Causes of pathology
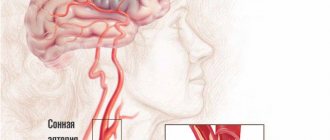
The main cause of stupor is stroke. It develops when the body is exposed to other provoking factors. Stunning is diagnosed in patients after traumatic brain injuries. If intoxication of the body is observed while taking certain medications, this leads to illness. During a stroke, oxygen starvation of the brain occurs, which leads to stupor .
If a person takes sleeping pills in excess, this leads to pathology. In tumor processes with metastasis, a pathological process is observed in the head. People who regularly drink alcohol or drugs are at risk. The pathological process is diagnosed with epilepsy or seizures, which are a symptom of a stroke.
Stupor develops after heat or sunstroke. If, during a stroke, severe viral or bacterial infections occur in the form of meningitis, encephalitis, viral hepatitis, then this becomes the cause of pathology. It is diagnosed in stroke patients when the body is dehydrated. The provoking factor is a severe allergic reaction to drugs that are used during the recovery period after a stroke.
Characteristics of the condition
Stupidity refers to quantitative syndromes of impaired consciousness. Such conditions develop as a result of a sharp change in metabolism in the head and are characterized by disruption of the sleep-wake cycle. The state of stunning always leads to a decrease in motor activity, up to absolute inhibition and switching off consciousness.
Stunning is a slowing down of all mental processes and disruption of verbal and visual contact with the outside world.
Typically, mild and moderate stunning are temporary conditions resulting from certain medical conditions. A healthy person can also feel a feeling of stupor: this can be caused, for example, by regular lack of sleep. In this situation, the patient needs to get some sleep and establish a work-rest routine.
Causes of stupor also include:
- traumatic brain injuries;
- intoxication due to taking medications;
- stroke;
- oxygen starvation of the brain;
- poisoning due to an overdose of sleeping pills;
complication of diabetes mellitus;- severe bacterial and viral infections: meningitis, viral hepatitis, encephalitis;
- heat or sunstroke;
- dehydration and lack of electrolytes;
- tumors or metastases in the head;
- electric shock;
- alcohol poisoning;
- drug overdose;
- seizure or epilepsy;
- severe allergies.
Stupidity is most often a symptom of the disease; it is often confused with another disorder of consciousness - delirium. The clinical picture for both syndromes is similar, however, with delirium, vivid delusional hallucinations occur, which are not inherent in the state of stunning.
With progressive deafness, it is extremely important to establish the cause of the syndrome.
To do this, a comprehensive diagnosis is carried out:
- visual examination of the patient: measurement of pressure, temperature, pulse, analysis of pupil movement;
- cardiogram for heart rate analysis;
- chest x-ray;
- blood and urine tests;
- determination of biochemical indicators of liver function;
- X-ray of the skull if a head injury is suspected;
- electroencephalography to determine the level of mental activity;
- toxicological analysis for intoxication;
- Ultrasound of the vessels in the head that supply the brain.
The most informative answer is provided by computed tomography or MRI. Regardless of the stage of deafness, the patient must be hospitalized in the neurological department.
Diagnostic measures
Mild to severe stupor is temporary and may go away on its own. If a patient is diagnosed with progressive stupor, he is advised to seek help from a doctor. The specialist will examine the patient and collect anamnesis, which will allow him to make a presumptive diagnosis.
During the visual examination, it is recommended to measure body temperature, blood pressure and pulse. The specialist also analyzes the movement of the pupils. To confirm a preliminary diagnosis, it is recommended to use additional methods:
- Ultrasound examination of the vessels that supply food to the brain.
- Cardiograms, which analyze heart rhythm.
- Toxicological analysis, which confirms or refutes intoxication of the body.
- Chest X-ray.
- Electroencephalography, which is used to determine mental activity.
- X-ray of the skull, which detects head injuries.
- A biochemical study that determines the performance of the liver.
If a pathological process is suspected, a comprehensive diagnosis is recommended, with the help of which the severity of the pathological process is determined and effective treatment is prescribed.
Stupefaction: what is this condition, a moderate and deep sense of consciousness in the head
Impaired consciousness is expressed in quantitative and qualitative changes.
Towards quantitative syndromes
disturbances (depression) of consciousness include: stupor, stupor, coma.
Quantitative disturbances of consciousness (depression of consciousness) develop due to morphological or pronounced metabolic changes in the brain, and are accompanied by a decrease in the level of wakefulness, motor activity, intellectual functions, up to complete depression and switching off of consciousness.
Total information
Rupture of a blood vessel. Hemorrhagic stroke is an acute emergency condition that occurs when blood penetrates from the vascular bed into the substance of the brain, under its membranes, or into the ventricles. Compared to ischemic stroke, it occurs in only 15%, and in Finland and Japan it is twice as common as in European countries.
Stun
Stun
- a decrease in consciousness in which limited verbal contact with the victim is maintained against the background of an increase in the threshold for perception of external stimuli and a decrease in one’s own mental activity.
Moderate stun
accompanied by slowing down, difficulty, impoverishment of mental activity, and a decrease in the ability for active attention.
Verbal contact with the victim is preserved, but answers to questions are delayed; sometimes it is necessary to repeat the question or pat the victim, who carries out the commands correctly, but slowly.
The patient is lethargic, quickly exhausted, his facial expressions are impoverished, his motor reaction to pain is purposeful, orientation in his own personality is preserved, orientation in the area, and especially in time, may be impaired.
Deep Stun
accompanied by constant drowsiness with rare episodes of motor activity, a sharp difficulty in mental activity.
Verbal contact with the victim is severely difficult, answers can only be obtained after persistent requests, they are monosyllabic in nature - “yes”, “no”, while the victim is able to provide his information: full name, age. It is possible to repeat the same word multiple times.
The victim is able to follow basic commands: open his eyes, show his tongue, etc. The coordinated defensive reaction to pain is preserved, but orientation in place and time is absent.
Nullification
(cloudy consciousness) - a mild degree of stupor, can be observed in the first stages of stun, reminiscent of a state of mild alcoholic intoxication - the victim experiences carelessness, lability of consciousness, absent-minded attention, while the victim may give answers to questions after a while and at random.
Doubtfulness
(state of half-asleep) - is a type of stupor, characterized by minimal motor activity.
The victim lies motionless with his eyes closed, makes no complaints, speech contact is minimal, only with persistent external influence. The patient gives correct answers to simple questions, but does not understand complex questions.
The patient can be brought out of a state of doubt for a short time with the help of persistent external stimuli.
First aid for stunning:
- Treatment of the underlying disease.
- Normalization of electrolyte metabolism, elimination of signs of dehydration if present.
- Normalization of acid-base status.
- Detoxification therapy.
- Normalization of metabolic processes in the brain. Nootropic drugs are prescribed for this purpose.
Restoration of motor functions
It is advisable to begin work on the rehabilitation of motor activity from the first days after the ONMC manifesto. It all starts with placing the sore limbs in a certain position. At the same time, they are secured with the help of a splint or sandbags.
The dominant role in restoring motor activity of the limbs belongs to the exercise therapy complex. Methods of its implementation, in addition to position therapy, gymnastics with passive exercises and learning to walk, include special sets of exercises that are aimed at different muscle groups.
Massage is no less important.
The use of modern biofeedback simulators, as well as verticalization systems, is relevant - their use allows you to significantly reduce the time required for the rehabilitation of motor skills.
At home, people also undergo rehabilitation and take medications, thanks to which they can achieve what was not done in terms of restoring lost functions in a medical institution.
It is clear that only with the help of medication it will not be possible to fully restore motor activity - it is necessary to perform a whole set of exercises, however, the patient makes the main progress in this direction in a specialized rehabilitation center, where there is all the necessary equipment. At home, he simply “polishes” his restored skills.
Sopor
Stupor is a deep depression of consciousness in which the victim retains coordinated defensive reactions, opening the eyes in response to stimuli.
The victim lies with his eyes closed; he can be briefly brought out of a drowsy state.
In this case, the patient is motionless or makes automatic stereotypic movements, reaching with his hand to the place of application of painful irritation, and a painful expression on his face may appear as a pain response.
Coma is a complete shutdown of consciousness without any signs of mental life, while the victim cannot be brought out of this state with the appearance of any signs of mental activity.
- Moderate coma
(coma I) - the victim has a preserved reaction to painful stimuli (flexion and extension movements of a dystonic nature), while protective motor reactions are not coordinated, the patient does not open his eyes, pupillary and corneal reflexes are preserved, abdominal reflexes are depressed, tendon reflexes are variable. Increased pathological foot reflexes and reflexes of oral automatism. - Deep coma
(coma II) - there are no reactions to external stimuli, various changes in muscle tone are observed, spontaneous breathing and cardiovascular activity are preserved even if they are severely impaired. - Terminal coma
(coma III) - bilateral mydriasis, diffuse muscle atonia, severe disturbances of vital functions, respiratory rhythm and frequency disorders, apnea, tachycardia or bradycardia, blood pressure is not determined.
Characteristics of the condition
Stupidity refers to quantitative syndromes of impaired consciousness. Such conditions develop as a result of a sharp change in metabolism in the head and are characterized by disruption of the sleep-wake cycle. The state of stunning always leads to a decrease in motor activity, up to absolute inhibition and switching off consciousness.
Stunning is a slowing down of all mental processes and disruption of verbal and visual contact with the outside world.
Typically, mild and moderate stunning are temporary conditions resulting from certain medical conditions. A healthy person can also feel a feeling of stupor: this can be caused, for example, by regular lack of sleep. In this situation, the patient needs to get some sleep and establish a work-rest routine.
Causes of stupor also include:
- traumatic brain injuries;
- intoxication due to taking medications;
- stroke;
- oxygen starvation of the brain;
- poisoning due to an overdose of sleeping pills;
- complication of diabetes mellitus;
- severe bacterial and viral infections: meningitis, viral hepatitis, encephalitis;
- heat or sunstroke;
- dehydration and lack of electrolytes;
- tumors or metastases in the head;
- electric shock;
- alcohol poisoning;
- drug overdose;
- seizure or epilepsy;
- severe allergies.
Stupidity is most often a symptom of the disease; it is often confused with another disorder of consciousness - delirium. The clinical picture for both syndromes is similar, however, with delirium, vivid delusional hallucinations occur, which are not inherent in the state of stunning.
With progressive deafness, it is extremely important to establish the cause of the syndrome.
To do this, a comprehensive diagnosis is carried out:
- visual examination of the patient: measurement of pressure, temperature, pulse, analysis of pupil movement;
- cardiogram for heart rate analysis;
- chest x-ray;
- blood and urine tests;
- determination of biochemical indicators of liver function;
- X-ray of the skull if a head injury is suspected;
- electroencephalography to determine the level of mental activity;
- toxicological analysis for intoxication;
- Ultrasound of the vessels in the head that supply the brain.
The most informative answer is provided by computed tomography or MRI. Regardless of the stage of deafness, the patient must be hospitalized in the neurological department.
Diagnostic approach
Diagnosis comes down to the study of clinical symptoms that can be detected during examination of the patient.
Pulse and pressure are measured, corneal and tendon reflexes, muscle tone, response to pain, and more are checked. During the initial examination, subcoma is distinguished from stunning and coma.
Then specialists determine what caused the person to fall into stupor. To do this, the patient is examined to find: head injuries, hemorrhages, alcohol odor, rashes, injection marks, and more. Body temperature, blood pressure, and blood glucose levels are measured. An electrocardiogram is taken.
Next, medical records are studied, the patient’s personal belongings are examined, relatives are interviewed, and other activities are carried out in order to find out about the patient’s other diseases, such as diabetes, liver failure, and epilepsy.
Source: https://medspina.ru/kosti-i-sustavy/oglushenie-pri-insulte.html
Types of stupor
The pathological process is classified according to its severity.
It is the mildest stage of stupor. With pathology, the patient experiences mild lethargy. He cannot fully perceive reality. With pathology, patients' motor activity decreases. If there is a mild stage of the disease, then a person can express his thoughts, but it takes a long time to find words for this.
With pathology, a person cannot think logically and directs his gaze to one point. The disease is accompanied by disorientation in time and space. Sometimes there is a clear consciousness and good mood, which alternates with the above symptoms.
This is the average severity of the pathological process, which often accompanies a stroke. The patient feels deep sleep, so a corresponding reaction occurs when exposed to strong irritants - injections, pinching, blows. When there is noise, a person opens his eyes and looks at one point .
The pathological process is accompanied by convulsive seizures. With stupor, there is a decrease in the reaction of the pupils to light. Stunning during a stroke causes tension in the neck muscles. Sometimes there is a way out of the state of stupor for a short period of time.
This condition is a profound stun. Before the onset of coma, a person is depressed and lethargic. Patients complain of ringing in the ears. A gradual loss of coordination of movements is diagnosed. The duration of precoma ranges from several minutes to several seconds . Next, the first stage of coma is observed, in which the patient’s eyes are closed. He can drink water and take liquid food. Human pupils react to light.
The second stage is characterized by unconsciousness. The appearance of cramps and chaotic muscle movements is observed. The bladder and intestines are emptied chaotically. The disease is accompanied by constriction of the pupils and lack of reaction to light. At the last stage, a decrease in body temperature and pressure, as well as impaired respiratory function, is diagnosed. There are no reactions to external stimuli.
Types of pathology
Symptomatic disorder of consciousness is classified according to severity. Let's look at their differences:
The mildest stage of stunning is nubilization, or moderate stunning. The condition is characterized by mild retardation of the patient, decreased motor activity, and poor perception of reality. At a mild stage of deafness, a person retains the ability to express himself, but it takes a long time to find words. This state is also called “fluctuating consciousness.” The following symptoms are characteristic of nullification:
lack of ability to think logically;- alienation and detachment from events happening around;
- gaze directed at one point;
- disorientation in space and time;
- temporary bouts of good mood and clear consciousness. The face of a person with mild stupor does not express emotions, the skin is pale, and the facial expression is sleepy. Often patients cannot remember events that happened to them and do not recognize friends and relatives. From time to time, patients come to their senses, accurately answer the questions posed, but the rest of the time they are in prostration.
First aid and therapy
When the first signs of stupor occur, the patient is recommended to provide first aid, which will have a positive impact on the effectiveness of further treatment of the pathological process. If an attack occurs indoors, it is recommended to provide fresh air. To do this, open the windows and doors in the room.
Read also: Death due to stroke
If a person is wearing restrictive clothing, it is removed or unbuttoned. It is recommended to constantly contact the patient - talk and ask questions . This will prevent him from completely shutting down. When the first signs of pathology appear, it is recommended to urgently call an ambulance.
If a person is diagnosed with a mild form of the pathological process, then he is recommended to take medications whose action is aimed at normalizing metabolic processes in the body. The use of Piracetam is most often recommended for patients. In case of stupor and coma, the patient is placed in the intensive care unit. The department recommends the use of a complex of resuscitation procedures.
Treatment of stupor is aimed at eliminating the cause of its occurrence - stroke. During the treatment of the pathology, swelling of the brain tissue is eliminated. It is also recommended to use techniques that maintain normal blood flow in the brain. During the treatment of the pathological process, it is recommended to adjust the blood sugar level. Patients are recommended to take vitamin therapy to replenish the lack of microelements in the body.
Patients are given medications whose action is aimed at restoring heart rhythm. If renal or liver failure develops, this requires appropriate therapy. After the patient is admitted to the hospital, the first step is to stop the bleeding in the brain using certain medications.
The prognosis of the pathological process directly depends on its causes and characteristics of its course. This is influenced by the timeliness of professional medical care. If the occurrence of stupor is observed against the background of an ischemic stroke, then the patient has a favorable prognosis. If the pathological process accompanies a hemorrhagic stroke, then in most cases there is a fatal outcome.
Danger of the syndrome
Any damage to the head, leading to even a mild stage of stunning, is a threat to life. Small changes in areas of the brain as it progresses lead to the death of nerve cells and death.
According to statistics, mild stunning is most often caused by drug or alcohol poisoning.
Stupor is observed after a cerebral hemorrhage, during inflammatory processes and traumatic brain injuries. The state of stupor can last for several months; it is not possible to predict whether a person will come out of it without complications.
To develop adequate treatment for patients in a coma, Swiss neurotraumatologists invented a scale that determines the level of consciousness. The analysis is carried out according to three key symptoms:
- opening the eyes;
- speech quality;
- physical activity.
Each sign is rated on a scale from 1 to 5, then the points are summed up:
- Highest score 15 points: clear consciousness.
- At 13, the diagnosis of “stun” is established.
- Up to 9 points the condition is perceived as stupor.
- Below 8 points – there is a comatose state.
Russian neurologists determine the level of consciousness using the Konovalov system:
- clear consciousness;
- stun;
- sopor;
- 3 stages of coma.
There is also the concept of “locked-in person syndrome”. Paralysis affects the entire muscular system, with the exception of the eyes. With absolute immobility, a person can only blink and move his eyes.
Regardless of the degree of impairment, a person with signs of deafness must be provided with first aid:
organize the air supply: open windows or take the patient out into the open;- unfasten buttons, loosen knots, unfasten belts;
- try to force the patient to answer questions, do not allow him to switch off completely;
- call an ambulance.
In mild cases of stunning, the patient is given drugs that normalize metabolic processes, the most famous representative of this group is Piracetam. Treatment of stupor and coma occurs in the intensive care unit and includes a complex of resuscitation procedures.
Clarity of consciousness is a determining factor in a person’s mental and physical health. Stunning is a dangerous symptom that can lead to paralysis, partial or complete loss of vision, hearing, and death. Periodically occurring numbness (tinnitus, dizziness, lethargy) can be an alarming symptom of a serious illness, so if suspicious signs are detected, you should contact a neurologist.
When does coma develop during a stroke?
The severity of a stroke depends on its form (hemorrhagic, ischemic), location and extent. More often, a coma occurs with a hemorrhagic stroke. Hemorrhage can occur both in the brain tissue and in the subarachnoid space. An ischemic stroke can be extensive and lead to a coma if there is a blockage of the large arteries supplying the brain.
Most often, a coma develops with a hemorrhagic stroke.
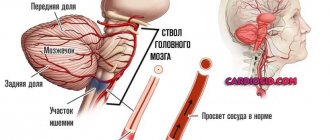
The location of the hemorrhage also matters; a stroke in the area of the brain stem is most dangerous for a person’s life, since vital centers that regulate the functioning of internal organs are located there. Almost 90% of patients with brainstem hemorrhagic stroke die immediately.
The coma may occur immediately or develop gradually over several hours. This is due to the fact that during hemorrhagic stroke and hemorrhage, the cells in the middle of the lesion are destroyed, and an inflammatory-necrotic process develops in them. The development of edema of brain tissue and secondary ischemic vascular spasm leads to dystrophic and inflammatory changes around the lesion.
Principles of treating stupor
A stuporous state, the consequences of which can be very severe, is not an independent phenomenon. It indicates a malfunction of the brain. Therefore, the goal of treatment should be to eliminate the underlying factor. In this case, therapy should be started as quickly as possible.
The trigger for stupor is often ischemia and swelling of the brain tissue. Early treatment prevents the brain from wedging into the natural openings of the skull and helps preserve the functionality of neurons.
Nerve cells in the penumbra (ischemic penumbra) are especially vulnerable. This is the area that is adjacent to the affected lesion in the brain. Incorrect treatment provokes an increase in symptoms due to the death of neurons in this area.
When treating stupor, the main actions are aimed at combating swelling of the nervous tissue and maintaining adequate blood circulation in the brain. The level of glucose in the blood is also corrected, the lack of microelements is compensated, and the causes of disturbances in the functioning of the heart, kidneys and liver are eliminated.
In case of infection, the use of antibiotics is indicated, and in the presence of hemorrhages, they resort to stopping the bleeding.
For stupor, all medications are administered intravenously into the body. In this case, the most effective drugs are glucose 40% and thiamine, as well as the use of these drugs with naloxone.
Further therapy for stupor depends on the degree of damage to the body and is prescribed by a doctor on an individual basis.
The main goal is to eliminate the cause that caused the disease. Lack of blood supply to the brain and its swelling can cause the death of neurons in the brain, and then an irreversible process begins in which a person slowly dies from the inside.
The doctor must immediately make a prognosis based on the data of tissue damage to the nervous system and adjust further actions. The sooner you seek help and begin treatment, the greater the chance for a full recovery the patient can have.
Patients in stupor require long-term care. From the very first day of treatment, you need to pay attention to the integrity of the skin in places where the body experiences the greatest stress in order to avoid bedsores in the future.
Move your limbs all the time without injuring the joints or causing pain; this is necessary so that the muscles do not lose tone and there are no contractures. To prevent bedsores, you also need to constantly change the position of the patient, turning him from one side to the other.
If the form of the disease is mild, then the patient can be fed in a sitting position in the usual way, if the form is severe, using a tube.
Typically, patients are administered vasodilators (papaverine, nicotinic acid) and dehydrating agents (glucose solution, aminophylline, magnesium sulfate, hypothiazide).
A prerequisite is compliance with bed rest.
Precomatose states during stroke
When a coma does not develop immediately, but over several hours, signs of its development can be noted:
- the patient is conscious, but does not seem to understand what is happening to him, he is stunned;
- he complains of pain in his head, he feels sleepy;
- there is an increase in temperature;
- general weakness, impaired movement in the limbs, their coordination;
- speech disorder;
- partial memory loss;
- delirium, confusion;
- vomiting, sometimes convulsions.
Often a precomatose state is accompanied by memory loss
These are the symptoms of so-called precomatose states:
- Stupor. State of stun, lack of understanding of what is happening.
- Somnolence. A state reminiscent of sleep, but the patient’s eyes can be open, with great difficulty you can rouse him, but he immediately stops reacting to others again.
- Sopor. It is not possible to wake the patient, but his corneal and swallowing reflexes are preserved, and he can open his eyes.
Unfavorable signs during the development of a coma are: different diameters of the patient’s pupils (anisocoria), poor reaction to light and the “doll’s head and eyes” symptom.
This reflex, also called oculocephalic, occurs when the patient's head is turned to one side and the eyes move in the opposite direction. This indicates damage to brain stem cells.
Some authors do not distinguish precomatose states, but consider them to be the first degree of coma. Already with the development of a precomatous state, the patient’s chances of survival are significantly reduced and amount to 30–85%.
Stages of development of coma
Coma is a complete absence of consciousness in a patient with a stroke; there are 4 degrees of coma, which differ in the level of muscle tone of the patient, the presence of reflexes, and the state of the functions of internal organs.
| Degree | Muscle tone | Reflexes | Functions of internal organs |
| 1 | Muscle tone is increased, the patient reacts to pain, can turn or move a limb that is not affected by paralysis, and suddenly open his eyes. | The swallowing reflex and the reaction of the pupil to light are preserved, and divergent strabismus may be observed. | Usually no changes are observed. |
| 2 | The patient does not respond to painful stimuli; there are movements in the muscles, but they are chaotic and not coordinated (spasms, fibrillation). | The pharyngeal reflex is preserved, but the reaction of the pupils to light decreases, pain reflexes are absent, and pyramidal reflexes may appear. | Pathological types of breathing appear: Kussmaul, Cheyne-Stokes. Breathing can be noisy, periodic, and stridorous. |
| 3 | Muscle tone is reduced, but not in all muscles. It depends on the location of the damage to the brain cells. Convulsions are possible. | The pharyngeal reflex is depressed, the reaction to light and the corneal reflex are absent. Tendon reflexes are reduced and indicate the location of the stroke. | Spontaneous urination and bowel movements are observed. The pressure drops, breathing is weak and irregular. Body temperature decreases. |
| 4 | The pupils are dilated. | Impaired heart function, often causing respiratory arrest. |
The higher the degree of coma, the less chance that a person can come out of it. Already at grade 3–4 it is minimal.
The patient's corneal reflex can be determined using a small piece of gauze or cotton wool. You need to touch the cornea, but not in the pupil area. The touch causes the eyelids to close. Its absence indicates damage to the brain stem.
The length of stay in a coma also matters. According to studies, if a coma lasts 4 months, even at stages 1–2, the probability of exiting it is reduced to 12–15%. Cases have been described where consciousness is restored even after a year, but this is rare.
What is stupor and how to treat it?
For a person, the state of wakefulness is considered normal . It indicates that the patient does not have any abnormalities in the work and functioning of the brain. But sometimes pathologies and diseases arise that can provoke a blackout. It is important to take into account the fact that in this case there is no change in consciousness, it is only slightly depressed.
Stupor is considered a quantitative impairment of consciousness. If a patient has a soporosis disorder, it is urgent to conduct a thorough diagnosis and establish the cause of this condition, since these factors have a negative impact on the condition of the brain.
Syndromes of depression of consciousness
Impaired consciousness is expressed in quantitative and qualitative changes.
Towards quantitative syndromes
disturbances (depression) of consciousness include: stupor, stupor, coma.
Quantitative disturbances of consciousness (depression of consciousness) develop due to morphological or pronounced metabolic changes in the brain, and are accompanied by a decrease in the level of wakefulness, motor activity, intellectual functions, up to complete depression and switching off of consciousness.
Stupor - what is it?
Stupor or stuporous disorder is a sign that the function of the cerebral cortex is impaired and inhibitory forms predominate in the human body.
This condition can occur when:
- various disorders and damage to nervous tissue;
- brain hypoxia;
- due to exposure to medications or substances produced in the body.
Stupor is a deep depressed consciousness of a person, which is manifested by a drowsy state. Depressed voluntary activity is also noted, but reflex activity is not affected.
This condition is diagnosed by the following signs:
- slight reaction of the pupils to light stimuli;
- a defensive reaction to pain occurs.
Sopor
Stupor is a deep depression of consciousness in which the victim retains coordinated defensive reactions, opening the eyes in response to stimuli. The victim lies with his eyes closed; he can be briefly brought out of a drowsy state. In this case, the patient is motionless or makes automatic stereotypic movements, reaching with his hand to the place of application of painful irritation, and a painful expression on his face may appear as a pain response.
Coma is a complete shutdown of consciousness without any signs of mental life, while the victim cannot be brought out of this state with the appearance of any signs of mental activity.
- Moderate coma
(coma I) - the victim has a preserved reaction to painful stimuli (flexion and extension movements of a dystonic nature), while protective motor reactions are not coordinated, the patient does not open his eyes, pupillary and corneal reflexes are preserved, abdominal reflexes are depressed, tendon reflexes are variable. Increased pathological foot reflexes and reflexes of oral automatism. - Deep coma
(coma II) - there are no reactions to external stimuli, various changes in muscle tone are observed, spontaneous breathing and cardiovascular activity are preserved even if they are severely impaired. - Terminal coma
(coma III) - bilateral mydriasis, diffuse muscle atonia, severe disturbances of vital functions, respiratory rhythm and frequency disorders, apnea, tachycardia or bradycardia, blood pressure is not determined.
Stupor during stroke
Soporous disorder occurs in patients after a stroke, in most cases after a hemorrhagic stroke. Depending on which area was affected and where the source of the stroke is located, stupor may develop directly during the recovery period.
The patient in such a situation does not have any motives or desires; his condition does not seem strange to him. Therefore, it is necessary for the patient after a stroke to pay due attention so as not to miss and recognize the pathology in time. Find out what causes a stroke from our similar article.
It is worth understanding that if you miss the moment of manifestation of stupor, the patient may experience a coma, which, in rare cases, results in positive results.
A soporous disorder does not always occur during a stroke ; prerequisites are needed for this. This condition can be caused by various disorders and complications after illnesses, overdose of sedatives.
Stupor may appear with some frequency, sometimes loss of consciousness lasts for several seconds. But even a couple of seconds can provoke coma and, as a result, death.
Caring for a comatose patient
As long as the patient is in a comatose state, his care must be careful. He is prescribed drugs that improve the state of cerebral circulation, neuroprotectors, antihypertensive drugs, and therapy against cerebral edema (diuretics, corticosteroids, plasma-substituting solutions).
A patient in a coma must receive the necessary nutrition to maintain the body's vital functions.
The patient needs to be fed so as not to bring the body to exhaustion. In stages 1–2, when the swallowing reflex is preserved, food can be given with a spoon, then when it is weakened or suppressed, it is necessary to introduce nutrients through a tube or parenteral nutrition is prescribed.
The possibility of exiting a comatose state depends on care, since if the patient is not cared for sufficiently, complications may arise (bedsores, congestive pneumonia), which, if an infection occurs, can lead to death.
Why does stupor occur?
Many serious illnesses and injuries can provoke stupor Temporary loss of consciousness can also occur due to head injury, as a result of which there is a decrease in blood flow in the brain, and even convulsions may occur.
Prolonged loss of consciousness occurs for reasons such as:
- Serious illnesses.
- Toxic effects of drugs on the body.
- Overdose of sedatives.
Also, a negative impact on the functionality of the brain.
The main reasons due to which soporous disorder occurs
- Neoplasms and abscesses in the brain.
- Brain hemorrhage
- injuries .
- Acute hydrocephalus.
- Stroke.
- Hypertensive crisis, which is characterized by a severe form.
- Vasculitis , damaging the central nervous system.
- Poisoning with toxic substances
- hypothermia or heatstroke here.
- Infectious diseases
- Sepsis.
- Metabolism problems
- Hypothyroidism.
- Metabolic disorders
- Disorders of water or electrolyte metabolism.
- Severe heart
How long does stupor last?
Stupor is a serious disorder that is not always possible to recognize. The patient's depressed state can last from a few seconds to several days, then the patient falls into a coma.
The symptoms of this disorder appear simultaneously with the signs of the main disease. The severity of stupor will depend on the degree of disturbance in the functioning of the central nervous system .
Soporous disorder can be compared to sleep: the patient stops moving, the muscles are not tense. If sharp sound stimuli arise, the person reacts - opens his eyes, but then immediately closes them.
You can only get out of this state by applying pain , but only for a short time. The patient may even resist.
As for human sensations in this condition, they are dull. The patient is unable to answer the question and respond to requests. He is not interested in the surrounding changes. The tendon reflexes are dulled, and the pupils have the same reaction to light stimuli. Breathing and swallowing are not impaired.
Read also: Bulbar stroke
It happens that the patient experiences incoherent muttering and incomprehensible movements; in such a situation, contacting the patient is simply useless .
Also, this condition may be accompanied by the following symptoms, which indicate damage to certain brain areas:
- Cramps and increased muscle tone in the neck are observed with intracranial hemorrhage.
- Paralysis and paresis are observed with damage to the pyramidal system.
Consequences of a stroke
All people susceptible to diseases of the cardiovascular system are afraid of stroke, an acute disorder of cerebral circulation, the consequences of which can be very serious.
Let's name some of them:
- A state of stupor or complete absence of consciousness.
- Changes in the frequency, depth and rhythm of breathing, until it stops.
- Increased heart rate, drop in systemic blood pressure. Cardiac arrest is possible.
- Involuntary bowel movements.
Neurological disorders:
- Pronounced facial asymmetry: unilateral drooping of the corner of the mouth, smoothness of skin folds in the nose area, on the forehead.
- Lack of speech or slurred words. Misunderstanding of spoken speech.
- Visual impairment - both eyes or one.
- Complete or partial paralysis of the limbs (usually unilateral), accompanied by an increase in the tone of the striated muscles
- Cramps.
Brain infarction
There are two types of stroke: hemorrhagic and ischemic. Ischemic is also called cerebral infarction.
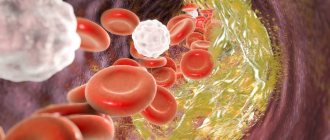
In an ischemic stroke, the arteries supplying the brain become blocked by a blood clot. Most often it occurs in people suffering from atherosclerosis, as well as with hypertension and atrial fibrillation. After an attack, a person’s physical and emotional state undergoes changes, and he changes his behavioral characteristics.
A person experiences stress, since the stroke itself is a devastating blow to the nervous system. Loss of control over the body, deterioration of memory and vision (up to loss) - all this is rejecting, causing irritation, anger, tearfulness, and aggression. The attention and care of loved ones is often met with hostility.
What causes disruption of vital functions
Violation of important functions after a stroke is caused by the loss of conductivity of brain cells - neurons. It is the conductivity of neurons that gives a person the opportunity to coordinate his movements, speak correctly, think actively, and so on. The same factor prevents the body from recovering after an attack.
Neurons die as a result of lack of delivery of blood and oxygen to the brain. The development of ischemic and hemorrhagic strokes is provoked precisely by vascular damage.
Brain after stroke
The number of cases of cerebrovascular accidents increases with age. People with a sedentary lifestyle are especially vulnerable in this regard.
The brain requires a constant supply of very large volumes of oxygen. This is due to the high metabolic rate. Compare: the mass of the brain relative to the entire mass of a person is quite small - 2%. But the oxygen and glucose entering the human body go to nourish the brain in significant quantities - 20 and 17%, respectively.
Since the brain does not have spare oxygen reserves, even with local anemia (ischemia), if it lasts more than five minutes, damage to its nerve cells occurs, and irreversible damage occurs.
During a stroke, some cells are damaged and some die. In the acute period, large areas of damaged cells are observed, which is also affected by edema. After a few weeks, when the exacerbation subsides, the area of damage decreases.
Shards of memory
Apoplexy causes a serious blow to a person's cognitive functions. First of all, from memory, partial or complete loss. A person may not remember his loved ones or his name.
Memory after a stroke is like a fragile vessel: it is either about to crumble, or has already broken up into small fragments that the sick person is unable to put back together.
About whom you can read the article given here.
Impact on vision
In addition to functional disturbances in the functioning of the body, a stroke is also accompanied by significant structural changes in the brain. Very often vision restoration is required.
A sudden deterioration in vision, by the way, is often a harbinger of apoplexy. It happens when the flow of blood is interrupted for even a minute. Visual impairment and headache are observed from the first minutes of the attack.
A stroke usually causes irreversible damage to the functioning of the body. With cerebral embolism and thrombosis, it can cause complete loss of vision. With relapse of mild ischemia, vision problems are often short-term in nature.
Paralysis after stroke
Paralysis and paresis are the most common consequences of strokes. They hit different places. It depends on where the brain damage is located. If the left lobe is affected, paralysis of the right side of the body or part of it will occur. And vice versa.
The statistics are impartial and inexorable: half of people who have had a stroke survive. And 50% of survivors remain disabled. Death occurs more often when hemorrhage occurs in the right hemisphere. Damage to the left side and paralysis of the right side of the body is considered a more favorable outcome and is better tolerated by patients.
The severity of paralysis of the right side depends on the location and extent of the brain lesion. Some people become deaf and blind, but can move and speak; someone retains communication functions, but loses motor activity; and the third was simultaneously hit by all the negative consequences of the stroke.
For unknown reasons, stroke kills cells in the left hemisphere more slowly. Therefore, the right side of patients recovers faster.
Signs of a soporous state
- A person with stupor seems to be sleeping, but may have some reaction to a strong irritant. If a sharp sound occurs, the patient’s eyes react – they open, but do not look for the source.
- If you press on the nail, the patient will withdraw his hand. A strong negative reaction may occur to the injection, but it is quite short-lived. The patient may even begin to swear or fight.
- If you conduct a general examination, you will notice decreased muscle tone and suppressed deep reflexes. There may be pyramidal signs due to decreased central motor neuron input.
- Focal neurological symptoms may also be observed in parallel , which will indicate local damage to structures and areas of the brain.
- If the stuporous state was provoked by hemorrhage inside the skull, then stiffness of the neck muscles and other meningeal symptoms will be noted. There may also be cramps and muscle twitching. Read more about the symptoms and treatment of cerebral hemorrhage.
- The patient may also experience hyperkinetic stupor - the patient mutters something to himself, makes unfocused movements.
Level of consciousness during stupor
As for the consciousness in such a situation, the patient is quite cloudy , and he is not able to answer any questions, the reaction is short-lived even to strong stimuli.
Stunning after a stroke: features of pathology – Nerves
With the development of a cerebral coma, a person completely loses contact with the outside world. This condition occurs after a hemorrhagic stroke or an extremely severe ischemic stroke.
The onset of extreme coma means brain death. Milder degrees may result in the restoration of consciousness or the transition to vegetative regulation of vital processes.
The prognosis for recovery is usually poor.
Read in this article
Signals from the outside world enter the brain through a special network of neurons called the reticular formation. It is responsible for the level of wakefulness, processes of excitation and inhibition in the central nervous system. During a stroke, this connection is destroyed due to:
- increased intracranial pressure;
- swelling of brain tissue;
- direct damage to stem cells;
- extensive focus of ischemia or hemorrhage in the cerebral hemispheres.
The most common cause of coma is a hemorrhagic stroke; it can begin with a severe loss of consciousness with a fatal outcome. Some patients experience a gradual progression of symptoms - from a state of stupefaction to the cessation of reaction to the environment.
Hemorrhagic stroke
The ischemic form of acute cerebrovascular accident leads to a coma only when a large arterial branch is blocked. Such patients, as a rule, have a recurrent stroke, there is no collateral (bypass) blood supply network, and widespread atherosclerotic vascular damage is noted.
And here is more information about hemorrhagic stroke of the brain.
Symptoms are determined by the degree of inhibition of higher nervous activity. Depending on the depth, there are several types of this severe stroke complication.
- confused consciousness
- stunned,
- the patient is inhibited or excited,
- there may be mental disorders;
- stupor,
- reaction to irritations is slow, reduced,
- the patient can drink, move, but does not respond to speech addressed to him,
- high muscle tone,
- the pupils narrow when light is directed at them, but the eyes diverge to the sides, “float”,
- skin reflexes are very weak;
- sopor,
- movements are rare and chaotic,
- there is no coordination,
- breathing is noisy, deep,
- involuntary release of urine and feces,
- pupils are narrow, there is practically no reaction to light,
- there is a response to irritation of the cornea and pharynx,
- twitching of individual muscle fibers,
- after tension, the muscles relax and periodically spasm;
- there is no consciousness, all types of reflexes,
- pupil less than 2 mm,
- low muscle tone, periodic cramps,
- involuntary physiological recoveries,
- blood pressure is sharply reduced,
- breathing is rare, not rhythmic, shallow,
- skin is cold;
- means brain death
- no reflexes, muscle tone,
- wide pupil,
- breathing stops
- pressure and pulse in large vessels are not determined.
The duration of the comatose state is very individual. It depends on the location and size of the focus of brain destruction, as well as the presence of concomitant heart lesions and the age of the patient.
The minimum duration is 1 - 2 hours, and the maximum lasts several years with the transition of patients into a vegetative state, in which there is no activity of the cerebral cortex, but autonomic reflexes are preserved.
Despite the fact that after 6 months the patient’s return to full consciousness is practically impossible, he continues to be considered a living person who needs to maintain breathing and heartbeat. The longer the period of coma, the less chance of subsequent normalization of brain function.
Cerebral hemorrhage usually occurs in a more severe form. The mortality rate in such patients reaches 70%; even after removal of the hematoma, the rate is not much lower. Unfavorable factors include:
- breakthrough of blood into the ventricles of the brain;
- uncontrolled arterial hypertension;
- large volume of hematoma;
- progressive cerebral edema;
- signs of displacement of the stem part;
- acute heart failure;
- increase in creatinine content in the blood;
- convulsive syndrome, lack of consciousness, reactions to painful stimuli for more than 3 days;
- age after 70 years.
With ischemic stroke, a more benign course is observed; it is rarely accompanied by a profound impairment of consciousness. This happens with repeated vascular accidents, massive blockage of the brain arteries with cholesterol plaques, lack of treatment or complete disregard of doctors’ recommendations.
- Blockage of arteries in the brain
- Precoma and the first degree of coma can still give the patient a chance for recovery; with a higher degree, the prognosis is considered doubtful, and the onset of extreme coma is usually regarded as fatal.
- The prognosis for the recovery of brain activity in old age is much worse. After regaining consciousness, patients usually retain a neurological defect in the form of:
- decreased vision;
- loss of sensitivity;
- motor disorders - paralysis, convulsions, hyperkinesis;
- abnormal reflexes;
- disorders of speech function, mental health;
- persistent loss of memory, ability to self-care.
However, a final conclusion about the consequences of a coma after a stroke can only be made on the basis of a complete diagnosis, which includes ultrasound of the vessels of the head and neck, MRI or CT of the brain in combination with angiography.
If intensive resuscitation measures are started in time, a successful operation is carried out, and the lesion does not spread to neighboring areas, and cerebral edema is managed, then the patient begins to come to his senses. The process of restoring lost functions occurs in the reverse order:
- first the eyes open, the pupil reacts to light, the corneal reflex;
- the ability to swallow and feel pain appears, the patient can follow the movements of people or objects with his eyes;
- consciousness goes through the stages of stupor and stupor, delirium and hallucinations are often noted;
- convulsive seizures are possible;
- if the course is favorable, contact with surrounding people is restored.
The transition from a coma to a vegetative state is accompanied by the opening of the eyes to flashes of light, loud sounds, the patient may groan, but he does not have a conscious response to stimuli. The grasping, chewing and swallowing reflexes are preserved. Due to complete immobility, pneumonia, bedsores, and urinary infections often appear.
Restoration of brain functions (before the period of its complete death) occurs due to the following processes:
- transformation of stem cells into neurons;
- regrowth of processes of surviving cells;
- replacement of lost functions by neighboring areas of the brain.
And here is more information about brainstem stroke.
Coma after a stroke develops in patients with extensive damage, more often with hemorrhage in the brain, signs of edema and dislocation of the brainstem. This complication has four degrees of severity, which further determine the prognosis for brain recovery. It is less favorable in older people.
Recovery from a coma occurs within an hour or several years. In this case, there may be a gradual awakening of consciousness or a transition to a vegetative state.
Source:
State of deep stunning during stroke
There are many different diseases that lead to impaired consciousness. Before touching on the causes of disorders of consciousness, we should briefly dwell on the brain structures responsible for the state of clear consciousness.
Types and symptoms of consciousness disorders
Based on the depth of the disturbance of consciousness, coma, stupor and stupor are distinguished.
Coma is an extreme degree of impairment of consciousness:
- there are no reactions to irritations (speech, pain);
- there is no sleep-wake alternation;
- eyes closed.
Stupor (in foreign literature the term stupor is more often used) is a milder degree of impairment of consciousness compared to coma. For stupor:
- the patient cannot be completely awakened, but there is a reaction to pain (a non-directional protective motor reaction is preserved, for example, withdrawing a hand when painful stimulation is applied to it);
- the reaction to speech is either weak (with mild stupor) or absent;
- after a short awakening (with mild stupor), the patient quickly falls back into an unconscious state and does not remember the moments of awakening in the future.
- Stunning is a state of incomplete wakefulness, which is characterized by loss or disruption of varying degrees of severity of the coherence of thoughts and actions due to a severe disorder of attention, drowsiness.
- Stunning should be distinguished from delirium (the most common cause of which is alcoholism), in which stunning is combined with psychomotor agitation, delirium, hallucinations, and activation of the sympathetic nervous system (increased blood pressure, sweating, tremors, tachycardia).
- In coma and deep stupor, in addition to impaired consciousness, other symptoms are observed:
- Disruption of the normal breathing rhythm; in severe cases, breathing becomes chaotic; Respiratory depression may even occur.
- Impaired reaction of the pupils to light.
- Disturbed eye movements (observed when lifting the eyelids): or floating movements, fixation of gaze.
- A variety of pathological activity can be observed: epileptic seizures, muscle twitching (myoclonus), parakinesis (involuntary movements reminiscent of voluntary ones in nature - according to the popular expression: “before death”).
- There may be a sharp increase in muscle tone or, conversely, a decrease (“atonic coma”).
Glasgow scale
- Opening for speech - 3
- Opening to pain - 2
- Follows a verbal command - 6
- Localizes pain - 5
- Withdrawals a limb with flexion in response to pain - 4
- Pathological flexion of all limbs from pain (decorticate rigidity) - 3
- Pathological extension of all limbs from pain (decerebrate rigidity) - 2
- No movement - 1
- Preservation of verbal responses
- Oriented and talking - 5
- Confused speech - 4
- Says incomprehensible words - 3
- Inarticulate sounds - 2
The total score is the sum of the scores of the three groups. 15 points - clear consciousness, - slight stun, - severe stun, 10-8 - stupor, 7-6 moderate coma, 5-4 - deep coma, 3 - death of the brain, extreme coma.
Diagnostics
It is important to establish not only the degree of impairment of consciousness, but also its cause. In addition to the medical history, which may remain unknown either in the absence of the patient’s relatives or due to their ignorance, additional research helps clarify the diagnosis.
- Blood and urine tests - general analysis, analysis of glucose levels in the blood, urine, levels of electrolytes, creatinine, calcium, phosphates in the blood, biochemical indicators of liver function, blood osmolality.
- Screening of toxic substances (carried out in specialized toxicology laboratories).
- Chest X-ray
- X-ray of the skull (if TBI is suspected)
- CT and MRI of the brain, revealing the presence of stroke, consequences of TBI (brain contusion, subdural hematoma, epidural hematoma, confusion of brain structures), encephalitis.
- Lumbar puncture followed by examination of the cerebrospinal fluid if meningitis or subarachnoid hemorrhage is suspected.
- Electroencephalography (EEG), which makes it possible to distinguish coma from mental “reactivity (with hysteria, catatonia).
Surveys
If the patient has impaired consciousness, then first of all it is necessary to determine the level of depression, differentiate stupor from coma, as well as from stunning. The main study is aimed at identifying the cause that disrupts brain activity, and also identifying parallel metabolic disorders.
After the patient is admitted to the hospital, the specialist tries to find out what preceded this condition. It is necessary to study the patient’s medical card and interview relatives. The victim’s personal belongings are examined to determine the presence of any drugs.
If the diagnosis of stupor has been confirmed, then a number of screening studies are performed:
- Inspect the body for any rashes or hemorrhages.
- is imperative to measure blood pressure and monitor its changes.
- Temperature is being
- is donated for sugar and alcohol.
- ECG and cardiac listening.
also required to determine the main indicators and electrolyte levels. If there is a suspicion that the patient has been poisoned, a toxicological study should be performed. Urine is tested for the presence of toxic substances. A lumbar puncture and an MRI or CT scan may also be prescribed .
Coming out of a coma
The patient’s exit from a coma is accompanied by a reverse development of symptoms, that is, first reflexes (pharyngeal, corneal) are restored, then muscle movements, and only then consciousness and speech appear.
If a patient with a stroke develops a coma, the prognosis in most cases is unfavorable. Even when recovering from a coma due to a stroke, the patient requires long-term rehabilitation over several years, or complete disability occurs. In the event of a stroke, only timely medical assistance can help. Therefore, at the slightest suspicion of cerebrovascular accident, call an ambulance.
Materials used in the article:
https://oinsulte.ru/travmy-golovy/chmt/oglushennost.html
https://golovalab.ru/insulto/simptomy/stepeni-komy-pri-insulte.html
https://lechiserdce.ru/gemoglobin/7720-totemu-dlya-gemoglobina.html
Post Views: 1,760