Description of ultrasound of the aorta of the heart
Ultrasound of the cardiac aorta - what is it and what are its types? This is an examination that is carried out using special equipment. A sensor moves across the body and sends ultrasound signals to the computer. There it is processed and displayed on the screen in the form of images or graphs. Echocardiography has several types:
- M-echocardiography or one-dimensional . The data is displayed on the monitor in the form of a graph.
- Two-dimensional (or B-echocardiography). The data is displayed on the monitor as a gray-white image. It shows the relaxation and contraction of the myocardium, the movement of the heart valves.
- Doppler echocardiography allows you to evaluate blood flow (including reverse flow). The image shows blood flow in blue and red colors. It depends on its direction. Not only the speed of blood flow is measured. But also the diameters of the holes through which it passes.
- Echocardiography with contrast allows any abnormalities to be more clearly visualized.
- Stress echocardiography is performed under physical activity. This way you can identify many diseases at an early stage.
Transesophageal echocardiography may also be performed. The sensor is inserted into the body through the throat.
How do changes in the functioning of the aorta affect systemic blood flow?
The aorta is the only vessel from which the systemic circulation begins. Any of her diseases cause severe hemodynamic disturbances, including cardiovascular failure.
The first thing that suffers is blood pressure. Due to sclerosis and calcification, the arterial wall becomes rigid and loses its elasticity, and this is one of the causes of hypertension. When an aneurysm ruptures, the opposite is true - blood pressure drops sharply.
Aortic valve defects are very dangerous. Failure leads to regurgitation, which is the return of blood to the ventricle, causing it to overstretch, leading to cardiomyopathy. As a result of stenosis, cardiac output is also reduced. However, this is due to the fact that the doors do not open completely. At the same time, blood flow in the coronary arteries is disrupted. This leads to the development of angina pectoris.
The degree of disturbance of blood flow largely depends on the localization of the pathological process: the closer it is to the beginning of the vessel, the more systemic its effect will be, while damage to only the abdominal region causes hypoxia of a limited area of the body (lower torso).
Why is echocardiography needed?
Using cardiac ultrasound, the structure of the organ is examined in detail and its ability to pump blood is assessed. Echocardiography is necessary to monitor pathological processes, timely detection of diseases, and for postoperative monitoring.
It allows you to determine the size of the heart chambers, the thickness of the septa and walls, and the area of the valves. During diagnosis, the diameter of the main vessels, the speed of blood flow and the volume of blood ejected by the heart chambers are assessed. This makes it possible to promptly identify pathological changes (including aortic aneurysm) and prescribe timely treatment.
Anatomical features of the aorta of the heart
The aorta is the largest vessel in the body (in terms of length, diameter, volume of blood flow). It has three-layer walls and many branches, through which all systems and organs are supplied with blood. Therefore, aortic pathologies affect the functioning of the entire organism as a whole.
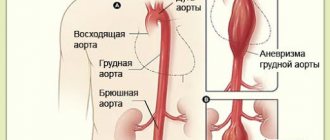
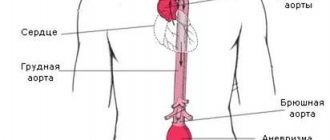
This main vessel is conventionally divided into three parts - the arch, the ascending and descending sections. The last one is the longest. Ends at the 4th lumbar vertebra. The iliac arteries originate there, which already belong to the abdominal aorta. The ascending part of the heart begins from the left ventricle.
Sections of the aorta: descending section (abdominal), aortic arch, ascending
The widest and thickest-walled vessel extending from the heart and forming a large circle of blood circulation is the aorta. It plays a key role in maintaining hemodynamics and blood supply to almost all vital organs.
The vessel is located in the thoracic part, directly above the apex of the heart and continues to the lumbar region: its beginning is represented by a bulb connected to the left ventricle of the heart, and the end is a branching into two iliac arteries.
The anatomy corresponds to the structure of all large vessels of the elastic type, and most pathologies can be surgically corrected if detected early.
Structure and departments
The anatomical structure of the aorta differs slightly from other arteries of the elastic type. Its shape is linear almost throughout its entire length, with a gradual decrease in diameter from the center to the periphery.
Periodically, the vessel bifurcates, forming two mirror-identical branches. In anatomy, this phenomenon is known as aortic bifurcation.
The walls of the tube consist of three layers, differing in histological characteristics:
- The intima, located on the inner surface, is the endothelial layer from which the aortic valve is formed. Normally it is tricuspid, but sometimes there is a genetic mutation when it is bicuspid.
- The media, located under the intimal part, consists of elastic and smooth muscle fibers that can stretch and contract quite strongly, maintaining a normal blood flow rate.
- The adventitia, located on the outer surface, consists of connective tissue fibers, collagen and elastin cells, which together create a fairly rigid frame.
Up to 5 liters of blood are transported through the vessel every minute. This volume creates constant pressure. Its normal values are considered to be 120-140 mm. rt. Art. (systolic indicator, that is, at the moment of cardiac output) and 70-90 mm. rt. Art. (diastolic indicator, that is, at the moment of filling of the left ventricle before the next ejection).
Depending on the distance from the heart, the diameter of the aorta gradually decreases from 40 at the root to 18 mm at the place where the bifurcation of the aorta into the iliac arteries is located.
The exception is the isthmus of the aorta, which is located near the heart on the arcuate part of the vessel. It has a smaller diameter than the areas located above and below.
Topographically, the bloodstream is divided into three parts: the ascending section, the arch and the descending section.
Rising department
The ascending aorta of the heart is located on the left side of the sternum at the level of the third rib. At the point where the heart tissue enters the vessel, the tricuspid semilunar valve is located.
This system is designed to prevent the backflow of arterial blood from the vessels into the left ventricle.
Distal to the valve, close to them, are the sinuses - small bulges on the wall in which the coronary arteries originate, delivering oxygenated blood to the myocardium.
At the exit from the heart, the aorta forms a bulb - a small extension, the walls of which are thicker than those of further sections. It is more durable and has increased elasticity to dampen sudden fluctuations in blood during cardiac output. At the level of the junction of the second rib with the sternum bone, the bulb narrows and becomes an arch.
Aortic arch
The aortic arch is a continuation of the ascending section and, as its name suggests, is a curved section that deviates to the left. Its end is located at the level of the fourth thoracic vertebra, where the arch passes into the descending section.
Sometimes, in the presence of a genetic abnormality of the vascular system, the right aortic arch is found instead of the left one. Its isthmus has the shape of a ring, inside which the esophagus and trachea can be located. With a right-sided aortic arch, there is no threat to the patient’s life, but the pulsation of the vessel provokes difficulties with breathing and swallowing.
Three branches branch off from the left and right aortic arches in the isthmus region, supplying the upper part of the body: brachiocephalic, left common carotid and left subclavian.
Descending department
The descending section has the greatest extent in the systemic circulation and is located in two sections:
- the thoracic aorta passes through the chest cavity;
- The abdominal aorta passes through the abdominal cavity.
Both the thoracic and abdominal aortas have a linear shape, from which arteries of smaller diameter periodically arise. The beginning of the section is located at the level of the fourth thoracic vertebra, and the end is at the level of the fourth lumbar vertebra.
The thoracic part of the vessel extends to the 12th thoracic vertebra, where it passes through an opening in the diaphragm and continues with the abdominal aorta. Along its entire length, unpaired and paired branches extend from it, supplying blood to the mediastinum, lungs, ribs, chest muscles, pleura, etc.
Arteries also branch from the abdominal part of the aorta, which are involved in the blood supply to the abdominal organs: the muscles of the anterior abdominal wall, liver, stomach and intestines, etc. It is also responsible for the blood circulation of the pelvic organs. The end of the abdominal aorta is the bifurcation of the vessel into the iliac arteries.
Functions
The aorta of the heart has a huge role to play. Being the beginning and main highway of the systemic circulation, it delivers blood to all organs of the chest, abdominal cavity and small pelvis.
From its arch originate the vessels that supply blood to the head and upper limbs, and from the abdominal part of the aorta blood enters the lower limbs.
From this we can conclude that almost all organs and tissues of the human body are supplied with blood through the aorta of the heart.
To the point where the aortic bifurcation begins, arteries branch off from it to all vital organs:
- in the chest cavity - to the heart and surrounding tissues;
- in the abdominal cavity from the infrarenal abdominal aorta - to the gastrointestinal tract and urinary organs;
- in the abdominal cavity from the intrarenal part of the vessel to the organs of the reproductive system.
The abdominal part of the aorta is completed by a bifurcation, that is, the bifurcation of the aorta, into the left and right iliac arteries, through which blood flows to the lower extremities.
In addition to nourishing tissues, the vessel takes part in the regulation of blood pressure. The mechanism of stretching and relaxing the walls prevents the formation of a large gap between blood pressure in systole and diastole.
Pathologies
The load to which the abdominal aorta and the thoracic section of the vessel located above are subjected often leads to the appearance of serious pathologies. Such diseases of the aorta are called acquired, that is, arising during the functioning of the body or the influence of external factors on it. These include:
- atherosclerosis - deposition of cholesterol on the walls of the vessel with subsequent calcification of plaques, as a result of which they lose their elasticity and worse regulate blood pressure;
- aneurysm - a pathological protrusion (pocket) on the wall, resulting from increased blood pressure on a vessel in which dissection or rupture may occur;
- aortic dissection - splitting of the vessel wall with blood entering the cavities, which often accompanies an aneurysm;
- inflammation of the vessel wall due to intoxication or an autoimmune process.
The list of congenital anomalies is more diverse, since it includes pathologies of an anatomical and physiological nature. Such diseases include:
- valve insufficiency, in which blood is thrown back into the ventricle, causing hypertrophy of the heart muscle and other pathologies;
- valve stenosis - fusion of the semilunar valves, due to which blood is not able to penetrate from the ventricle into the circulatory system at a normal speed;
- stenosis is a limited narrowing of a vessel, as a result of which the blood pressure in the upper area remains too high, and in the lower area – too low;
- Marfan syndrome - insufficiency of the connective tissue layer of the wall, in which aneurysms occur on the vessel and the valves become dysfunctional;
- bifurcation of the arch is a pathology in which the vessel has an additional bifurcation in the area of the esophagus and trachea, the latter are compressed in a ring, which makes swallowing and breathing difficult;
- right-sided arch - an abnormal position of the bend of the vessel, which sometimes leads to difficulties with breathing and swallowing.
The higher the affected part of the vessel is located, the greater the impact on health the pathology has. For example, the abdominal aorta affected by atherosclerosis provokes changes in the functioning of individual organs of the gastrointestinal tract, sometimes the pelvis and lower extremities, and with changes in the thoracic region, the heart, all organs located below the pathological focus, and even the brain will suffer.
Diagnostic methods
When signs of disease appear, a comprehensive diagnosis is carried out. It consists of instrumental studies:
- computed or magnetic resonance imaging;
- X-rays of the abdominal or chest cavity;
- EchoCG.
The listed procedures help the doctor detect pathological changes, determine their scale and exact location. To clarify changes in the functionality of the aorta of the abdominal cavity or thoracic region, Dopplerography and ultrasound of the vessel are used.
Laboratory blood tests for pathologies of the circulatory system are not very informative. They are used as auxiliary tools to confirm the diagnosis. For example, after visualizing a foreign body attached to the wall, the doctor uses tests to determine what it could be: if cholesterol is high, atherosclerosis is diagnosed, and if platelet levels are high, thrombosis is diagnosed.
Source: //bloodvessel.ru/krovenosnaya-sistema-cheloveka/aorta
Aortic pathologies
Normally, the aorta is hollow, tubular, with smooth walls. Their thickness is up to 3 mm, the diameter in the ascending part is 2-3.7 cm, in the arc region - 2.4 cm, in the descending part - 1-1.3 cm. Systolic amplitude is more than 7 mm. In case of deviations from the norm, various pathologies are recorded:
- Aortic aneurysms on cardiac ultrasound (fusiform or saccular) can complicate atherosclerosis or become manifestations of other pathologies - aortoarteritis, syphilitic aortitis, Erdheim's disease (medionecrosis) or Marfan syndrome. Aneurysms also appear after injuries or congenital anomalies (for example, with the aortic bicuspid valve).
- Tyakayasu disease (arch aortitis).
- Dissection (dissection) of the aorta. The lesion can appear in the ascending or descending part, in the arch and lower part.
- Nonspecific aortoarteritis.
- Aortic dilatation is accompanied by connective tissue dysplasia.
- Aneurysm of the sinuses of Valsava is characterized by protrusion of the walls. May occur with supravalvular stenosis or aortoarteritis. Children may be diagnosed with dilatation of the sinuses of Valsava, which has not reached the level of an aneurysm.
- Calcification of the aorta causes the development of aortic stenosis.
Atherosclerosis is the most common disease. It is characterized by compaction and thickening of the walls of the aorta (diffuse or local). At the same time, the contours are uneven. Damage to the walls can be mild, moderate or severe. There are also congenital defects of the aorta.
Standards for adults
Normal ultrasound readings in an adult should correspond to the following digital ranges:
- LV myocardial mass (left ventricle): men/women – 135–182 g/95–141 g, respectively;
- LV myocardial mass index: male – from 71 to 94 g/m2, female – from 71 to 89 g/m2;
- end diastolic size (EDS)/ESR (end systolic size): 46–57.1 mm/ 31–43 mm, respectively;
- LV wall thickness in relaxation (diastole) – up to 1.1 cm;
- blood ejection during contraction (FB) – 55–60%;
- the amount of blood pushed into the vessels - from 60 ml to 1/10 liter;
- RV size index – from 0.75 to 1.25 cm/m2;
- pancreatic wall thickness – up to ½ cm;
- ECD of the pancreas: 0.95 cm–2.05 cm.
Normal ultrasound indicators for the IVS (intergastric septum) and atria:
- wall thickness in the diastolic phase – 7.5 mm–1.1 cm;
- maximum deviation at systolic moment is 5 mm–9.5 mm.
- final diastolic volume of the RA (right atrium) – from 20 ml to 1/10 liter;
- LA dimensions (left atrium) – 18.5–33 mm;
- LA size index – 1.45–2.9 cm/m2.
The aortic opening normally ranges from 25 to 35 mm 2. A decrease in the indicator indicates stenosis. The heart valves should be free of tumors and deposits. Valve performance is assessed by comparing normal sizes and possible deviations in four degrees: I – 2–3 mm; II – 3–6 mm; III – 6–9 mm; IV – over 9 mm. These indicators determine how many millimeters the valve sags when the valves are closed.
The outer lining of the heart (pericardium) in a healthy state has no adhesions and does not contain fluid. The intensity of blood flow is determined during an additional examination to ultrasound - Dopplerography.
An ECG reads the electrostatic activity of heart rhythms and heart tissue. An ultrasound examination evaluates the speed of blood circulation, the structure and size of the organ. Ultrasound diagnostics, according to cardiologists, is a more reliable procedure for making the correct diagnosis.
Materials used in the article:
https://www.kievoncology.com/26-kompyuterno-tomograficheskaya-diagnostika-zabolevaniy-sosudov/kt-izobrazhenie-aorty-v-norme.html
https://apkhleb.ru/uzi/rasshifrovka-serdca
https://www.vseozrenii.ru/simptomy-glaznyh-boleznej/davyashchaya-bol-v-glazah/
Post Views: 78
Causes and clinical manifestations of aortic damage
Damage to the aorta appears as a result of pathologies of the cardiovascular system, high blood pressure, and inflammatory processes. The cause may be congenital heart defects. Many diseases are provoked by other pathologies. Clinical manifestations may vary:
- constant shortness of breath;
- cardiopalmus;
- chest pain;
- heart murmurs;
- lack of air;
- loss of consciousness;
- fast fatiguability;
- constant dizziness.
Patients often complain of dizziness and fatigue. Symptoms depend on the disease.
Complications
Complications occur in 18-23% of cases.
The risk of complications is proportional to the diameter of the formation. Individual risks increase in the presence of hypertension, pregnancy and concomitant diseases. Possible complications:
- Delamination;
- Gap;
- Bleeding into the pericardium, pleural cavity, lung;
- Hematoma in the chest cavity;
- Secondary infection;
- Cardiac tamponade;
- Compression of the spinal cord roots;
- Death.
Dissecting aneurysm of the thoracic aorta
Dissection is the divergence of the layers of the vascular wall with the formation of a hematoma, which stretches the expanded area to critical values.
Symptoms:
- Rapid deterioration in health;
- Pallor;
- Pain in the chest or interscapular space;
- Tachycardia;
- Increasing shortness of breath.
The pain is descending in nature and moves to the abdominal area within a few hours. Characterized by rapid loss of consciousness. The prognosis is unfavorable. The risk of rupture increases with persistent hypertension and averages 70-80%.
Rupture and its signs
The rupture can be a consequence of dissection, trauma to the chest, and can also be spontaneous (typical for the saccular form).
Symptoms:
- Diffuse or girdling pain;
- Weakness;
- Dizziness, fainting;
- Shallow rapid breathing;
- Tachycardia (pulse may become thready);
- Loss of consciousness;
- Clinical death.
The prognosis is extremely unfavorable . Mortality in the first minutes reaches 40-50%, with concomitant collapse - 80%.
Causes of death due to ruptured aneurysm of the thoracic aorta:
- Acute heart failure;
- Internal blood loss;
- Fibrillation.
Diagnosis of aortic pathologies
First, a cardiologist performs an external examination of the skin, listens to the heart, and listens to the patient’s complaints. Pulse and blood pressure are measured. Then ultrasound and echocardiography are prescribed. Diagnostics reveals changes in the G wave and 5T segment, left ventricular hypertrophy. With cardiac tamponade, an echocardiogram shows a decrease in the amplitude of the waves. Aortography helps detect:
- flap of the inner layer;
- filling defects;
- penetration of the contrast agent into the intramural area;
- double lumen;
- aortic insufficiency;
- compression of the lumen by false.
Using ultrasound, the ascending aneurysm is clearly visible. Diagnostics are also prescribed for descending. If ultrasound does not provide an accurate picture, additional x-rays, CT or MRI may be required. The devices have built-in Dopplers that allow you to trace the direction of blood flow in the heart chambers. During an ultrasound, their condition is assessed, the walls, myocardial movement, and the shape of the valves are measured. If deviations from the norm are detected, this indicates pathology of the aorta.
What treatment and correction methods exist and are considered effective?
A peculiarity of aortic pathologies is that their treatment mainly involves invasive surgical intervention. Conservative therapy is used only to support vital signs and relieve symptoms, which allows for safe surgery.
There is now a trend towards minimally invasive endoscopic operations, which are safer and more effective.
Today the following surgical treatment methods are used:
- resection with anastomosis – used for small aneurysms or coarctation;
- prosthetics;
- coronary artery bypass grafting (creation of bypass circulatory pathways) – for occlusive diseases, ischemic heart disease or heart attack;
- implantation of artificial valves, balloon valvuloplasty,
Indications for ultrasound of the aorta of the heart
An ultrasound examination is performed if any abnormalities in the functioning of the heart are detected. Echocardiography is the simplest and fastest way to determine pathologies even at an early stage of development. Indications for ultrasound:
- angina pectoris;
- shortness of breath (if its origin is not clear);
- heart murmurs and heart defects;
- myocardial infarction;
- thrombosis;
- swelling;
- varicose veins of the lower extremities.
Ultrasound is also indicated when signs of heart failure, acute or chronic ischemia appear. Alarming symptoms may include pale or bluish skin.
conclusions
Due to the peculiarities of anatomy and physiology, the aorta is the leading vessel of the human body. It provides blood supply to all tissues, and therefore any of its pathologies lead to extensive disturbances in the functioning of the entire organism. In recent years, the mortality rate from vascular pathologies has been decreasing due to the introduction of new minimally invasive surgical treatment techniques.
Source: cardiograf.com
The aorta is the largest, most powerful blood vessel in the human body. Powerful, therefore, it seemed that nothing “took” him. However, aortic aneurysm is the scourge of modern cardiovascular surgery. In normal conditions, in adult women and men, the diameter of the lumen of the ascending aorta is about 3 cm, the descending part is 2.5 cm, the abdominal segment of this large vessel is even smaller - 2 cm. The diagnosis of an aneurysm is announced only if the diameter of the affected aorta increases by 2 or more times compared to the norm.
An aneurysm is an abnormal bulge that occurs in the walls of an artery. The walls of the arteries are quite thick and strong, the muscle fibers of which they are composed allow them to withstand intense blood pressure. However, if there is a weak area in the artery wall, the pressure causes the area to bulge, thereby forming an aneurysm.
An aortic aneurysm can develop in two parts of this artery:
- the abdominal part passing through the lower part of the abdominal cavity is an abdominal aortic aneurysm;
- A thoracic aortic aneurysm developing in the chest cavity. This type of aneurysm is less common, but both types are equally dangerous to human health and life.
Depending on the appearance, the aneurysm can be: 1. fusiform 2. saccular.
Small aneurysms usually pose no threat. However, they can increase the risk of: the formation of atherosclerotic plaques at the site of the aneurysm, which cause further weakening of the artery walls; formation and separation of a blood clot, therefore increasing the risk of stroke; an increase in the size of the aneurysm, which means compression of nearby organs, which causes pain; aneurysm rupture. The main complication of aneurysms of any location is their dissection followed by possible rupture (mortality rate - 90%).
Causes and risk factors
The main causes of aneurysm are diseases and conditions that reduce the strength and elasticity of the vascular wall:
- atherosclerosis of the aortic wall (according to various sources, from 70 to 90%); inflammation of the aorta (aortitis) of a syphilitic, giant cell, mycotic nature;
- traumatic injury;
- congenital systemic connective tissue diseases (for example, Marfan or Ehlers-Danlos syndrome);
- autoimmune diseases (nonspecific aortoarteritis);
- iatrogenic causes caused by medical manipulations (reconstructive operations on the aorta and its branches, cardiac catheterization, aortography).
Risk factors for the development of atherosclerosis and aneurysm formation:
- male gender (the incidence of aneurysms in men is 2–14 times higher than in women);
- smoking (during screening diagnostics of 455 people aged 50 to 89 years in the Department of Vascular Surgery of the Moscow Regional Research Clinical Institute, it was revealed that 100% of patients with abdominal aortic aneurysms had a smoking history of more than 25 years, and as a result of the Whitehall study it was proven that life-threatening complications of aneurysms occur 4 times more often in smokers than in non-smokers);
- age over 55 years;
- family history;
- long-term arterial hypertension (blood pressure above 140/90 mm Hg);
- physical inactivity;
- excess body weight;
- increased blood cholesterol levels.
They also talk about a dissecting aneurysm, which is formed as a result of rupture of the inner membrane with its subsequent dissection and the formation of a second false channel for blood flow.
Depending on the location and extent of the dissection, 3 types of pathology are distinguished: 1. Dissection begins in the ascending aorta and moves along the arch (50%). 2. Dissection occurs only in the ascending aorta (35%). 3. Dissection begins in the descending aorta and moves down (more often) or up (less often) along the arch (15%). Depending on the duration of the process, a dissecting aneurysm can be: acute (1–2 days from the appearance of the endothelial defect); subacute (2–4 weeks); chronic (4–8 weeks or more, up to several years).
SYMPTOMS OF AN AORTIC ANEURYSM
Aortic aneurysm manifests itself in different ways - it mainly depends on the size of the aneurysmal sac and its location (below is a visual clinical picture using the example of an aneurysm of the sinus of Valsalva). In some cases, no symptoms are observed at all (in particular, before the aneurysm ruptures, but this will be a different diagnosis), which makes early diagnosis difficult. The most common complaints from patients with an aneurysm of the ascending aorta: pain in the chest (in the area of the heart or behind the sternum) - due to the fact that the aneurysmal protrusion presses on nearby organs and tissues, as well as due to the pressure of the blood flow on thinned and weak wall; shortness of breath, increasing over time; feeling of palpitations (“As if something is pounding in the chest” - a comment from patients); dizziness; with large aneurysms, attacks of headaches, swelling of the soft tissues of the face and upper half of the body are disturbing - due to the development of the so-called superior vena cava syndrome (because the aneurysm presses on the superior vena cava).
An aortic arch aneurysm is characterized by:
- difficulty swallowing (due to pressure on the esophagus);
- hoarseness of the voice, sometimes coughing - if the aneurysm puts pressure on the recurrent nerve, which is “responsible” for the voice;
- suddenly increased salivation and slow pulse - if pressure spreads to the vagus nerve, which controls salivation and pulse rate;
- strained breathing, and later shortness of breath if the trachea and bronchi are compressed by a huge aneurysm;
- unilateral pneumonia - if an aneurysm, pressing on the root of the lung, interferes with its normal ventilation, then, as a result, congestion occurs in the lungs, which, when an infection occurs, develops into pneumonia.
With an aneurysm of the descending aorta, the following appear:
- pain in the left hand (sometimes up to the fingers) and shoulder blade;
- with pressure on the intercostal arteries, a lack of oxygen supply to the spinal cord may develop, which is why paresis and paralysis are inevitable;
- in case of constant long-term pressure of a large aneurysm on the vertebrae, they may even be displaced;
- in milder cases, due to pressure on the intercostal nerves and arteries - pain, as with radiculitis or neuralgia.
The most common complaints with an aneurysm of the abdominal aorta:
- a feeling of fullness in the stomach and heaviness in the epigastrium (upper floor of the abdomen), which the patient initially tries to explain by overeating or stomach pathology;
- belching;
- in some cases, reflex vomiting (appears as a reaction to the pressure of the aortic aneurysm on nearby organs and tissues);
- When palpated, a tense, tumor-like pulsating formation is felt. Sometimes patients can independently detect this pulsation.
DIAGNOSIS OF AORTIC ANEURYSMS AND ITS COMPLICATIONS
An aortic aneurysm in the period before rupture has rather meager clinical manifestations: murmurs that are heard on auscultation; the doctor listens not only to the chest, but also to the abdominal cavity; a tumor-like pulsating formation, which is found with deep but careful palpation (sometimes it is actually regarded as a tumor, since it is quite dense to the touch); incomprehensible discomfort at the site of aneurysmal protrusion formation. Therefore, to clarify the pathology before it “gives birth” to dangerous complications, instrumental diagnostic methods are used: fluoroscopy and radiography of the chest and abdominal cavity - they visualize a tumor-like formation (its pulsation is visible during fluoroscopy); echocardiography - if an aneurysm of the ascending aorta is suspected; Doppler ultrasound (USDG) - for signs of aneurysm in other parts of the aorta; CT and MRI.
TREATMENT AND SURGERY FOR AORTIC ANEURYSM
If an aneurysm is diagnosed, but its progression is not observed, doctors adopt conservative tactics: further careful observation by a vascular surgeon and cardiologist - monitoring the general condition, blood pressure, pulse, repeated electrocardiography and other more informative methods to monitor the possible progression of the aneurysm and notice in time the prerequisites for complications of an aneurysm; antihypertensive therapy - in order to reduce blood pressure on the thinned wall of the aneurysm; anticoagulant treatment - to prevent the formation of blood clots and possible subsequent thromboembolism of medium and small vessels; reducing the amount of cholesterol in the blood (using both drug therapy and diet). Surgical intervention is resorted to in the following cases: large aneurysms (at least 4 cm in diameter) or with a rapid increase in size (by half a centimeter in six months); complications that threaten the patient’s life - aneurysm rupture and others; complications that, although not critical from the point of view of death, sharply reduce the patient’s quality of life - for example, pressure on nearby organs and tissues, which causes pain, shortness of breath, vomiting, belching and similar symptoms.
PROGNOSIS FOR AORTIC ANEURYSM
Aortic aneurysm is a nosology that should be constantly under close monitoring by doctors. The reason is possible complications, which in most cases threaten human life. Over time, the aneurysm progresses morphologically (the altered wall becomes thinner and thinner, the protrusion increases). The life and health of a patient can be saved only through careful monitoring of the course of the disease and, if necessary, immediate surgical intervention.
PREVENTIVE MEASURES
Prevention, thanks to which it is possible to prevent the occurrence of aortic aneurysm in healthy people, is nonspecific (that is, effective not only in the case of this pathology) and includes: complete cessation of smoking; reducing alcohol standards to the level of “only for holidays”, or better yet, a complete refusal; physical education and sports; elimination of factors that cause a rise in blood pressure (stress, kidney disease); treatment and prevention of pathology that contributes to the formation of aortic aneurysm (atherosclerosis); immediate alertness in the event of a sudden, at first glance inexplicable appearance of interruptions in the functioning of the heart, gastrointestinal tract and respiratory system and immediate examination by specialized specialists to exclude an aortic aneurysm; regular, high-quality, not just for show, medical examinations with a vascular surgeon and cardiologist. If an aortic aneurysm is already present, preventive measures are indicated in order to prevent complications of this disease: well-chosen anticoagulant therapy to prevent the formation of blood clots in the lumen of the aneurysm; a significant reduction in physical activity - otherwise they can cause overstrain of the thinned wall of the aneurysm, which will result in its rupture; sometimes a complete refusal of physical activity is necessary until the doctor clarifies the diagnosis and assesses the risk; antihypertensive treatment - thanks to it, it is possible to avoid an increase in the pressure of the blood flow on the thinned wall of the aneurysm, which can rupture at any moment; careful psychological control - in some patients, even minor stressful situations pushed the aortic aneurysm to rupture.
Source: www.cardio-tomsk.ru
Preparation for the event
Preparing for an ultrasound does not require diet or drinking regimen, or bowel cleansing. You can eat your last meal three hours before the test. Sometimes preliminary drug therapy may be required (for example, to equalize blood pressure and rapid pulse). Before intravascular ultrasound, the last meal is allowed 6 hours before the procedure, and liquid intake is stopped 4 hours before the procedure.
What diseases can be detected
Using ultrasound, it is possible to identify hidden abnormalities in athletes who experience heavy stress on the heart. Diagnostics helps to identify:
- Hypertension, a sign of which is coarctation of the aorta or stenosis (valve dysfunction). The disease is also indicated by dilation of the aorta in the ascending part and atherosclerotic plaques at the mouth.
- Cardiac valve defects. The mitral is most often affected.
- Mitral valve stenosis. In this case, the contents of the left ventricle are released into the aorta.
- Mitral valve insufficiency is characterized by reverse blood flow.
- Aortic tricuspid valve defects. With stenosis, the opening becomes smaller and the myocardium thickens. Aortic insufficiency is accompanied by incomplete closure of the valve. During an ultrasound, the length of the blood stream that is thrown into the left ventricle is assessed.
An ultrasound may reveal complications after a heart attack. For example, cardiac aneurysm, rupture of the septum between the ventricles, disruption of the papillary muscle and organ walls, tamponade.
Transesophageal echocardiography allows you to examine the mitral valve, identify aortic root abscess, and infective endocarditis. Diagnostics helps to identify septal defects and aortic aneurysms.
Today, ultrasound is the safest and most universal diagnostic method. The price of the examination depends on the region, location of the clinic, and equipment. In clinics, ultrasound is performed free of charge, in private medical institutions - from 110 rubles and can reach up to 2000 rubles. (if other organs are examined at the same time).
During the diagnosis of the aorta, a study of the heart and blood flow is simultaneously performed. The results obtained help to identify many pathologies in the initial stage.
Major diseases and developmental abnormalities
All diseases of the aorta, depending on their origin, are divided into two large classes: congenital and acquired.
The first include genetically determined developmental defects:
- Valve insufficiency - due to the underdevelopment of the valves, they do not close completely, and therefore, during diastole, part of the blood returns to the ventricle. As a result, myocardial hypertrophy develops and the initial part of the aorta expands.
- Valve stenosis is characterized by fusion of the leaflets, which makes it difficult for blood to pass through a narrow opening, which causes a decrease in systolic output and the development of dilated cardiomyopathy.
- Coarctation is a narrowing of the thoracic aorta. The modified segment can be from two millimeters to several centimeters in length, resulting in a significant increase in pressure in the area above the narrow part, but a significant drop in the lower sections.
- Marfan syndrome is a genetically determined disease characterized by damage to connective tissue. It is characterized by the frequent occurrence of aneurysms and valve defects.
- A double aortic arch is a defect in which the vessel is divided into two parts. Each of them bends around the esophagus and trachea, as a result of which they are enclosed in a ring. Hemodynamics are usually not impaired, the clinic is characterized by difficulty swallowing and breathing.
- Right-sided aortic arch - with this anomaly, the artery does not go to the left, as it should be normally, but to the right. The disease is usually asymptomatic, except in cases where the aortic ligament forms a ring around the trachea and esophagus, thereby compressing them.