Mitral valve plastic surgery is performed for pathologies of this part of the heart that cannot be cured with conservative methods. Reconstruction of the valve allows you to restore all its functions, prevent heart failure, and save the patient’s life. During the operation, plastic structures are used to completely rehabilitate the heart and avoid repeated problems with the valve. The procedure has its own characteristics, preparation and recovery rules.
Indications for surgery for mitral stenosis
Clinical signs, together with examination data and, first of all, the area of the left atrioventricular orifice, determine the timing of surgical intervention. Mitral stenosis with a mitral valve area ≤1 cm2 is considered critical. In physically active patients or patients with large body weight, a narrowing of the opening of 1.2 cm2 may also be critical. Surgical intervention (open mitral commissurotomy or mitral valve replacement) significantly improves the functional status and long-term survival of patients with mitral stenosis - 67% and 90% of patients are alive within 10 years. However, patients who underwent commissurotomy frequently underwent reoperation during this period (42% vs. 4%). Despite the higher risk of surgery in patients with high pulmonary hypertension and right ventricular failure, their condition improves with a decrease in pulmonary artery pressure. Thus, the indication for surgery in patients with mitral stenosis is a decrease in the area of the mitral valve <1.5 cm2 and II and more functional NYHA class.
Etiology:
- Inflammatory lesions: rheumatism, systemic scleroderma, aortoarteritis.
- Degenerative processes: myxomatous degeneration.
- Atherosclerosis.
- Infectious processes: infective endocarditis.
- Congenital pathology: bicuspid aortic valve.
With aortic valve pathology, the frequency of complications in the form of infective endocarditis is higher than with mitral valve pathology.
Bicuspid aortic valve is the most common congenital heart defect (prevalence: 2%). If this anomaly is detected in childhood, patients should be under the supervision of a cardiologist throughout their lives, and if clinical symptoms of aortic stenosis appear, also a cardiac surgeon. There is a tendency to increase the frequency of involutional (degenerative-atherosclerotic) causes of aortic stenosis, which has led to an increase in age patients over 60-65 years of age requiring surgical correction of aortic disease. With congenital or rheumatic valve damage, a long latent period without clinical manifestations is observed. Mortality and the risk of complications increase significantly with the onset of symptoms of the disease. With angina pectoris, fainting and manifestations of heart failure caused by systolic dysfunction of the left ventricle, the average life expectancy is 5, 3 and 2 years, respectively. In asymptomatic patients, the risk of sudden death is low (even with severe aortic stenosis), while in the presence of symptoms, 15–20% of patients die suddenly.
Indications for surgery for mitral insufficiency
The annual mortality rate for drug treatment of symptomatic mitral valve prolapse is 6.3%. In these patients, a strategy of early surgery after diagnosis is associated with a better long-term prognosis, resulting in improved contractility and regression of left ventricular hypertrophy, and a decrease in left heart volumes. On the other hand, in patients with significantly damaged contractile function of the left ventricle, improvement in the latter may not occur. In this regard, surgical treatment of mitral regurgitation should be carried out before the CSI index reaches 40-50 ml/m2, since its increase ≥60 ml/m2 suggests an unfavorable prognosis. Other good prognostic markers for adverse effects of surgery are high NYHA functional class, concomitant coronary pathology, older age, and low right ventricular ejection fraction. Mitral valve plastic surgery for myxomatous lesions suggests good early and long-term functional results. Because fewer complications and lower in-hospital mortality are observed with valve repair compared with valve replacement, surgery should be performed early after diagnosis. The appearance of left ventricular systolic dysfunction dictates the need to maintain anullopapillary continuity during surgical correction. Surgical correction of ischemic mitral regurgitation is associated with a higher risk (9-30%), which is due to a decrease in the contractile function of the left ventricular myocardium. Mitral valve plasty is indicated for grade III-IV mitral valve insufficiency and preserved contractility of the left ventricle (co-option height ≤ 11 mm). In patients with reduced contractility (EF≤40%), grade II mitral insufficiency is also an indication for correction. In case of rupture of the papillary muscle or cooptation height ≥ 12 mm, bioprosthetic replacement of the mitral valve with preservation of the subvalvular apparatus is indicated. Patients who have undergone plastic surgery on the mitral valve, due to the preservation of the integrity of the fibrous framework of the left ventricle, have better survival and long-term prognosis. The 5-year survival rate after mitral valve repair compared to mitral valve replacement is 58-64% and 36-47%, respectively. According to the Mayo Clinic, the 5-year mortality rate in patients with ischemic mitral regurgitation with medical treatment was 62%, while with surgical treatment it was 39%. Patient survival is inversely proportional to the size of the effective regurgitant opening and the volume of the regurgitant jet. The 5-year survival rate in patients with an effective regurgitation orifice area of ≤20 mm2 and ≥ 20 mm2 was 47% and 29%, and in patients with a regurgitation volume of ≤30 ml and ≥ 30 ml, 44% and 35%, respectively. At the same time, in patients with organic mitral regurgitation, the area of the effective regurgitation orifice ≥40 mm2 is a risk factor that determines the same long-term survival. If surgical correction of mitral regurgitation is performed before volume overload myopathy reaches an irreversible stage, left ventricular function returns to normal. On the other hand, a delay in surgery, even with a favorable course of the postoperative period, leads to persistence of signs of congestive heart failure 5, 10, and 14 years after surgery in 23%, 33%, and 37% of patients. III/IV preoperative NYHA functional class is a prognostic sign that determines the long-term prognosis of patient survival. A decrease in ejection fraction after mitral replacement for mitral regurgitation is the result of a postoperative increase in afterload. Activation of the neurohumoral system may contribute to the deterioration of heart failure patients by limiting vasodilation. The persistence of excessive neurohumoral activation probably reflects incomplete restoration of left ventricular contractility after surgical treatment.
Preparing for surgery
Preparation for valve surgery begins immediately after the cardiologist has suggested the need for this operation. The patient’s action algorithm in this case can be determined based on the following aspects:
- The first thing you need to do is get a consultation with a cardiac surgeon, but come to his appointment with the latest results of a heart ultrasound and ECG.
- If the cardiac surgeon confirms the need for intervention on the heart valves, the patient must decide whether he will receive cardiac surgery treatment free of charge or at his own expense.
- In the case of a free operation, the patient must take all medical documents (extracts from the hospital, examination results, referral from a cardiac surgeon) to the regional department of the Ministry of Health in order to receive a quota.
- After receiving a quota (sometimes you have to wait several months), the patient must undergo the examination necessary for the operation. This includes blood tests for HIV and viral hepatitis, blood tests for coagulation (VSC, APTT, INR, prothrombin time and index, etc.), general clinical tests (blood, urine), FEGDS and some others.
- Once the patient has a referral to the appropriate clinic and test results, he should call the hospital where such operations are performed and find out what time he should be admitted to the hospital.
- After the patient arrives at the clinic, he is admitted to the cardiac surgery department, where, after examination by doctors, preoperative preparation will be carried out.
- On the eve of the operation, the patient is prohibited from eating (the last meal should be no less than 8 hours before the operation).
Preoperative preparation
In patients with signs of congestive heart failure, aggressive diuretic therapy and sodium restriction are required before surgery. For atrial fibrillation, patients need digoxin, beta blockers, and calcium antagonists to slow the heart rate. Patients with acute mitral regurgitation are often in cardiogenic shock; their condition is stabilized with the help of inotropes, arterial vasodilators, and intra-aortic balloon counterpulsation. Vasodilators reduce peripheral vascular resistance and accelerate the rhythm, reducing the amount of regurgitation into the left atrium.
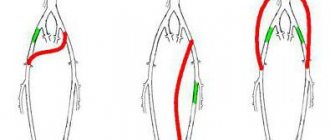
Mitral commissurotomy
For mitral stenosis, the operation of mitral commissurotomy remains relevant to this day. Since the first valvotomy performed by Elliot Cutler in 1923, the procedure has undergone a number of modifications. The ability to control the position of the dilator in the projection of the mitral orifice using transesophageal echocardiography allows this procedure to be performed from a minimally invasive approach. To do this, a left-sided thoracotomy is performed using a 6 cm incision in the fifth intercostal space. After dissection of the pericardium, a mattress suture on pads is placed at the apex of the left ventricle and a Dubost dilator is inserted through it. The dilator branches, under the control of transesophageal echocardiography, are carried into the stenotic opening and opened to 2.5-3 cm. The effectiveness of minimally invasive commissurotomy is monitored by echocardiography
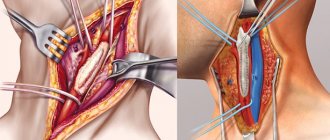
Traditional mitral commissurotomy. 2-EchoCG image of the dilator position during minimally invasive commissurotomy. 3-Doppler EchoCG absence of regurgitation Open operations on the mitral valve are carried out mainly through a longitudinal median sternotomy. The heart-lung machine is connected according to the vena cava – ascending aorta circuit. Normothermic and antegrade perfusion is performed, and in case of ischemic mitral insufficiency, combined - ante/retrograde hypothermic cardioplegia. The optimal approach to the mitral valve is an incision in the left atrium posterior to the interatrial groove.
Access to the mitral valve through the left atrium. SVC, IVC – superior vena cava and inferior vena cava; LA and RA – left and right atria. It is possible to use access through the right and left atrium. This approach promotes better exposure of the mitral valve, however, injury to the interatrial septum can lead to various disorders 169″[/img] Access to the mitral valve through the right, the roof of the left atrium and the interatrial septum Minimally invasive open correction of the mitral valve is carried out through a right anterolateral thoracotomy in the 5th intercostal space. Connection of the AIK is carried out as standard directly in the wound or through the femoral vessels using the Seldinger catheter technique.
Access to the mitral valve during minimally invasive surgery
Operation technique
Plastic surgery is performed only in a hospital setting, in an office specially equipped for the operation. If it is carried out using an endoscope, there will be monitors in the room to monitor the process. First, the patient is taken for premedication, and sedatives and hypnotics are injected into a vein. After falling asleep, the plastic surgery itself begins.
The surgeon makes an incision on the front wall of the chest, then the breast bones. They open access to the heart layer by layer. A cardiopulmonary bypass machine (ACB) is connected. This device will simulate the work of the lungs, saturating the blood with oxygen while manipulations are performed on the heart. Tubes from the blood pump are connected to the chambers of the heart; blood will flow to it, be saturated with oxygen and disperse throughout the body. Then the surgeon begins the main stage of work, it will depend on what exactly happened to the valve.
For mitral insufficiency, a so-called annuloplasty is performed. A plastic ring is placed near the valve opening to restore lumen and normal blood flow.
The sashes can be connected manually - this is suture plastic. If stenosis is diagnosed, a commissurotomy is needed. This is the manual separation of fused leaflets in a valve. Stenosis surgery is also carried out without connecting to the artificial blood pressure pump; it is performed through a small hole between the ribs on the left side. During the procedure, the patient's condition is monitored using medical equipment. Blood pressure and respiration are constantly measured. When all the work is completed, the AIK is turned off, and the surgeon sutures the opening sites layer by layer. External seams are treated with an antiseptic and a tight bandage is applied. Before taking the patient out of the operating room, his condition is checked again.
In the first days after the operation, the patient is constantly monitored by doctors. He remains in the hospital for another 5-7 days, depending on the complexity of the operation and the speed of rehabilitation. In the first 1-2 days, bed rest and diet are indicated.
Activity is gradually restored under medical supervision. Then the operated patient is discharged, prescribed medications for rehabilitation and a routine examination by a cardiologist and therapist.
Simple mitral valve disorders are resolved using minimally invasive techniques. Several small incisions are made in the chest, into one of which an endoscope, a device with a micro-camera, is placed. The surgeon performs the operation without a strip opening, so after such manipulations the patient undergoes rehabilitation faster.
Mitral valve replacement
The operation should be performed without damaging the anatomical structures surrounding the mitral annulus (circumflex branch of the left coronary artery, atrioventricular node, aortic valve leaflets and left atrial appendage), the location of which is shown in the figure.
Localization of intracardiac structures around the mitral valve annulus After visual assessment of the mitral valve, it is excised with careful decalcification of the annulus. The chordae are cut off at the level of the heads of the papillary muscles to prevent possible jamming of the valves of the mechanical prosthesis. Lillehei in 1964 first suggested the importance of the subvalvular apparatus as an important functional component of the systolic and diastolic work of the left ventricle, capable of maintaining optimal ventricular geometry. After excision of the chordal ligamentous apparatus, the global systolic function of the left ventricle can decrease by 33-46%; on the contrary, after prosthetics with complete or partial preservation of the subvalvular structures, the contractile ability of the ventricle improves. The contribution of preservation of the chords, the anterior leaflet of the mitral valve, is slightly greater than the preservation of the chords of the posterior leaflet. Mitral valve repair improves ventricular function by maintaining optimal ellipsoidal geometry of the left ventricle. In patients with mitral stenosis, preservation of these structures likely has little effect on left ventricular dysfunction but may prevent implantation of a graft of sufficient diameter. In patients with mitral regurgitation, this procedure should be performed, especially in the presence of preoperative left ventricular failure. When implanting a bioprosthesis, the leaflets of the native valve, with the exception of severe fibrosis or calcification, do not require resection. When replacing the mitral valve with a mechanical prosthesis, maintaining the mitral valve sails can lead to jamming of the prosthetic leaflets. As a rule, the posterior leaflet of the native valve does not interfere with the function of the mechanical prosthesis and can be completely preserved. The technique for preserving the subvalvular apparatus is different and consists in partial resection of first the anterior leaflet, and, if necessary, the posterior one, with subsequent fixation of them to the fibrous annulus of the mitral valve.
Technique for preserving subvalvular structures For fixation of prostheses, 3\0 or 2\0 sutures with Teflon gaskets are used. The method of suturing depends on the type of implanted prosthesis. Biological valves are fixed by sutures from the ventricular side (non-everting or subcircular suture). When inserting a prosthesis into the mitral annulus, care must be taken to ensure that none of the sutures form a loop around the prosthesis post. Mechanical prostheses are fixed with sutures applied from the atrium. This method prevents the possibility of jamming of the prosthetic valves by the muscle tissue of the left ventricle.
Technique for applying fixing sutures during implantation of bio- (1) and mechanical (2) prostheses The depth of the sutures should not exceed 2-3 mm, especially in the area of the posterior part of the ring, since cutting the sutures entails the formation of a dissecting aneurysm of the posterior wall of the left ventricle. This complication, manifested by massive bleeding due to ventricular rupture, requires complete excision of the prosthesis and closing the dissection with a patch from the inner surface of the left ventricle. Fixation of the prosthesis with a continuous suture is currently rarely used due to the possible complete separation of the prosthesis due to the development of infection. In case of atrial fibrillation, before the left atrium is closed, its appendage is ligated or sutured from the inside to prevent thrombus formation. The left atrium is sutured with 3\0 thread.
Prosthetic heart valves – what are they?
Since the 1970s, the configuration of prosthetic valves has undergone some changes. Valves based on ball prostheses are considered one of the most outdated.
Later, valves based on hinged disc prostheses began to be used.
The most modern valves are those based on bicuspid hinged prostheses, which are currently used.
In addition, in patients with an increased risk of thrombosis, models obtained from the pig heart are used - biological prostheses, or xenografts.
The disadvantage of mechanical prostheses is the high rate of formation of blood clots on the valve leaflets , which is associated with a high risk of pulmonary embolism, ischemic stroke, thrombosis of the femoral arteries with possible amputation of a limb, etc. In this regard, in elderly people (over 65 years old) It is preferable to perform valve replacement surgery with a biological prosthesis. It is also possible to have an operation with prosthetic replacement of the aortic valve with the patient’s own pulmonary valve with simultaneous replacement of the latter with a biological prosthesis.
The disadvantage of biological prostheses is the high risk of re-development of bacterial inflammation on the installed porcine valve.
The service life of the valves in the absence of complications is from 10 to 15 years; if the valve wears out, it is possible to perform a second operation to replace it.
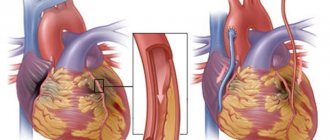
Related operations
Coronary artery bypass grafting is the most common procedure performed to correct mitral heart disease, especially of ischemic origin. Distal anastomoses on the posterior and inferior surfaces of the heart must be performed before valve replacement to prevent injury to the posterior wall of the left ventricle during cardiac enucleation. Correction of tricuspid valve disease is performed after completion of manipulations on the mitral valve. For this, additional access is used through the wall of the right atrium, if it was not opened when accessing the mitral valve. If it is necessary to correct concomitant aortic heart disease, the sequence of actions is as follows: first, the aortic valve is excised, then the mitral valve is corrected, and the aortic prosthesis is implanted last. Before removing the aortic clamp, careful prophylaxis of air embolism through the left ventricular apex, ascending aorta, and left atrium drainage is performed using volume loading and increased pulmonary excursion. Postoperative arrhythmias are a fairly common occurrence. Drug correction is carried out with amiodarone, β-blockers, digoxin. In patients with tachyform atrial fibrillation, if there is no effect of therapy, cardioversion may be performed. Bradyarrhythmias require more frequent pacing. Anticoagulant therapy is indicated in all patients with mechanical or biological valves. Warfarin is prescribed on the second postoperative day under the control of the international normalized ratio (INR), which should be 2.5-3.5. For patients with bioprostheses and sinus prostheses, therapy lasts 6-12 weeks, for patients with atrial fibrillation and mechanical prostheses - for life.
How is the operation performed?
Preoperative preparation is limited to the prescription of sedatives and hypnotics. The operation is performed under general anesthesia on the same or the next day after hospitalization using a heart-lung machine, which performs the functions of pumping blood throughout the body during manipulations.
After putting the patient into deep sleep, a median sternotomy is performed - a longitudinal incision of the skin and sternum. Next, an incision is made in the left atrium for mitral valve replacement and in the aortic wall for aortic valve replacement. After this, the prosthesis ring is fixed with continuous sutures and the dissected part of the heart is sutured.
After installing the prosthesis, electrodes for temporary cardiac stimulation must be applied, and the surgical wound is sutured. Wire sutures are used to fuse the edges of the sternum.
In the early postoperative period, the patient is in the intensive care unit with artificial ventilation, the cessation of which is possible only when the patient is completely stabilized and spontaneous breathing is restored.
The operation time is from three to six hours, and the hospital stay is determined by the general condition of the patient and ranges from two to four weeks.
In addition to open heart operations, it is currently possible to perform minimally invasive operations, in particular, with a mini-access from an intercostal incision on the right or left without dissecting the sternum, as well as with endovascular intervention.
minimally invasive aortic valve replacement
The latter is used only for aortic valve replacement and is carried out by introducing a biological prosthesis through the femoral vein into the right and then into the left atrium with further location in the aorta.
Endovascular heart valve replacement is primarily preferred for individuals for whom open heart surgery is contraindicated.
Video: report on valve replacement surgery
Mitral valve repair
A. Carpentier in 1983 theoretically substantiated and first performed plastic surgery on the mitral valve. He proposed three main types of correction: type I - remodeling of the mitral valve ring using the implantation of a rigid or flexible plastic ring, ensuring restoration of its normal area and shape; Type II – elimination of excess mobility of the leaflets by resection of the corresponding segment of the leaflets, shortening and translocation (from the posterior to the anterior leaflet) of the mitral valve chords; Type III – restoration of mobility of chords and valves (fenestration of primary chords and papillary muscles, resection of secondary chords). To simplify the understanding of plastic procedures on the mitral valve, A. Carpentier proposed a surgical anatomical classification of the mitral valve: the anterior leaflet is divided into three portions (AI, A2, A3) and the posterior leaflet is also divided into three portions (PI, P2, P3). S. Duran (1994) divides the anterior leaflet into two portions (AI, A2), the posterior leaflet into three portions (PI, PM, P2) and identified commissural portions (CI, C2)
Surgical anatomy of the mitral valve. 1 - according to A. Carpentier, 2 - according to S. Duran
Annuloplasty
Typically, dilatation of the mitral valve annulus occurs due to its posterior part, since the anterior part of the annulus is connected to a rigid structure - the interventricular septum. Revision of the mitral valve makes it possible to determine the possibility of performing plastic surgery: the valves must be sufficiently mobile without pronounced prolapse. To select the size of the ring, a special calibration device (template) is used, which allows, based on measuring the length of the base of the anterior leaflet of the mitral valve, to determine the required size of the plastic ring. Subsequently, mattress sutures are placed along the entire perimeter of the valve ring and parallel to it to a depth sufficient to capture the fibrous ring. In this case, it is necessary to avoid damage to structures located in direct contact with the mitral valve annulus. Different types of rings are used: rigid, flexible, full or partial. The use of rigid rings is mandatory for mitral regurgitation of ischemic origin, especially with ischemic cardiomyopathy, since the rigid structure is more reliable in the isolated postoperative period. For the same purpose, rings of small (No. 26-28) sizes (hypercorrection) have recently been more often used for plastic surgery for ischemic mitral insufficiency. The ring is fixed according to the marks dividing it in accordance with the normal anatomical ratio of the length of the base of the anterior (1\3) and posterior (2\3) cusps of the mitral valve.
Technique of annuloplasty on a rigid ring: 1 – determination of ring size; 2 – suturing along the perimeter of the mitral valve; 3 – ring fixation For annuloplasty, it is possible to use incomplete rings (rigid or flexible) or a strip of biological or synthetic material 46-52 mm long with fixation along the posterior 2/3 of the circumference of the mitral valve. Mattress sutures are carried out by capturing the fibrous ring and overlapping each other by 1/2, which provides additional strength of fixation.
Technique of annuloplasty on a half ring: 1,2 – diagram of sutures; 3.4 – fixation of the half ring At the final stage, the tightness of the valve must be monitored by injecting saline solution under pressure into the cavity of the left ventricle. Detection of significant regurgitation during the test requires revision of the subvalvular structures, since regurgitation is a consequence of incomplete cooptation of the leaflets due to prolapse of one of them.
Carrying out a hydraulic test of valve tightness It is possible to apply an additional suture according to O. Alfieri at the site of regurgitation. It must be remembered that this method can lead to stenosis of the atrioventricular orifice if the ring for plastic surgery is selected in a small size (No. 26-28). Dissatisfaction with the results of plastic surgery is an indication for prosthetic replacement already at this stage of the operation. Additional monitoring of the effectiveness of the plastic procedure is carried out using transesophageal echocardiography after restoration of cardiac activity.
Cost of the operation
In most cases, surgery to replace heart valves is performed free of charge, thanks to quotas from the Russian healthcare system under the compulsory medical insurance system. However, if for some reason it is not possible to obtain a quota, there is always the option of carrying out the operation at your own expense.
The cost of the operation itself, the prosthesis and rehabilitation in the early postoperative period ranges from 90 to 300 thousand rubles , and the higher the price, the more complex the operation is, for example, the simultaneous replacement of the aortic valve and pulmonary valve is higher than one of them.
Heart valve replacement surgeries are carried out in all major cities of Russia, and now such interventions are not rare or inaccessible to the population.
Edge-to-edge plastic surgery
O. Alfieri et al. (2001) proposed a method for eliminating prolapse of the anterior leaflet of the mitral valve using a suture attaching the prolapsed part of the anterior leaflet to the unchanged posterior leaflet (Fig.). This maneuver creates a double-lumen atrioventricular opening, limits the mobility of the anterior leaflet and ensures the tightness of the valve. Subsequently, the O. Alfieri suture began to be used as an addition to create better MV competence in case of inadequacy of other plastic procedures on the mitral valve.
Technique for performing edge-to-edge plastic surgery according to O. Alfieri
Pros and cons of the operation
Surgery on the mitral valve is performed in two ways.
- Prosthetics and suturing for dilatation of the valve ring.
- Plastic surgery of valves when they are not fully operational.
- Correction for limited mobility of the valves.
Surgical intervention of any kind has virtually no negative consequences. The main danger is complications after open-heart surgery. However, this risk is reduced to tenths of a percent.
But the operation has many advantages. These include:
- almost zero possibility of thromboembolic or infectious complications;
- almost one hundred percent recovery and survival of patients;
- there is no need for lifelong use of antiplatelet drugs and anticoagulants;
- disappearance of symptoms of chronic heart disease;
- increase in life expectancy.
How to replace a valve apparatus
Resection of valves
Manipulation is carried out mainly on the posterior leaflet, since it most often prolapses with myxomatous valve degeneration. During echocardiography and during intraoperative revision of the mitral valve, the prolapsed part of the leaflet is detected (most often this is the P2 portion - PM). Its quadriangular resection is performed along with elongated or torn chords. The resulting gap in the ring is closed with 1 or 2 seams on spacers. Ring plication is the most important technical point of the operation, since it should not only reliably ensure the approximation of the resected parts of the valve, but also not lead to deformation of the a.circumflexa. When tying ring plicating sutures, care must be taken to ensure that the edges of the sash are not overly stretched. The sash is sewn with a continuous seam using 5\0 thread. The mitral ring after quadriangular resection is necessarily strengthened with a hard or soft corrective ring.
Quadriangular resection of the posterior mitral valve leaflet Sliding resection of the posterior mitral valve leaflet was proposed by A. Carpentier to prevent left ventricular outflow tract obstruction syndrome caused by anterior systolic movement of the anterior mitral valve leaflet. This syndrome develops in 5-10% of patients after quadriangular resection of the posterior leaflet. It is caused by the excess volume of tissue in the wing sails. After resection of the posterior leaflet and implantation of the ring, the cooptation line moves forward, as a result of which the long anterior leaflet narrows the outflow tract from the left ventricle. More often, the syndrome develops after implantation of rigid correction rings. Left ventricular outflow tract obstruction syndrome is provoked by hypovolemia, vasodilation and the use of inotropic drugs. In uncomplicated cases, volume loading, increased afterload, and withdrawal of inotropes are sufficient to reduce or eliminate the hemodynamic consequences of this syndrome, which undergoes regression over time. The best strategy in patients with a potential development of left ventricular obstruction syndrome is to supplement quadriangular resection with a sliding resection of the posterior leaflet. In patients with excess leaflet tissue (posterior leaflet height greater than 1.5 cm), the goal of performing a sliding resection of the posterior leaflet is to reduce its height in order to move the leaflet cooptation line posteriorly. After quadriangular resection, the base of the posterior leaflet is separated from the ring at a distance of 1.5-2 cm on both sides of the resection site. Plicating sutures are placed on the mitral valve annulus, after which the leaflet is sutured to the reduced posterior part of the mitral valve annulus with 4/0 suture. The operation is complemented by implantation of a corrective ring. This procedure virtually eliminates the risk of left ventricular outflow tract obstruction syndrome in patients with degenerative mitral valve disease.
Technique for performing sliding resection of the posterior leaflet. 1 - the arrow indicates the location of obstruction of the left ventricular outflow tract; 2,3,4 - stages of the operation In Barlow's disease, bullous deformity and prolapse of not only the posterior but also the anterior leaflet of the mitral valve often develop. In this situation, simultaneously with quadriangular resection of the posterior leaflet, a triangular resection of the anterior leaflet of the mitral valve is performed, followed by suturing the edges with a continuous 5\0 suture. An integral element of the operation is strengthening the created structure with a soft or hard ring.
Resection of the anterior (triangular) and posterior (quadriangular) mitral valve leaflets In patients with mitral annulus calcification, decalcification is necessary to facilitate implantation of a corrective ring. To facilitate debridement, the posterior leaflet can be separated from the ring as in a sliding resection. After removal of calcifications when there is a threat of formation of a dissecting aneurysm of the left ventricle, the area where debridement was performed is covered with a pericardial patch, to which the bases of the mitral valve leaflets are sewn.
Operations on chordae and papillary muscles of the mitral valve
Surgeries on the chordae and papillary muscles of the mitral valve are used, as a rule, for prolapse of the anterior leaflet. The most commonly used types of operations are shortening, translocation and creation of artificial chords. Methods for shortening the chordae were first proposed by A. Carpentier for the correction of prolapse of the anterior leaflet of the mitral valve. Pathologically elongated chords are shortened by tucking them into the previously dissected papillary muscle, or by fixing the excess part of the chords to the edge of the anterior leaflet of the mitral valve. The durability of these methods is questionable, since in the long term there is a possibility of rupture of shortened chords.
Technique for shortening chords Translocation of chords involves moving the chords of the posterior valve that are normal in length to the prolapsing area of the anterior valve. To do this, a quadriangular resection of the posterior part and fixation to the prolapsed part of the anterior mitral valve leaflet is performed. The advantage for this procedure is that precise measurement of the length of the translocated chordae is unnecessary, since they always have a natural length to ensure normal co-option of the valves. The defect in the posterior leaflet is restored using the method described above.
Technique for translocation of posterior chords to the anterior mitral valve leaflet The creation of artificial chords is also used to correct prolapse of the anterior mitral valve leaflet. For this purpose, a thread made of polytetrafluoroethylene (4\0-5\0) is used, which has sufficient strength to ensure acceptable durability. The neochordae pass through the head of the papillary muscle and the free edge of the anterior leaflet of the mitral valve. The length is carefully measured to create a good co-option of the valves.
Creation of artificial chords
Heart valve reconstruction surgery. Memo to the patient
Heart valve repair (reconstruction) surgery is a common procedure performed to restore the health of people suffering from insufficiency or narrowing of the heart valves. It is usually performed on patients who have not been helped by drug therapy or whose condition has worsened and requires surgery for life-saving reasons.
What is heart valve disease?
Humans have four heart valves. Each, individually or in combination, may allow blood to flow backwards (insufficiency) or be narrowed and not allow enough blood to flow through (stenosis). If this defect arose during life, then it is acquired, and if before birth (it does not matter when after birth it was discovered), then we are talking about a congenital defect. Acquired defects often arise as a consequence of rheumatism. The bicuspid aortic valve (occurs in 1-2% of the population; it is usually tricuspid) wears out faster and calcifies at 50–60 years of age. Age-related valve calcification (usually aortic or mitral) or valve insufficiency is also often observed.
What is an operation?
In most cases, with mitral valve insufficiency and in some cases with aortic valve insufficiency, valve repair (reconstruction) can be performed; in most cases, with stenosis, valve replacement is performed. The surgeon has mechanical and biological valves at his disposal. When implanting a mechanical valve, which works throughout life without replacement, lifelong blood thinning with a special medication is necessary, while a biological valve does not require additional medications, but is subject to degeneration (destruction), which occurs after 10–20 years, depending on the age of the patient at the time of surgery. In this case, a repeat operation to replace the valve is required.
Why is the operation performed?
The purpose of valve surgery is to normalize blood flow to the heart and avoid additional stress on the heart. The main strategic goal for surgeons is to preserve their own valve, if possible.
This operation reduces the need for medications and improves physical endurance, duration and quality of life.
When does hospitalization occur?
Usually the patient is hospitalized one day before surgery. This is quite enough for a full examination before surgery. At the same time, you will receive instructions on how to clear mucus from your lungs, you will be taught different coughing techniques and deep breathing exercises. You will be able to meet the surgeon, cardiologist and anesthesiologist who will care for you during and after surgery.
Is it normal to feel fear and anxiety before surgery?
This is a completely normal condition. Your anxiety will decrease if you realize the necessity and timeliness of this operation. Talk to doctors, ask all your questions. If necessary, they will give you a mild sedative.
What happens the day before surgery?
The day before the operation, the surgeon will visit you to discuss with you the details of the upcoming operation and answer all your questions. The anesthesiologist will examine you and tell you how vital body functions will be maintained during the operation. He will also ask you questions about your health, previous surgeries, and your sensitivity to certain medications that may be used during surgery. After a light lunch, the nurse will carry out preparatory procedures, shave you and give you a laxative.
What happens on the day of surgery?
Before you are taken to the operating room, give your personal items (glasses, dentures, watches, jewelry, and contact lenses) to a family member or nurse. About an hour before surgery, you will be given medication that will significantly reduce anxiety and make you feel drowsy. Once you are in the operating room, the anesthesiologist will administer anesthetic drugs to help you sleep soundly and not feel pain during the operation.
What happens immediately after surgery?
When the operation is over, you will be transferred to the intensive care unit. There you will wake up. It is likely that when you wake up, you will not immediately be able to move your arms and legs. It is possible that the uncomplicated course of the operation and good condition immediately after it will allow the doctors to wake you up in the operating room. The first time after waking up, you will not feel your limbs and are unlikely to have control over their movements. This is nothing unusual; it is a normal consequence of anesthesia. After a short period of time, sensitivity and coordination of movements will be restored.
How long does the operation last?
The operation usually lasts from 3 to 6 hours. The duration of the operation depends on its complexity and the individual characteristics of the patient. Therefore, it is impossible to say in advance exactly how long this or that operation will last. Naturally, the more valves that need to be operated on, the longer the operation takes.
Where will the cuts be made?
The incision to access the heart will be made in the middle of the chest, i.e. it will pass along the midline of the sternum. Sometimes surgery on the mitral or tricuspid valve is performed through the right lateral approach.
Why will there be tubes and wires attached to the body?
Wires and tubes will be attached to various parts of your body to help you recover quickly and easily from surgery. Small tubes (called catheters) will be inserted into blood vessels in your arms, neck or thigh. Catheters are used for intravenous administration of medications, fluids, drawing blood for analysis, and continuous monitoring of blood pressure. Their placement and use will not cause you any pain. In addition to catheters, one or more tubes will be inserted into your chest cavity. They will help suck out the fluid that accumulates there after surgery.
Electrodes, attached at one end to a monitor at your bedside and the other to your body, will help medical staff monitor the rhythm and frequency of your heart using ECG data. In addition, thin wires may be attached to the lower part of the chest, which will stimulate the heart if necessary. Finally, when you wake up from surgery, you will have a special breathing (endotracheal) tube in your mouth. It will not cause pain, but you will not be able to talk.
The nurse will show you how you can reach out to others if you need to. When you can breathe on your own, the breathing tube will be removed. This usually happens within the first 24 hours after surgery. It is possible that the breathing tube will be removed in the operating room after you wake up, which will make it easier and shorten the period of your stay in the intensive care unit.
Is there anything unusual in the intensive care unit?
There is no doubt that the environment in the intensive care unit will seem a little unusual to you. Firstly, it is not so easy to keep track of time in a room in which the lights are constantly on, and the staff are always busy with some kind of activity. Secondly, trace effects from the drugs administered at the time of the operation, which provided full anesthesia, will remain in your body. You cannot discount the state of euphoria caused by the realization that such a difficult operation is already behind you. Under these conditions, your feelings can deceive you.
You may feel disoriented and confused. Feelings of disorientation may be exacerbated by the effects of pain medications. That is why it is likely that your hands will be fixed for some time so that you do not inadvertently harm the process of your postoperative rehabilitation. The feeling of confusion and disorientation that you will experience will be temporary.
Nothing serious will happen, all problems will be resolved within one or two days, after which you will be transferred to a calmer ward. As soon as you can rest normally, your clarity of thoughts will be restored, and the alternation of sleep and wakefulness will become normal again.
Is it normal to have a fever?
All patients have a fever after surgery - this is completely normal. Sometimes, due to the increase in temperature, you will sweat profusely at night or even during the day. The fever may persist for three or four days after surgery.
What can be done to speed up recovery?
In the early postoperative period, you will be required to strictly follow a number of recommendations. Firstly, you must immediately notify the nurse on duty of any changes in your health for the worse. Secondly, you must, independently or with the help of your caregivers, maintain clear control of the fluid you consume and excrete, making notes that are necessary for your treating doctor. Thirdly, you will need some effort and constant exercises with a special apparatus aimed at restoring normal breathing and preventing postoperative pneumonia.
To enhance the effect of breathing exercises, you will be recommended to exercise with the Triflow apparatus every hour. In addition, to stimulate coughing, the medical staff will make massaging movements over the surface of your lungs with elements of tapping. This technique creates internal vibration, which enhances secretion in the lungs and makes coughing easier. Many patients are afraid to cough after surgery, believing that it will harm them or slow down the healing of the wound.
There is no such danger; on the contrary, coughing is very important for your rehabilitation after surgery. Some patients find it easier to cough if they press the palms of their hands or a special roller to their chest. It is necessary to consult with your surgeon about the timing when you can lie on your side.
When can you start eating?
You will be able to swallow liquid within an hour after the breathing tube is removed from your throat. It is difficult to predict how quickly after this you can switch to pureed food, and then to a normal diet: this happens differently in all patients and depends on individual characteristics - usually this happens on the first or second day after surgery. You can get the most complete recommendations from your attending physician.
What type of activity is usually prescribed for patients?
In each specific case, the level of recommended activity will be individual. On the second or third day after the operation, you will only be allowed to sit on a chair or walk around the room. Later you will be allowed to leave the room. As the day of discharge approaches, you will be advised to take the stairs or take long walks along the corridor. Immediately after the operation, you will not have the strength to wash yourself, but after one and a half to two weeks, patients are allowed to take a shower and wash their hair.
What is the best position to be in bed?
At first you need to lie on your back. But if you lie motionless on your back for a long time, secretions may accumulate in your lungs, so already on the first day after the operation you will be seated on the edge of the bed several times, and on the second day in a chair in the morning and evening. Further activity depends on your condition, and on the third day you will be allowed to go to the toilet.
Will I be in pain after surgery?
Most patients complain of discomfort, but you can avoid severe pain with the help of modern painkillers. Unpleasant sensations are caused by the incision and muscle pain. It will be easier for you if you choose a comfortable position for yourself and are persistent in activating your state. Pain after surgery is not a necessary condition and should in no way interfere with your activity and recovery. But if you feel severe pain, tell your doctor or nursing staff and you will be given adequate pain relief.
How will the wound heal?
Shortly after surgery, the bandage will be removed from the incision on your chest. The air will promote drying and healing of the postoperative wound. First, your stitches will be washed with antiseptic solutions and bandages will be applied. Somewhere between 10 and 12 days, if healing is successful, the sutures will be removed, and the safety electrode will also be removed.
Later, you can gently wash the incision area with soap and water. We should not forget that full fusion of the sternum will be achieved in a few months, so you will need to discuss with your doctor when you can increase the load on the shoulder girdle.
How long will I be in the hospital?
Typically, after surgery to replace heart valves, patients spend two to three weeks in the clinic. But the length of your stay may vary. As a rule, this is associated with the prevention of concomitant diseases, and since this operation will require great effort from the entire patient’s body, this can provoke an exacerbation of chronic diseases. Gradually you will notice an improvement in your general condition and a surge of strength.
How will I feel when I leave the hospital?
Quite often, patients feel fear and confusion upon discharge. Sometimes this is because they are afraid to leave the hospital where they felt safe under the care of experienced doctors. They think that returning home is risky for them. You must remember that the doctor will not discharge you from the clinic until he is sure that your condition has stabilized and that further recovery will take place at home or in a sanatorium.
Will I have problems traveling home?
Typically, patients are taken home by their relatives. If you have to travel by bus, train or plane, inform your doctor, and he will give you full recommendations for each of these cases.
Do I need a special diet?
Your doctor will explain to you how to eat to reduce your risk of developing heart and vascular diseases. It is very important to reduce the amount of salt and saturated fats you consume, which are found most abundantly in animal fats. Do not think that after undergoing surgery you will not have any heart problems. Unless you make significant changes to your diet and lifestyle (quitting smoking, doing recreational exercises), your risk of developing heart disease will remain very high. In addition to following certain rules when choosing food, watch your weight. Moderation and common sense are what should be used when choosing food and drink.
What about smoking?
You can't smoke. Over the past decade, convincing material has accumulated indicating the harm caused by smoking to the heart, lungs and other organs. Smoking is the most easily avoided cause of death. It should be remembered that smoking can cause death not only from heart disease. but also from cancer. Even the healthiest people are not recommended to smoke. Those at risk of coronary artery disease have even fewer reasons to reach for a cigarette. If you smoke – QUIT!!!
How do patients feel when they return home?
It is normal that you will feel weak after discharge. Although you may attribute this weakness to heart surgery or heart disease, in reality it's all about weakness in your overused muscles, especially the large ones. It is known that if you put even a young man to bed for a week, he will lose approximately 15% of his muscle strength.
It is therefore not surprising that an older patient who has been in the hospital for two weeks or more quickly becomes tired and weak when he returns home and tries to resume normal activities. The best way to restore muscle strength is through exercise. Walking is especially effective after surgery, but be careful not to overdo it. The main criterion for dosed loads is the pulse rate; it should not exceed 120 beats per minute during exercise in the initial period.
If for some reason your heart rate exceeds this number, you should change the pace, sit down and give your body a break. In addition to the purely physical impact, returning home can also affect you psychologically. Patients often complain of depression. These sensations may be caused by emotional release after surgery. Patients sometimes feel that their recovery is going too slowly. They may feel sad and feel like time has stopped. If you feel like you are becoming depressed, it is best to discuss this condition with your spouse, relatives, close friends, a psychologist or a doctor.
What medications should I take?
You should only take medications that your doctor prescribes. Do not take the same medications you took before surgery unless prescribed. Do not take over-the-counter medications without your doctor's approval. If you have a mechanical valve implanted, you will need to take blood thinning medication for the rest of your life.
In addition, you will regularly need to monitor your blood clotting (INR) using a special device that can be purchased in Berlin. You need to learn how to use it before leaving home. You can obtain more detailed information from your attending physician. If you are taking a blood thinning medication (warfarin or Coumadin), elective surgery should be accompanied by a switch to heparin a week before surgery. 10 days after surgery, you can start taking your blood thinning medication again.
Please remember to take prophylactic antibiotics during invasive examinations, dental visits or surgeries to prevent endocarditis.
In what cases do I need to see a doctor?
Contact your doctor if you notice signs of infection, local or general (redness of the surgical scar, discharge, fever, chills), increased fatigue, shortness of breath, swelling, excess weight gain, changes in heart rate, or any other signs or symptoms. that seem dangerous to you.
Will I be able to return to work soon?
Patients who performed sedentary work can resume it on average six weeks after discharge. Those who do hard physical work have to wait longer.
How should I behave at home?
You must adhere to the following rules:
- Get up in the morning at your usual time.
- Swim or shower as needed.
- Always change into different clothes, do not walk around the house all day in night clothes. You should think of yourself as a healthy and active person, not as a seriously ill person.
- After periods of activity, after breakfast and lunch, you should lie down and rest. Rest periods after increased activity are very beneficial, so after taking a walk in the morning (a few blocks from home), come back and get some sleep.
Walking is especially beneficial for you, as it will speed up your recovery. Apart from walking, you should have no problems doing housework. You can go to the theater, restaurant, shops, visit friends, drive a car and climb stairs. In some cases, your doctor may prescribe a more rigorous gradual progression schedule as part of your overall rehabilitation process. Following this program, a few weeks after the operation you will be able to walk 2 - 3 km per day.
Usually these walks require you to go outside, but if it's very cold or too hot, try getting the required miles indoors. Extreme environmental temperatures cause the body to expend more effort to do the same job. It would be unwise to overload your body with long walks if the weather is very cold or hot.
When can I be sexually active?
You will be able to resume sexual activity whenever you want. But it should be borne in mind that full fusion of the sternum will be achieved in 3 - 4 months, therefore, during sex, positions that minimize the load on the sternum are preferred (for example, a partner on top). If any problems arise, you should consult a doctor.
When will I be able to drive the car?
You will be able to drive a car as soon as your physical condition allows you to do so. It is usually best to wait a few weeks after discharge. But if driving a car is your profession, then discuss with your doctor the timing of your recovery period, since in the process of driving a car, the sternum experiences certain loads when turning the steering wheel.
When should I see my doctor again?
How often you visit your doctor after surgery depends on your condition and your doctor's recommendations. Typically, patients are given a date for follow-up consultation upon discharge. When you return home from the clinic, you will need to arrange a visit to your family doctor or local cardiologist at your place of residence.
Do I need to change my lifestyle?
As a rule, surgery allows patients to return to a normal lifestyle. The purpose of the operation is to return to work or, if you are already retired, to live a full life. After surgery, you may want to change something in your lifestyle. It is wise to quit smoking to reduce your risk of having a heart attack. Quit smoking, constantly monitor your blood pressure, watch your weight, reduce your intake of salt and saturated fats - all this will help you maintain your health for a long time and avoid new problems.
Some doctors recommend that their patients work for a strictly limited time. If you constantly think that you may not have enough time to complete your work, you will constantly find yourself in situations that contribute to stress and increased irritability, which can lead to a heart attack.
Sometimes you can reduce the feeling of time pressure by consciously slowing down the pace of your work or trying not to make a big deal about the problem. If you realize that a particular situation may cause you irritation, try to avoid it or, if possible, allay your fears by discussing the problem with people who are distantly related to it.
What does the future hold for me?
As you recover from surgery, you will be able to fully appreciate its beneficial effects. You will see that you need less and less medications, maybe you will be able to stop taking them altogether, and physical activity will tire you less and less. Your quality of life will undoubtedly improve.
The memo partially uses materials from Vitaly Milekhin , Moscow.
print version
An employee of the Center, Doctor of Medicine, Private Associate Professor, Senior Cardiac Surgeon Evgeniy Potapov, will promptly answer your questions and discuss your treatment plan with the director.
To get a consultation, you can call: +49 30 45932065 or +49 1621034983 or send a request by filling out the form .
Papillary muscle translocation
In ischemic mitral regurgitation, regurgitation is caused by displacement of the posterior papillary muscle towards the apex of the left ventricle, which impairs co-option of the mitral valve leaflets. In this regard, moving the posterior papillary muscle closer to the mitral valve annulus reduces posterior leaflet tension and improves cooptation. The technique for performing this procedure involves placing a traction suture through the papillary muscle and fixing it to the posterior part of the mitral valve annulus.
Posterior papillary muscle translocation technique
Restoring mobility of valves and chords
Limitation of the movement of the leaflets is caused by fibrous thickening of the subvalvular apparatus, the leaflets themselves, commissure fusion and calcification. In most patients, with pronounced changes in these structures, valve replacement is necessary, but in some patients with limited calcification of the leaflets and fibrosis of the subvalvular structures, open commissurotomy can be performed. The dissection of fused leaflets along the commissures should end 2 mm from the annulus, since a more extensive commissurotomy can lead to mitral insufficiency. Additionally, to increase the mobility of the valves, fenestration of the primary chordae and papillary muscles is performed, as well as resection of the secondary chordae.
Fenestration of the primary chordae and papillary muscles Mobilization of the subvalvular structures significantly increases leaflet mobility and the effective orifice area of the mitral valve. If a hydraulic test after completion of the manipulation reveals regurgitation, additional implantation of a corrective ring may be necessary.
Results of mitral plasty operations
Using plastic methods, 90% of valves with degenerative changes can be restored. In-hospital mortality after isolated mitral valve repair does not exceed 1%, and long-term survival is comparable to the general population. Provided that corrective rings are used and residual regurgitation after correction is no more than grade I, the 10-year freedom from reoperation is 93-97%. The results of plastic surgery on the mitral valve in cases of rheumatic disease are somewhat worse. The 10-year freedom from reoperation is 72%. However, in appropriately selected patients with pure mitral stenosis, commissurotomy provides a good effect - 91% of patients do not require reoperation within 10 years. In patients with mixed lesions, valve morphology usually limits the ability to achieve good results and half of them require reoperation within 14 years. Hospital mortality after plastic correction of ischemic mitral regurgitation is 3-6%, and 5-year survival is only 58%. Patients with papillary muscle rupture have a better long-term prognosis, likely due to better preservation of left ventricular function. For most patients with ischemic mitral regurgitation, mitral valve repair is preferable. Increasing the life expectancy of patients with ischemic cardiomyopathy depends not only on the correction of mitral regurgitation, but also on the effectiveness of revascularization and surgical remodeling of the left ventricle. 30-50% of patients undergoing mitral valve surgery have atrial fibrillation. Considering that persistence of atrial fibrillation for more than one year after mitral valve repair requires constant use of indirect anticoagulants, which reduces the quality of life, simultaneous Cox-Maze III procedure is indicated for such patients. The use of microwave, ultrasound or laser energy for this purpose significantly reduces the operation time and leads to success in 70-80% of patients.
Mitral prosthetics in Belarus - European quality at a reasonable price
Professor, Doctor of Medical Sciences Yu.P. Ostrovsky
Recovery after plastic surgery
Heart surgery requires gradual rehabilitation. In the first month after plastic surgery, it is recommended to take very good care of the entire body: give up bad habits, follow the prescribed diet, and avoid stress.
During this period, you need to avoid foods that are too salty, fried, or fatty. Also, drinking plenty of water additionally puts a strain on the cardiovascular system; you should try to drink no more than 1.5 liters of water per day. Alcohol is completely excluded.
It is imperative to undergo routine examinations. The doctor will evaluate the effectiveness of the plastic surgery and the patient’s condition and adjust the treatment. If your health worsens in the postoperative period, this is a reason to call an ambulance or come to an unscheduled appointment. Physical activity should be reduced, sometimes go for leisurely walks, breathe fresh air.
In most cases, such an operation ends successfully for the patient. Over time, all functions of the heart are restored, and the person can return to an active lifestyle, which is confirmed by reviews.
After the first 4 weeks, an examination is scheduled to ensure the success of the procedure. To do this, you need to undergo an ultrasound of the heart, cardiography, urine and blood tests. In the first year after plastic surgery, the patient visits the doctor every month, then twice a year, if there are no complaints.