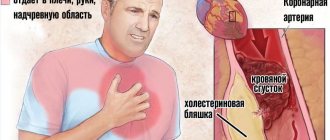
The aorta is the largest vessel in the human body and transports blood directly from the heart. Since the entire volume of blood passes through it in 1-2 minutes, damage and pathologies of this part of the circulatory system can lead to almost instant death. One of the diseases that leads to sudden death in 70% of cases is aortic dissection. Its main difficulty lies in the complete absence of symptoms in the early stages and the inability to quickly stop life-threatening complications.
Causes
The main cause of aortic dissection is the loss of elasticity of the vessel against the background of significant cellular changes. Vascular tissues lose their firmness and elasticity, and are destroyed due to cyclically increasing and decreasing blood pressure. The disease progresses slowly, and the process ends with a rupture of the aorta, the causes and symptoms of which in most cases are familiar only to doctors.
According to statistics, most cases of detachment of the aortic walls are congenital, and only 20% of patients have acquired pathological changes.
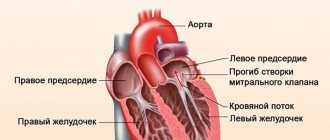
The mechanism of development of aortic dissection is the destruction of the inner lining of the vessel - the intima. Blood penetrates between it and the muscle layer, and under its pressure, the middle layer gradually peels off from the outer serous membrane. Since the latter has a small thickness, each impulse of blood can provoke a rupture of the vessel with profuse hemorrhage into the surrounding tissues.
Like an abdominal aortic aneurysm, a dissection in a large blood tube occurs due to increased arterial blood pressure. The reasons for this change may be congenital anomalies:
- localized narrowing of the aorta (coarctation) is a congenital disease that has severe symptoms, which makes it possible to detect dissection in the early stages;
- Aortic valve stenosis is a congenital pathology of the connective, muscular or conductive structures of the valve system;
- genetic transformations of the vascular system - Morphan syndrome, Ehlers syndrome and others.
The number of acquired pathologies that can cause dissection of a section of the aorta is more numerous. They are divided into three conditional groups:
- Traumatic. It includes conditions that resulted in a physical impact on the inner lining of the aorta or on all its layers: bruises of the chest, penetrating wounds, fractured ribs, unsuccessfully performed minimally invasive intervention with the introduction of a catheter into the aorta, surgical intervention near the location of the vessel.
- Associated with systemic diseases. It includes systemic pathologies that affect the functionality of blood vessels: early or late toxicosis of pregnancy, hypertension, autoimmune diseases.
- Associated with aortic pathologies. The group includes inflammatory and infectious vascular diseases, in particular aortitis, as well as atherosclerotic changes in the aorta and aneurysms.
With acquired dissection, the signs of pathology are in most cases erased or masked by the symptoms of the underlying disease. That is why doctors are able to diagnose them only with rapid progression.
What treatment methods do vascular surgeons typically use?
The first step when aortic dissection occurs is to stabilize the patient's condition. This requires hospitalization in the intensive care unit, where the patient will be provided with oxygen support, monitoring of cardiac and respiratory activity will be established, catheters for intravenous administration of medications will be installed, additional examination will be carried out and, if necessary, prepared for surgery.
First of all, the patient will be prescribed medications whose mechanism of action is to lower blood pressure and correct any rhythm disturbances that have arisen. Their introduction is necessary to prevent further dissection of the aorta into other parts and to prevent aortic rupture. The drugs of choice in this situation are beta blockers, for example esmolol [Brevibloc], labetalol [Normodyne, Trandate], metoprolol [Lopressor, Toprol XL]), which reduce the effect of adrenaline on the heart and blood vessels. vessels. Nitroglycerin is also used in therapy, which causes dilation of blood vessels, mainly the veins of the lower extremities, which reduces blood flow to the heart and lowers blood pressure. Of course, these drugs should not be used when the patient is in shock with low blood pressure. All drug support usually depends on the patient's hemodynamic status, blood pressure and cardiac contractility.
Due to the high risk of aortic rupture and progression of dissection, patients diagnosed with Stanford type A dissection require urgent surgical treatment. During the operation, the affected area of the aorta is removed and its prosthetics are performed. If the aortic valve is damaged, its replacement and implantation of an artificial valve can also be performed.
Fig.8 Prosthesis of the ascending aorta
Medical (non-surgical) treatment is preferred for type B aortic dissection, when the descending aorta is involved in the pathological process. With this type of dissection, treatment tactics are determined individually for each patient. If there is no threat of dissection progression, no signs of involvement in the dissection process of large arteries arising from the aorta, and no signs of circulatory disorders in the organs supplied by these arteries, then conservative treatment tactics are used. When diagnosing a complicated course, the patient needs more aggressive treatment, endovascular correction or open surgery.
Fig.9 Endoprosthetics for type B aortic dissection
Classification of pathology
The official classification of aortic dissections divides the pathology according to various criteria: localization, degree of damage to the vessel walls. It is used by surgeons to more simply describe a clinical case and further select treatment tactics.
Based on localization, the disease is divided into the following types (according to De Bakey):
- The first type is an extensive dissection of the vessel in the area from the ascending to the abdominal aorta. It is considered the most difficult due to its large length. It is accompanied by specific symptoms, therefore it is diagnosed earlier than other varieties.
- The second type is a pathology of limited prevalence, affecting the ascending aorta and arch. Due to the limited area of the lesion, it is accompanied by mild symptoms, but it is quite easy to operate, since the surgical field is well visualized.
- The third type - the area of destruction is limited only to the descending parts of the aorta. The disease is not accompanied by symptoms until the final stage with rupture of the aortic wall.
According to the degree and duration of the pathological process, three types of aortic dissection are distinguished:
- acute - primary destruction of the intima and further destructive process within 1-2 weeks;
- subacute - deeper dissection of the vessel, which occurs within 2 weeks and lasts up to 2 months;
- chronic - severe modification of the vessel wall with a high risk of rupture, lasting up to six months.
More than 70% of patients experience life-threatening complications of dissection within the first 10 days from the onset of the pathological process. Less than 1% of patients survive to enter the chronic stage.
Forecasts and preventive measures
A diagnosis of aortic dissection is considered very life-threatening. Lack of immediate medical care is the cause of death within two weeks of the onset of pathology in seventy-five percent of cases. Death often occurs due to multiple consequences of the disease.
Timely diagnosis and correct treatment allow the patient not only to survive, but also to return his life to its previous course. According to statistics, the survival rate of patients with ascending arch dissection is about seventy percent, while the chance of recovery with the localization of the detachment away from the heart increases to ninety percent.
Prevention of aortic dissection involves timely treatment of cardiovascular health problems. People who have a predisposition to cardiac diseases in their pathogenesis should undergo examinations on time, control their blood pressure, lead a correct lifestyle, monitor the cholesterol level in the blood, and unconditionally and strictly follow the recommendations of doctors.
Symptoms depending on the form
With dissecting aortic aneurysms, the symptoms practically do not depend on the location of the destructive process. This means that all types of the disease proceed approximately the same. The only difference between the clinical signs of a dissecting aortic wall is the degree of intensity of the symptoms, by which the doctor can determine whether the situation is tolerable
Emergency condition
With acute manifestation of aortic dissection, clinical manifestations become most pronounced. The main symptoms to suspect the disease are:
- a sharp jump in blood pressure by 30-50 points with a further spontaneous decrease in levels to critically low levels;
- sharp, unbearable pain behind the sternum, localized between the shoulder blades or in the area just below the neck and accompanied by a feeling of pressure and fullness, lumbago;
- tachycardia, accompanied by a feeling of anxiety, a feeling of acute lack of air.
- clouding of consciousness, shortness of breath, cold sweat, pallor and blue discoloration of the nasolabial triangle.
The listed symptoms are found in all patients in different variations. More rare signs of dissection requiring urgent intervention are impaired peripheral blood supply, intestinal disorders, transient ischemic attacks and repeated fainting.
Chronic form
The symptoms of chronic dissection are erased, gradually intensifying over two days. At the initial stage, the patient complains of discomfort in the sternum. In addition to the weak but constantly present compression and pain in the lower part of the neck or between the shoulder blades, he is bothered by:
- false urge to defecate;
- intestinal disorders (flatulence, nausea);
- hoarseness up to complete loss of voice;
- shortness of breath, darkening of the eyes;
- peripheral edema, which is especially noticeable in the legs;
- pallor of the mucous membranes, whitening of the fingertips.
After 1-2 days, an emergency condition develops, accompanied by corresponding symptoms.
About 40% of patients with chronic pathology die before diagnosis, about 60% - in the first 7 days after seeing a doctor, about 80% - within a month.
By location and length
| Type | Features of delamination |
| 1 | Starts in the ascending part Extends to the aortic arch Moves to the descending part |
| 2 | Defect only in the ascending zone |
| 3a | Originates below the left subclavian artery Extends within the descending portion |
| 3b | Same as for type 3a Extends to the abdominal part of the vessel |
According to clinical manifestations and prognosis
| Type | Its features |
| Proximal | Located in the ascending part And/or involves the aortic arch Does not depend on the state of the downstream part |
| Distal | Localized below the origin of the left subclavian artery Does not involve the proximal part |
Typing according to clinical manifestations and localization
Diagnostics
If signs of a dissecting aortic aneurysm appear, diagnosis must be carried out within several hours. The most important role is played by describing to the patient all the symptoms and indicating the exact time of their onset. Already on their basis, the doctor can make a preliminary diagnosis and prescribe studies that make it possible to establish the localization of the dissection and the extent of the spread of the destructive process. For this use:
- X-ray of the chest and abdomen;
- ultrasonography;
- MRI of the chest and abdominal cavity (the second option is used if type 1 of the disease is suspected).
Additionally, classical techniques are used: auscultation to detect sinus noises, ultrasound of the abdominal cavity.
Dissecting aortic aneurysm: research methods
ECG. There are no or nonspecific changes (left ventricular hypertrophy, changes in segment 7 or wave 7). Particular attention is paid to signs of AMI (if aortic dissection affects the ostium of the right coronary artery, then inferior AMI may develop).
Survey radiography. Changes may not be detected, but with hindsight they almost always are. A targeted search should be made for radiographic signs such as widening of the mediastinum, blurred contours or bulging of the aortic arch, unclear contour of the aorta, detachment (>5 mm) of the capcified inner membrane from the outer contour of the aorta. If possible, compare the obtained images with previous ones.
Blood OAK, urea and electrolytes, cardiac enzymes, blood group, Rh factor. Modern monoclonal antibodies can detect smooth muscle myosin heavy chains and differentiate between aortic dissection and AMI.
Treatment
To eliminate dissection of an aortic aneurysm, the only effective method is surgery. The operation is performed immediately after diagnosis and determination of the localization of the destructive process.
In medicine, isolated cases have been recorded where it was possible to stabilize the patient’s condition and control aortic dissection for several years. Such unique situations were made possible thanks to early identification of the problem.
Treatment of dissection is carried out by replacing the damaged area of the vessel with prosthetics. The intervention is performed in an open manner, regardless of the location of the dissection. At the initial stage, an additional branch of the blood supply is created, allowing blood to be directed to bypass the dissected area. Then the vascular surgeon excises the altered fragment of the aorta and installs a graft in its place - a prosthesis that replicates the removed tube in characteristics and size. At the end of the operation, the bypass artificial vessel is removed.
The operation does not guarantee that aortic dissection is defeated, since the etiological factors, that is, the causes of the disease, remain. To weaken their negative impact on the aortic walls in the postoperative period, lifelong conservative therapy begins. It consists of taking a complex of drugs:
- beta-blockers, calcium channel antagonists and ACE inhibitors to stabilize blood pressure;
- cardioprotectors and cardiac glycosides to stabilize heart rate;
- statins for the prevention of atherosclerotic changes;
- antiplatelet agents to prevent the formation of blood clots.
The prognosis after the intervention and if the recommendations are followed is favorable for 90% of patients, while in the absence of therapy only 15% manage to live longer than a year.
Symptoms of aortic dissection
Symptoms of vascular wall dissection are varied and can mimic almost all cardiovascular, as well as neurological and urological diseases. The clinical picture is determined by the localization of the primary fenestration of the aorta and the extent of the dissection process. Dissection is a dynamic process and with more or less long-term observation of the patient in the final stage of the disease, the clinical picture may differ significantly from the initial one.
The process can have three forms of flow:
- acute (up to 2 days);
- subacute (up to 2-4 weeks);
- chronic (months and even years).
A history of hypertension is usually noted. The most common symptom of aortic dissection is pain so intense that it often causes a collapsed state. A drop in blood pressure stops the process of aortic dissection, which somewhat reduces the intensity of pain and stabilizes the general condition of patients. The undulating course of the disease again leads to increased blood pressure and continued dissection of the aortic wall. In this case, the nature of the pain syndrome in terms of its primary localization and irradiation changes significantly.
Read also: Myocardial dystrophies - causes, symptoms, diagnosis, treatment
In type II dissection, the pain is usually localized behind the sternum and mimics acute myocardial infarction. This situation is especially common in cases where the dissection actually extends to the aortic root and contributes to compression of the coronary arteries. The pain syndrome really has a coronary origin. With further type I aortic dissection, the pain “moves” to the interscapular region, and then gradually “descends” along the spine to the lumbar region.
With type III aneurysms, pain is initially localized in the interscapular region. Patients compare it to a dagger stab in the back. The pain radiates to the left arm, the left half of the chest, and spreads to the lower back. When the dissection process spreads to the abdominal part of the aorta with type I and III aneurysms, pain appears in the epigastric, hypogastric region or is localized in the lumbar region. With retrograde dissection of type III aneurysms, pain can be retrosternal infarct-like in nature and radiate to the neck, which is caused by dissection of the aortic arch. Much less often, aortic dissection occurs with low-intensity pain. In a number of patients, aortic dissection is practically asymptomatic and the first signs of the disease are symptoms of ischemia of the brain or spinal cord, aortic insufficiency, ischemia of the kidneys, digestive organs and lower extremities. Often the first sign of dissection is the development of a pulsating formation in the abdomen, interpreted as an aneurysm of the abdominal aorta.
Dissection of the branches of the arch and descending thoracic and abdominal aorta can be accompanied by: 1) acute and then chronic ischemia of the brain or spinal cord; 2) acute ischemia of the digestive organs; 3) stable renovascular hypertension or renal infarction; 4) acute ischemia of the lower extremities. In this regard, patients can be given a variety of diagnoses - stroke, thrombosis of mesenteric vessels, renal colic, thromboembolism of the aortic bifurcation; and hospitalize them in hospitals of various profiles.
With the acute development of the disease and breakthrough of the aneurysm into the pericardial cavity, pleural cavity or retroperitoneal space, the first clinical signs may be pain and a typical picture of internal bleeding.
Symptoms of compression of adjacent organs, characteristic of true aneurysms of the thoracic aorta, can also develop with dissecting aortic aneurysms. With type II aneurysms, symptoms of venous hypertension of the head, neck, and upper extremities associated with compression of the superior vena cava are often observed. With type I aneurysms with aortic arch dissection, symptoms may appear associated with compression of the trachea, left bronchus (shortness of breath, stridor, frequent pneumonia) and the recurrent nerve (hoarseness, dry cough).
In some cases, the clinical picture with a dissecting aneurysm of the thoracic aorta is similar to the clinical picture of myocardial infarction, and with dissecting the abdominal aorta - with the picture of renal colic. The onset of pain during aortic aneurysm dissection is usually acute and sudden, while in acute coronary insufficiency the pain can increase gradually. The localization of pain is of great importance: with a dissecting aortic aneurysm, pain rarely radiates to the arms, and the localization of pain can change with a gradual movement of pain along the back, along the spine along the course of the aortic dissection; Gradually, pain can spread to the lower abdomen and pelvis.
With true renal colic, dysuria and other symptoms are usually characteristic. Evidence of the presence of a dissecting aortic aneurysm is also the appearance, following pain, of symptoms associated with the spread of aortic dissection in the area of origin of the great vessel or several vessels (pulse asymmetry in the upper and lower extremities, hemiparesis, paraplegia or stroke, pain in the lumbar region, hematuria, scrotal edema ). Various “peripheral vascular mask” diseases (like Takayasu syndrome), as well as “pneumonic” and gastrointestinal diseases (like acute abdomen) are also known.
Prevention
It is possible to prevent the occurrence of dissecting aneurysm of the thoracic aorta and other parts of the circulatory system only in the presence of acquired forms of the disease. Genetic and congenital abnormalities do not allow one to avoid the occurrence of pathology.
To avoid such a dangerous and rapidly developing disease, it is enough to exclude from life factors that can negatively affect the condition of blood vessels:
- get rid of bad habits - smoking, alcoholism, drug addiction;
- take medications only as prescribed by a doctor and in the agreed doses;
- avoid severe stress and excessive physical exertion, and also eliminate physical inactivity;
- adhere to the principles of healthy eating.
For patients in whom a dissected aneurysm has been diagnosed and removed, more stringent clinical recommendations have been drawn up. In addition to a special diet low in salt and solid fats, they are required to avoid any physical activity for six months. During the first 6 months after surgery, even household activities are sharply limited. After recovery, you must constantly take medications, regularly visit a doctor and undergo tests.
Examination for dissecting aortic aneurysm
Most patients are diagnosed with arterial hypertension at the time of admission. Hypotension is more common with upper aortic dissection (20-25%) and is due to blood loss, acute aortic incompetence (which may be accompanied by heart failure), or tamponade.
Check blood pressure in both arms and carefully evaluate the pulse in the peripheral vessels. The absence or change in the nature of the pulse indicates an expansion of the zone of dissection.
Auscultation may reveal regurgitation of the aortic valve and sometimes a pericardial friction rub. The consequence of rupture of the lower part of the aorta and the breakthrough of blood into the left pleural cavity may be dullness of sound in the left lower parts of the lungs, detected by percussion.
Neurologic deficits may result from carotid artery dissection, compression (hemiplegia), or occlusion of a spinal cord artery (paraplegia with sensory deficit).
- Congenital vascular diseases (bicuspid aortic valve)
- Inflammatory process in the wall of blood vessels (Coarctation of the aorta)
- Giant cell arteritis
- Takayasu arteritis
- Behçet's disease
- Syphilis
- Injury while braking (Road injury)
- Trauma (Fall from height)
- Pregnancy
- Iatrogenic disorders (Catheterization)
- Cardiac surgery
Marfan syndrome: the distance between the fingers of the hands apart is greater than the height, the distance from the pubic bone to the foot is greater than the distance from the pubic bone to the vertex, retraction of the sternum, scoliosis, gothic palate, anterior dislocation of the lens, dilatation of the thoracic aorta or aortic valve insufficiency, increased concentration in the urine hydroxyprolene (in some cases).
Complications
Vessel wall dissection is considered the main cause of aortic rupture in the abdomen and chest. This condition is key, that is, the most common complication of the disease and is diagnosed in 70% of patients with pathology not detected in time. From the moment the aorta ruptures until death due to massive blood loss takes from 2 to 5 minutes. The death of a patient occurs most quickly when the aorta of the heart ruptures.
Less common consequences of dissection are cerebral stroke or myocardial infarction. In 20% of cases, detection of vascular anomalies occurs only after their manifestation. Among the least common complications of the pathology is asystole - sudden cardiac arrest.
Etiology of the disease
Dissecting aortic aneurysm is a complication of the pathological condition of the artery, in which partial or complete destruction of its walls occurs. Depending on the etiology, two forms of the disease are classified:
- inflammatory - caused by infection or allergen;
- non-inflammatory - caused by mechanical damage, blockage of blood vessels.
The most common causes of rupture and dissection of an abdominal aortic aneurysm are:
- advanced atherosclerosis, accompanied by ischemia and a significant change in the condition of the vessel walls;
- hypertension;
- syphilis;
- focal necrosis of the artery walls due to infectious lesions;
- congenital defects of the aorta;
- physical overload;
- nervous tension;
- violation of the integrity of the aorta by an adjacent process or foreign body;
- closed abdominal trauma.
The state of the vascular system is negatively affected by smoking, excess weight combined with a sedentary lifestyle, genetic predisposition and chronic pathologies (diabetes mellitus, heart disease, etc.). Pregnant women over 40 years of age and elderly people are at risk. In rare cases, congenital aortic aneurysm occurs.