- General characteristics of the abdominal aorta
- What function does it serve?
- Branches of the large unpaired arterial vessel
- Which doctor is treating you?
- Possible pathologies and complications of the abdominal aorta
- Prevention of abdominal aortic diseases
The abdominal aorta (abdominal) is responsible for feeding the lower part of the body - the abdomen and limbs. The health of the intestines, urinary and reproductive systems also depends on its performance. We will find out what pathologies threaten the abdominal aorta, how to treat them, and how to prevent possible diseases.
General characteristics of the abdominal aorta
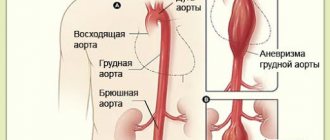
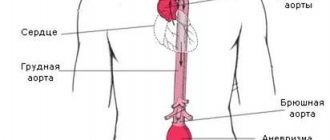
The aorta is the largest blood vessel in the human body. Its origin is the left ventricle of the heart. Passing sequentially through the chest and abdominal cavities, the aorta pumps arterial blood. Since the latter has very high pressure, the walls of the aorta are thicker and more elastic than those of other vessels. The aorta has many sections that are located in the chest area, and only the abdominal aorta passes through the abdominal area.
The abdominal aorta is located in front of the spine and is what delivers blood to the lower part of the body. The point of origin of the vessel is the aortic opening of the diaphragm, it is located opposite the 12th vertebra. Along the entire “path,” the vessel has many branches that feed different structures of the abdominal cavity.
The abdominal aorta in normal condition has the following dimensions:
- diameter – 18-20 mm;
- length – 13-15 cm.
The end of the abdominal aorta is located at the level of the 4th-5th vertebra. Here the aorta bifurcates into two iliac arteries directed in opposite directions.
Human anatomy is such that the abdominal aorta is maximally protected from damage, since the spine is located behind it. It is located slightly to the left of the medial (midline) line. In front of the aorta are the pancreas, duodenum, and the root of the mesentery of the small intestine.
What function does it serve?
The task of the abdominal aorta is to supply blood to the lower abdomen. It delivers oxygen and nutrients along with the blood:
- into the abdominal cavity;
- to your feet.
Thanks to the abdominal aorta, the functioning of:
- genitourinary system;
- digestive system.
This vessel also maintains normal blood pressure due to the elasticity of its walls. When the heart contracts, the walls of the aorta are stretched by a large volume of blood, and when it relaxes, the wall returns to its original position. Due to this mechanism, a large difference between systolic and diastolic blood pressure is prevented.
Systolic pressure evaluates the tension and filling of the arteries with blood at the moment of maximum contractile activity of the heart. Diastolic shows the minimum tension at the moment of myocardial relaxation.
Branches of the large unpaired arterial vessel
The aorta has many branches - parietal and splanchnic. The branches in the abdominal region are divided into:
- Parietal (parietal). They nourish the abdominal walls. This group consists of paired arteries:
- Inferior phrenic artery. This is a large paired vessel responsible for supplying blood to the adrenal glands and the lower surface of the diaphragm.
- Lumbar artery. These are two pairs of large vessels. They supply blood to the back, spinal cord, abdominal muscles, fiber, and skin.
- Visceral (splanchnic) paired arteries:
- Renal (renal) artery. Located behind the inferior vena cava. Near the kidney it has a branch that feeds the adrenal gland.
- Middle adrenal (suprarenal) artery. It nourishes the adrenal gland and is connected to the branches of the inferior and superior adrenal arteries.
- Testicular/ovarian artery (male/female) – supplies the genitals.
- Visceral azygos arteries:
- The celiac trunk, from which blood flows towards the stomach, liver, spleen. This is a 1-2 cm long vessel that arises from the aorta at the level of the 12th vertebra. It is divided into 3 arteries - the left pancreas (supplies the stomach with blood), the common hepatic artery (nourishes the liver, gall bladder, stomach walls and greater omentum) and the splenic artery (supplies the spleen, stomach walls and part of the pancreas).
- Superior mesenteric artery. Begins at the level of the 2nd lumbar vertebra. It passes through the anterior wall of the duodenum, and then divides into a number of branches. Nourishes the pancreas, as well as the intestines - cecum, ileum, colon, jejunum.
- Inferior mesenteric artery. Originating at the level of the 3rd lumbar vertebra, and dividing into several branches, it supplies blood to the intestines - rectum and colon.
content .. 149 150 151 152 153 154 155 156 157 158 159 ..
Branches of the thoracic and abdominal aorta (human anatomy)
Thoracic aorta
Two groups of branches depart from the thoracic aorta: visceral, rami viscerates, and parietal, rami parietales (Fig. 153).
Rice. 153. Vessels and nerves of the posterior wall of the left half of the chest cavity (the lung is turned away). 1 - truncus synipathicus; 2 - v. hemiazygos; 3- aorta descendens; 4 - v. hemiazygos ace; 5 - a. et v. intercostales posteriores, n. intercostalis; 6 - n. vagus; 7 - a. subclavia; 8 - plexus brachialis
Visceral branches of the thoracic aorta. The largest branches of the thoracic aorta are the following.
Bronchial branches
, rami bronchioles, which in number 3-4 originate from the anterior surface of the aorta at the level of the origin of the third intercostal arteries, enter the gates of the right and left lungs. An arterial plexus is formed around the intraorgan bronchi, which supplies blood to the bronchi, connective tissue stroma of the lung, peribronchial lymph nodes, and the walls of the upper pulmonary arteries and veins. The bronchial branches anastomose with the branches of the pulmonary arteries.
Esophageal branches
, rami esophagei, pericardial, rami pericardiaci, and mediastinal, rami mediastinals, are smaller and supply the corresponding formations with blood.
Parietal branches of the thoracic aorta. 1. Posterior intercostal arteries
, ah. intercostales posteriores, in an amount of 9-10 pairs, extend from the posterior wall of the aorta and are located in the III-XI intercostal spaces. The last posterior intercostal artery is the subcostal, a. subcostalis, goes below the XII rib and anastomoses with the lumbar arteries. The I and II intercostal spaces receive blood from the subclavian artery due to a. intercostalis suprema. The right intercostal arteries are slightly longer than the left ones and pass under the pleura behind the organs of the posterior mediastinum. The intercostal arteries at the heads of the ribs give off dorsal branches to the skin and muscles of the back, the spine and the spinal cord with its membranes. Continuations of the posterior intercostal arteries are located under the parietal pleura, and from the angles of the ribs they penetrate between the external and internal intercostal muscles to the costal groove. Anterior to the linea axillaris posterior, starting from the eighth intercostal space and below, the arteries lie in the intercostal spaces below the corresponding rib, give off lateral branches to the skin and muscles of the lateral part of the chest, and then anastomose with the anterior intercostal branches of the internal mammary artery. Branches extend from the IV, V and VI intercostal arteries to the mammary gland. The upper intercostal arteries supply blood to the chest, the lower three - the anterior abdominal wall and diaphragm.
2. Superior phrenic arteries
, ah. phrenicae superiores, paired, originate from the aorta above the hiatus aorticus. They supply blood to the lumbar part of the diaphragm. Anastomose with the lower intercostal arteries, with the branches of the internal thoracic and lower phrenic arteries.
Abdominal aorta
The abdominal aorta, aorta abdominalis, is located to the left of the midline; its length is 13-14 cm; initial diameter 17-19 mm. It is covered by the parietal peritoneum, stomach, pancreas and duodenum. It is crossed by the root of the mesentery of the small and transverse colon, the left renal and splenic veins. Autonomic nerve plexuses are located around the abdominal aorta,
lymphatic vessels and nodes. In the area of the hiatus aorticus behind the aorta lies the beginning of the thoracic lymphatic duct, and the inferior vena cava is adjacent to it on the right. At the level of the IV lumbar vertebra, the abdominal aorta is divided into paired common iliac arteries and the unpaired median sacral artery. The splanchnic and parietal branches begin from the abdominal aorta (Fig. 154).
Rice. 154. Abdominal aorta and its branches (according to Kiss-Sentagotai). 1 - aorta thoraeica; 2 - esophagus; 3, 35 - aa phrenicae inferiores; 4, 36 - diaphragma; 5 - glandula suprarenalis sinistra; 6, 34 - aa suprarenales superiores; 7 - truncus coeliacus; 8 - a. suprarenalis media; 9 - a. suprarenalis inferior; 10 - a. renalis; 11 - a. mesenterica superior; 12 - ren sinister; 13 - truncus sympathicus; 14, 31 - aa et vv testiculares; 15 - a. mesenterica inferior; 16 - aorta abdominalis; 17 - m. quadratus lumborum; 18 - a. iliaca communis sinistra; 19 - a. rectalis superior; 20, 30 - ureteri; 21 - a. et v. sacrales medianae; 22, 27 - a. et v. iliacae externae; 23 - a. iliaca interna; 24 - v. saphena magna; 25 - a. et v. femorales; 26 - funiculus spermaticus; 28 - m. psoas major; 29 - v. iliaca communis dext., 32, 38 - v. cava inferior; 33 - v. renalis; 37 - vv. hepaticae
Internal branches of the abdominal aorta. 1. Celiac trunk
, truncus coeliacus, with a diameter of 9 mm, a length of 0.5-2 cm, extends ventrally from the aorta at the level of the XII thoracic vertebra (Fig. 155). Under the base of the celiac trunk is the upper edge of the body of the pancreas, and on the sides of it is the celiac nerve plexus. Behind the parietal layer of the peritoneum, the celiac trunk is divided into 3 arteries: the left gastric, common hepatic and splenic.
Rice. 155. Celiac trunk and its branches. 1 - lig. teres hepatis; 2 - a. cystica; 3 - left lobe of the liver; 4, 16 - ductus choledochus; 5 - v. portae; 6 - v. cava inferior; 7 - a. gastrica sinistra; 8 - truncus coeliacus; 9 - aorta abdominalis; 10 - stomach; 11 - pancreas; 12 - a. gastroepiploica sinistra; 13 - a. gastroepiploica dextra; 14 - a. lienalis; 15 - a. hepatica communis; 17 - ductus cysticus; 18 - ductus hepaticus communis; 19 - right lobe of the liver; 20 - vesica fellea
Left gastric artery
, a. gastrica sinistra, initially passes behind the parietal peritoneum, goes up and to the left to the place where the esophagus enters the stomach, where it penetrates the thickness of the lesser omentum, turns 180°, descends along the lesser curvature of the stomach towards the right gastric artery. From the left gastric artery branches extend to the anterior and posterior walls of the body and the cardiac part of the stomach, anastomosing with the arteries of the esophagus, the right gastric and short arteries of the stomach.
Common hepatic artery
, a. hepatica communis, directed to the right of the celiac trunk, located behind and parallel to the pyloric part of the stomach. At the beginning of the duodenum, the common hepatic artery divides into the gastroduodenal artery, a. gastroduodenalis, and the hepatic artery itself, a. hepatica propria. From the latter originates the right gastric artery, a. gastrica dextra. The proper hepatic artery at the porta hepatis divides into right and left branches. The cystic artery departs from the right branch to the gallbladder, a. cystica. A. gastroduodenalis, penetrating between the pyloric part of the stomach and the head of the pancreas, is divided into two arteries: the superior pancreatic-duodenal, a. pancreaticoduodenalis superior, and the right gastroepiploic artery, a. gastroepiploica dextra. The latter passes in the omentum along the greater curvature of the stomach and anastomoses with the left gastroepiploic artery. A. gastrica dextra is located on the lesser curvature of the stomach and anastomoses with the left gastric artery.
Splenic artery
, a. lienalis, passes behind the stomach along the upper edge of the pancreas and at the hilum of the spleen is divided into 3-6 branches. From it depart: branches of the pancreas, rami pancreatici, short gastric arteries, aa. gastricae breves, - to the fundus of the stomach, left gastroepiploic artery, a. gastroepiploica sinistra, - to the greater curvature of the stomach and the greater omentum, anastomosing with the right gastroepiploic artery.
2. Superior mesenteric artery
, a. mesenterica superior, unpaired, arises from the anterior surface of the aorta at the level of the first lumbar vertebra (Fig. 156). The beginning of the artery is located between the head of the pancreas and the lower horizontal part of the duodenum. At the lower edge of the latter, the artery enters the root of the mesentery of the small intestine at the level of the II lumbar vertebra. The superior mesenteric artery gives off the following branches: the inferior pancreatic-duodenal artery, a. pancreaticoduodenalis inferior, anastomosing with the superior artery of the same name; 18-20 arteries of the jejunum and ileum, aa. jejunales et ilei, going in the mesentery to the loops of the jejunum and ileum; ileocecal artery, a. iliocolica, - to the cecum; it gives rise to the artery of the vermiform appendix, a. appendicular is, which is located in the mesentery of the process. The right colic artery, a., departs from the superior mesenteric artery to the ascending colon. colica dextra, to the transverse colon - middle colic artery, a. colica media, which runs deep into the mesocolon. The listed arteries anastomose with each other.
Rice. 156. Arteries and veins of the small and large intestines in front; the loops of the small intestine are retracted to the left; The transverse colic is pulled upward; the visceral layer of the peritoneum is partially removed (according to R. D. Sinelnikov). 1 - omentum majus; 2 - a. colica sinistra; h - a. mesenterica superior; 4 - v. mesenterica superior; 5 - aa. et vv. jejunales; 6 - aa. intestinales; 7 - appendix vermiformis; 8 - a. appendicularis; 9- aa. et vv. ilei; 10 - colon ascendens; 11 - a. et v. iliocolicae; 12 - a. Colica dextra; 13 — ascending branch a. colicae dextrae; 14 - a. et v. colica media; 15 pancreas; 16 - right branch a. colicae mediae; 17 - colon transversum
3. Inferior mesenteric artery
, a. mesenterica inferior, unpaired, like the previous one, starts from the anterior wall of the abdominal aorta at the level of the third lumbar vertebra. The main trunk of the artery and its branches are located behind the parietal layer of the peritoneum. It is divided into three large arteries: the left colon, a. colica sinistra - to the descending colon; sigmoid arteries, aa. sigmoideae - to the sigmoid colon; upper rectum, a. rectalis superior, - to the rectum. All arteries anastomose with each other. The anastomosis between the middle and left colic arteries is especially important, since it connects the beds of the superior and inferior mesenteric arteries.
4. Inferior phrenic artery
, a. phrenica inferior, steam room, is separated immediately after the aorta exits through the diaphragmatic opening. A special branch departs from it to the adrenal gland - the superior adrenal artery, a. suprarenalis superior, supplying blood to the diaphragm and adrenal gland; anastomoses with the upper arteries of the same name, lower intercostal and internal thoracic arteries (see Fig. 154).
5. Middle adrenal artery
, a. suprarenalis media, steam room, branches from the lateral surface of the aorta at the level of the lower edge of the first lumbar vertebra. In the thickness of the adrenal gland, it anastomoses with the superior and inferior adrenal arteries.
6. Renal artery
, a. renalis, steam room, 7-8 mm in diameter (see Fig. 154). The right renal artery is 0.5-0.8 cm longer than the left. In the renal sinus, the artery divides into 4-5 segmental arteries, which form an intraorgan branching system. At the hilum of the kidney, the inferior adrenal arteries, aa, depart from the renal arteries. suprarenales inferiores, supplying blood to the adrenal gland and the fatty capsule of the kidney.
7. Testicular artery
, a. testicularis, steam room, branches at the level of the II lumbar vertebra behind the root of the mesentery of the small intestine (see Fig. 154). Branches of the fatty membrane of the kidney and ureter extend from it in the upper part. In women, this artery is called the ovarian artery, a. ovarica; supplies blood to the corresponding sex gland.
8. Lumbar arteries
, ah. lumbales, paired, with 4-5 branches branching from the posterior wall of the abdominal aorta. They supply blood to the muscles and skin of the back, the spinal cord and its membranes.
9. Median sacral artery
, a. sacralis mediana, is an unpaired branch of the aorta (see Fig. 154). It arises from the aorta at the site of its division into two common iliac arteries. Supplies blood to the sacrum, surrounding muscles and rectum.
Pelvic arteries (human anatomy)
The abdominal aorta at the level of the IV lumbar vertebra is divided into two common iliac arteries, aa. iliacae communes, 1.3-1.4 cm in diameter, following along the medial edge of m. psoas major. At the level of the upper edge of the sacroiliac joint, these arteries are divided into the external and internal iliac arteries.
Internal iliac artery
, a. iliaca interna, steam room, lies on the lateral wall of the small pelvis. At the upper edge of the greater sciatic foramen, the artery divides into parietal and visceral branches (Fig. 157).
Rice. 157. Parietal and splanchnic arteries of the left part of the male pelvis. The bladder and rectum are turned to the right and downward. 1 - branches a. circumflexae ilium profundae to m. transversus abdominis; 2, 6 - a. epigastrica inferior; 3 - branches to m. iliacus; 4 - a. testicularis; 5 - a. circumflexa ilium profunda; 7 - a. obturatoria; 8 - a. umbilicalis; 9 - a. vesicalis superior; 10 - additional branch to the bladder; 11 - a. vesicalis inferior; 12 - ductus deferens sinister; 13 - vesicula seminalis; 14 - a. recta-lis media and its branch a. ductus deferentis; 15 - a. glutea inferior; 16 - a. pudenda interna; 17 - a. sacralis lateralis; 18 - a. glutea superior; 19 - a. iliaca externa; 20 - a. iliaca interna; 21 - a. iliaca communis sinistra; 22 - a. iliaca communis dextra
The parietal branches of the internal iliac artery are as follows:
1. Iliolumbar artery
, a. iliolumbalis, passes behind n. obturatorius, a. iliaca communis and under m. psoas major is divided into two branches: the lumbar, ramus lumbalis, and the iliac, ramus iliacus. The first vascularizes the lumbar muscles, spine and spinal cord, the second - the ilium and the muscle of the same name.
2. Lateral sacral artery
, a. sacralis lateralis, steam room, is located near the anterior sacral foramina, through which its branches penetrate into the sacral canal.
3. Obturator artery
, a. obturatoria, steam room, penetrates through the obturator canal into the medial part of the thigh between m. pectineus and m. obturatorius externus. Supplies blood to the pubis, adductor muscles of the thigh, ischium and femoral head. In 1/3 of cases, the obturator artery arises from a. epigastrica inferior and runs along the lower edge of the fossa inguinalis medialis, which must be taken into account during operations for inguinal hernias.
4. Superior gluteal artery
, a. glutea superior, steam room, penetrates the gluteal region through the foramen suprapiriforme. Supplies blood to the gluteus minimus and medius muscles.
5. Inferior gluteal artery
, a. glutea inferior, steam room, exits to the posterior surface of the pelvis through the foramen infrapiriforme. Supplies blood to the gluteus maximus muscle and the sciatic nerve. All parietal branches of the internal iliac artery anastomose with each other.
Visceral branches
The internal iliac artery is as follows.
1. Umbilical artery
, a. umbilicalis, steam room, is located under the parietal peritoneum on the sides of the bladder, then rises into the umbilical cord and reaches the placenta. After birth, part of it from the navel side is obliterated. The superior cystic artery, a., departs from the initial section of the artery to the apex of the bladder. vesicalis superior.
2. Inferior cystic artery
, a. vesicalis inferior, steam room, goes down and forward, enters the wall of the bottom of the bladder. It also supplies the prostate gland, seminal vesicles, and vagina with blood.
3. Artery of the vas deferens
, a. ductus deferentis, steam room, supplies the duct with blood.
4. Uterine artery
, a. uterina, steam room, penetrates the base of the broad uterine ligament and at the cervix gives off a branch to the upper part of the vagina, then rises upward and in the thickness of the broad uterine ligament gives off branches to the cervix and body of the uterus. Its terminal branch accompanies the fallopian tube and ends at the hilum of the ovary.
5. Middle rectal artery
, a. rectalis media, steam room, enters the lateral surfaces of the organ. Anastomoses with the superior and inferior rectal arteries.
6. Internal pudendal artery
, a. Pudenda interna, steam room, is the terminal branch of the visceral trunk. Through the foramen infrapiriforme it exits to the posterior surface of the pelvis, and then through the foramen ischiadicum minus it penetrates into the fossa ischiorectalis, where it gives off branches to the perineum, rectum and external genitalia (a. perinei. a. dorsalis penis, a. rectalis inferior).
External iliac artery
, a. iliaca externa, steam room, has a diameter of 10-12 mm, m. psoas major reaches the lacuna vasorum, where at the lower edge of the inguinal ligament it continues into the femoral artery (see Fig. 157). In the pelvic cavity, the external iliac artery gives two branches:
1. Inferior epigastric artery
, a. epigastrica inferior, steam room, begins 1-1.5 cm above lig. inguinale, located behind the parietal layer of the peritoneum medial to the deep inguinal ring, near which the spermatic cord crosses the artery. Here a begins from it. cremasterica to the muscle that suspends the testicle. The inferior epigastric artery, near the lateral border of the rectus abdominis muscle, reaches the umbilicus. Anastomoses with the superior epigastric, lumbar, and inferior intercostal arteries.
2. Deep artery
, surrounding the ilium, a. circumflexa ilium profunda, steam room, begins distal to the beginning of the inferior epigastric artery. Accompanies the inguinal ligament and reaches the iliac crest. Supplies blood to the transverse and internal oblique abdominal muscles. Forms a connection with the superficial artery surrounding the ilium and the iliopsoas artery.
content .. 149 150 151 152 153 154 155 156 157 158 159 ..
Possible pathologies and complications of the abdominal aorta
Abdominal aorta diseases are caused by problems with blood flow. To identify the reasons why blood circulates poorly, Doppler ultrasound is performed. This examination provides a good view of the abdominal aorta. Next, we will consider the most dangerous pathologies of this vessel.
Aneurysm
Abdominal aortic aneurysm is a dangerous, difficult to diagnose disease. The essence of the pathology is protrusion of the vessel wall caused by damage:
- inflammatory;
- traumatic;
- atherosclerotic.
The disease is initially asymptomatic and is detected during an ultrasound of the abdominal cavity.
With an abdominal aortic aneurysm, the following symptoms are observed:
- dull pain in the abdomen, pulling and bursting;
- feeling of heaviness in the umbilical area;
- throbbing in the abdomen;
- indigestion - upset stool, lower back pain, nausea, belching, numbness in the legs.
If an aneurysm is not diagnosed early, it can rupture. In this situation, the patient experiences:
- severe abdominal pain;
- weakness;
- dizziness;
- Vomiting may occur.
A strongly pulsating formation is palpated in the left abdominal area.
Factors contributing to the appearance of an aneurysm:
- male gender;
- bad heredity;
- age over 50 years;
- smoking;
- alcohol abuse;
- excess weight;
- diabetes;
- high blood pressure;
- high cholesterol.
Aneurysm rupture can cause:
- heavy physical activity;
- hypertensive crisis;
- injury.
Treatment of an aneurysm is prescribed based on the patient’s condition:
- Conservative. There is no medicine that can remove an aneurysm. But patients are prescribed cardiotropic and lipid-lowering drugs, anticoagulants, antiplatelet agents, antibiotics, and anti-inflammatory drugs. Drug therapy is needed to prevent the condition from getting worse.
- Operational. The only way to eliminate an aneurysm. The person being operated on is given general anesthesia. Indication for elective surgery is an aneurysm larger than 5 cm.
Atherosclerosis
Atherosclerosis of the abdominal aorta is one of the diseases of the cardiovascular system. Elderly people are at risk. Recently, the disease has also occurred in fairly young people.
Causes of atherosclerosis:
- Smoking and alcohol abuse.
- Sedentary lifestyle. Lack of physical activity.
- Poor nutrition. Abuse of fried, smoked, spicy, salty foods.
- Frequent stress, improper sleep and rest patterns, overwork.
- Background diseases that provoke atherosclerosis are hypertension, diabetes mellitus, hyperthyroidism.
- Metabolism disorders - protein and lipid, which causes increased cholesterol in the blood.
Symptoms:
- Discomfort in the abdominal area.
- Frequent pain in the gastrointestinal tract, especially after eating.
- Dyspepsia, stool motility disorder - diarrhea and constipation.
- After eating - heartburn, mild nausea.
- On the left side of the navel there is increased pulsation.
- Weight loss.
As atherosclerosis develops, other symptoms may appear:
- Swelling of the face.
- Difficulty and rare urination.
Treatment of atherosclerosis of the abdominal aorta is complex. The same as for atherosclerosis of any localization. They adjust their lifestyle, diet, and prescribe medication. The use of folk remedies is allowed - after consultation with the doctor. If necessary, surgical intervention is prescribed.
The diet is aimed at the predominance of plant foods over animal foods; sea fish and fiber are recommended. Diet No. 10 is recommended, limiting the consumption of salt, meat, dairy products, spicy, fried, and smoked foods.
Drug treatment is selected individually, after these studies. Fibrates and statins are prescribed.
Abdominal aortitis
Aortitis is a disease consisting of inflammation of the aortic wall. The inner, middle and outer layers of the aorta are affected - these are endaortitis, mesaortitis, periaortitis, respectively. Aortitis usually accompanies other vascular pathologies or infectious processes.
Aortitis can appear in people with:
- Takayasu disease;
- giant cell arteritis;
- ankylosing spondylitis;
- relapsing polychondritis;
- bacterial endocarditis;
- psoriatic arthritis;
- tuberculosis;
- Reiter's disease;
- syphilis;
- deep mycoses;
- sepsis;
- medianecrosis of the aorta;
- Cogan's syndrome.
There are several types of aortitis:
- allergic;
- infectious.
The disease can occur acutely, subacutely, chronically.
Symptoms of aortitis:
- blood circulation in the branches of the aorta is impaired;
- the appearance of pain of varying intensity;
- weakness, chills, cold extremities;
- systolic murmurs over the affected area of the aorta.
Complications of aortitis are aortic dissection and aneurysm formation.
The goal of treatment is to eliminate the causes of aortitis, relieve pain and restore normal blood circulation. Prescribed medications:
- antibiotics;
- immunosuppressants;
- anti-inflammatory drugs;
- analgesics.
Leriche syndrome
This is a relatively rare disease that involves blockage of the lower abdominal aorta and its major branches. At risk are men over 50 years of age.
The factors that provoke the disease are almost the same as for aneurysm and atherosclerosis - male gender, smoking, heredity, etc. Typically, Leriche syndrome occurs due to atherosclerosis of the iliac arteries and aorta.
The syndrome can be acquired or congenital; it consists of a narrowing of blood vessels, which ends with a complete cessation of blood flow. In severe cases, tissue death is observed, and patients face amputation of the lower extremities. The syndrome is accompanied by ischemia of the heart and cerebral vessels.
The main causes of Leriche syndrome:
- embolism;
- thrombosis;
- inflammation of the aorta;
- hypoplasia and aplasia of the aorta;
- chronic arterial diseases.
Symptoms:
- numbness and weakness of the legs;
- tingling and burning sensation in the legs;
- pain in the calf muscles after a long walk.
Further, the symptoms intensify, complications appear:
- impotence;
- lameness;
- thrombosis and acute disturbance of blood flow;
- decreased muscle tone in the legs;
- disappearance of the pulse in the arteries of the legs.
The skin of the legs becomes pale, then turns blue. There is hair loss, the appearance of bruises, necrosis, and trophic ulcers.
The syndrome is diagnosed based on visual examination and coagulogram. The treatment is complex. At first, medication and physiotherapeutic treatment is sufficient.
In severe situations, surgery is required. Depending on the condition, the patient may be offered:
- Prosthetics. After removing part of the artery, a synthetic prosthesis is installed
- Endarterectomy. Having removed the atherosclerotic plaque, the vessel is sutured.
- Aortofemoral bypass surgery. An anastomosis is established on the affected area.
- Stenting. An artificial element is placed in the diseased vessel through which blood moves.
All diseases of the abdominal aorta - aneurysms, aortitis, thrombosis - are extremely life-threatening. An important condition for saving lives is timely contact with specialists.
Mesenteric artery infarction
This is a dangerous complication consisting of ischemia of the intestine and visceral peritoneum due to blockage of the vessel by a thrombus. The cause of the pathology is cardiovascular diseases, congenital pathologies, hereditary factors. Subsequently, tissue death and peritonitis occur. Treatment is urgent surgery. Mortality – 60%.
The abdominal part of the aorta and its pathologies
Abdominal aortic disease is invariably associated with interference with healthy blood flow. Doppler ultrasound helps diagnose the reasons why this happens. The abdominal part of the aorta is clearly visible. With the help of the study, the specialist obtains data on the state of the blood flow, which nourishes all the organs of the abdominal cavity.
Doppler ultrasound allows you to obtain the most complete data on the condition of the abdominal aorta
Pathologies that are detected using ultrasound:
- Atherosclerosis caused by damage to the artery. The appearance of this disease is invariably associated with improper metabolic processes of vascular tissues and, as a consequence, cholesterol deposits.
- Abdominal aortic aneurysms. An aneurysm is an increase in the lumen of a vessel when its diameter exceeds 2 centimeters.
- Stenosis of the celiac trunk. Unlike aneurysm, these diseases are characterized by a too narrow diameter of the vascular branches of the abdominal aorta. In this case, there are disturbances in blood flow and, as a result, insufficient blood supply to the digestive organs.
- Occlusion is a narrowing of blood vessels and, as a rule, their absolute obstruction. This is a critical stage of progressive stenosis or atherosclerotic changes. Duplex scanning of the abdominal aorta allows you to obtain data that indicates the causes of the development of this pathology.
- Thrombosis, which can cause symptoms of atherosclerosis of the abdominal aorta, injury or infection. The sluggish process of narrowing of the aortic vessels gives rise to occlusion. Such diseases provide a favorable environment for the occurrence of thrombosis.
- Tortuosity of the aorta. This is a hereditary factor. Disruption of blood flow in the aorta is caused by changes in the main characteristics: elongation; tendency to form loops; numerous bends.
- Dehiscent aneurysm. This type of aneurysm can occur due to damage to the internal membranes of the branches of the aorta.
- Double arc. This is a congenital defect. Throughout life, it provokes pressure in the area of the esophagus and trachea.
Ultrasound allows you to diagnose an aneurysm with almost 100% confidence
Prevention of abdominal aortic diseases
To prevent damage to the walls of the abdominal aorta, comprehensive prevention is needed:
- Quitting smoking and alcohol.
- Regular examination.
- Proper nutrition. Remove products with animal fats.
- Elimination of stress and heavy physical activity.
- Treat in a timely manner pathologies that provoke the formation of atherosclerotic plaques - diabetes, high blood pressure, obesity.
- Once a year, thoroughly examine your body. This especially applies to people over 40 years of age.
- Prevent infection with infectious diseases.
- Do physical exercise and sports.
The abdominal aorta, being part of the largest vessel in the body, plays an important role in the functioning of the vascular system. Not only the functioning of the organs and structures of the entire lower part of the body, but also human life depends on the full functioning of the abdominal aorta.
What it is
We should start by defining the aorta. The aorta is the largest vessel in our body, and accordingly its importance is high. An aneurysm is an enlargement of a blood vessel. An aortic aneurysm can form in the thoracic or abdominal regions. Moreover, aneurysm of the abdominal aorta is much more common. This condition of the vessel may not cause any harm for a long time, however, an aneurysm is very dangerous due to the unpredictable course of expansion and the threat of rupture of the vessel walls when they become thinner - and this condition already poses a threat to life due to severe internal bleeding. In addition, blood clots can form at the site of vessel expansion due to changes in blood flow - the danger of this condition is the risk of the blood clot breaking off and clogging a smaller vessel.