What is the principle of abdominal aortic aneurysm surgery and when is it indicated?
What examination is necessary before surgery for an abdominal aneurysm?
What preparation is necessary before surgery for resection of an aortic aneurysm?
How is surgery performed for abdominal aortic aneurysm?
What are the features of performing resection of an abdominal aortic aneurysm?
What happens after abdominal aortic replacement surgery?
What is the average cost of surgery to remove an abdominal aortic aneurysm?
Systematization of manifestations of aortic aneurysm
Currently, there is no unified approach to systematizing the manifestations of peritoneal aortic aneurysm. Most often, doctors and authors of medical works use the method of A. Pokrovsky and R. Ermolyuk, according to which aneurysms are divided:
- by etiology – acquired (non-inflammatory or inflammatory) and congenital;
- according to morphology - into false (traumatic origin), true and stratifying;
- by shape - diffusion and saccular;
- according to the course of the clinical process - into diseases with an uncomplicated course, complicated and dissecting;
- by type and location - on the proximal segment of the peritoneal aorta, on the infrarenal section, as well as with total damage to the entire section of the abdominal aorta.
According to medical statistics, up to 95% of aneurysms are localized in the infrarenal region.
Anesthesia during surgery
The operation can be performed under general anesthesia or under epidural anesthesia (injection in the back). General anesthesia is required for large aneurysms extending to the level of the renal arteries or higher. General anesthesia is required for access using a wide midline laparotomy. With retroperitoneal access to the aorta, epidural anesthesia can be limited. During operations for an aneurysm, cardiac activity and blood pressure must be monitored using special equipment. For anesthesia and intensive care, a catheter must be installed in the central vein (most often the subclavian). Kidney function is assessed by the amount of urine, for this purpose a catheter is inserted into the bladder. During anesthesia, the level of central venous pressure is monitored and drugs are administered to regulate the volume of circulating blood and electrolytes. If necessary, blood and plasma transfusions are performed to replace those lost during surgery. Special dispensers administer drugs that regulate blood pressure levels. During a long operation, a hemofiltration device may be connected to eliminate possible intoxication. Anesthesia during aortic surgery is very important and the comfort of surgeons and the immediate results of surgical intervention depend on its course.
Causes of development of abdominal aortic aneurysm
- atherosclerosis, in which the appearance of cholesterol plaques on the wall of the aorta gradually reduces its strength, which contributes to protrusion in one of the areas;
- congenital predisposition, transmitted through the male line, confirmed by many years of observations: the presence of an aneurysm in the father indicates a 50% chance of this disease occurring in his son;
- an inflammatory process of a chronic, sluggish nature that occurs in the aortic wall itself or in the adipose tissue that surrounds the vessel;
- traumatic damage to the wall due to trauma or injury to the abdomen, surgery or endovascular intervention.
Atherosclerotic manifestations become the cause in 85-90% of cases of the development of acquired aneurysm in the abdominal aorta. Signs of predisposition to the development of the disease are smoking, arterial hypertension and chronic pulmonary diseases.
Endovascular interventions for aortic aneurysms
Open surgery for aortic aneurysms is a fairly proven and reliable method. It still remains the main method of surgical treatment of aneurysms (more than 80% of operations to eliminate aortic aneurysms in Russia are open interventions). However, not all patients are able to withstand it.
Intravascular interventions are a minimally invasive alternative treatment for aortic aneurysms. The principle of the method is that a remote delivery device is inserted through the main artery (subclavian, femoral), through which a vascular endoprosthesis is inserted - the so-called stent graft. The aneurysmal dilatation is switched off from the blood flow, and the blood flow goes along a new channel.
A stent graft is a metal frame covered with synthetic material. A stent graft is manufactured individually for each patient.
Most often, the abdominal aorta is endoprosthetized below the origin of the renal veins to the bifurcation site. The stent-graft for this section of the abdominal aorta is modular and consists of two parts. One part (prosthesis for the aortic trunk and one iliac artery) is inserted through one femoral artery, and the second part (endoprosthesis of the second iliac artery) is inserted through the femoral artery on the other side.
The operation is performed in a special X-ray operating room under X-ray control.
After delivery to the desired location, the stent-graft is released from the delivery system and installed in the required position. The structure is held in place by the elasticity of the metal frame and hooks that penetrate the aortic wall.
The main advantages of endovascular interventions:
The operation does not require general anesthesia and is performed under epidural or even local anesthesia. This makes it possible to perform operations on patients with chronic diseases for whom open surgery is contraindicated.
- The operation is non-traumatic and is performed without large incisions.
- Less severe pain syndrome.
- Reduced blood loss.
- There is no need to clamp the aorta, which eliminates ischemic complications from the heart and internal organs.
- Reducing length of hospital stay.
- Fewer postoperative complications.
However, the installation of an intravascular stent also has its disadvantages; this is mainly due to the risk of incomplete exclusion of the aneurysmal sac due to a loose fit to the aortic walls. This situation is called "leaking". As a result of the leakage, the aneurysmal dilation will still gradually increase, which can lead to its rupture.
Patients who have undergone endovascular treatment of an aneurysm should be regularly monitored for timely detection of this phenomenon.
Before surgery, patients must be informed about the possible consequences and failures of open and endovascular treatment. In addition, it is necessary to stipulate that in case of unsuccessful endoprosthetics there must be agreement to switch to the open method of surgery with all the ensuing risks.
Therefore, in the case of planning surgical treatment of aortic aneurysms, the patient’s commitment to one or another method is very important.
The five-year survival rate after surgery to remove aortic aneurysms is 65-70%.
Video: definition, diagnosis, types of operations
Symptoms of aortic aneurysm
In approximately a quarter of cases, an abdominal aortic aneurysm develops completely asymptomatically and is discovered by chance during an ultrasound or x-ray examination of the abdominal cavity. If the disease is not detected in time, there is a high probability of a sudden rupture of the aneurysm, which is externally accompanied by sudden pallor and loss of consciousness. The life of a patient with a ruptured aneurysm depends on how quickly he is taken to the hospital and placed on the operating table.
However, the asymptomatic course of the disease is not very common. As a rule, the development of an abdominal aortic aneurysm is indicated by:
- dull, aching pain in the epigastrium (in the upper abdomen) and mesogastrium (near the navel), often acquiring the character of attacks and even radiating to the lower back;
- a pulsating sensation reminiscent of a heartbeat and felt in the epigastric or mesogastric area.
These symptoms appear individually or in combination, depending on the type of aneurysm.
Risk factors and groups
- Age. Aortic aneurysm most often occurs in people over 60 years of age.
- Tobacco smoking. Smoking is one of the main risk factors for the formation of thoracic aortic aneurysm. With increasing smoking experience, the risk of aneurysm formation increases.
- Arterial hypertension. High blood pressure damages the blood vessels in the body and thereby increases the risk of developing an aortic aneurysm.
- Atherosclerosis. Increased levels of cholesterol and other substances that can damage the inner layer of blood vessels are also an important factor in the formation of aneurysms.
- Floor. Aortic aneurysms occur more often in men than in women. However, women with an aortic aneurysm have a higher risk of rupture than men.
- Race. Aortic aneurysm occurs more often in white people than in people of other races.
- Family history. If someone in the family has had cases of aortic aneurysm, then his blood relatives have an increased risk of developing an aneurysm. These people tend to form aneurysms at a younger age and have a higher risk of rupture.
Who is in more danger?
- Age - 50-79 years
- Gender – male (3 times more often)
- Smoking (increases risk 4-5 times)
- Patients with uncontrolled arterial hypertension (high blood pressure);
- Overweight patients;
- Patients with atherosclerotic lesions of blood vessels supplying the brain;
- Patients with impaired blood cholesterol metabolism (dyslipidemia);
- Patients whose relatives also had an aneurysm (the risk is doubled).
Men who smoke in adulthood are at greatest risk (statistically, every 10 have an aneurysm).
After operation
After installation of the prosthesis and suturing, the patient is admitted to the intensive care unit. In open surgery, the stay lasts from 5 to 7 days. Endoscopic manipulation is more gentle and requires less close medical supervision.
After the intensive care unit, the patient is transferred to the general unit, where he will spend another 2–3 weeks, and then the surgical sutures are removed. The exact period depends on the individual characteristics of the body: how quickly the recovery will take place after the manipulations, as well as on the presence or absence of complications.
The patient is then discharged home. He should be seen by a cardiologist or cardiac surgeon at his place of residence. Constant monitoring is necessary, which means visiting a doctor every month or, if indicated, more often. Then the number of examinations decreases: at first every six months, and 3 years after the operation it is enough to see a cardiologist once a year.
Taking medications
Patients who have undergone surgery require lifelong medication as indicated to prevent complications. The list of drugs includes:
- antibiotics for surgical interventions (including dental and gynecological procedures);
- antiplatelet agents that reduce the risk of blood clots;
- medications that lower blood pressure (diuretics, beta blockers and other types):
- medicines that fight chronic diseases (diabetes, tuberculosis, HIV, etc.).
The exact list of drugs, their dosage and dosage regimen are selected on an individual basis.
Complications
Immediately after surgery, complications may occur, including those that threaten the patient’s life. Among them:
- bleeding;
- thromboembolism;
- pulmonary edema;
- suppuration;
- kidney dysfunction.
There are also long-term consequences. The first places among them are occupied by thrombosis and infection of the installed prosthesis. Intestinal fistulas and sexual dysfunction occur less frequently in male patients.
Recommendations
An aneurysm is a serious pathology, and the operation to install a prosthesis is a serious surgical intervention. Therefore, the patient must permanently reconsider his habits and lifestyle. Compliance with the rules will help to avoid the re-formation of pathology, because the operation eliminates only the consequence - the aneurysm, and not the reasons for which it formed .
The patient needs:
- To refuse from bad habits.
- For the first month, lead a gentle lifestyle. This recommendation also includes maintaining a positive emotional state, including avoiding stressful situations.
- Do not lift weights over 5 kg.
- Eat right and watch your weight.
- Monitor blood pressure 2 times a day, maintaining it in the normal range (approximately 130/85).
- 4-6 months after surgery, begin light physical exercise without weights, after consulting with your doctor.
These are universal recommendations: others will be given by the cardiologist based on the individual characteristics of the patient.
Signs of RUPTURE of an abdominal aortic aneurysm:
- The appearance of abdominal pain, or a change (intensification) of pre-existing pain;
- The appearance of pain in the lower back, radiating to the groin, thighs, genitals;
- Possible clinical picture of myocardial infarction;
- Hypotension;
- Enlargement of a pre-existing pulsating mass in the abdominal cavity;
- Anemia;
- Possible bloody vomiting, etc.
More than 70 percent of patients with complicated abdominal aortic aneurysms were misdiagnosed during hospitalization.
Diagnostics
Ultrasound longitudinal and transverse B-scanning of the abdominal aorta is performed in three standard positions; under the diaphragm, at the level of the visceral branches and above the bifurcation. Depending on the echographic picture, it is proposed to distinguish three degrees of expansion of the diameter of the abdominal aorta (V. A. Sandrikov et al., 1996):
I degree - expansion of the abdominal aorta (diffuse or local): under the diaphragm and at the level of the visceral branches - up to 3 cm; above the bifurcation - up to 2.5 cm;
II degree - developing aneurysm of the abdominal aorta: under the diaphragm and at the level of the visceral branches - up to 4 cm; above the bifurcation - up to 3.5 cm;
III degree - abdominal aortic aneurysm: under the diaphragm and at the level of the visceral branches - from 4 cm; above the bifurcation - from 3.5 cm (including small aneurysms - up to 5 cm).
With an aneurysm, the expansion of the abdominal aorta is visualized as a rounded formation with a clear outer contour, an anechoic central part and hypoechoic parietal overlays with an uneven indistinct contour. The speed of blood flow in the area of the aneurysm is reduced, and the blood flow is turbulent.
For angiographic diagnosis of abdominal aortic aneurysms, Seldinger aortography in two projections is most often used. However, in patients with occlusion of the iliac arteries or in the presence of data on the location of the upper level of the aneurysm, translumbar aortography is indicated. In identifying suprarenal aneurysms, catheterization of the aorta through the axillary artery is advisable. The main angiographic sign of an aneurysm is the expansion of the lumen of a certain segment of the aorta compared with its superior or underlying portion. Based on the X-ray picture, aneurysms with a diameter of up to 3 - 5 cm are considered small, up to 5 - 7 cm - medium, up to 7 - 16 cm - large, more than 16 cm - giant. However, the true size of the aneurysm may not correspond to its size on the aortogram due to the presence of parietal thrombosis. In addition, in the case of complete thrombosis of the aneurysm, only the central part of the aneurysmal cavity is contrasted, creating the illusion of an intact aorta. Before the onset of an aneurysm, the aorta bends to the left. Most aneurysms lack contrast enhancement of the lumbar arteries.
A plain X-ray of the abdominal organs with an abdominal aortic aneurysm reveals a shadow of the aneurysmal sac and calcification of the wall. In contrast to aortic calcification in atherosclerosis, the calcified wall of the aneurysm is visualized like an arcuate line convex in relation to the spine. A fusiform aneurysm of the abdominal aorta is often visible.
X-ray contrast examination of organs and the gastrointestinal tract determines the displacement of the stomach and duodenum away from the center of the abdominal cavity. Intravenous urography in patients with aneurysms provides information about deviations in the position of the ureters, their external compression, and pyeloectasia.
On CT, an abdominal aortic aneurysm appears as a round formation with a smooth contour and a thin wall, often with foci of calcification. Along the inner surface of the wall there are parietal thrombi in the form of a semilunar or flat formation, which changes the correct cross-section of the aorta.
MRI also provides information about the structure of the aneurysm, the state of its contours and visceral branches of the abdominal aorta, the presence of thrombotic masses, and zones of dissection.
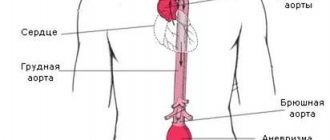
An abdominal aortic aneurysm is a local expansion of the lumen of the abdominal aorta, developing as a result of a pathological change in its walls or an abnormality in their development. Among all aneurysmal lesions of blood vessels, abdominal aortic aneurysm accounts for 95%. The disease is diagnosed in every twentieth man over the age of 60; women suffer less frequently.
Abdominal aortic aneurysm - main diagnostic methods:
- Physical examination - includes palpation of the abdomen, percussion, i.e. tapping, listening to the peritoneum using a phonendoscope, measuring pulse and blood pressure.
- Laboratory tests of physiological fluids - urine and blood. They help diagnose and determine the cause of the aneurysm.
- Duplex ultrasound examination is the “gold standard” for screening patients (detection and follow-up);
- CT angiography is the “gold standard” of preoperative examination and in cases where information from ultrasound scanning is insufficient;
- X-ray of the abdominal organs;
- Contrast-enhanced MRI angiography;
- X-ray contrast aortography.
Treatment tactics for abdominal aortic aneurysm
- If the size of the aortic aneurysm is less than 5.0 cm in diameter, the patient needs correction of risk factors under the dynamic supervision of a cardiologist, cardiovascular surgeon, and regular monitoring studies;
- If the size of the aortic aneurysm is ≥ 5.0 cm, then the patient requires surgical treatment to eliminate the risk of aneurysm rupture and other life-threatening complications.
- If the aneurysm is more than 3.0 cm and its size increases ≥ 6 mm per year, then the patient also needs surgical treatment.
An established diagnosis of an abdominal aortic aneurysm is an indication for surgery (at any age).
Contraindications for surgery:
- acute disorders of coronary and cerebral circulation with severe neurological deficits,
- circulatory failure stage IIB-III.
Prognosis after aortic replacement
The immediate postoperative period usually takes 10-14 days and depends on the immediate results of the operation. Within 1-3 days, patients require intensive care, and prolonged artificial ventilation is possible. We usually start lifting patients on the 3rd day after the intervention. We are allowed to walk by 5 days. If the postoperative period proceeds smoothly, the patient is discharged home on the 10th day.
After discharge, you must wear a special bandage on your stomach for a month. A month later, a control ultrasound scan is performed to assess the patency of the artificial prosthesis and the state of blood flow in the legs.
After open aortic surgery, the patient returns to normal daily activities after 3-6 months. The patency of vascular grafts is maintained at 93% over a five-year period after surgery. Ultrasound monitoring allows you to identify possible developments of problems and take timely measures to eliminate them.
Abdominal aortic aneurysm surgery
Abdominal aorta replacement
This is a standard open surgical procedure. In our Center, this operation is performed through a mini-access - an incision on the abdominal wall 5-7 cm long (while in the standard version the incision is 15-20 cm long). After processing the surgical field and preparing a vascular prosthesis of the required length for the time required for the operation, the abdominal aorta is clamped above and below the aneurysm. The aneurysm is excised and a prepared vascular graft is sewn in place of the removed area. After checking the tightness of the seams and installing drains, the wound is sutured.
At the Clinic of High Medical Technologies named after. N.I. Pirogov St. Petersburg State University in the treatment of an aneurysm of the abdominal aorta uses vascular prostheses impregnated with silver, which differ from conventional ones in being particularly resistant to infection. The operations last on average 3-4 hours, after which the patient is transferred to the intensive care unit for observation. In the standard course of the early postoperative period, the next morning the patient is transferred to the ward of the specialized department. The total length of hospitalization for such patients is about 7 days.
It should be noted that there are various forms of the disease that complicate the standard course of treatment, which in some cases may require longer hospitalization.
Aortic endoprosthetics
- A more modern method of treating abdominal aortic aneurysm, related to hybrid surgery. This method combines open surgical technologies with endovascular ones; it represents the replacement of an aneurysmally dilated section of the aorta from the inside using a special prosthesis, made in most cases “to order” (this explains its high cost). The vascular prosthesis is specially placed in the delivery system. It is straightened directly into the cavity of the aneurysm, under the control of an X-ray machine. Thus, the prosthesis eliminates the impact of systemic arterial blood flow on the weak, stretched walls of the aorta.
This method allows you to achieve results comparable to the open surgical technique, only with fewer complications, reducing the length of hospitalization and rehabilitation of the patient by 2 times! The use of this modern method is limited only by some anatomical parameters of the aorta itself and the high cost of the endoprosthesis.
Principle of operations for aortic aneurysm
The basic principle of operations for aortic aneurysm is the replacement of the area of the aorta affected by the aneurysm with an artificial prosthesis. This can be achieved either by removing such a section and suturing the aorta with an end-to-end prosthesis (this is the principle of open operations), or by placing an artificial shunt inside the vessel without removing the aneurysmal extension (this is the principle of intravascular minimally invasive operations).
Less commonly practiced are operations for resection of a saccular aneurysm with suturing of the aortic walls without installing a shunt, as well as palliative operations (for example, wrapping the aorta in synthetic tissue to prevent further expansion).
Prognosis and prevention
Unfortunately, abdominal aortic aneurysm is one of the most insidious and unpredictable vascular pathologies, in which the probability of death exceeds 50%. Prevention and timely detection of an aneurysm are essential for a positive outcome. Quitting nicotine addiction, as well as monitoring blood pressure and taking timely measures to normalize it, helps reduce the risk of developing an aneurysm.
Technological progress is helping to reduce the number of diagnostic errors: modern research methods make it possible to identify pathology even in the absence of symptoms. Therefore, people who are at risk - smokers, hypertensive patients, elderly people, as well as those who have a high probability of developing a congenital pathology - should consult a doctor more often for a diagnostic examination. Often, patients are unaware of the development of an aneurysm until it ruptures, but then medical care may not be provided in a timely manner.
Be sure to consult a cardiac surgeon about being examined for the presence of an abdominal aortic aneurysm. Timely detection of the disease can save your life and in any case preserve your health and performance.
Cost of the operation
Surgeries for aortic aneurysms are high-tech types of medical care. To perform this operation, you can obtain a quota from the regional Ministry of Health and carry it out free of charge in any cardiovascular center specializing in such operations.
However, it is necessary to reveal some nuances. First, treatment quotas are limited. You can't wait for them. Secondly, quotas do not cover the cost of aortic replacement, in particular the cost of a stent graft. The endoprosthesis, as a rule, is still paid for by the patient himself.
Prices for surgery depend on the type of intervention, the rank of the clinic, the need for artificial blood circulation and, of course, the cost of the prosthesis itself.
The surgical benefit itself for open surgery costs about 250,000 rubles. The cost of endoprosthesis replacement without taking into account the stent graft varies from 150,000 to 500,000 rubles. The cost of an endoprosthesis starts from 450,000 rubles.
Abroad, such operations cost from 7 thousand to 35 thousand dollars.
Causes and risk factors
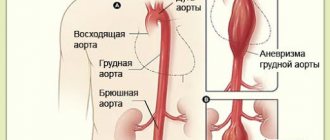
The results of numerous studies have shown that the main etiological factor of an abdominal aortic aneurysm, as well as other localizations of this pathological process (thoracic aorta, aortic arch), is atherosclerosis. In 80-90% of cases, the development of the disease is caused by it. Much less frequently, the development of acquired abdominal aortic aneurysms is associated with inflammatory processes (rheumatism, mycoplasmosis, salmonellosis, tuberculosis, syphilis, nonspecific aortoarteritis).
Often, an abdominal aortic aneurysm forms in patients with congenital defects in the structure of the vascular wall (fibromuscular dysplasia).
Causes of traumatic aneurysm of the abdominal aorta:
- spinal and abdominal injuries;
- technical errors when performing reconstructive operations (prosthetics, thromboembolectomy, stenting or aortic dilatation) or angiography.
Factors that increase the risk of developing an abdominal aortic aneurysm are:
- smoking – smokers make up 75% of all patients with this pathology; the longer the smoking history and the number of cigarettes smoked daily, the higher the risk of developing an aneurysm;
- age over 60 years;
- male gender;
- the presence of this disease in close relatives (hereditary predisposition).
Rupture of an abdominal aortic aneurysm most often occurs in patients suffering from chronic bronchopulmonary diseases and/or arterial hypertension. In addition, the size and shape of the aneurysm influence the risk of rupture. Symmetrical aneurysmal sacs rupture less frequently than asymmetrical ones. And giant dilations, reaching 9 cm in diameter or more, rupture in 75% of cases with massive bleeding and rapid death of patients.
Symptoms
The symptoms of aortic protrusion depend on the clinical course of the pathology. With an uncomplicated disease, an abdominal aortic aneurysm may remain undetected for years. In some cases, such a pathology is discovered by chance as part of a routine examination, medical examination, or during abdominal surgery for other health problems. This is precisely why it differs from thoracic aortic aneurysms, which cause noticeable changes in well-being almost from the very beginning.
An aneurysm of a vessel in the abdominal cavity has nonspecific signs that can be mistaken for renal colic, an inflammatory process in the pancreas, and pathological changes in the spine. This is due to the fact that the main symptom of the disease is a dull or aching pain localized in the upper and middle abdomen on the left side. In some cases, the pain spreads to the lower back, groin area and sacrum.
A distinctive feature of an aneurysm in the abdominal region is pulsation, which is felt upon palpation of the anterior abdominal wall.
When the tumor reaches a large size, it compresses nearby organs and tissues, causing the patient to develop various syndromes:
- intestinal, accompanied by heaviness in the abdomen, belching, nausea, chronic constipation and increased gas production;
- urological, accompanied by urinary retention, the appearance of traces of blood in the urine; in men, varicocele may develop due to compression of the abdominal vein by an aneurysm;
- ischiocardicular, accompanied by lumbar pain, decreased sensitivity and motor activity of the lower extremities;
- ischemic, accompanied by intermittent claudication, trophic changes in soft tissues, signs of varicose veins.
Such manifestations make it possible to judge the pathology of blood vessels in the abdominal cavity, since the symptoms of a thoracic aortic aneurysm in most cases affect the functionality of the lungs and heart and indirectly affect the blood supply to the brain. This pathology manifests itself as shortness of breath, headaches and neurological disorders. In rare cases, when a pathological focus in a vessel of the abdominal cavity is a continuation of an aneurysm in the descending aorta, both groups of symptoms may be of a cross nature.
Clinic
Aneurysms up to 4-7 cm in diameter do not cause subjective complaints. Sometimes an aortic aneurysm is discovered by chance. An asymptomatic course of the disease can be observed in 25-45%
sick. If symptoms are present, patients note dull, aching pain in the abdomen (in 90% of cases), and the presence of a pulsating formation (60%). A systolic murmur (75%) is heard above the aneurysmal dilatation. These are the main symptoms of an abdominal aortic aneurysm (AAA). Almost 1/4 of patients have a lack of appetite, weight loss, belching, vomiting, unstable stool or constipation, which may be due to compression of the duodenum or involvement of the visceral branches of the aorta in the pathological process. Arterial hypertension is detected in 60% of patients. Ischioradicular syndrome with sensory and motor disorders may occur. It is caused by compression of the spinal cord roots in the lumbar region. Symptoms of ischemia of the lower extremities may be associated with embolism from fragmented thrombotic masses from the aneurysm cavity and concomitant occlusive lesions of the main and peripheral arteries.
The severity of the clinical condition of predominantly elderly patients dictates the need for a correct assessment of the condition of both the aneurysm itself and concomitant diseases. In the diagnostic algorithm for examining patients, in addition to general clinical ones, the following research methods are used:
- plain radiography of the abdominal cavity;
- X-ray examination of the chest organs;
- ultrasound duplex scanning of the abdominal aorta, arteries of the lower extremities and brachiocephalic arteries;
- computed tomography of the abdominal aorta;
- nuclear magnetic resonance imaging of the abdominal aorta;
- X-ray contrast angiography;
- electrocardiography;
- echocardiography;
- study of kidney function (excretory urography and isotope renography);
- study of external respiration function;
- studies of the state of the gastrointestinal tract;
In most patients, the diagnosis of an aneurysm can be made without the use of invasive research methods, but before surgery, X-ray contrast aortoarteriography is necessary to clarify the condition of the main and peripheral arteries.
Differential diagnosis is carried out with a retroperitoneal lipoma, a package of enlarged retroperitoneal lymph nodes, lymphosarcoma, tumors of the stomach, intestines, and pancreas. An erroneous diagnosis is possible in the presence of a tumor or a horseshoe-shaped kidney, with a drooping, wandering kidney, when it is adjacent to the aorta and has a transmitting pulsation. The data from the study clarify the clinical picture.
The prognosis is unfavorable. Only 10-36.4% of patients live more than 5 years after diagnosis without surgical intervention, 50-70% of patients die from aneurysm rupture and bleeding.
Observations of patients have shown that aneurysms with a diameter of less than 3 cm increase per year on average by 0.21 cm, with a diameter of 3-4.9 cm - by 0.43 cm, and with a diameter of 6 cm - up to 0.75 cm per year. More than 80% of aneurysms progressively increase in size, 15 - 20% do not change. Aneurysms with a diameter of 4 cm or less are complicated by dissection and rupture in 9.5% of cases, with a diameter of 4 - 6 cm - in 23.4%, and with a diameter of 7 - 10 cm - in 45.6% of cases. This is the basis for indications for surgical treatment. If the aneurysm diameter increases by more than 5 cm per year, the indications for surgery are absolute. Age in itself is not a contraindication to surgery.
When determining the risk of surgery, three levels should be distinguished:
- first - age of patients over 75-85 years, mild unstable angina with ejection fraction less than 50%, but above 30%, creatininemia less than 2 mg%;
- second - age 85-90 years, stable angina, history of myocardial infarction, ejection fraction less than 30%, but above 20%, impaired pulmonary function, creatininemia 2-3.5 mg%;
- third - age over 90 years, angina pectoris II-III classes.
Prevention
For timely detection of abdominal aortic aneurysm, patients suffering from atherosclerosis or having a history of this vascular pathology are recommended to undergo systematic medical observation with periodic instrumental examination (radiography of the abdominal cavity, ultrasound).
Quitting smoking and active treatment of infectious and systemic inflammatory diseases are of no small importance in the prevention of aneurysm formation.
Video from YouTube on the topic of the article:
The first descriptions of an abdominal aortic aneurysm date back to the 16th century. The first successful resections of an abdominal aortic aneurysm with replacement of the defect with a homograft were performed in France.
Great contributions were made by De Beki, Crawford and Cooley, who used corrugated synthetic prostheses. In Russia, resection of an abdominal aortic aneurysm was first performed by V.A. Zhmur (1958), then B.V. Petrovsky, Yu.E. Berezov and others.
The main cause of abdominal aortic aneurysms is atherosclerosis (80-85%). Men get sick 3 times more often than women. In 95-96% of patients, aneurysms are located below the renal arteries, which is probably due to impaired blood flow to the vasa vasorum in this area.
Treatment
The only effective treatment for abdominal aortic aneurysm is surgical intervention to radically eliminate the deformed section of the vessel. It is impossible to cure or stop the progression of the pathology without surgery. in addition, ignoring the problem and trying to solve it with conservative methods can provoke life-threatening complications.
There are several types of operations for aortic aneurysm:
- resection of a fragment of a tube with protrusion and subsequent restoration of the bed with a graft of a special design - used when the straight section of the vessel is damaged at a distance from the branches;
- bifuctional prosthetics of the aorto-iliac part of the bloodstream - performed when the iliac branches are involved in the pathological process;
- installation of a stent graft, which allows isolating the formed aneurysmal sac from the general bloodstream without removing it.
Interventions are carried out as planned. The exception is acute cases: rupture or significant dissection of the walls of the aneurysm. In these cases, the operation is performed urgently.