology, is accompanied by an increase in body temperature, signs of intoxication, headache, weakness, drowsiness, sweating, and loss of appetite.
Signs in adults include loss of function due to the inability to perform even simple movements.
The intensity of the clinical manifestations of the disease depends on the course of the pathology, the form of the rheumatic process and the individual characteristics of the patient’s body.
which heart valves are most often affected by rheumatism
Rheumatism of the heart is a serious chronic disease in which the inflammatory process, which began as a result of an infectious lesion of the joints, covers the membranes of the heart and entails disorganization of the connective tissue of the heart.
There are several reasons for the development of this disease:
- frequent and untreated infectious diseases of the nasopharynx (tonsillitis, chronic tonsillitis, chronic pharyngitis, etc.);
- infection with group A β-hemolytic streptococcus;
- previous scarlet fever;
- hereditary factor.
Some people have a predisposition of the body in the form of a hyperreaction to streptococcal infection, which not only causes rheumatism, but also causes its exacerbations.
There is a concept of “familial” rheumatism of the heart, which is caused by a long stay in a streptococcal environment and unfavorable living conditions, as well as an inherited polygenic predisposition to the disease.
Signs of rheumatism of the heart usually appear 1 to 2 weeks after a streptococcal infection. However, in some cases, the disease can proceed for a long time, almost unnoticeably for the patient, progressing at a slow pace.
The most common manifestations of the disease include:
- general weakness, fatigue;
- severe joint pain;
- increased sweating;
- pale skin;
- heart rhythm disturbances;
- nosebleeds;
- weight loss;
- lack of appetite;
- dyspnea;
- increase in body temperature.
A symptom of rheumatism such as pain in the heart deserves special attention. These pains, as a rule, are of a pulling, stabbing nature and are often combined with a rapid heartbeat.
If this disease is not treated promptly, it can lead to heart disease or joint deformation. A heart defect is a defect in the structure of the heart, leading to a failure of its normal functioning. Rheumatic heart defects often develop with repeated rheumatic attacks.
Most often, with rheumatism of the heart, the mitral valve is affected - the lumen narrows, or the valve begins to allow blood to flow in the wrong direction. Defects of the aortic and other heart valves are somewhat less common.
It is worth considering that heart defects may not produce symptoms for a long time and are detected only with careful diagnosis.
Rheumatism of the heart requires complex treatment in a hospital setting, the main principles of which are:
- Bed rest
is recommended for the entire treatment period. Subsequent restoration of physical activity should occur at a slow pace. - Diet:
avoiding salt, limiting fluids and carbohydrates, adequate intake of protein, potassium-containing foods (dried apricots, buckwheat porridge, potatoes, etc.). - Drug therapy:
prescription of antibiotics, anti-inflammatory and vitamin preparations. In some cases, cardiac therapy is performed. - Sanatorium-resort treatment
is recommended during the recovery period after treatment and in the future as supportive measures.
Treatment of rheumatism of the heart with folk remedies
Traditional medicine suggests using medicinal plants to treat this disease. Here are a few recipes:
- Pour a tablespoon of a mixture of 10 g of buckthorn bark, 40 g of birch leaves and 50 g of willow bark into a glass of boiling water. Leave for an hour, strain and take a glass of infusion twice a day.
- Prepare a tincture of yellow acacia twigs with leaves, pour 30 g of raw material with 200 g of vodka. Infuse in a dark place for 10 days, then strain and take 20 drops three times a day with water.
- Take the juice of half a lemon, diluted half with hot water, on an empty stomach.
Source: womanadvice.ru
Which heart valves are most often affected by rheumatism?
LECTURE No. 7. Rheumatism (Sokolsky-Buyo disease)
Rheumatism is a systemic toxic-immunological inflammatory disease of connective tissue with a predominant localization of the process in the cardiovascular system. The disease develops at any age, mainly among adolescents and children (7-15 years). Women get sick more often than men.
Etiology
. The disease is caused by group A β-hemolytic streptococcus.
Pathogenesis
. Released streptococcal antigens (streptolysin-O, streptokinase, streptohyaluronidase) lead to the development of the acute phase of inflammation with cellular exudation and phagocytosis.
In the connective tissue, reparative processes develop: cell proliferation, stimulation of the formation of mucopolysaccharides. The work of the immune system is activated through increased functioning of the complement system and lysosomal enzymes.
Chronic inflammation gradually develops with the transfer of activity to immune mechanisms, collagen formation with the formation of fibrosis processes.
Pathological anatomy
. There are 4 phases of development of morphological changes, each lasting 1–2 months.
Phase I – mucoid swelling of the interstitial tissue and collagen fibers.
Phase II – fibrinoid changes with disorganization of collagen fibers, the formation of structureless fields impregnated with fibrin.
Phase III – formation of Ashoftallalaevsky granulomas with the appearance of perivascular accumulations of lymphocytes and other cells.
Phase IV – sclerosis (fibrosis) with the transformation of cells in granulomas into fibroblasts and the gradual formation of a scar.
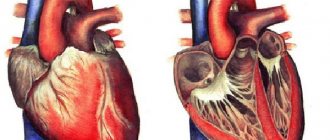
The heart is the main target organ for rheumatism. Deformation of the heart valves leads to the formation of their insufficiency, then to narrowing and deformation of the atrioventricular orifices.
The development of heart defects often occurs in the form of combined and combined forms.
Classification
. The clinical classification according to Nesterov A.I. (1990) takes into account:
1) phase of the disease (active or inactive, specifying the degree of activity of the process - minimal, medium, high);
2) clinical and anatomical characteristics of damage to the heart and other organs;
3) the nature of the course of the disease (acute, subacute, protracted, continuously relapsing, latent);
4) state of blood circulation (0, I, IIa, IIb, III degree of impairment).
Clinic
. The first period is called pre-rheumatism. It lasts 2–4 weeks from the end of the streptococcal infection until the onset of manifestations of the disease. Rheumatism never begins at the height of infection.
Appear: malaise, fatigue, loss of appetite, palpitations, tingling in the joints, hyperhidrosis, pale skin. The second period represents a rheumatic attack.
Fever may appear with syndromes of damage to the joints, heart (primary rheumatic carditis) and other organs. The third period represents a long period of clinical manifestations.
Recurrent rheumatic carditis with progressive heart damage and the formation of complex heart defects are noted.
Inflammation of all membranes of the heart (pancarditis) is possible; the endocardium and myocardium are most often affected. Tachycardia appears, less often bradycardia. The borders of the heart are normal or moderately enlarged.
On auscultation, a muffled first sound is heard, a soft systolic murmur at the apex (associated with myocarditis). Sometimes a third tone may appear.
As the noise intensity increases, mitral valve insufficiency may develop (not earlier than 6 months from the onset of the attack).
New defects of the valvular endocardium are formed in the form of combined and combined heart defects.
Diagnostic criteria for rheumatism
according to Kissel-Jones (as modified by the American Rheumatological Association, 1982). Major and minor criteria for the course of the disease are identified.
Major criteria include: carditis, polyarthritis, chorea, annular erythema, subcutaneous rheumatic nodules. Minor criteria include: previous rheumatism, arthralgia, fever, increased ESR, increased C-reactive protein, leukocytosis, prolongation of the PQ interval on the ECG, increased titer of anti-streptococcal antibodies in the blood, detection of streptococcal antigen.
If two major and one or two minor criteria are present, the diagnosis is considered reliable; if one major and two minor criteria are present, the diagnosis is considered probable.
Additional diagnostic testing
.
Of the laboratory indicators, a general blood test (hypochromic anemia, leukocytosis with a shift to the left, an increase in ESR), a biochemical blood test (the appearance of C-reactive protein, increased fibrinogen, dysproteinemia, β2-hyperglobulinemia, increased content of haptoglobin, ceruloplasmin, acid phosphatase).
An immunological study should be carried out to determine the increase in the titer of antibodies ASG, ASL-O, ASA, and myocardial antibodies.
Instrumental research methods include ECG (detection of various rhythm and conduction disturbances) and Doppler echocardiography.
X-ray examination can be informative in severe cases, when there is an enlargement of the left chambers of the heart. During the first attack, no heart changes are detected.
Differential diagnosis
. Should be performed with infectious myocarditis. The disease develops at the height of infection; it is not characterized by progression or signs of valvulitis.
Among connective tissue diseases, it is necessary to take into account periarteritis nodosa, systemic lupus erythematosus, and scleroderma.
With neurocircular dystonia of the cardiac type, there are various complaints, but there are no objective signs of the disease.
In primary tuberculosis syndrome, there are no radiological symptoms of the primary complex or antistreptococcal antibodies. Mantoux and Pirquet tests are performed, and tuberculosis mycobacteria in sputum are examined.
Treatment
. With active rheumatism, mandatory hospitalization is required for up to 40–60 days or more.
An appropriate regimen is prescribed: in the absence of carditis - semi-bed rest for 7-10 days, then free; in the presence of carditis - strict bed rest for 2-3 weeks, then semi-bed rest and loose.
From the diet, table No. 10 is prescribed with a protein content of at least 1 g/kg, limiting table salt to 6 g/day.
Mandatory early prescription of antibiotics is carried out: benzylpenicillin 1.5–4 million units per day (depending on the degree of activity) for 2 weeks. Then they switch to a prolonged form: bicillin-5 1.5 million units every 2 weeks for 2 months.
After this, antibiotic therapy is carried out every 3 weeks every month for at least 3 years in patients without a history of carditis and for at least 5 years in patients with a history of carditis.
If you are allergic to penicillin, antibacterial drugs of other groups are used - macrolides, oral cephalosporins.
Glucocorticoid drugs are prescribed only for severe carditis, acute (less often - subacute) course of the disease: prednisolone 20-30 mg/day for 2-3 weeks, then the dose is reduced until the drug is completely discontinued, the course of treatment is 1.5-2 months.
Source: https://folkmap.ru/krov/kakie-klapany-serdtsa-naibolee-chasto-porazhayutsya-pri-revmatizme/
Risk factors
Rheumatic heart disease most often develops when a person has risk factors.
These include the following:
- The medical history includes facts about relatives having rheumatoid arthritis, lupus erythematosus and other systemic disorders.
- Gender. Women suffer from rheumatic carditis more often than men.
- When streptococcus affects the heart, rheumatism is more likely to occur in children under 15 years of age than in adults. Older people are also prone to the disease.
- Prone to frequent viral infectious diseases.
- Weakening of the immune system is dangerous. The body will not be able to independently counteract the pathogen from the hemolytic streptococcus group, as a result of which the risk of disease increases. This happens after physical or mental stress, fasting, surgery, severe somatic and infectious pathologies.
- In combination with a congenital heart defect. The valve apparatus is characterized by weakness, which occurs with defects.
Classification
Classification of the disease involves several types of division. They are based on the prevalence of the pathology, the degree of damage to the heart structures and other signs.
According to the degrees of the active phase and severity of manifestations, acute and chronic rheumatic heart disease are distinguished.
Depending on the phase they differ:
- Active phase rs. There are minimal, moderate and high activity.
- Inactive phase rs. There are no clinical manifestations of the disease, which characterizes chronic rheumatism during remission.
Based on what caused the development of the pathology, there are rheumatic and non-rheumatic myocarditis. Not only beta-hemolytic streptococcus, but also other pathogens, viruses, bacteria, fungi, etc. can provoke damage to the heart valves during rheumatism.
In accordance with the clinical and anatomical features of heart damage, the following are distinguished:
- The inflammatory process is localized within the heart and does not spread to other parts.
- Damage to other organs (kidneys, joints, lungs, skin and subcutaneous fat). The disease Chorea is a complication of rheumatism in the same way as other syndromes, including erythema annulare and subcutaneous nodules.
Acute rheumatic fever and chronic rheumatic heart disease are distinguished by damage to different layers of the myocardium. Types of disease:
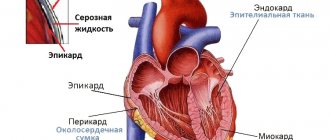
- Endocarditis. Inflammation of the inner lining of an organ. This leads to damage to the heart valves during rheumatism, since as a result of the pathological process the tissues tend to become denser and deformed.
- Myocarditis. Damage to the muscle membrane, which provokes the development of heart failure.
- Pericarditis. The appearance of changes in the outer shell.
- Pancarditis. Involvement of all membranes in the pathological process that causes acute rheumatic heart disease. This threatens to disrupt the functioning of the organ and stop it.
Rheumatic heart disease: types and codes according to ICD-10, treatment and prevention of rheumatism
Rheumatic heart disease is a group of acquired chronic degenerative diseases of the heart valves, characterized by progressive post-inflammatory fibrosis and destruction of the valve leaflets.
The disease develops within 1-3 years from the moment of acute rheumatic fever. The incidence rate is 2 cases per 100,000 population.
What it is?
First of all, rheumatic heart defects are accompanied by hemodynamically significant disorders of the heart valves - aortic, mitral or tricuspid. A secondary symptom is changes in the chambers of the heart. Autoimmune antibodies are the cause of disruption of the connective tissue of the cusps in the valves.
After such disorganization, the valve leaflets are no longer able to close the valve opening. The increased blood flow into systole increases the left atrium, which leads to stagnation of blood, first in the small and then in the systemic circulation.
Among adults, such defects are common in women 40–60 years old, with a slightly lower incidence rate in men of the same age. More often, rheumatism occurs in children from 6 to 16 years old.
Here, hereditary and constitutional predisposition to the disease is of great importance. Rheumatism in children is of an infectious-allergic nature; it is impossible without a previous streptococcal infection (pharyngitis, scarlet fever, tonsillitis).
Find out more useful information about rheumatic heart disease from Elena Malysheva’s video:
What diseases are caused by rheumatism causing heart defects?
Rheumatism is a complication of acute infectious diseases of the throat, skin, kidneys and other organs caused by group A beta-hemolytic streptococcus.
| Causal disease | Frequency, % |
| Tonsillitis (tonsillitis) | 33 |
| Acute glomerulonephritis | 23 |
| Erysipelas of the skin | 7 |
| Streptoderma | 7 |
| Pharyngitis | 5.2 |
| Scarlet fever | 3.3 |
| Meningitis | 2.1 |
| Endocarditis | 1.3 |
| Pneumonia | 1.2 |
Rheumatism leads to the development of heart defects:
- Rheumatic myocarditis is an inflammation of the muscular lining of the heart, most often not causing serious complications.
- Rheumatic endocarditis - the inner lining is inflamed. Often causes mitral valve insufficiency.
- Rheumatic pericarditis - the outer membrane becomes inflamed. Characteristic for severe rheumatic carditis.
- Pancarditis is the most complex case in which all layers of the heart are inflamed and it is unable to contract normally. It causes serious complications and circulatory disorders, and can also lead to cardiac arrest.
Classification, clinical picture and complications
| Nosology | Clinic | Complications |
| Mitral stenosis | Shortness of breath, hemoptysis, blue discoloration of the nasolabial triangle, pallor (later cyanosis) and cold skin | Pulmonary hypertension, pulmonary edema |
| Mitral regurgitation | Cough streaked with blood, arterial hypertension, diffuse cyanosis, enlarged liver and abdomen, dense edema | Atrial fibrillation, acute right ventricular failure |
| Aortic stenosis | Pale and dry skin, arterial hypertension, fainting | Cardiac asthma |
| Aortic insufficiency | Paleness, swelling and pulsation of neck veins, lability of blood pressure, palpitations | Left ventricular hypertrophy |
| Tricuspid stenosis | Blue skin, dense swelling of the legs, weight gain, “frog” belly | Acute right ventricular failure, ventricular fibrillation |
| Tricuspid insufficiency | Warm swelling of the legs, fluid accumulation in the abdominal cavity, swelling and tortuosity of the superficial veins | Arrhythmia, atrial and ventricular fibrillation |
ICD-10 codes
Mitral:
- I05.0 - stenosis;
- I05.1 - insufficiency;
- I05.2 - combined lesion.
Aortic:
- I06.0 - stenosis;
- I06.1 - insufficiency;
- I06.2 - combined lesion.
Tricuspid:
- I07.0 – stenosis;
- I07.1 - insufficiency;
- I07.2 - combined lesion.
Combined:
- I08.0 – aortic-mitral;
- I08.1 - mitral-tricuspid;
- I08.2 – aortic-tricuspid;
- I08.3 – aortic-mitral-tricuspid.
Other:
- I09.8 - damage to the pulmonary valve.
Frequency of occurrence
| Mitral | 48.3% (70-85% of patients are women) |
| Aortic | 32.3% (60-75% of patients are men) |
| Tricuspid | 14.7% |
| Combined defects | 4.1% |
| Combined | 2.8 % |
Why is the mitral valve most often affected?
The predominant lesion of the mitral valve is associated with the peculiarities of its anatomical structure. The valve consists of two leaflets supported by thin and tensile fibers (chords). At the moment of contraction of the ventricle, the blood exerts pronounced pressure on the chords, which leads to bending of the valves (prolapse).
Prolapse in most cases does not have clinical manifestations, but is a factor in the delay in this area of autoimmune complexes formed during rheumatism, which causes more frequent damage to the mitral valve.
At what age is it most often formed?
The average age of development of pathology is 35-45 years. In the natural course of the disease, the five-year survival rate is 50%.
Could it be congenital?
This disease is acquired (acquired during life). As a result of genetic mutations, the fetus can only develop congenital anomalies, in the formation of which rheumatism takes an indirect part (if detected in a pregnant woman).
The fetus cannot develop rheumatism due to the presence of the placental barrier and the absence of antibodies against streptococcus.
Diagnostic methods
How are rheumatic heart defects diagnosed? The rheumatic nature of the disease can be confirmed by:
- Interview and study of medical documentation (history of streptococcal infection);
- Determination of the level of antistreptolysin-O in the blood (ASL-O level is increased);
- Isolation of streptococcus from the throat (smear);
- Biopsy followed by histology (immune complexes are detected in a microslide of the heart).
First, the doctor examines and interviews the patient. Pay attention to unnatural paleness of the skin, reaching cyanosis in some places on the face, shortness of breath and swelling. Listening to the heart is carried out to identify arrhythmia and extraneous noise, the nature of which is determined by further research.
A survey is needed to identify possible causes of rheumatism and subsequent defects; the patient tells the doctor about past infectious diseases and diseases of close relatives.
If rheumatic defects are suspected, doctors take blood from the patient for general, biochemical and immunological analysis. These studies provide information about the presence of inflammation and infections in the body.
Among instrumental studies , the simplest is an electrocardiogram (ECG), which checks the heart rhythm and identifies the type of arrhythmia, blockade, and signs of ischemia. Using phonocardiography (PCG), the presence of heart murmurs and their relationship to defects is determined. The size of the heart is checked using a chest x-ray.
The main examination, thanks to which the hypothesis about the presence of a defect is often confirmed or refuted, is an echocardiogram (EchoCG, otherwise known as ultrasound of the heart).
It is used to diagnose a decrease in the contractility of the heart and disorders in its structure.
Most diagnostic methods can be carried out at the initial examination, when the diagnosis has not yet been confirmed, or in dispensary groups when a rheumatic defect has already been detected.
Treatment regimens used
Conservative (non-surgical) treatment is aimed at reducing the risk of complications of rheumatism, as well as correcting heart rhythm and preventing heart failure . It is recommended to take action immediately after rheumatism is detected. During the febrile period, the patient is treated inpatiently; strict bed rest is required.
Antibacterial and anti-inflammatory drugs are prescribed. After the last rheumatic attack, mandatory relapse prevention is carried out over the next five years.
All patients with acquired defects are referred to an appointment with a cardiac surgeon, who determines the current timing for surgical intervention.
Patients with stenosis undergo a commissurotomy, accompanied by separation of the valve leaflets - this ensures normal blood flow. In case of insufficiency, the operation is reduced to prosthetics of the affected valves. The combined defect is treated by replacing the damaged valve with an artificial one; sometimes, instead, prosthetics are performed along with commissurotomy.
Consequences
- Atrial fibrillation;
- Ventricular flutter and fibrillation;
- Acute left or right ventricular failure;
- Chronic heart failure;
- Pulmonary edema.
Primary and secondary prevention measures for streptococcal diseases
Timely preventive measures can prevent the development of rheumatism and heart damage.
Primary prevention:
- Hygiene and hardening;
- Sanitation of foci of infection (treatment of sore throat, erysipelas and other streptococcal infections) with penicillin and macrolide preparations;
- Annual medical examinations with a smear to determine streptococcus.
Secondary prevention is indicated for people with previous infection and is carried out using penicillin antibiotics (bicillin prophylaxis):
- Extensillin 2.4 million units intramuscularly;
- Benzathine-benzylpenicillin – 0.6-2.4 million units intramuscularly.
Minor changes in the valve apparatus without disturbances in the myocardium initially remain in the compensation phase and do not affect the patient’s ability to work.
The transition to the decompensation phase and prognosis are determined by many circumstances: infections, overexertion, repeated attacks, pregnancy and childbirth.
Increasing damage to the valves is the cause of the development of insufficiency, and the most acute decompensation often leads to death.
A conditionally positive prognosis in most cases is possible only with high-quality surgical treatment. In this case, changes in hemodynamics are often completely cured.
For rheumatic diseases, it is recommended to give up bad habits and try to reduce physical activity, follow a special diet, engage in physical therapy and undergo treatment courses at cardiological resorts.
The heart is one of the main human organs, and even minor disruptions in its functioning lead to serious consequences. Rheumatism and the accompanying heart defects can develop unexpectedly, after suffering infectious diseases, but those at greatest risk are people who are genetically susceptible to cardiac diseases .
To avoid complications, you need to promptly consult a doctor at the first suspicion. Modern methods of diagnosis and treatment make it possible to partially or completely get rid of acquired rheumatic disease.
2 Comments
Source: https://oserdce.com/serdce/poroki/priobretennye/revmaticheskie.html
Diagnostics
Diagnostic methods for identifying the disease involve a comprehensive approach. Propaedeutics includes not only a rheumatological examination, but also a thorough history taking.
It is necessary to find out whether the person suffered from scarlet fever, tonsillitis or other infectious diseases shortly before the first signs of pathology appeared, and also whether there is a prolonged fever of unknown origin,
Examination of the patient will help establish the diagnosis. The disease is indicated by: pallor of the skin, swelling of the extremities, a bluish tint to the lips, ears and tip of the nose, and the appearance of specific nodules on the skin.
Auscultation and additional laboratory tests will help determine rheumatism:
- General blood analysis. An increase in the erythrocyte sedimentation rate and an increase in the number of leukocytes with a shift of the formula to the left are detected.
- Tests that detect rheumatism. Research is being carried out on rheumatoid factor, glycoproteins, antistreptolysin and sialic acids.
- Determination of C-reactive protein.
- Analysis of the titer of antinuclear antibodies to double-stranded DNA and the level of circulating immune complexes. The presence of certain leukocyte alloantigens makes it possible to confirm pathology.
Diagnostic techniques play an important role in diagnosing the disease and acquired heart defects. They are instructions that a person must fulfill. Diagnose using the main methods:
- Ultrasound examination of the heart. Allows you to determine the size of the organ, the condition of the internal wall, changes in the structure of the heart valves (mitral, aortic). Cardiac ultrasound is the gold standard in diagnosis.
- Electrocardiogram (ECG). According to the examination, a violation of the heart rhythm is determined.
- Ultrasound of the kidneys, liver, spleen, chest x-ray. Necessary for differentiating the disease from other pathologies.
Diagnosis of rheumatism
In order to make a diagnosis of any pathology of the mitral valve, it is necessary to comprehensively evaluate the patient’s complaints, survey data (possibly previous rheumatic heart disease), objective examination (auscultation) and additional studies.
The appearance of a patient who has rheumatic mitral valve disease has the following signs:
- the typical patient has an asthenic physique with undeveloped muscle mass and cold upper extremities;
- cyanosis of the lips, chin, nose, ears, combined with a bright bluish-pink blush on the cheeks and pallor around the eyes (due to dilation of skin vessels and prolonged hypoxemia).
The auscultatory picture of mitral defects is quite bright and a competent specialist who knows this method can easily suspect this pathology.
Electrocardiography (ECG) helps to identify thickening or damage to the myocardium, detect changes in the size of cavities, and verify arrhythmias.
X-ray of the chest cavity is important for diagnosing dilatation of the cavities of the heart and the severity of damage to the bronchopulmonary tree.
However, the “gold standard” for detecting heart defects is echocardiography. The value of ultrasound examination is determined by the fact that it allows not only to identify the degree of narrowing or widening of the atrioventricular opening, to evaluate the anatomy of the valves themselves, but also provides data on intracardiac circulation.
The diagnosis is difficult because its manifestations are nonspecific. It is necessary to take into account the connection with a previous streptococcal infection and an increase in the level of anti-streptococcal antibodies in the blood. Taking into account major and minor criteria helps the diagnosis. The combination of two major criteria or one major and two minor when indicating a previous streptococcal infection makes the diagnosis very likely. carried out primarily with infectious-allergic myocarditis (IAM) and neurocirculatory dystonia (NCD). Unlike rheumatism, IAM occurs at the height of infection without a latent period and is not accompanied by articular syndrome, symptoms of vasculitis, or laboratory signs of high activity of the process. Patients with NCD are characterized by a variety of cardiac complaints, low-grade fever in the absence of signs of myocardial damage (changes in heart sounds, the appearance of murmurs) and changes in blood tests characteristic of rheumatic carditis.
In some cases, primary rheumatism is differentiated from systemic lupus erythematosus, infective endocarditis, etc. As immunosuppressive therapy in patients with high activity of the process, occurring with signs of serositis, vasculitis, corticosteroids are prescribed: prednisolone 20–30 mg per day for 10–14 days with a gradual reduction of the dose by 2.5 mg every 3-4 days to 10 mg, after which the dose is reduced weekly. With less activity of the process, as well as after treatment with corticosteroids, aminoquinoline derivatives are prescribed for 6–8 months. up to 1–2 years.
Shabalov N.P.
Treatment of rheumatism
Treatment of rheumatic heart disease is a long process. The disease requires a responsible approach. Only by starting therapy in a timely manner can rheumatism be cured and the development of complications prevented.
Clinical recommendations for the treatment of the disease include the use of a comprehensive regimen. This includes drug therapy, traditional methods, physiotherapy, the use of physical therapy, massage and other auxiliary methods.
First aid for acute rheumatic fever is the use of anti-inflammatory drugs, antibiotics and glucocorticosteroids.
Further treatment is prescribed taking into account the clinical picture of the disease and examination results.
Drug therapy
It is necessary to consider how to treat rheumatic carditis. Therapy of the disease involves the simultaneous use of different groups of drugs.
Treatment for chronic rheumatic heart disease includes:
- Nonspecific anti-inflammatory drugs. They have a complex effect: relieve pain, inflammation, reduce swelling. These include: Paracetamol, Meloxicam, Ibuproprofen, Indomethacin, Voltaren, etc.
- Glucocorticosteroids. They have powerful anti-inflammatory, antihistamine and analgesic properties. You should use hormonal medications for rheumatism only on the recommendation of a doctor.
- Antibiotics for rheumatism of the joints and heart are a key stage of treatment. In this case, agents based on penicillin or sulfonamides are used.
- Quinoline drugs. Indicated for use in recurrent forms of the rheumatic process. These include: Plaquenil, Delagil. At the same time, it is recommended to use salicylates, in particular Aspirin.
- Cytostatic immunosuppressants. They are used in the absence of a positive result from glucocorticosteroids and quinoline drugs, when heart tissue is severely damaged. While taking cytostatics, it is necessary to monitor the main hematological parameters.
- Diuretics and cardiac glycosides. Tablets and medications can only be selected by a doctor, because their use is indicated in cases of severe damage to the cardiovascular system.
- Gamma globulins. Helps desensitize the body. Medicines are used only in the absence of an acute inflammatory process in the membranes of the heart.
- Vitamins. Designed to strengthen the immune system and increase the patient's own defenses. For rheumatism, ascorbic acid and rutin are used.
- Symptomatic therapy. High temperature during acute rheumatic fever is reduced by antipyretics.
When conducting therapy, it is necessary to take into account how long the treatment of the disease lasts. Medicines for rheumatism of the heart are prescribed for a long time, until the patient’s condition is completely stabilized and laboratory parameters are normalized. In the future, there may be a need for maintenance therapy.
When joints are involved in the pathological process, it is advisable to use external agents: ointments, creams, gels based on NSAIDs.
Adjuvant therapy
Treatment of heart rheumatism is carried out not only with medications, but also with auxiliary methods.
Homeopathic medicines show good results. However, it takes a long time to achieve a positive effect.
During the recovery period, it is recommended to use physiotherapeutic methods: ultraviolet irradiation of joints, electrophoresis, mud therapy, dry heat, etc.
Massage and physical therapy for rheumatism can activate blood circulation, improve metabolic processes in affected tissues, prevent muscle atrophy, maintain mobility in joints and prevent dysfunction of the limbs.
Massage for rheumatism is carried out only by a specialist. The procedure is indicated outside the period of exacerbation or if clinical symptoms are mild.
Semi-precious stones cure rheumatic heart disease, weakness of the heart, inflammation in the joints, and help cope with fever. The following have healing properties: ruby, cat's and tiger's eyes, sapphire.
Forecast
Chronic rheumatic heart disease has a poor prognosis, especially if there are severe lesions of the valve apparatus.
An important role is played by the age at which the first attack of rheumatic fever was registered. In children, the pathology is more severe than in adults, which can threaten the formation of heart defects.
Some patients are interested in the question of whether invadity is given for rheumatic carditis. National guidelines require assessment to establish irreversible changes in the cardiovascular system. In the future, the disabled child is subject to medical supervision.
Rheumatic heart disease: symptoms, diagnosis, treatment
Rheumatic heart disease can develop in people of any age. The pathology is more often diagnosed in women after 40 years of age, although it also occurs in men and children. This is the most common organic lesion of the heart valve apparatus.
Mechanism of occurrence
Rheumatism is a severely developing complication of diseases of infectious origin. The problem is characterized by damage to the connective tissue by the inflammatory process.
Most often, the cardiovascular system suffers from this. Rheumatic changes lead to changes in the boundaries of the heart and are accompanied by the formation of nodular formations on the walls of the ventricles and heart muscle.
With the development of the inflammatory process, the nodules become scarred.
Because of this, cardiosclerosis, endocarditis and other pathologies subsequently occur.
As a result of the defects, the functioning of the valves that ensure normal blood flow is disrupted. Under the influence of rheumatism, valve insufficiency develops. Of the manifestations, the most common is a violation of the outflow of blood during diastole.
Nodules and scars impair the passage of blood, causing the organ to become overloaded, the underlying valves to expand, and hypertrophic changes to develop in the tissues of the heart. Such difficulties in the functioning of the organ cause oxygen starvation and congestive heart failure.
At the initial stages of development, rheumatic heart defects are mild. As the disease progresses, the functions of the mitral valve deteriorate, and it does not close the hole completely, which is why large volumes of blood enter the organ.
Increased blood flow leads to an enlargement of the left atrium. This is dangerous due to the development of stagnation in both circulation circles. The disease progresses under the influence of hereditary and constitutional predisposition. This is due to the fact that infectious diseases do not always cause rheumatism, and it does not always lead to the development of defects.
How are they classified?
Rheumatic defects can be isolated, when the functioning of one valve is impaired, or combined, when there is a failure in several valves.
In connection with pathological changes, the development of:
- Stenosis. At the same time, the valves are fused and the passage between the chambers is reduced. Due to the anomaly, the required amount of blood does not penetrate into the cavity. Pathology usually occurs in older people.
- Insufficiency. The disease is characterized by incomplete closure of the valves. Due to dysfunction, the outflow of blood is disrupted, and some of it returns back to the heart and stagnates there. This causes an increase in load on the organ and an increase in size.
- Combined defects. In this case, the deficiency is combined with stenosis. The disease has a severe clinical picture and complications.
Depending on the damage to the cardiac membrane, the pathology develops in the form of:
- Rheumatic myocarditis. The inflammatory process affects the muscular lining of the heart. The disease is not accompanied by complications.
- Rheumatic endocarditis. Mitral valve insufficiency is caused by damage to the inner lining.
- Rheumatic pericarditis. Inflammation of the pericardium leads to destruction of the outer membrane. The pathology is usually severe.
- Pancardita. This is the most dangerous scenario. In this case, all layers of the heart become inflamed, and its contractility is impaired. The disease is accompanied by serious disturbances in blood flow and sudden cardiac arrest.
The consequences depend on the type of pathological process.
Diagnostics
Rheumatoid heart disease is diagnosed using a physical examination, laboratory and instrumental examinations.
If a pathological process is suspected, blood is taken for general and biochemical examination to determine the inflammatory process and the presence of infection. After this, instrumental techniques are prescribed to confirm the diagnosis. These include:
- Electrocardiogram. With its help, heart rhythm disturbances are detected and the type of arrhythmia is determined. Ischemic disorders and heart block are also determined.
- Phonocardiography. It is necessary to record extraneous noise and associate it with defects.
- X-ray examination of the chest. The procedure determines the presence of hypertrophic changes in the heart. The image also shows the presence of congestion and damage to the atria.
- Echocardiography. Using ultrasound, they determine how much the contractility of the heart has decreased and identify changes in the structure of the heart muscle and valves.
After confirming the diagnosis and determining the type of pathology, treatment is prescribed.
Complications
Damage to the heart by rheumatic disease leads to:
- heart rhythm disturbances;
- chronic form of heart failure;
- stroke;
- blockage of a pulmonary artery by a thrombus;
- infective endocarditis.
Pathologies develop if the disease is not treated.
Possible complications
Complications of rheumatism are caused by damage to the valves and other structures of the heart.
Main consequences:
- Impaired pumping function of the heart. This threatens the development of heart failure.
- Transition of the pathological process to the chronic stage. In this case, relapses cannot be ruled out, which leads to myocardial sclerosis.
- The occurrence of rheumatic heart disease. The heart valves are most often affected during rheumatic attacks. As a result of scar changes, adhesions are formed, leading to the formation of stenosis and other disorders. These include: mitral stenosis and mitral heart disease, mitral valve insufficiency and aortic defects.
- The likelihood of a stroke or heart attack increases, which is due to an increased tendency to thrombus formation in rheumatism.
- Heart failure. Possible as a result of acute cardiac arrhythmia.
Symptoms, signs and chief complaints of patients
The clinical picture of the disease depends on the type of the defect itself, the degree of disturbances in intracardiac and systemic hemodynamics, the duration of the pathological process and the level of problems from other organs and systems.
In the compensation stage, which occurs without signs of heart failure, patients do not complain about their health and may not come to the doctor’s attention for a long time. And only with the development of decompensation the following complaints and signs appear:
- shortness of breath – associated with increased pressure in the pulmonary circulation (PCC);
- hemoptysis - due to sweating of blood cells with pronounced stagnation in the veins of the ICC;
- dull cardialgia;
- interruptions in the functioning of the cardiac system - palpitations, arrhythmias, atrial fibrillation, extrasystoles.
Combined (not combined) mitral valve disease very quickly decompensates, as a result of which it is accompanied by stagnation of blood in the systemic circulation, which clinically manifests itself as swelling of the neck veins, heaviness in the right hypochondrium and enlargement of the liver (hepatomegaly), edema of the lower extremities.
Diet for rheumatism
Nutrition for rheumatism should be complete and balanced. The diet should contain foods containing large amounts of protein and low carbohydrates. You need to eat often, at least 5-6 times a day.
Chronic rheumatic heart disease involves enriching the menu with fermented milk products. Fresh vegetables and fruits are healthy.
The menu should include low-fat varieties of fish and meat, chicken eggs, currants, rhubarb, etc.
The diet for rheumatism limits the consumption of salt, spicy, salty, fried, fatty foods.
Disease prevention
There is primary and secondary prevention of rheumatism of the heart. Primary measures are aimed at preventing streptococcal infection. To do this, you need to strengthen your immune system, harden yourself, visit a sauna, and a swimming pool. Organize a complete, balanced diet.
To prevent complications, you need to promptly consult a doctor for medical help for ARVI or sore throat. Do not ignore antibacterial therapy if angina develops.
Secondary prevention is aimed at preventing rheumatic heart defects. For this purpose, long-acting bicillin prophylaxis is used.
Prevention of the formation of defects is carried out by a rheumatologist, who monitors patients throughout their lives.
Mitral heart disease (combined, rheumatic, etc.): symptoms, treatment, diet, etc.
Heart disease is a disease caused by pathological changes in valves or openings that impair the functioning of the heart muscle. According to statistics, in terms of frequency of detection, the disease is second only to atherosclerosis and hypertension.
Mitral disease develops due to damage to the bicuspid valve, which is located on the left side of the heart. During normal operation, the valves are open, blood moves into the left ventricle, and from there into the aorta, after which the valve closes. Narrowing of the vessels of the mitral orifice and insufficiency of the left ventricular valve cause disruption of blood flow, which leads to disruption of the heart.
Types and reasons
Defects are divided into congenital and acquired. Congenital - formed during gestation. They may be a consequence of impaired intrauterine development of the fetus or a previous infection. Pathology is detected during ultrasound examination. Immediately after birth, the child develops hypoxia (oxygen starvation) and impaired respiratory function.
Normal structure of the heart
An acquired defect develops throughout life. Experts identify combined and combined defects. When combined, narrowing of the orifices and valve insufficiency are simultaneously present.
Combined defects are expressed in damage to one or more valves: tricuspid, mitral and aortic.
Provoking factors are:
- autoimmune diseases caused by streptococcal infection;
- infectious diseases;
- tuberculosis;
- connective tissue diseases.
Rheumatoid manifestations are considered the main cause of mitral valve disease. Pathology occurs in 80% of cases. Rheumatism affects all structural components of the heart muscle. After suffering inflammation, thickening of fibrous tissue (a type of connective tissue) occurs on the mitral valve. Scarring shortens the valves, preventing the valve from opening normally.
Mitral disease is divided into:
- mitral stenosis;
- heart valve insufficiency;
- complex (combination of the first two forms).
Quite often, cardiologists detect mitral valve prolapse. This is the sagging of one or both valve walls into the left atrium as the left ventricle contracts. Pathology does not have a serious impact on a person’s well-being. Occurs in 25% of the population, women under 30 years of age are most often affected.
Mitral stenosis of the heart
Characterized by sticking of the valve walls. Over time, the flaps stick together, which causes the opening to narrow.
As a result, blood is poorly redistributed into the left ventricle from the left atrium, causing it to overflow. The normal mitral orifice ranges from 2–6 cm2.
When narrowing to 1 cm2, the pressure in the pulmonary atrium increases to 200 mm Hg. Art., forcing the blood to be pushed through with effort.
The walls of the valve stick together, causing the opening to narrow
Increased pressure and increased blood flow causes growth of the left atrium. If the disease progresses, pulmonary edema is possible. Over time, congestion spreads to the right side of the heart, causing swelling of the entire body.
Mitral regurgitation
With this anomaly, the valve leaflets do not close completely; blood flows back into the left atrium, which gradually stretches and hypertrophies.
At first, the body uses protective mechanisms, but congestion ultimately causes an enlargement of the right side of the heart.
Combined defect
If rheumatoid arthritis affects several orifices and valves of the heart muscle, they speak of a combined or complex defect. It manifests itself in insufficiency of the mitral and aortic valves, narrowing of the aortic orifice and limitation of the bicuspid valve.
Causes serious disturbances in the functioning of the heart. Complications include: chaotic heart rhythm, thromboembolism (acute blockage of a blood vessel by a thrombus). The course of the disease is often unfavorable and leads to death.
Symptoms
Clinical characteristics depend on the degree of heart valve damage. At first, the disease is asymptomatic, the person feels healthy. As the disease progresses, the following symptoms appear:
- dyspnea;
- cough;
- heart rhythm disturbance (arrhythmia or tachycardia appears);
- swelling of the limbs;
- fast fatiguability.
The patient's main complaint is an exhausting cough streaked with blood.
With mitral disease, the patient is characterized by a yellowish complexion, acrocyanosis of the lips (coloring of the lips dark blue due to insufficient blood supply). Due to the significant release of histamine-like substances, a bright blush appears on the cheeks.
From the moment of damage to the heart valve to the full clinical picture, the latent period lasts about 20 years. It mainly affects females aged 30 to 40 years. Mitral stenosis affects 76% of women from the total number of patients.
Mitral regurgitation, on the contrary, is more often diagnosed in men. Expressed in shortness of breath and heart rhythm disturbances. Sometimes there is a feeling of pressure in the chest, an aching, dull pain.
Diagnosis of the disease
Heart disease is diagnosed using:
- electrocardiography;
- daily ECG indicators;
- phonocardiography;
- MRI;
- rheumate tests;
- radiography.
Combined heart defects are difficult to diagnose because there is a layering of clinical symptoms. The primary diagnosis is made by visual examination of the patient. Instrumental examination can detect cardiac muscle hypertrophy and rhythm disturbances.
With the help of a phonocardiograph, murmurs and tones in the heart are assessed, radiography reveals congestion in the lungs, proliferation of chambers, and myocardial hypertrophy. If necessary, the patient undergoes probing, venography, and aortography.
Research will not only reveal the defect with great accuracy, but will also show the degree and form of severity of the disease.
With a combined defect, noise characteristic of stenosis and mitral insufficiency is recorded on the phonocardiogram. X-ray can reveal an expansion of the boundaries of the heart and a modification of the pulmonary pattern. Echocardiography and Doppler echocardiography confirm the diagnosis, clarify changes, the amount of pressure and regurtitation (backflow of blood) in the valves.
Treatment
Mitral heart defects are treated with medication and surgery.
Important! Patients need to reconsider their lifestyle and diet to prevent processes that can lead to heart failure.
It is recommended to reduce physical activity and avoid anything that leads to heavy breathing and rapid heartbeat.
You should limit your salt intake, as it retains fluid in the body, which creates additional stress on the muscle. In nutrition, preference is given to a dairy-vegetable diet; it is necessary to completely abandon fatty foods. They contain a lot of cholesterol, which leads to the formation of plaques and the development of atherosclerosis.
Alcohol, strong tea, and coffee provoke increased heart rate and a lack of nutrients in the myocardium, as a result of which the heart wears out faster.
Drug therapy
Treatment with drugs is aimed at preventing relapses, thromboembolic complications, and normalizing the heartbeat. To improve heart function the following is attributed:
- anticoagulants;
- diuretics;
- panangin, riboxin;
- beta blockers.
Surgical intervention
The operation is performed only if the patient has mitral stenosis. A special catheter is inserted into the patient, which is directed to the mitral valve and its opening is widened. This operation can be performed on the heart of a child who is in the womb. In this case, the catheter is inserted through the blood vessels of the woman's umbilical cord.
Most often, patients undergo prosthetic valves. In case of combined defects, plastic surgery of one or more valves is performed.
Surgical intervention is contraindicated for pulmonary emphysema, diffuse cardiosclerosis, hepatitis, and exacerbation of rheumatism.
ethnoscience
Traditional medicine acts as a supportive, strengthening therapy. Decoctions and infusions of medicinal herbs should be used only in combination with drug treatment.
Important! Refusal of traditional methods of treatment can lead to death.
Traditional medicine recipes:
- motherwort infusion – 4 tbsp. l. Brew herbs with a glass of boiling water. Place in a water bath for 15 minutes. Filter. Take 100 ml 2 times a day for 30 minutes. before meals.
- Beetroot juice – mix freshly squeezed juice with honey in a 2:1 ratio.
- Lovage infusion – 40 g of dried roots, pour 1 liter of water, boil for 5-7 minutes. Leave the broth for 3 hours, strain. Drink 100–120 ml 3 times a day. Helps with moderate defects and swelling.
- Collection of herbs - drink like regular tea. Brew snapdragon, prickly tartar, toadflax grass, centaury.
Prognosis and prevention
The prognosis of mitral valves in most cases is unfavorable. If combined defects are not treated, survival is up to 5 years in 45% of patients and only 6% - up to 10 years.
After the operation the situation improves. If only one valve is affected, the survival rate is 72%.
With combined defects, the outcome of the disease is determined by rheumatic lesions of the heart muscle and the frequency of attacks. In the case of severe hemodynamic disturbances (blood supply is impaired, the body does not receive enough oxygen and nutrients), the function of the scarred myocardium sharply decreases, which subsequently leads to death.
Prevention consists of preventing rheumatoid attacks, which are provoked by tonsillitis, pharyngitis, and scarlet fever.
Constant monitoring by a cardiologist, cardiac surgeon, or rheumatologist is recommended. Pregnancy is allowed provided that the blood circulation is fully compensated.
Mitral heart disease is a serious disease that in most cases is fatal. To prevent the development of the disease, you need to adhere to a healthy lifestyle, balance your diet and think positively.
- Anatoly Kupriyanov
Source: https://creacon.ru/bolezni-serdtsa/mitralnyie-poroki-serdtsa-raznovidnosti-simptomyi.html