Abdominal aortic aneurysm is a pathological change in the tissue of the aorta, leading to its expansion. Because of this, proper blood circulation is disrupted and other complications appear, including those that can lead to death. Therefore, when an aneurysm reaches a dangerous size, an operation is indicated to replace the affected area of the aorta with a prosthesis . This is a serious surgical intervention that requires a rehabilitation period under the close supervision of doctors and patient compliance with important recommendations.
Why is an aneurysm dangerous?
An aortic aneurysm may not manifest itself in any way at the initial stages of development. Sometimes there may be pain that is quite tolerable. However, this is a ticking time bomb. The main dangers of an aneurysm:
Under certain conditions, the thinned wall of the aorta can rupture. This is a very serious complication. Without emergency surgery, a person dies from acute blood loss. Even an urgent blood transfusion will not help here (you cannot fill a leaky vessel).
Break.- Delamination. The wall of the aorta is multilayered; when one of the membranes is torn, the blood flow delaminates the wall. This process is accompanied by very severe pain, poor circulation, and shock.
- Thrombosis in an aneurysm. In the area of protrusion of the aortic wall, turbulence in the blood flow occurs, and the speed of blood flow slows down here. Blood clots begin to form on the altered wall, gradually increasing in size. Blood clots are dangerous due to rupture and thromboembolism of the main and peripheral arteries.
- Pressure on neighboring organs. Depending on the location, a bulging and enlarged aorta can compress the organs of the mediastinum, bronchi, abdominal organs, and compress vascular bundles and nerve trunks.
Video: the occurrence of an aortic aneurysm
Recovery after bypass surgery
Recovery after coronary artery bypass surgery should be carried out under the supervision of a specialist. This is important not only because the patient needs to quickly normalize his condition, but also because CABG eliminates only the consequences of cardiac dysfunction. The underlying cause, for example, atherosclerotic vascular lesions, remains. Coronary artery bypass surgery is a serious trauma for the body; it leads to many responses that can become pathological.
The patient and the specialist face a number of tasks, the success of which determines the effectiveness of the operation.
These include:
- prevent the development of complications;
- resume heart function in full;
- stimulation of regenerative processes in damaged areas;
- slow down the progression of atherosclerotic and other pathological processes in the myocardium;
- adapt the patient to psychological and physical stress;
- to form skills that are relevant for new living conditions: household, social, labor.
It is considered that the set goals have been achieved if the patient returns to a lifestyle relevant to a healthy person.
Recovery after bypass surgery includes the following areas:
- patient care in the first days;
- drug therapy;
- systematic monitoring of condition dynamics;
- attitude towards a healthy lifestyle and giving up bad habits;
- physical rehabilitation;
- breathing exercises;
- mental rehabilitation;
- physiotherapeutic procedures and sanatorium-resort treatment.
After the operation, the patient is transferred to the intensive care unit, where he is under the control of devices and medical personnel. At this time, a number of examinations are carried out:
- general blood analysis;
- X-ray;
- electrocardiography.
Recovery after bypass surgery during this period requires the patient to stay warm, so he is wrapped in a warm blanket. On the first day, the temperature may rise - this is a variant of the norm and a manifestation of the body’s protective functions. Also characteristic of the recovery state is increased sweating.
The patient spends 1-1.5 weeks in the hospital. A week after CABG, the sutures are removed from the chest and leg, if the vein was taken from there. It takes about 6 weeks for the sternum to heal. During this period, high physical activity is prohibited. Using a special bandage will help speed up recovery after bypass surgery. Antibacterial drugs, painkillers and sedatives are prescribed.
It is necessary to perform breathing exercises - a specialist will teach them before the operation. The easiest way to develop your lungs is to inflate balloons. However, there are special techniques that are used for recovery after coronary artery bypass surgery.
To prevent congestion, vibration massage is performed over the lung area with gentle tapping movements.
Despite bed rest, it is necessary to move - change body position. Once the doctor gives permission, you can turn on your side. Physical activity is increased gradually: first, you are allowed to sit on a chair, then move around the ward, along the corridor. After this, the patient tries to walk up the stairs. Before discharge, he takes walks in the fresh air.
Wearing a bandage and compression stockings will speed up recovery after cardiac bypass surgery. You can buy them at an orthopedic store.
Water procedures are not prohibited, but washing is only allowed in the shower, and so that a direct stream of water does not fall on the wound area. Swimming and visiting the pool are allowed only after the sternum has healed.
Drug treatment is based on taking drugs such as:
- antiplatelet agents;
- ACE inhibitors;
- beta blockers;
- statins.
Antiplatelet agents are needed to thin the blood. These are medications that patients with coronary artery disease must take for life. The most common drug is aspirin.
Beta blockers reduce the load on the heart and normalize heart rate and blood pressure. Their use is relevant for hypertension, tachyarrhythmia, and heart failure.
Statins are characterized by an anti-inflammatory effect.
Physical recovery after bypass surgery begins almost immediately. The very next day the patient sits down, and on the second day he gets out of bed. Gymnastics and massage are necessary.
Recommended types of sports activity are walking, walking in the fresh air, and subsequently swimming. Experts recommend using cardio equipment, cycling, and walking up the stairs.
The recovery period after bypass surgery does not prohibit sexual activity. However, you should choose positions that will not put pressure on the chest. But you will have to give up driving a car for a month. Doctors do not advise traveling during the first few months. If there is a need to leave, then before departure it is mandatory to undergo a cardiological examination and consult a specialist.
Mental recovery after bypass surgery is an integral part of rehabilitation. Psychoemotional disorders are often a consequence of complex surgery. Patients experience increased anxiety and doubts about the possibility of improving their well-being. Psychosomatics works in such a way that this uncertainty flows into a deterioration in physical condition: headaches and dizziness appear. To avoid such situations, it is necessary to work with a psychotherapist. New attitudes are formed, and if necessary, drug treatment is used - sedatives. Physiotherapy and massage are also effective.
Smoking after CABG is strictly prohibited. Nicotine leads to increased blood clotting, leads to vasospasm, impairs the transport of oxygen to tissues and the conduction of impulses in the myocardium.
Recovery after heart bypass surgery includes physiotherapy: electrosleep, magnetic therapy, laser, electrophoresis.
It is highly recommended, if possible, to undergo recovery after bypass surgery in a specialized sanatorium. The advantages in this case are numerous: constant monitoring combined with a well-designed diet and the implementation of dosed exercises under the supervision of a specialist.
The patient should pay great attention to changes in his well-being. You should contact a specialist immediately in the following cases:
- changes indicating the development of an inflammatory process in the suture area: hyperemia, local increase in temperature, pain, discharge from the wound;
- general weakness;
- difficulty breathing;
- weight gain, swelling;
- tachycardia;
- chest pain.
Recovery after heart bypass surgery, both in the hospital and at home, should be under the supervision of a doctor, as there is a risk of complications. Possible consequences include:
- arrhythmias;
- bleeding;
- heart attack;
- stroke;
- thrombosis;
- penetration of infection into the wound;
- renal failure;
- chronic pain in the incision area.
One of the key factors in both primary and secondary prevention of heart pathologies is proper nutrition. Recovery after bypass surgery involves following a strict diet.
Considering the danger of developing atherosclerosis and ischemic heart disease from dietary factors, it is necessary to highlight the following:
- high calorie foods leading to obesity;
- lack of polyunsaturated acids, which are needed to normalize cholesterol metabolism;
- foods rich in cholesterol;
- fiber deficiency;
- excessive salt intake;
- excess animal proteins that impair vascular permeability and negatively affect lipid metabolism and blood clotting;
- deficiency of substances necessary for the body: magnesium, potassium, zinc, iodine, vitamins PP, A, ascorbic acid, B6.
First of all, it is necessary to reduce the calorie intake. It should be 2400-2600 kcal.
The diet should include 70-90 g of protein, 80 g of fat, 300-350 g of carbohydrates.
5-6 small meals per day are recommended. Food should be at normal temperature and not over-salted. The permitted volume of liquid is 1.2-1.5 liters per day.
Experts advise including the following dishes on the menu:
- soups based on vegetable broth with well-cooked cereals;
- lean meats and poultry;
- seafood;
- dairy products;
- whole grains;
- vegetables and fruits;
- fresh juices;
- almonds and walnuts.
Patients with diabetes are at high risk of developing complications. These people are at risk, which requires special attention from medical personnel. It is important to provide the body with proper rest - sleep at least 8 hours, and avoid emotional turmoil.
The prognosis for patients after surgery is favorable - life expectancy can be increased by 10-15 years.
After cardiac bypass surgery has been performed, recovery must proceed in strict accordance with these recommendations; you cannot rely only on the operation performed. The professionalism of the doctor also plays a big role.
Aneurysm is an insidious disease that is rarely accompanied by clinical signs and is usually discovered by chance.
This is a pathology in which the wall of the artery bulges due to stretching or thinning. In this case, the lumen of the vessel expands more than 2 times. Theoretically, this can occur in any artery, but the largest ones are most often affected.
Its complete removal can only be done surgically. Below we will discuss the indications for surgery and modern methods of treating pathology.
Tactics for identifying an aortic aneurysm
Of course, an aneurysm is an anatomical defect that cannot be eliminated by any medications. If an aortic aneurysm is detected, the patient is referred for consultation with a vascular surgeon.
But this does not mean that all aneurysms are immediately taken to the operating table. This is mainly due to the fact that operations for aortic aneurysms are quite complex, are carried out only in specialized departments of cardiovascular surgery, require high-tech costs, and are also associated with a fairly high risk of postoperative complications. Patients with an aortic aneurysm usually have a lot of concomitant chronic diseases, which only aggravate this risk.
Therefore, uncomplicated small aneurysms are managed conservatively. The majority of such patients are monitored dynamically, they are given recommendations for the prevention of complications and progression of aortic protrusion.
In what cases is surgery suggested?
- Aneurysms of the ascending, thoracic aorta, as well as the abdominal section below the level of origin of the renal arteries, measuring more than 4.5 cm in women and more than 5 cm in men.
- Aneurysms of the thoracoabdominal aorta, as well as the abdominal aorta above the origin of the nephric vessels, are more than 5.5 cm in diameter.
- An increase in the size of the aneurysm by more than 6 mm per year.
- Multichamber aneurysm.
- Saccular aneurysm with a narrow neck.
- An eccentrically located thrombus in an aneurysm.
- Recorded thromboembolism.
- Symptomatic aneurysms (accompanied by pain or compression of neighboring organs), regardless of their diameter.
In cases of rupture or dissection of an aneurysm, surgery is performed immediately for health reasons.
Diagnostics
Very often patients do not make any complaints. But if symptoms appear, they are nonspecific. The most common symptoms include pain in the abdomen, back, or chest area. Patients describe this pain in different ways: some feel moderate to severe pain or tenderness in the middle or upper abdomen or lower back, while others feel the aneurysm itself as a beating and pulsating mass in the abdominal cavity. But, as noted, many may not experience any symptoms. Sometimes abdominal aortic aneurysm
may be detected during a routine physical examination. When palpating the abdomen, the doctor may detect a bulge or pulsation in the abdominal cavity. But most often, an aneurysm is detected during medical tests such as an abdominal ultrasound (ultrasound) or computed tomography (CT) scan. The size and location of the abdominal aortic aneurysm, as well as the general condition of the patient, help to choose the right treatment method. If the aneurysm is small, your doctor may recommend surveillance (regular examinations to monitor its size). A large aneurysm or a rapidly enlarging aneurysm has a high chance of rupture and requires treatment.
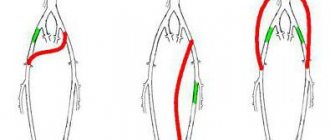
Principle of operations for aortic aneurysm
The basic principle of operations for aortic aneurysm is the replacement of the area of the aorta affected by the aneurysm with an artificial prosthesis. This can be achieved either by removing such a section and suturing the aorta with an end-to-end prosthesis (this is the principle of open operations), or by placing an artificial shunt inside the vessel without removing the aneurysmal extension (this is the principle of intravascular minimally invasive operations).
Less commonly practiced are operations for resection of a saccular aneurysm with suturing of the aortic walls without installing a shunt, as well as palliative operations (for example, wrapping the aorta in synthetic tissue to prevent further expansion).
Examination and preparation before surgery
If an aortic aneurysm is suspected, the patient is first referred for an ultrasound scan (an aneurysm is often discovered by chance during an ultrasound scan of the retroperitoneum for other reasons or during a screening examination).
Next, to confirm the diagnosis and obtain a detailed picture and dimensions, the following is carried out:
- Intravascular ultrasound examination.
- X-ray contrast angiography.
- CT angiography with contrast.
- Magnetic resonance imaging.
Surgery for an aortic aneurysm is very complicated and carries a high risk of complications. Therefore, in addition to the usual preoperative examination, it is necessary to undergo a series of functional tests, which assess the degree of insufficiency of a particular body system.
- Patients with COPD with unsatisfactory respiratory reserve require adequate selection of bronchodilators. It is strongly recommended to quit smoking 1-1.5 months before the planned operation.
- Patients with coronary heart disease should be especially well examined. When planning an open operation, it is recommended to perform coronary angiography and, if necessary, myocardial revascularization (coronary artery stenting or CABG).
- All patients with diseases of the cardiovascular system are prescribed beta blockers, antiplatelet agents, and statins at least a month before surgery. Careful selection of antihypertensive drugs is necessary to achieve maximum control of hypertension.
- If the platelet count in the blood is less than 130,000, an additional hematological examination is performed.
- When the level of creatinine in the blood increases and the glomerular filtration rate decreases, patients are referred to a nephrologist.
- The presence of hemodynamically significant stenosis of the carotid arteries is subject to correction first.
- If ulcerative and erosive changes in the mucosa are detected on FGDS, they are treated conservatively until complete healing.
- After compensating for the basic functions of the body, 10 days before the operation, all basic standard tests, chest x-rays, and examination by specialists are once again prescribed.
- 30 minutes before surgery, a single daily dose of a broad-spectrum antibiotic is administered parenterally.
What lifestyle should a patient with an abdominal aortic aneurysm lead?
Before surgery. If the aneurysm is small (up to 5 cm), and elective surgery is not planned, doctors take a wait-and-see approach and monitor the patient. The patient should visit the doctor every six months for examination; if the aneurysm grows rapidly (more than 0.5 cm per six months), he will be scheduled for surgery.
After surgery, the patient visits the doctor monthly in the first year, then every six months in the second year and then once a year.
Both before and after surgery, the patient must take medications prescribed by the doctor. It is recommended to follow the following simple steps to maintain a healthy lifestyle to prevent aneurysm growth and complications:
- Proper nutrition and excess weight loss. Fatty, fried, spicy, salty foods are excluded. Animal fats and confectionery products are limited. Fresh vegetables and fruits, cereals, dairy products, low-fat poultry, meat and fish, juices, compotes, fruit drinks are recommended. Eating 4 – 6 times a day, in small portions. It is better to cook products in steamed, boiled, pureed form.
- Reducing cholesterol levels - taking statins as prescribed by a doctor, limiting the intake of cholesterol from food.
- Controlling blood pressure levels - eliminating psycho-emotional stress, heavy physical labor, regularly taking medications that normalize blood pressure, limiting sodium in food.
- Complete cessation of smoking and alcohol. It has been proven that smoking provokes the growth of an aneurysm, and alcohol increases blood pressure, which can provoke a vascular accident.
- Elimination of significant physical activity (in the early postoperative period, complete bed rest with gradual restoration of motor activity). Sports activities are contraindicated. Walking for short distances is acceptable.
- Correction of concomitant diseases - diabetes mellitus, heart disease, liver disease, kidney disease, etc.
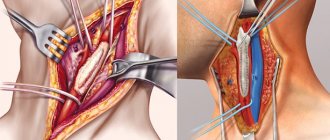
Introduction to open surgery for aortic aneurysm
Surgeries for aortic aneurysm are performed only in specialized cardiovascular centers after careful preparation of the patient, correction of his risk factors and compensation for chronic diseases.
Depending on the location of the aneurysm, appropriate wide access to it is carried out.
- For an aneurysm of the ascending aorta and aortic arch, sternotomy (incision of the sternum).
- For thoracic aneurysm - thoracotomy (incision along the intercostal spaces of the left half of the chest).
- If the lesion is localized in the thoracoabdominal aorta, thoracophrenolumbotomy is performed.
- For an aneurysm of the abdominal aorta, a median laparotomy from the xiphoid process to the pubis or retroperitoneal access (the incision is made in the lumbar region).
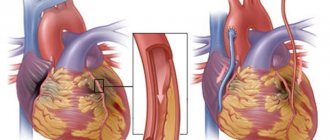
The operation is performed under general endotracheal anesthesia. When operations on the ascending aorta and arch require the use of a heart-lung machine and controlled hypothermia. It is also possible to apply temporary bypass shunts to isolate this section of the aorta from the blood circulation.
Principle of operation: the aorta is clamped with a clamp above and below the aneurysm within the unchanged wall. The area with the aneurysm is excised and anastomosis is performed with the prosthesis.
If necessary, anastomoses are created with arteries arising from the aorta at the site of the removed site.
open surgery
There are different types of prostheses. Currently, Dacron knitted and woven prostheses, as well as polytetrafluoroethylene (PTFE) prostheses, are mainly used. The long-term results of their use are comparable; the choice is determined by the surgeon’s preference. The configuration of the prosthesis can be either linear or complex (with bifurcations, with the departure of corresponding branches). Often it is necessary to manufacture an individual prosthesis according to the size and shape for a specific patient.
Reasons for development
Knowing exactly the reasons for the development of pathology, you can protect yourself. Prerequisites include:
- atherosclerosis – the formation of vascular plaques, which is accompanied by damage to the internal lining of the vessel;
- inflammation and subsequent damage to the aorta - observed in tuberculosis, syphilis, rheumatism and other diseases;
- genetic disorders - characterized by weakness of the vascular walls;
- traumatic damage to the vascular walls - blows and other closed injuries to the abdomen, back;
- rehabilitation period after surgery – they are rare and in most cases are false;
- fungal infections - develops against the background of immunodeficiency due to HIV or drug addiction, often develops against the background of fungal penetration into the blood (this provokes sepsis and other destruction of the walls of blood vessels).
The causes may not provide an accurate picture of the progression of the disease. It is much more important to study the risk factors for pathology.
Complications after open resection of aortic aneurysm
As already mentioned, open surgery carries a high risk of postoperative complications. Main complications:
- Myocardial infarction.
- Arrhythmias.
- Stroke.
- Heart failure.
- Pneumonia.
- Pulmonary embolism (PE).
- Kidney failure.
- Ischemic intestinal paresis and intestinal obstruction.
- Bleeding.
- Infectious and suppurative complications (peritonitis, mediastinitis, meningitis, suppuration of the surgical wound, sepsis).
- Deep vein thrombosis of the lower extremities.
The aortic replacement operation lasts 3-4 hours. After the operation, the patient is transferred to the intensive care unit, where he is under constant monitoring of functions for several days. Painkillers and antibiotics are prescribed. Parenteral nutrition and infusion of physiological solutions are being established. Mobilization is recommended the day after surgery. The rehabilitation period lasts up to 3 months.
Methods of implementation and possible complications
There are two ways to perform surgery. The first is an open abdominal operation, during which the doctor opens the peritoneum, removes a section of the damaged aorta with a scalpel, and instead inserts a prosthesis made of synthetic material. The patient recovers within three months. The success rate of treatment is 90%.
This technique has its pros and cons. The positive aspects include the fact that the installed prosthesis is more reliable, it “works” longer than an endoprosthesis. A patient after surgical treatment needs less careful and frequent monitoring than a patient with an endoprosthesis. This explains why open access is still successfully practiced by doctors. The negative aspects include the need to use general anesthesia (it is poorly tolerated by older people), there is a large volume of intervention, significant blood loss, and there is a need for blood transfusions.
The second method is endovascular. This is a less traumatic operation. The surgeon makes small incisions in the area where the femoral arteries are located. Their diameter is 2 cm. The components of the prosthesis are introduced into the lumen of the vessels. They are packaged in a special delivery device. “With packaging,” the diameter of the instrumentation is only 8 mm, so it easily fits through the described hollow tubes.
Carefully, in increments of 30-40 cm, the doctor pushes the prosthesis to the desired area of the aorta. Then, using endoscopic equipment, an artificial analogue is “assembled” on site. It consists of a mesh frame and thin material through which blood cannot leak. Essentially, the damaged artery is reconstructed. Its new site takes on the throughput function. This operation is well tolerated by older people. It is performed under local anesthesia. The surgeon and patient may communicate.
The postoperative period is only three to four days. The risks of complications are minimal. But the use of this method of intervention is impossible with very tortuous vessels; after the operation, the patient is under medical supervision for a long time. Repeated manipulations aimed at strengthening the walls of blood vessels often become necessary. The aorta can dilate again if the patient does not monitor blood pressure and refuses treatment for hypertension.
The risks of abdominal surgery are high. It can provoke myocardial infarction, stroke, heart and kidney failure, pneumonia, pulmonary thromboembolism, ischemic intestinal cut, bleeding, peritonitis, meningitis. Possible suppuration of the surgical wound, sepsis.
When using endovascular intervention, there is a risk of incomplete shutdown of the aneurysm sac. This situation leads to blood leakage. As a result, the aneurysm sac will continue to increase in size. This will sooner or later end in aortic rupture and death.
Endovascular interventions for aortic aneurysms
Open surgery for aortic aneurysms is a fairly proven and reliable method. It still remains the main method of surgical treatment of aneurysms (more than 80% of operations to eliminate aortic aneurysms in Russia are open interventions). However, not all patients are able to withstand it.
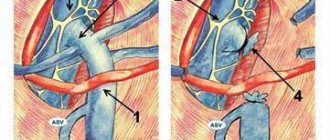
Intravascular interventions are a minimally invasive alternative treatment for aortic aneurysms. The principle of the method is that a remote delivery device is inserted through the main artery (subclavian, femoral), through which a vascular endoprosthesis is inserted - the so-called stent graft. The aneurysmal dilatation is switched off from the blood flow, and the blood flow goes along a new channel.
A stent graft is a metal frame covered with synthetic material. A stent graft is manufactured individually for each patient.
Most often, the abdominal aorta is endoprosthetized below the origin of the renal veins to the bifurcation site. The stent-graft for this section of the abdominal aorta is modular and consists of two parts. One part (prosthesis for the aortic trunk and one iliac artery) is inserted through one femoral artery, and the second part (endoprosthesis of the second iliac artery) is inserted through the femoral artery on the other side.
The operation is performed in a special X-ray operating room under X-ray control.
After delivery to the desired location, the stent-graft is released from the delivery system and installed in the required position. The structure is held in place by the elasticity of the metal frame and hooks that penetrate the aortic wall.
The main advantages of endovascular interventions:
The operation does not require general anesthesia and is performed under epidural or even local anesthesia. This makes it possible to perform operations on patients with chronic diseases for whom open surgery is contraindicated.
- The operation is non-traumatic and is performed without large incisions.
- Less severe pain syndrome.
- Reduced blood loss.
- There is no need to clamp the aorta, which eliminates ischemic complications from the heart and internal organs.
- Reducing length of hospital stay.
- Fewer postoperative complications.
However, the installation of an intravascular stent also has its disadvantages; this is mainly due to the risk of incomplete exclusion of the aneurysmal sac due to a loose fit to the aortic walls. This situation is called "leaking". As a result of the leakage, the aneurysmal dilation will still gradually increase, which can lead to its rupture.
Patients who have undergone endovascular treatment of an aneurysm should be regularly monitored for timely detection of this phenomenon.
Before surgery, patients must be informed about the possible consequences and failures of open and endovascular treatment. In addition, it is necessary to stipulate that in case of unsuccessful endoprosthetics there must be agreement to switch to the open method of surgery with all the ensuing risks.
Therefore, in the case of planning surgical treatment of aortic aneurysms, the patient’s commitment to one or another method is very important.
The five-year survival rate after surgery to remove aortic aneurysms is 65-70%.
Video: definition, diagnosis, types of operations
Symptoms
A characteristic feature of an aneurysm is that for many years it can be completely asymptomatic . This is due to the rather slow growth of the aneurysmal defect . When the bag reaches a sufficient size, dull, aching and constant pain may appear, which will be localized mainly in the lumbosacral region and abdomen. Also, an aortic defect can be palpated in the form of a tumor-like formation, over which a systolic murmur can be heard. Characterized by decreased appetite, nausea and vomiting.
When an aneurysm ruptures, the patient feels sharp pain, a drop in blood pressure occurs, and tachycardia appears.
Cost of the operation
Surgeries for aortic aneurysms are high-tech types of medical care. To perform this operation, you can obtain a quota from the regional Ministry of Health and carry it out free of charge in any cardiovascular center specializing in such operations.
However, it is necessary to reveal some nuances. First, treatment quotas are limited. You can't wait for them. Secondly, quotas do not cover the cost of aortic replacement, in particular the cost of a stent graft. The endoprosthesis, as a rule, is still paid for by the patient himself.
Prices for surgery depend on the type of intervention, the rank of the clinic, the need for artificial blood circulation and, of course, the cost of the prosthesis itself.
The surgical benefit itself for open surgery costs about 250,000 rubles. The cost of endoprosthesis replacement without taking into account the stent graft varies from 150,000 to 500,000 rubles. The cost of an endoprosthesis starts from 450,000 rubles.
Abroad, such operations cost from 7 thousand to 35 thousand dollars.
Advantages of resection
If such treatment is ignored, the person may die. Statistics show that out of 100 patients, 40 have a rupture in the first year after the onset of the disease. This means that resection can save a life and protect a person from serious complications:
- digestive tract disorder;
- intestinal ischemia;
- organic changes in the digestive system;
- portal hypertension syndrome.
to the point ↑