Arachnoiditis of the brain, the symptoms of which can have varying degrees of severity, is an inflammation of one of the membranes (the so-called arachnoid) of the brain. This disease can cause permanent disability. This danger makes the problem of timely diagnosis and comprehensive treatment of the disease urgent.
Characteristic features of cerebral arachnoiditis include a decrease in the rate of blood outflow and an increase in the permeability of capillary walls. The combination of these factors leads to the development of congestion in the soft tissues. These features largely determine the clinical picture of the disease.
Causes
In every second case, the cause of arachnoiditis is infectious diseases or purulent focal inflammation (meningitis, tonsillitis, influenza, otitis media), in every third case it is a traumatic brain injury (hemorrhage, brain contusion), and in every tenth case the exact origin of the pathology cannot be established .
But doctors identify risk groups, belonging to which increases the likelihood of developing arachnoiditis:
- if a person lives in a state of constant stress, moral fatigue and emotional exhaustion;
- if he very often suffers from acute respiratory diseases;
- if a person lives in harsh climatic conditions, for example, in the Far North;
- if his work involves heavy physical labor;
- if the body is under constant chemical or alcohol intoxication.
Sometimes the cause of the disease is pathology of the endocrine system and metabolic disorders.
Etiology of the disease, causes
It is impossible to single out one cause of the disease. Arachnoiditis of the brain can be either an independent nosology or a consequence of a previously suffered inflammatory process .
Most often it is provoked by tonsillitis, rheumatism, chronic inflammatory processes of the ENT organs, childhood infections that occur in adults, and traumatic brain injuries.
A number of cases have been described in which arachnoiditis manifested itself against the background of chronic intoxication with salts of heavy metals, oncology of the brain or spinal cord.
This disease was first classified and given its modern name in 1845, thanks to the work of A. T. Tarasenkov. It is also worth noting that the World Health Organization, when revising ICD-10, does not allocate a separate code for arachnoiditis, but classifies it as meningitis.
Pathogenesis
In the arachnoid membrane of the brain, reactive inflammation occurs as a result of exposure to a pathogen or its toxins, as a result of which there is a violation of lymph and blood circulation. There are several types of disease depending on the location and nature of the changes - these are cerebral, cystic, adhesive, adhesive-cystic and spinal arachnoiditis. The disease can have an acute, subacute or chronic course.
As a result of impaired circulation of the cerebrospinal fluid, in some cases the development of hydrocephalus may occur:
- occlusive hydrocephalus occurs as a result of impaired outflow of fluid from the ventricular system of the brain;
- Aresorptive hydrocephalus can develop as a result of impaired absorption of fluid through the dura mater due to the occurrence of an adhesive process.
[adsen]
Diagnosis of brain arachnoiditis
In most cases, obvious signs of cerebral arachnoiditis, which can be called dizziness, frequent headaches with regular nausea and vomiting, do not cause suspicion in the patient. At the initial stage, they appear several times during the month and only when the disease becomes chronic do they occur quite often and last a long time, so they force a person to seek medical help.
The difficulty is that the symptoms of developing arachnoiditis are characteristic of a large number of ailments, so treatment is often delayed. To make an accurate diagnosis, the doctor will need to conduct a number of examinations:
- Ophthalmological examination. The most common type of disease is opticochiasmatic arachnoiditis. Approximately half of patients have signs of posterior fossa involvement.
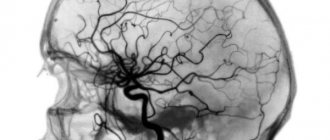
- Magnetic resonance imaging. This research method makes it possible to determine the presence of inflammation in the brain in 99% of cases. The examination reveals the presence of cysts and inflammation in the arachnoid membrane of the brain. It also allows you to exclude other pathologies that have the same manifestations (abscess, tumor, etc.).
Accumulation of cerebrospinal fluid in the convexital space. Cerebral arachnoiditis on MRI in T2 mode
- A clinical blood test makes it possible to determine the inflammatory process in the body and the presence of infection in it. It is also possible to identify an immunodeficiency state, that is, to detect the main causes of the development of the disease.
- Radiography makes it possible to diagnose intracranial hypertension.
- Consultation with an otolaryngologist is indicated for people with manifestations of hearing loss.
- Lumbar puncture allows you to determine the level of intracranial pressure. In the case of development of brain arachnoiditis, an increased amount of protein and neurotransmitters can be detected in the cerebrospinal fluid.
Only after a comprehensive examination and accurate diagnosis will the doctor be able to prescribe the correct treatment.
Classification
According to the nature of the course, the disease is divided into three forms: acute, subacute and chronic. Depending on the form in which the pathology occurs, one or another symptomatology will be visible.
According to the location in the brain, the following types are distinguished: localization of zones
- the spinal type occurs on the posterior surface of the spinal cord membrane, is formed as a result of injury, and may appear after some time.
- cerebral arachnoiditis, formed on the convex surface of the brain in the postcranial fossa/
Cerebral arachnoiditis, in turn, is divided into subtypes:
- arachnoid cyst of the posterior cranial fossa;
- arachnoiditis of the cerebellopontine angle.
- basilar;
- convexital;
Also, retrocerebellar arachnoiditis can be:
| Adhesive type | is a purulent inflammation of the lining of the brain with the formation of adhesions that cause severe pain. |
| Cystic-adhesive mixed type | with it, both adhesion of brain tissue and the formation of cystic growths are observed. |
| Cystic type | It is also characterized by inflammation of the lining of the brain, only with additional formation of cysts against the background of the disease. |
Classification and symptoms of the disease
There are several types of arachnoiditis:
- True. The cause of this pathology is an autoimmune process or an allergic reaction. Typically, this form of arachnoiditis is considered common, as it can affect the upper cellular layer of the cerebral cortex. This lesion is quite rare, occurring in only 5% of cases of all diseases of the meninges.
- Residual arachnoiditis is triggered by injury or infection that affects the nervous system. The result of this pathology is the appearance of adhesions and cysts filled with cerebrospinal fluid.
The disease can also be classified according to the predominant changes in the subarachnoid space:
- Cystic arachnoiditis. Fibrous tissue grows between the membranes, which provokes the formation of cavities filled with cerebrospinal fluid.
- Sticky. In this case, effusion forms, as a result of which loose adhesions develop. They interfere with the circulation of cerebrospinal fluid.
- Mixed. This is a combination of symptoms and features of the course of the two previous types of arachnoiditis.
If we take the localization of the pathology as the basis for the classification, then it can be:
- Diffuse (extensive). It is diagnosed in most cases, since the inflammatory process spreads to almost the entire membrane and also affects neighboring tissues. Symptoms are not clearly expressed. There are general cerebral signs caused by impaired circulation of the cerebrospinal fluid.
- Limited. Such arachnoiditis is rare, because the arachnoid membrane does not have clear boundaries, so inflammation affects most of it.
- Convexital. Arachnoiditis spreads to that part of the membranes that is located on the outer surface of the brain. Its course is considered easier. However, it is accompanied by epileptic seizures, emotional disorders, paralysis and paresis.
- Basal. It is localized at the base of the skull and affects the brain stem, nerves and cerebellum. Here vision is impaired, on both sides. First, the visual field changes to some colors (red and green). In addition, intense headache appears and the functions of the oculomotor nerves are disrupted. When examining the fundus, optic nerve atrophy is visible.
- Posterior cranial fossa. There is a great variety of symptoms. If the nerves of the skull are damaged, hearing loss and damage to the trigeminal nerve may occur. If inflammation affects the cerebellum, then there is a disorder of coordination and motor skills. The patient also has severe hypertensive syndrome.
The last classification parameter is the rate of development of the pathological process. Here are the following types:
- Spicy. If arachnoiditis develops very quickly, the patient’s temperature rises greatly and vomits profusely. However, this form of pathology can be cured quickly, without serious consequences.
- Subacute. The pathology is constantly progressing, sometimes exacerbating, sometimes fading. With cerebral arachnoiditis, symptoms increase slowly. First, asthenia, severe weakness and fatigue, moderate headache, problems with emotional background, and increased irritability appear.
- Chronic. Over time, the inflammatory process progresses, and the person develops focal and cerebral symptoms. For example, the headache intensifies, nausea and vomiting are noted, and the eyes begin to hurt. The patient develops tinnitus and his fingertips turn blue. He is constantly thirsty and has high sensitivity to bright lights and loud sounds.
The patient often experiences sleep and memory disturbances, and anxiety. There are other symptoms: sensitivity to weather changes, excessive sweating, excessive urination, loss of smell (total or partial).
Course of inflammation
In most cases, the disorder does not lead to severe pain or fever, which complicates diagnosis and causes late consultation with a doctor. But there are also exceptions.
- Acute course - observed, for example, with arachnoiditis of the cistern magna, accompanied by vomiting, fever and severe headache. This inflammation can be cured without consequences.
- Subacute – observed most often. In this case, mildly expressed symptoms of a general disorder are combined - dizziness, insomnia, weakness, and signs of suppression of the functionality of certain parts of the brain - hearing impairment, vision, balance, etc.
- Chronic – if the disease is ignored, inflammation quickly passes into the chronic stage. At the same time, the signs of a general cerebral disorder become more and more stable, and the symptoms associated with the source of the disease gradually intensify.
Symptoms of pathology
Signs by which a doctor may suspect a disease are a set of symptoms of a cerebral disorder. However, there are also symptoms characteristic of arachnoiditis:
- Headache in some cases accompanied by nausea and even vomiting. It mainly bothers the patient in the morning. The pain is local. After any effort (sudden movement, straining, etc.), its manifestations intensify.
- Dizziness.
Read more about the causes of dizziness. We'll tell you what can make you feel dizzy.
- General weakness of the body.
- Sleep disorders.
- Memory impairment.
- Increased irritability.
Dr. Myasnikov Alexander Leonidovich in the program “About the Most Important Thing” will talk about the most alarming clinical causes of sharp and severe headaches:
As a rule, during the disease the entire surface of the arachnoid membrane becomes inflamed. In the case of limited arachnoiditis, disturbances occur in a separate area. Depending on where the source of the disease is located, the following symptoms are possible:
- The convexital type of arachnoiditis is manifested by irritation of the brain. In this case, the patient may experience seizures similar to epileptic ones.
- If the swelling is more developed in the occipital region, hearing and vision impairment occurs. The patient notes loss of the visual field, and during an examination of the fundus, the doctor may note optic neuritis.
- The patient reacts sharply to changes in weather. At the same time, he experiences excessive sweating or chills. In some cases, a person complains of a constant feeling of thirst. Sometimes there is an increase in body weight.
- When the cerebellar angle is damaged, pain occurs in the occipital part of the head, dizziness and tinnitus. There is an imbalance.
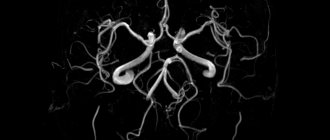
The figure shows the largest cisterns of the subarachnoid space. Depending on the location of the inflammation, the patient experiences different clinical manifestations of the disease.
- Cystic arachnoiditis can have various manifestations, which are associated with the nature of the adhesions. If it does not lead to an increase in ICP, the disease may not be detected for several years. During this time, balance gradually deteriorates and synchronization is lost.
- When the anterior lobes of the brain are damaged, memory decreases, the patient’s psychological state is disrupted, convulsions and various mental abnormalities appear.
- It is very difficult to identify adhesive cerebral arachnoiditis, since it is not characterized by localization of manifestations, and the symptoms are similar to those of many diseases.
- If arachnoiditis affects the occipital cisterns, then signs of damage to the facial nerve appear. The patient's body temperature rises.
Read about the main causes of Bell's palsy (inflammation of the facial nerve) in a detailed article.
It is worth noting that cerebral arachnoiditis does not develop spontaneously. From the moment of an infectious disease to the appearance of the first symptoms, at least several months or even 1 year can pass. In case of injury, the disease can make itself felt only 2 years after brain damage. Phases of exacerbation of the disease are always followed by periods of remission.
The onset of the pathology is subacute. The patient complains of irritability, headache or dizziness, constant weakness and fatigue. Over time, as the inflammatory process progresses, focal or cerebral signs of the disease appear.
Neurologist Mikhail Moiseevich Shperling talks about the symptoms of increased intracranial pressure:
This disease is characterized by the formation of adhesions and fusion of the membranes of the brain, as a result of which the outflow of cerebrospinal fluid is necessarily disrupted. When cerebrospinal fluid accumulates in the subarachnoid space or cysts, this leads to expansion of the brain cavities. Thus, intracranial pressure increases, which is considered one of the main symptoms of the disease.
Symptoms of arachnoiditis
Before talking about the symptoms that are characteristic of arachnoiditis, it should be noted that the signs of the disease depend on the location and are divided into three types - cerebral, spinal and cerebrospinal.
Cerebral arachnoiditis is primarily characterized by severe inflammation in the lining of the human brain, as well as the following symptoms:
- urinating too much;
- Convulsions, and in some cases severe seizures;
- Hearing disorders;
- Increased body temperature;
- Sleep problems;
- Memory and attention decrease;
- Partial or complete loss of the sense of smell;
- General weakness of the body, as well as excessive fatigue during physical or mental stress;
- Acrocyanosis (skin acquires some unusual blue tint);
- Constant dizziness, which is accompanied by excruciating pain in the head.
In situations where spinal arachnoiditis is present, almost the same symptoms are observed, but there are others, for example, a person is bothered by frequent pain in the lumbar region, as well as near the spinal region.
In addition, the patient is bothered by tingling in the extremities of the body, temporary paralysis, and sometimes numbness of the legs. In the most severe cases, a person feels disturbances in the genital organs, in particular, the level of potency decreases. The cerebrospinal type of the disease combines symptoms that are characteristic of both spinal and cerebral arachnoiditis.
Types of disease
Each type of pathology is characterized by certain signs and a special course of the pathological process.
Epidemic
Another name is lethargic. Diagnosed in both children and adults. Symptoms manifest themselves in a sharp increase in temperature, intense headaches, and pain in the joint tissue.
The patient experiences confusion, delusions, and hallucinations. Later, squint, difficulty breathing, and excessive sweating are added.
Kleshchevoy
The frequency of detection of this species increases in spring and summer, when infected ticks are most active. The causative agent of the disease is transmitted through the bite of an encephalitis tick.
Once ingested, the infection enters the brain through the bloodstream. The person begins to be afraid of bright light, pain in the head increases, and vomiting develops. Numbness of the limbs occurs, muscle structures are paralyzed.
Komariny
Another name for the species is Japanese. Infected mosquitoes transmit the virus. The disease is accompanied by high body temperature, vomiting, and confusion. Tremors of the limbs and convulsive seizures are recorded. The species is characterized by a high mortality rate.
Flu-like
Develops as a complication of influenza. Manifested by nausea, headache, weight loss, weakness. The disease often puts the victim in a comatose state.
Measles
Since measles is a childhood disease, this type of encephalitis is characteristic of children. Inflammation of the brain begins to develop several days after measles.
The patient becomes weaker, develops a feverish state, and suffers from epileptic attacks. The disease damages the nerves of the skull, causing paralysis and myelitis.
Diagnostics
Inflammation of the arachnoid membrane of the brain is diagnosed by comparing the clinical picture of the disease and data from additional studies:
- plain radiograph of the skull (signs of intracranial hypertension);
- electroencephalography (changes in bioelectric parameters);
- tomography (computer or magnetic resonance imaging) of the brain (expansion of the subarachnoid space, ventricles and cisterns of the brain, sometimes cysts in the intrathecal space, adhesive and atrophic processes in the absence of focal changes in the brain substance);
- studies of cerebrospinal fluid (moderately increased number of lymphocytes, sometimes slight protein-cell dissociation, leakage of fluid under increased pressure).
Diagnosis of arachnoiditis includes a complete neurological examination. In the process of a full analysis, reflexes, vegetatives, and sensitivity are examined.
Diagnostic methods
The dominant diagnostic method is puncture, during which a specialist takes cerebrospinal fluid (CSF). The biological material is examined and lymphocytic pleocytosis and protein concentration are detected.
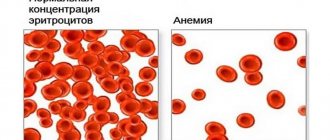
A blood test reveals a high number of leukocytes, and the erythrocyte sedimentation rate increases. Epileptic activity is recorded. During magnetic resonance imaging, pathological changes in the brain are recorded. When examining the fundus, congestion of the optic nerve is determined.
The disease is diagnosed based on the results obtained from bacteriological and serological tests. Virological identification is very difficult.
Consequences
Arachnoiditis can cause the following complications:
- seizures;
- severe visual impairment;
- persistent hydrocephalus.
These are quite serious complications. So, with convulsive seizures, the patient will have to take anticonvulsant medications all the time. This consequence of arachnoiditis develops in approximately 10% of cases and is typical only in severe cases of the disease itself.
In 2% of cases, patients suffering from this disease experience severe vision loss. It is extremely rare for patients to completely lose it. The most dangerous complication of arachnoiditis is persistent hydrocephalus, as it can be fatal.
Symptoms of brain inflammation
During the development of meningoencephalitis, which is a very serious disease, general septic symptoms develop. Symptoms of inflammation of the cerebral cortex and its membranes may be as follows:
- Body temperature rises sharply, chills ;
- feeling the urge to vomit;
- severe headache;
- no appetite ;
- hearing deteriorates;
- photophobia and increased sensitivity to sounds are noted;
- seizures may develop;
- stiff neck is observed;
- blood pressure rises;
- inhibition is noted.
If inflammation of the cortex or membranes of the brain occurs, specific symptoms of brain tissue are noted:
- coordination is impaired;
- sometimes skin rashes occur;
- the nerves of the skull are affected;
- anisoreflexia develops .
Symptoms of inflammation of the blood vessels of the brain and its cortex in children manifest themselves similarly. Along with a sharp rise in body temperature, signs of intoxication of the body are noted: severe headache, nausea and vomiting. Acute inflammation of the blood vessels and cortex affects the nervous system and provokes the development of increased sensitivity to external stimuli and the manifestation of general anxiety.
It should be noted that the clinical picture of the disease develops very quickly, and signs of this disease begin to appear already in the first or second day. At this time, tension in the muscles of the neck and back is noted, and this symptom is most noticeable in young children.
It is important to note that if a number of signs appear, emergency assistance should be called immediately. The following signs should alert you:
- convulsions;
- loss of consciousness;
- disorientation;
- paresis;
- oculomotor disorders.
If the course of meningoencephalitis is complicated, the following manifestations develop:
- rare and irregular heartbeat;
- speech and swallowing disorders;
- shallow and rapid breathing;
- state of coma (with fulminant course).
With the development of cerebral edema, death is likely.
Treatment of arachnoiditis
Treatment for arachnoiditis is usually carried out in a hospital. It depends on the etiology and degree of disease activity. Drug treatment is carried out over a long period of time, in courses, taking into account the etiological factor and includes:
- Antibacterial or antiviral drugs;
- Antihistamines (pipolfen, diphenhydramine, suprastin, claritin, etc.);
- Anticonvulsant therapy (carbamazepine, finlepsin);
- Anti-inflammatory drugs - glucocorticoids (especially for allergic and autoimmune inflammation);
- Absorbable treatment aimed against adhesions in the interthecal space (lidaza, rumalon, pyrogenal);
- Diuretics for hypertension syndrome (mannitol, diacarb, furosemide);
- Neuroprotective treatment (mildronate, cerebrolysin, nootropil, B vitamins).
Since the disease lasts a long time, is accompanied by manifestations of asthenia and emotional disorders, a number of patients need to be prescribed antidepressants, sedatives, and tranquilizers.
In all cases of arachnoiditis, other foci of bacterial or viral infection are searched for and treated, since they can be a source of repeated inflammation of the meninges. In addition to antibiotics and antiviral drugs, general strengthening measures, taking multivitamin complexes, good nutrition and an adequate drinking regimen are indicated.
General information
Meningoencephalitis is a condition in which the patient develops inflammation of the membranes of the brain and spinal cord. The peculiarity of this disease is that it combines the symptoms of two quite serious diseases. Encephalitis of an inflammatory process in the brain. With meningitis , inflammation of the membranes of the brain occurs. If both of these processes develop simultaneously in a patient, then he is diagnosed with meningoencephalitis. With concomitant damage to the spinal cord, paralysis . During the development of this disease, the patient exhibits meningeal, infectious, and variable focal symptoms. The inflammatory process can be initial or occur as a result of the development of a pathological process. If we are talking about secondary involvement of the medulla, then meningoencephalitis in this case is a complication of meningitis, but if the inflammation gradually spreads to the cerebral membranes, then the disease is a complication of encephalitis. Most often, this condition develops in young children, which is associated with the immaturity of the immune system and the blood-brain barrier.
Surgical intervention
Severe optico-chaosmal arachnoiditis or arachnoiditis of the posterior cranial fossa in the case of progressive decrease in vision or occlusive hydrocephalus are an indication for surgical treatment.
The operation may involve restoring the patency of the main cerebrospinal fluid pathways, removing cysts, or separating adhesions that lead to compression of nearby brain structures.
In order to reduce hydrocephalus in arachnoiditis, it is possible to use shunt operations aimed at creating alternative pathways for the outflow of cerebrospinal fluid: cystoperitoneal, ventriculoperitoneal or lumboperitoneal shunting.
Consequences and complications
The consequences of meningoencephalitis can be very serious, especially if treatment is not started on time. A serious complication of this disease is infectious-toxic shock, which develops as a result of the release of dead cells, toxins and waste products of microorganisms into the blood in large quantities.
The consequences of meningoencephalitis in adults can be manifested by the development of cerebral edema due to the accumulation of escudate in cerebral tissues. In turn, cerebral edema in adults and children leads to the fact that the brain structures are displaced and impinge on the trunk, resulting in progressive bulbar palsy . This condition is fraught with the development of cardiac and respiratory failure.
The consequences of meningoencephalitis in children may be similar. If the disease progresses, children may develop infectious-toxic shock , cerebral edema , renal failure , and increased cerebral pressure. In young children, the disease can lead to mental retardation.
Prognosis for arachnoiditis
In most cases, patients with arachnoiditis receive the third disability group. However, if they have severe visual impairment and frequent epileptic seizures, they may be assigned a second disability group.
The first disability group includes patients with opticochiasmatic arachnoiditis, which caused complete blindness. Work in transport, at heights, near fire, in noisy rooms, in unfavorable climatic conditions, and with toxic substances is contraindicated for patients with arachnoiditis.
Treatment Options
Treatment of arachnoiditis can only be carried out in a hospital setting. The therapeutic technique is selected depending on the severity of the disease and the degree of damage.
Most often, drug therapy is prescribed to eliminate the problem using:
- Anti-inflammatory glucocorticoids such as Prednisolone or Methylprednisolone.
- Absorbable drugs like Lidaza, Rumalon and others.
- Antiepileptic drugs (Keppra, Finlepsin).
- Dehydration drugs. They help lower intracranial pressure.
- Neuroprotectors and metabolites (Ginkgo Biloba, Nootropil).
- Antiallergic drugs.
- In some cases, psychotropic drugs may be used. These are antidepressants, tranquilizers, sedatives.
If there are foci with purulent processes, then they must be opened and cleaned. Similar procedures may be needed for patients with sinusitis, otitis media and other pathologies.
In some cases, surgery cannot be avoided. It should be performed if a person suffers from arachnoiditis of the posterior wall of the skull or opto-chiasmatic arachnoiditis, which is accompanied by loss of vision or the development of occlusive hydrocephalus.
During surgical treatment, the patency of the cerebrospinal fluid pathways is restored, adhesions are separated, and cystic formations that put pressure on nearby areas of the brain are removed.
To reduce the intensity of cerebral hydrops, shunting may be performed. Shunts are used to create additional drainage pathways for fluid.