Home / Heart
Back
Published: 01/31/2020
0
10
- 1 What are coronary stents and why are they needed?
- 2 Is stenting or bypass surgery better – what do experts say?
- 3 Application area
- 4 Indications
- 5 Indications for stenting surgery
- 6 Stages of operation
- 7 Postoperative period
- 8 Is stenting possible during pregnancy?
- 9 Possible complications
- 10 Drug therapy
- 11 Lifestyle changes
- 12 Where is stenting performed?
What are coronary stents and why are they needed?
A coronary stent is a medical device that is a frame in the shape of a metal cylinder, installed in narrow places in the artery (with cholesterol deposits) to widen them, thereby ensuring normal blood flow.
Stents can combat arterial stenosis that occurs due to the deposition of atherosclerotic plaques. Cholesterol is deposited on the walls of the arteries and narrows the lumen, thereby preventing blood flow. Poor blood flow causes oxygen starvation and lack of nutrients in the organs.
Stents differ from each other:
- Length. The size of the stents varies from 8 to 38 millimeters.
- Diameter. There are from 2.25 to 6 millimeters.
- By design. They differ in the shape of the elements from which they are created.
- Material. They are made from steel, cobalt-chrome, PLLA polymer and others.
- Coated. Stents are available without coating or with drug coating Sirolimus, biolimus and others.
- Method of disclosure. They can open either independently or with the help of a balloon on a catheter.
- By type of drug coating. The medications used are Sirolimus, everolimus, paclitaxel and others.
Stents are available: 8, 10, 13, 16, 18, 23, 28, 33, 38 mm.
Stents are available: 2.25, 2.5, 2.75, 3, 3.25, 3.5, 3.75, 4, 4.25, 4.5, 4.75, 5, 5.25, 5.5, 5.75, 6 mm.
By design:
- mesh (made of woven mesh);
- tubular (from a tube);
- wire (made of wire);
- ring (from separate rings).
According to the material from which the frame is made:
- stainless medical steel;
- cobalt-chrome alloy;
- alloy of platinum and chromium;
- polylactose acid (PLLA) polymer.
By type of coverage:
- Uncoated with bare metal.
- Drug-coated, which releases a drug that reduces the likelihood of future artery narrowing.
- With a double coating - external and internal, for healing the artery itself and preventing the formation of blood clots.
- Coated with antibodies, attracting endothelial cells, reducing the risk of thrombosis.
- Dissolving, made from a material that dissolves and releases a drug coating that prevents the recurrence of stenosis.
By opening method:
- self-expanding;
- opened by a balloon.
By drug coverage:
- Sirolimus;
- Zotarolimus;
- Everolimus;
- Biolimus;
- Paclitaxel.
Depending on the manufacturer, stents may differ in their characteristics and price. In Russia, the production of stents is carried out in accordance with GOST R ISO 25539-2-2012.
Prediction of how long you can live after surgery
If blood flow in the coronary arteries is completely restored after coronary bypass surgery and the patient takes all prescribed therapy, then the prognosis is considered favorable.
Restoring adequate blood supply to the myocardium can relieve the patient from pain associated with myocardial ischemia, reduce the number of angina attacks, and improve exercise tolerance.
Long-term results of surgical intervention:
- restoration of working capacity;
- reducing the risk of developing myocardial infarction;
- reducing the risk of sudden death from acute coronary syndrome;
- improving exercise tolerance;
- increase in life expectancy;
- medications are taken only for prophylactic purposes.
How long do you live after heart bypass surgery?
The average lifespan of a shunt is 10 years. To assess the viability of the shunt, coronary angiography is performed, based on the results of which a decision is made on the need for repeated surgical treatment. A full course of rehabilitation after cardiac surgery allows you to maximize the service life of the installed shunt.
Reviews from patients who have undergone bypass surgery are mostly positive. After the operation, the heart undergoes remodeling; during this period, patients note a deterioration in their health, and it seems to them that the operation was unsuccessful. However, after a while, after a complete restructuring of the blood supply to the myocardium, the patients’ well-being significantly improves, exercise tolerance increases, and chest pain goes away. In the long term, reviews are mostly positive.
A gentle surgical option to restore adequate blood supply to the myocardium is cardiac stenting. The essence of the operation is to insert a special stent into the coronary vessel, which, after deployment, completely opens the lumen of the affected artery and restores blood flow. The rehabilitation period after stenting surgery is much shorter than with bypass surgery, because The intervention is not performed on an open heart, but a stent is inserted through the groin or through the arm.
Education: Graduated from the Bashkir State Medical University with a degree in General Medicine. In 2011, she received a diploma and certificate in the specialty “Therapy”. In 2012, she received 2 certificates and diplomas in the specialty “Functional Diagnostics” and “Cardiology”. In 2013, she took courses on “Current issues in otorhinolaryngology in therapy.” In 2014, she completed advanced training courses in the specialty “Clinical Echocardiography” and courses in the specialty “Medical Rehabilitation”. In 2020, she completed advanced training courses in the specialty “Vascular Ultrasound”.
Work experience: From 2011 to 2014, she worked as a therapist and cardiologist at the Municipal Budgetary Healthcare Institution Polyclinic No. 33 in Ufa. Since 2014, she worked as a cardiologist and functional diagnostics doctor at the Municipal Budgetary Healthcare Institution Polyclinic No. 33 in Ufa. Since 2020, he has been working as a cardiologist at the State Budgetary Healthcare Institution Polyclinic No. 50 in Ufa. He is a member of the Russian Cardiological Society.
Is stenting or bypass surgery better – what do experts say?
Both operations are currently used as radical treatments for coronary artery stenosis. But they differ significantly from each other. The operation of stenting the heart vessels is the introduction into the human body of a kind of conductor that helps the stenotic artery to function normally. The stent is a foreign body.
Only a cardiac surgeon can answer this question regarding each specific patient with angina during an in-person examination. However, some benefits have been identified for both treatments.
Thus, stenting is characterized by a less traumatic operation, better tolerance by patients, and no need for general anesthesia. In addition, the patient spends fewer bed days in the hospital and can start working earlier.
Bypass surgery is performed using one’s own tissues (veins or arteries), that is, there is no foreign body in the body. Also, the likelihood of re-stenosis of a bypass is lower than that of a stent. If the patient has diffuse damage to the coronary vessels, bypass surgery can solve this problem, unlike a stent.
So, in conclusion, I would like to note that despite the fact that many patients are wary of the possibility of heart surgery, they should listen to the recommendations of the attending physician and, if stenting is necessary, they should give their thoughts a positive attitude and boldly go for the operation.
Sometimes, with heart problems, the condition becomes so serious that conventional medications no longer help. In such cases, you have to resort to some radical methods to improve the situation. Let's look at two options for surgical intervention and find out how bypass surgery differs from stenting.
The condition of the heart depends on the quality of its blood supply. And this, in turn, is determined by the degree of vascular patency. When everything is in order, they have smooth walls, and the blood moves without stopping along the right path. But over time, the vessels in some places can become very narrow and become overgrown with atherosclerotic deposits.
All this disrupts blood flow. The tissues of the main organ begin to experience oxygen starvation. The logical consequence in such a situation is the development of cardiac ischemia. Complete blockage of the vessel is especially dangerous.
In an area deprived of blood supply, the tissue dies and myocardial infarction occurs. The operations in question make it possible to prevent such an outcome, and sometimes even save the life of a person already in critical condition.
Comparison
The goal of both interventions is to normalize blood flow. However, the result in each case is achieved in its own way. Considering the difference between bypass surgery and stenting, it is worth noting that the second of these operations is easier and is often performed faster.
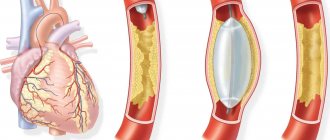
Stenting usually does not require the patient to be put under anesthesia. The essence of the procedure is to expand the problem area of the vessel by installing an implant.
To do this, a puncture is made in the area of the femoral artery under local anesthesia. Through this slot, a long narrow tube is inserted into the vessel.
At its end there is a deflated balloon, on top of which a stent is fixed, also compressed.
The structure is advanced through the artery under X-ray control and brought to the affected area. After this, the can is inflated.
Inflating, it causes the stent to expand and firmly fix itself in the form of a flexible tubular mesh in the walls of the vessel.
Then all the auxiliary instruments are removed, and only the implant remains in the body, which subsequently prevents the lumen from narrowing and ensures the normal passage of blood.
Stenting
Bypass surgery is a more complex and risky operation, but is nevertheless sometimes necessary.
Such intervention is performed when the installation of a stent is futile or impossible.
This method is used, for example, when the diameter of the affected vessel is miniature, in the case of atherosclerotic changes of a large extent, or when multiple blockages of the lumens are detected.
Here, the meaning of the surgical actions is to create an artificial blood flow path using a shunt. In this case, the blocked part of the vessel is excluded from the circulation system. The shunt most often becomes a fragment of a vein or artery from another area of the body. In some cases, artificial materials are used.
Bypass surgery
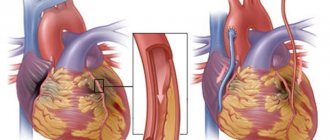
To restore blood flow in this way, an incision is made in the chest area. The person being operated on is under anesthesia. Bypass surgery is often performed on a non-functioning heart, while providing artificial circulation. If possible, make do with small incisions in the intercostal spaces.
What is the difference between bypass surgery and stenting? It also lies in the terms of rehabilitation after the actions taken. In the first case, the recovery period lasts longer, in the second, the patient usually gets back to his usual routine faster. In addition, bypass surgery entails many more possible limitations in the future than stenting.
Coronary heart disease (CHD) is a real problem for humanity in the 21st century. Poor nutrition and a sedentary lifestyle lead to excess cholesterol forming atherosclerotic plaques on blood vessels, significantly impairing blood flow. The most dangerous thing for the “proper” functioning of the heart is the narrowing of the lumen in large arteries.
Insufficient oxygen supply to the myocardium is one of the reasons for the development of coronary artery disease. Thanks to the latest methods of treating heart disease, it has become possible to improve the condition of patients suffering from coronary artery disease.
Such procedures today are stenting and bypass surgery of large vessels, after which it is possible to fully restore oxygen supply to the heart, but it is clear that specialists have not been able to do better for many years.
Despite some disagreements among surgeons and cardiologists, both methods of restoring vascular patency have been demonstrating good performance in the treatment of coronary artery disease for a long time. But still, each of them differs in the way the procedure is carried out, and also has its own advantages and disadvantages. We'll look at which ones next.
If you have any additional questions, our experienced specialists will be able to advise you free of charge.
Just enter your question in the pop-up form.
Fast and efficient
Stenting is one of the methods of restoring blood flow, it is considered minimally invasive and is based on the introduction of a stent into the affected area. A stent is a kind of frame in the form of a tube made of mesh material.
When installing it, an x-ray endovascular technique is used. That is, through a small puncture on the thigh or arm, a deflated balloon with a metal mesh on it is brought through the artery to the site of blockage using a catheter.
The stenting procedure takes no more than an hour and is performed using X-ray equipment and contrast agents.
Due to the fact that the operation takes place without large incisions and under local anesthesia, the likelihood of complications is minimized. After such an operation, the patient can get up within a few days and soon be discharged from the hospital.
But, despite many positive reviews from patients and doctors, low trauma and safety, this procedure also has its contraindications. Stenting, for example, cannot be performed in patients with diabetes mellitus or in cases of multiple vascular lesions.
In addition, there is a possibility of restenosis in the first two years after surgery, which can be eliminated by repeating a similar operation. Fortunately, today stents with a special coating are used, which minimizes the occurrence of re-narrowing of the vessel.
Long but reliable
One of the modern methods of restoring vascular patency is stenting and bypass surgery. These procedures are most often used in the case of coronary heart disease, when the coronary arteries that supply the heart muscles become blocked by atherosclerotic plaque at a certain interval.
During stenting, a special metal structure in the form of a mesh is installed into the lumen of the vessel, which eliminates the narrowing.
Both operations performed by Israeli surgeons are effective, but have their advantages and disadvantages.
The great advantage of stenting is the ability to perform it without making extensive incisions. An x-ray endovascular technique is used, when a thin catheter is brought to the site of narrowing through a peripheral artery under the control of x-ray equipment and with the use of contrast agents.
In this case, only a small puncture is required in the area of a peripheral vein, for example, the femoral vein, so the traumatic nature of the operation and the risk of developing infectious complications are minimized. Through a catheter, a metal mesh on a balloon is delivered to the required area, which is inflated and installed in the lumen of the artery.
In this case, it is possible to install not only one stent, but also 3-4.
What is bypass surgery?
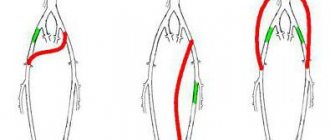
To understand the difference between bypass surgery and stenting of cardiac vessels, let’s take a closer look at how the shunt is installed. The goal of surgery is to redirect blood flow away from clogged arteries.
The principle of the operation was developed by Soviet scientist Vladimir Demikhov in 1960. During the Great Patriotic War he worked as a pathologist. It was at this time that he came up with the idea of creating a bypass route to supply the heart with blood.
The scientist proposed suturing the thoracic artery to the cardiac artery in the area below the plug. Such a prosthesis is called a shunt. In surgery, they resort to suturing with the radial artery of the arm or the great saphenous vein of the leg.
Compared to stenting, this approach provides a long-term effect. It is rare for a patient to return with symptoms. A shunt is used if 3 or more arteries are blocked. In other cases, stenting or balloon angioplasty is performed.
Installing a shunt allows you to determine the location of the plaques. But the method has many contraindications and possible complications, and the cost is higher than stenting.
Application area
One of the common causes of the development of heart pathologies is a decrease in vascular elasticity and vasospasm. The arteries gradually lose their ability to expand, which leads to local disturbances in blood supply. Also, if the process is chronic, this contributes to the accumulation of cholesterol deposits on the vascular walls.
Stenting is a procedure for integrating a special dilating device into a vessel. It is a tube with a mesh texture that can take the desired shape when implanted. The device acts as a frame. As a result, the narrow or spasmodic section of the artery should expand, and the blood flow should return to its previous state.
This treatment method belongs to endovascular surgical interventions and is considered minimally invasive. It is performed exclusively by experienced surgeons of the highest category.
Let's consider the stenting algorithm using the heart as an example. The catheter on which the element is fixed is passed through the femoral artery through the introducer. The conductor must be moved to the designated area where it is planned to install the expander. As soon as the catheter is inserted, the artificial frame is fixed, inflated under the action of the balloon, and normalizes blood supply to the heart muscle.
The operation involves local anesthesia. The average duration is relatively short, from 20 minutes to 3 hours. If necessary, the surgeon installs several devices at once.
Stents are an outstanding invention that can save the lives of many patients. But it is not suitable for all patients suffering from stenosis. Like other medical instruments, stents have advantages and disadvantages.
Advantages:
- Minimally invasive, to eliminate the problem you do not need to make large surgical incisions on the body, but only a small hole on the body into which a catheter with a stent is inserted. Fast healing. The patient can be discharged on the 3rd day.
- Use of local anesthesia during surgery. There is no need to put a person to sleep. High percentage of successful cure (90%).
Flaws:
- There is a possibility of secondary stenosis, the appearance of blood clots and heart attacks. Occurs in 10% of patients.
- Complexity of the operation. The installation of stents in the heart is performed only by highly qualified surgeons.
- Some drug-eluting stents are expensive.
- Not all patients can undergo stenting – there are contraindications.
Main differences between operations
To clarify which is better: stenting or cardiac bypass surgery, let’s summarize the differences between these operations:
- Anesthesia. For stenting, local anesthesia in the area of the artery through which the prosthesis is inserted is sufficient. The operation does not require large incisions or stitches. Shunt installation is a long and complex procedure performed under general anesthesia.
- Providing access. The femoral artery is used to insert the stent. The shunt requires more extensive access. Surgeons have to make an incision in the sternum, sometimes in the ribs or intercostal spaces, and open the pericardium.
- Age of patients. Installation of a shunt is indicated if stenting is not possible. Accordingly, the age of patients with a shunt is much older.
- Use of a heart-lung machine. Used to create a shunt when it is necessary to turn off the heart. In the case of stenting, this is not necessary.
- Angiography. X-ray examination of blood vessels with the introduction of a contrast agent is necessary before surgery. Stenting is performed with coronary angiography, and a shunt is attached after it.
- Duration of the operation. It only takes a few minutes to install the stent. Creating a shunt is a long-term intervention, lasting up to 6 hours. The duration of the procedure also depends on the number of affected areas.
- When they are discharged. Stenting does not require long-term medical supervision, so the patient is sent home within 24 hours. After installation of the shunt, the patient remains in the clinic for another 10-14 days.
- Rehabilitation period. Recovery time after a stent is about 2 weeks. For a shunt, the period is extended to 3-4 months; during the operation, an incision was made in the sternum. After bypass surgery, the patient is recommended to wear a medical corset.
- Risk of relapse. After stenting, blockage of blood vessels develops faster. Being a foreign body, the stent provokes the formation of blood clots. Plaques can also form in the shunt, but this process is slow and can take up to 10 years. In both cases, if there is a relapse, repeat surgery is indicated.
- Life expectancy of patients. According to statistics, 95% of patients survive within a year. Within 5 years this figure is reduced to 86%. With bypass surgery, life is extended by another 15-25 years.
Having considered what cardiac bypass and stenting are, we can say that the first, although it is a complex operation, leads to lasting results and fewer relapses.
Indications
Installation of coronary stents may be indicated by a doctor in the following cases:
- complete blockage of the coronary artery during or after myocardial infarction;
- narrowing or complete blockage of the arteries with a high risk of heart failure;
- narrowing or complete blockage of blood vessels with a high risk of severe angina.
Stenting is done only in cases where there are no contraindications to the operation. In another case, bypass surgery is performed.
- If intervention is required in an artery with a diameter of less than 3 mm.
- If the patient has a large number of cholesterol plaques, more than 1 centimeter in length.
- If the patient is allergic to iodine-containing drugs.
- If the patient has a large number of cholesterol plaques, more than 1 centimeter in length.
- If the patient has poor blood clotting.
- If the patient has a serious condition, accompanied by a drop in blood pressure, impaired consciousness, shock, liver, kidney or respiratory failure.
- The patient has malignant tumors that cannot be treated.
If a patient is contraindicated for stenting, but still wants this operation, then in some cases he may insist on having it performed at his own risk.
The operation of coronary stenting is indicated for patients with the following forms of coronary heart disease:
- Progressive angina - increased frequency, duration and intensity of attacks of chest pain that are not relieved by taking nitroglycerin under the tongue,
- Acute coronary syndrome (pre-infarction condition), threatening the development of acute myocardial infarction in the near future without treatment,
- Acute myocardial infarction,
- Early post-infarction angina - attacks of heart pain that occur in the first weeks after an acute heart attack,
- Stable angina FC 3-4, when frequent, prolonged painful attacks significantly reduce the patient’s quality of life,
- Repeated stenosis or thrombosis of a previously installed stent or shunt (after coronary artery bypass surgery).
stenosing atherosclerosis of the coronary arteries is the main prerequisite for the operation.
It is preferable to install a drug-coated stent in the following categories of patients:
- Persons with diabetes mellitus, impaired kidney function (patients receiving hemodialysis),
- Persons at high risk of developing restenosis,
- Patients who have undergone bare stent surgery and develop restenosis
- Patients with repeated graft stenosis after CABG surgery.
For emergency reasons, for example, in case of acute myocardial infarction, a stent can be installed even in a patient in serious condition, if it is caused by cardiac pathology. However, surgery may be contraindicated in the following cases:
- Acute stroke,
- Acute infectious diseases,
- End-stage liver and kidney failure,
- Internal bleeding (gastrointestinal, pulmonary),
- Disorders of the blood coagulation system with a high risk of life-threatening bleeding.
Stenting can be performed urgently or routinely. In emergency surgery, coronary angiography (CAG) is first performed, based on the results of which a decision is immediately made to introduce a stent into the vessels. Preoperative preparation in this case comes down to the introduction of antiplatelet agents and anticoagulants into the patient’s body - drugs that prevent increased blood clotting (to avoid thrombosis). As a rule, heparin and/or clopidogrel (warfarin, Xarelto, etc.) are used.
Before a planned operation, the patient must perform the necessary research methods to clarify the degree of vascular damage, as well as assess the contractile activity of the myocardium, the ischemic zone, etc. For this, the patient is prescribed CAG, ultrasound of the heart (echocardioscopy), standard and stress ECG, transesophageal electrical stimulation myocardium (TEFI - transesophageal electrophysiological study). After all diagnostic methods have been completed, the patient is hospitalized in the clinic where the operation will be performed.
The evening before the operation, a light dinner is allowed. It is likely that some cardiac medications will need to be discontinued, but only as directed by the attending physician. Breakfast before surgery is not allowed.
Stenting itself is performed under local anesthesia. General anesthesia, dissection of the chest and sternum, and connection of the heart to a heart-lung machine (ACB) are not required. At the beginning of the operation, local anesthesia of the skin is performed in the projection of the femoral artery, which is accessed through a small incision.
Next, the balloon, which is always inside the stent in a compressed state, is inflated using air injection, and the stent, being a spring structure, is straightened out, tightly fixed in the lumen of the artery.
After this, the catheter with the balloon is removed, a tight aseptic dressing is applied to the skin incision, and the patient is transferred to the intensive care unit for further observation. The entire procedure lasts about three hours and is painless.
After stenting, the patient is observed for the first day in the intensive care unit, then transferred to a regular ward, where he remains for about 5-7 days until discharge from the hospital.
Combining coronography with angioplasty and stenting is undesirable
In most situations, according to leading experts, it is undesirable to combine coronary angiography, which is a diagnostic procedure , with therapeutic procedures: angioplasty and stenting. If coronary angiography diagnoses coronary artery stenosis, but the patient's condition does not require emergency medical care, it is not recommended to immediately proceed to angioplasty and stent placement. The decision to choose a technique should be made collectively, after careful discussion of all aspects of the procedure, while respecting the patient's rights to participate in the treatment process and obtaining informed consent.
Currently, American and European associations of doctors specializing in the treatment of cardiovascular pathologies recommend using the Heart Team concept in clinical practice. The team should be composed of both cardiologists and cardiac surgeons, and consider each clinical case individually. This is how strategic decisions are made at the Herzliya Medical Center private clinic when it comes to treating patients with serious cardiovascular diseases.
Indications for stenting surgery
Before stenting, the patient is examined. They take basic tests, do echo and electrocardiography. Coronary angiography is performed by injecting contrast into the circulatory system and performing an X-ray examination. A map of the coronary arteries is obtained. The site of stent insertion is determined.
As a rule, to prepare for surgery, doctors may require:
- Avoid food and water 8 hours before surgery.
- Avoid taking blood thinning medications 3 days before stenting.
- Shave your groin and wash yourself.
- Eliminate or reduce the intake of glucose-lowering drugs 2 days before surgery.
Coronary stenting. Indications.
Like any other surgical intervention, even minimally invasive, stenting of cardiac vessels has quite serious risks, so the indications for this procedure should promise benefits that significantly exceed the risks. This is possible in the following situations:
- Progressive angina. A situation where a patient is forced to regularly call an ambulance due to frequent and unpredictable attacks of angina.
- Acute coronary syndrome or myocardial infarction in the early stages of development
- Early post-infarction angina, a situation in which angina attacks recur during treatment for myocardial infarction.
- Stable angina pectoris with low quality of life on the background of adequate drug therapy.
- High risk of cardiovascular accidents and/or death, identified as a result of non-invasive examination methods.
Of course, stenting can be performed only if the technical feasibility of the intervention is confirmed based on previously performed coronary angiography.
Operation stages
- The operation is performed in an operating room equipped with an angiograph, which allows the doctor to observe the artery and the movement of the catheter on a monitor screen. The patient is placed on his back and sedated to keep him calm and relaxed.
- Doctors cover the patient with sterile linen and neutralize the stent insertion site.
- Local anesthesia is given.
- A thin wire is inserted into the artery through a needle, which acts as a conductor.
- An introducer is inserted along the guidewire, through which other instruments will be inserted into the artery and the wire is removed.
- Through the introducer, the doctor carefully inserts a thin catheter with a stent and a balloon.
- A contrast agent is injected into the coronary artery to accurately visualize the movement of the stent.
- The stent continues to be carefully moved to the desired location.
- The stent is expanded using a balloon on the catheter, thereby normalizing the diameter of the artery.
- After stent placement, the introducer and catheter are removed from the patient.
- A compressive bandage is applied to the catheter insertion site.
Consequences and complications
Complications can develop if the patient has concomitant pathology:
Most often, after surgery, bleeding occurs in the anastomotic area and rhythm disturbances are recorded. Possible complications:
- acute circulatory disorder in the brain and myocardium;
- thrombosis of the venous bed;
- renal failure;
- local complications in the form of wound infection and the formation of postoperative keloid scars;
- closure or narrowing of the shunt.
Postoperative period
After stenting, the patient is transferred to a ward where nurses monitor him.
If the catheter was inserted through the femoral artery, the patient is instructed to lie for 6 hours without bending his leg. If the stent was inserted through the radial artery, the patient can sit immediately and walk a few hours later.
To quickly remove contrast from the body, the patient is prescribed to drink a lot of water.
The patient is discharged after 1-3 days.
During this period, a set of measures is formed for the patient that will help him recover faster and reduce the risk of complications and recurrence of the disease.
After the operation, the patient lies in bed for 1-3 days in the hospital. At this time, doctors closely monitor the patient. After this, the person is discharged home, where he must also be at emotional and physical rest and observe bed rest. He should not take a bath or shower or exert himself physically.
During the recovery period, drug treatment is prescribed for six months, designed to reduce the risk of re-stenosis, thrombosis and heart attack. And increase the length and quality of life.
During the recovery period, the doctor prescribes everything necessary to:
- Improve a person's physical abilities.
- Restore heart functionality.
- Slow down the process of ischemia.
- Bring laboratory parameters back to normal.
- Prevent possible complications after surgery.
- To form in the patient a correct lifestyle that ensures longevity.
- Provide psychological comfort.
Stenting and Bypass. Is there a difference?
Doctors are used to speaking in their own language, understandable only to them.
This significantly reduces the time doctors communicate with each other and simplifies it. Medical terms in Latin are pronounced more simply and concisely than in any other language and are understandable to doctors anywhere in the world. Therefore, when communicating with patients, it is difficult to switch to normal human language and this causes a complete misunderstanding of the situation on the part of the patient. It seems to us, doctors, at this moment that we have said everything, all the questions have been sorted out and there are no problems left.
However, people who are far from medicine, and these are the majority, left the doctor with a mess in their heads that is very difficult to sort out. If information is unclear, most people try to ignore it completely.
This, in my opinion, is where mistrust in medicine in general and low adherence to treatment arises. Here again is an incomprehensible term. Low adherence to treatment means a complete or partial refusal of the doctor’s prescriptions, although compliance with these prescriptions is in the interests of the patient, because he came to the doctor specifically for this.
The problem is complex, so do not hesitate to ask the doctors any questions, ask them to translate terms that you do not understand into Russian. In the treatment of coronary heart disease, there are two surgical methods, which in medical jargon sound like STENTING and BYPASS.
The difference in pronunciation and spelling is small, but these are two fundamentally different methods of restoring normal blood flow in the arteries of the heart clogged with cholesterol plaques.
Stenting is a slang word; you won’t find it in official medical documents, but doctors pronounce it when communicating with patients and among themselves. The medical term is percutaneous coronary intervention (PCI) or endovascular coronary angioplasty (CA).
Bypass surgery means: coronary artery bypass grafting (CABG) surgery. Agree, the names are complex and long, even doctors find it difficult to pronounce them, so the shortened version is used in conversation. What is the fundamental difference?
So, doctors say STENTing, which means percutaneous coronary angioplasty (PCI). What is it? Stenting - removal of a blood clot from a coronary artery and installation of stents is a minimally invasive operation.
The term “minimally invasive” surgery means that during the operation the trauma that is caused to the patient’s organs and tissues is minimal or virtually absent. The term “invasive” operation refers to all operations where tissues and organs are cut and must be performed under anesthesia.
Stenting is performed through a small puncture in the skin on the wrist or groin, the patient is fully conscious, the injection site is numbed with lidocaine or another anesthetic, the procedure lasts no more than an hour. In this case, the patient does not experience pain; sometimes there are sensations in the chest, similar to angina pectoris.
The surgeon passes a thin conductor through the artery in the arm to the very beginning of the aorta, under X-ray control finds the arteries of the heart, inserts the conductor into them and places a stent in the place where the thrombus is located. A stent is a metal structure that is installed in the lumen of the artery so that the internal diameter of the artery is maintained at a normal level.
Rehabilitation after this procedure is minimal; with planned stenting, the patient can walk within a couple of hours. Despite the apparent ease for the patient, this is a very serious intervention - heart surgery.
During the operation, contrast is injected and X-ray exposure occurs. She has her own indications and contraindications. There is always a risk of complications both during and after surgery. The scope and outcome of the operation greatly depend on the experience of the operating surgeon.
If the lesions of the coronary arteries are complex from an anatomical point of view and the risk of surgical complications after stenting is too great, then doctors may decide to perform coronary artery bypass grafting (CABG).
BYPASS is an invasive operation that is performed under anesthesia, often on a non-functioning heart (depending on the type of operation) and using a heart-lung machine (CAB). The rehabilitation period after this operation is quite long and takes from several weeks to several months.
The essence of the operation is that additional vessels are sewn bypassing the damaged arteries, which are taken from other parts of the patient’s body. The intervention is performed under anesthesia and with incisions in the chest.
This operation is indicated for those patients who have damaged all three main coronary arteries, or the trunk of the left coronary artery (LCA) with damage to the right coronary artery (RCA) and there is pathology of the heart valves.
In any case, the indications for performing a particular type of operation are determined by doctors, weighing the possible risks of the operation and the potential benefits of this type of intervention in a particular patient, taking into account the characteristics of his disease and concomitant pathology.
The technique of performing these two operations is fundamentally different, but the essence is the same - restoration of normal blood flow in the heart during coronary artery disease. The treatment tactics after these two operations are absolutely the same.
Patients who have undergone STENTING or BYPASS need to take the same medications for a long time, stop smoking, follow the principles of a healthy diet and maintain physical activity in the form of regular aerobic exercise under the constant supervision of a cardiologist.
Consultation with a specialist is required.
Anna Korenevich is a cardiologist. Candidate of Medical Sciences. Expert in the field of treatment, prevention and rehabilitation after myocardial infarction.
Source: //zen.yandex.ru/media/id/5d2dd016d5135c00ad3b7718/5d39b27231878200aeb6f65c
Is stenting possible during pregnancy?
Installation of stents is not recommended for pregnant women, as during the operation an X-ray is taken, which can be harmful during pregnancy. The operation can be stressful; the pregnant patient is given contrast, anesthesia and other drugs, which can also have a negative effect on the fetus. Some drugs may cause allergic reactions.
Surgery for pregnant women is prescribed only in extreme cases; the surgeon informs the patient in advance about the possible risks and consequences and performs the operation only with her consent.
Complications of cardiac artery stenting
Unfortunately, with stenting, like any other surgical intervention, complications are possible. The following conditional division of these complications is accepted: Intraoperative complications, i.e. arising during the operation:
- Heart rhythm disturbances
- Myocardial infarction
- Vessel dissection, i.e. detachment of the inner lining of the artery
- Angina attack
- In rare cases, death can occur.
Rarely, but it is possible for a situation to develop in which a transition from stenting to coronary artery bypass surgery is possible.
- Heart rhythm disturbances
- Stent thrombosis, with possible development of myocardial infarction
- Hematoma at the puncture site
- True or false aneurysm of the punctured artery
Late postoperative complications
Possible complications
Thus, intraoperative (during surgery) complications are the occurrence of life-threatening arrhythmias (ventricular fibrillation, ventricular tachycardia), incision of the coronary artery (dissection), and extensive myocardial infarction.
Early postoperative complications are acute thrombosis (sedimentation of blood clots at the site of stent installation), aneurysms of the vascular wall with the possibility of rupture, and cardiac arrhythmias.
A late complication after surgery is restenosis, the growth of the inner lining of the vessel onto the surface of the stent from the inside with the appearance of new atherosclerotic plaques and blood clots.
Prevention of complications consists of careful X-ray monitoring of stent installation, the use of the highest quality materials, as well as taking the necessary medications after surgery to treat atherosclerosis and reduce blood clots. The correct attitude of the patient also plays a significant role here, because in any field of surgery it is known that in positively minded patients the postoperative period proceeds more favorably than in persons predisposed to anxiety and restlessness. Moreover, complications develop in less than 10% of cases.
In some cases, complications may occur after stenting. The reason may be an incorrectly performed operation or the characteristics of the patient’s body, how it reacts to the installed stent.
- Thrombus formation at the site of stent placement is the most common complication. To reduce the likelihood of blood clots, the patient is given blood thinning medications.
- Bleeding with hematoma. Occurs due to the introduction during surgery of drugs that reduce blood clotting. Rarely seen.
- Infection of the incision site where the catheter is inserted.
- Allergy to radiopaque contrast agent or drug coating on the stent.
- Re-narrowing of an artery in another location, as plaques carried by blood from a previously problematic area can break off and block another area in the artery.
- Restenosis is the body’s reaction to the installed stent, expressed in excessive growth of the inner lining of the vessel in the area where normal lumen was restored.
- Heart attack during stenting.
There is a greater risk of complications in patients with chronic diseases such as diabetes, kidney disease and blood clotting disorders. To exclude a number of complications, the patient is thoroughly studied before the operation and adjustments are made to the treatment, regulating blood clotting with medication, and selecting a stent with the desired drug coating. Carefully monitoring the patient's condition after surgery.
Angioplasty and CABG: definition
| Coronary angioplasty and stenting | Coronary artery bypass grafting |
| Coronary angioplasty and stenting are the most common procedures in modern invasive cardiology. During angioplasty, atherosclerotic deposits are removed from the walls of the coronary arteries that supply blood to the heart muscle (myocardium). After angioplasty, in order to prevent restenosis (re-narrowing) of the coronary arteries, a stent is installed in their lumen - a supporting frame. Stenting is considered an extremely effective treatment for patients with coronary heart disease (CHD) and acute disruption of the blood supply to the myocardium - infarction. This procedure is performed as part of vascular catheterization and does not belong to the category of surgical interventions. | Coronary artery bypass grafting is a heart operation that creates a bypass path around the stenotic area of the coronary artery. For this purpose, a shunt is used - a segment of a blood vessel. Its donor is the patient himself: the shunt is formed from a vessel in the chest or lower limb. One of the main advantages of bypass surgery is the reliability of the alternative path (Bypass) of blood supply to the myocardium: bypasses have a long viability and maintain their patency for a long time. |
Drug therapy
After stent installation, the patient is usually prescribed the following medications:
- Antiplatelet, reducing the risk of blood clots. (Aspirin, Aspicard, Aspinat, Trombogard, Acetylsalicylic acid, Clopidogrel, Detromb, Trombex and others. Prescribed by the doctor to each patient individually.)
- Statins, which lower cholesterol levels and reduce the likelihood of restenosis. (Simvastatin, Pravastatin, Pitavastatin, Lovastatin, Atorvastatin, Rosuvastatin and others. Prescribed by the doctor to each patient individually.)
- Drugs that reduce the risk of heart attack.
The range of medications prescribed depends on the patient’s condition and health characteristics. It is necessary to strictly take in full all medications prescribed by the doctor for the period of treatment. After stenting surgery, it is strictly forbidden to self-medicate and take medications at your own discretion.
In which cases is it better to do bypass surgery, and in which stenting?
All of the listed pros and cons of both types of cardiac intervention and their differences play a minor role in the choice of surgical treatment method. Bypass or stenting is decided by the doctor after a comprehensive assessment of the patient’s condition, in particular the vessels of his heart. For this purpose, the SyntaxScore is used, which determines more effective and less dangerous tactics. Especially with complex lesions or atherosclerotic stenosis of the trunk of the left coronary artery.
Whatever operation is prescribed, the course of the postoperative period depends on the patient’s strict compliance with the doctor’s instructions. This includes taking medications, following a diet, and doing daily exercise. Consequently, the duration and fullness of life after stenting or bypass surgery depends on the patient himself.
Lifestyle change
As a rule, in 90% of cases, patients note the absence of angina attacks. However, this does not mean that you can forget about your health and continue to live as if nothing had happened. Now you must take care of your lifestyle and, if necessary, correct it. To do this, just follow simple rules:
- Stop smoking and drinking strong alcoholic drinks.
- Follow the principles of healthy eating. There is no need to exhaust yourself with constant starvation diets in the hope of normalizing high cholesterol levels in the blood (as the basis for the development of atherosclerosis). On the contrary, you should get proteins, fats and carbohydrates from food, but their intake should be balanced, and the fats should be “healthy”. Fatty meats, fish and poultry should be replaced with lean ones, and fried foods and fast food products should be completely eliminated from the diet. Get more greens, fresh vegetables and fruits, dairy products. Also useful are cereal products and vegetable oils - olive, flaxseed, sunflower, corn.
- Take medications prescribed by your doctor - lipid-lowering drugs (if cholesterol levels are high), antihypertensive drugs, antiplatelet agents and anticoagulants (under monthly monitoring of blood clotting). Particular attention should be paid to prescribing the last group of drugs. So, in the case of installing a simple stent, “double prevention” of its thrombosis consists of taking Plavix and aspirin in the first month after surgery, and in the case of a drug-coated stent - in the first 12 months. Premature stopping of taking medications according to the regimen prescribed by the doctor is unacceptable.
- Avoid significant physical activity and sports. Loads adequate to the patient’s condition in the form of walking, light jogging or swimming are sufficient.
- After the operation, visit a cardiologist at your place of residence according to his appointments.
- Stenting is not a disabling operation, and if the patient remains able to work, he can continue to work.
Life expectancy also increases - more than 90% of patients live quietly in the first five years after surgery. This is also evidenced by reviews from patients whose quality of life improves significantly. According to patients and their relatives, angina attacks almost completely disappear, the problem of constant use of nitroglycerin is eliminated, the patient’s psychological state improves - the fear of death during a painful attack disappears.
Atherosclerosis, as a rule, is caused by an incorrect lifestyle, and in order to fully recover after surgery and avoid arterial stenosis in the future, it is necessary to change your lifestyle to a healthy one.
The transition to a healthy lifestyle is:
- Do morning exercises, move and walk quietly for 30 minutes - 1 hour about 3-4 days a week.
- Completely eliminate active and passive smoking.
- You can safely enjoy swimming, skiing, use an exercise bike or treadmill evenly and measuredly for up to 6 hours a week.
- Avoid alcoholic drinks.
- Avoid fatty, fried and salty foods.
- Do not consume more than 4 grams of salt per day.
- Drink tea instead of coffee.
- Attend examinations by your attending physician.
- Eat more vegetables, fruits, fish, rye and bran bread.
The diet and exercise program is prepared by the attending physician. For successful recovery, you must fully adhere to the schedule he has drawn up.
| Our company offers high-quality stents for coronary vessels. You can familiarize yourself with the entire range of manufactured medical equipment for cardiac surgery in the website catalog. We are pleased to present you a coronary stent at a price affordable for every consumer! | Go to directory {amp}gt; |
What is the difference between bypass surgery and stenting?
stent in the coronary artery of the heart
A patient with myocardial ischemia is forced to constantly take certain medications that prevent the formation of blood clots, high blood pressure and high cholesterol levels in the blood.
However, despite medical treatment, patients with significant stenosis often develop acute myocardial infarction.
An excellent method of treating coronary artery disease and preventing heart attack is the installation of a stent in the lumen of the coronary artery.
A stent is a thin metal frame in the form of a flexible mesh, which is inserted into the lumen of the artery in a compressed state and then expands like a spring. Due to this, atherosclerotic plaques are “pressed” into the artery wall and the vessel wall expanded in this way is no longer stenotic.
Types of stents
modern stents
Currently, in vascular surgery, stents made of an alloy of cobalt and chromium are used in the form of wire, mesh, tubular and ring structures. The main qualities of stents should be radiopacity and good survival in the lumen wall.
Recently, many stents are coated with drugs that prevent the growth of the inner wall of the vessel (intima), and thus reduce the risk of repeated stenosis (restenosis). In addition, such a coating prevents the sedimentation of blood clots on a foreign body in the lumen of the vessel, which is the stent.
Thus, drug coating reduces the risk of recurrent myocardial infarction.
The design of the stent for a particular patient is directly selected by the treating cardiac surgeon. Today, there is no fundamental difference between the shape of stents, since they are all designed in accordance with the anatomical differences in different patients and fully perform their function.
How is stenting different from bypass surgery?
Both operations are currently used as radical treatments for coronary artery stenosis. But they differ significantly from each other. The operation of stenting the heart vessels is the introduction into the human body of a kind of conductor that helps the stenotic artery to function normally. The stent is a foreign body.
In coronary artery bypass grafting (CABG), the patient's own artery or vein is used as a vessel that allows blood flow to the heart. That is, a bypass path is created that overcomes the obstacle in the form of a site of stenosis, and the affected coronary artery is switched off from the blood flow.
Indications for stenting surgery
The operation of coronary stenting is indicated for patients with the following forms of coronary heart disease:
- Progressive angina - increased frequency, duration and intensity of attacks of chest pain that are not relieved by taking nitroglycerin under the tongue,
- Acute coronary syndrome (pre-infarction condition), threatening the development of acute myocardial infarction in the near future without treatment,
- Acute myocardial infarction,
- Early post-infarction angina - attacks of heart pain that occur in the first weeks after an acute heart attack,
- Stable angina FC 3-4, when frequent, prolonged painful attacks significantly reduce the patient’s quality of life,
- Repeated stenosis or thrombosis of a previously installed stent or shunt (after coronary artery bypass surgery).
stenosing atherosclerosis of the coronary arteries is the main prerequisite for surgery
A drug-eluting stent is preferred in the following categories of patients:
- Persons with diabetes mellitus, impaired kidney function (patients receiving hemodialysis),
- Persons at high risk of developing restenosis,
- Patients who have undergone bare stent surgery and develop restenosis
- Patients with repeated graft stenosis after CABG surgery.
Contraindications for surgery
For emergency reasons, for example, in case of acute myocardial infarction, a stent can be installed even in a patient in serious condition, if it is caused by cardiac pathology. However, surgery may be contraindicated in the following cases:
- Acute stroke,
- Acute infectious diseases,
- End-stage liver and kidney failure,
- Internal bleeding (gastrointestinal, pulmonary),
- Disorders of the blood coagulation system with a high risk of life-threatening bleeding.
Preparation and performance of the operation
Stenting can be performed urgently or routinely. In emergency surgery, coronary angiography (CAG) is first performed, based on the results of which a decision is immediately made to introduce a stent into the vessels.
Preoperative preparation in this case comes down to the introduction of antiplatelet agents and anticoagulants into the patient’s body - drugs that prevent increased blood clotting (to avoid thrombosis).
As a rule, heparin and/or clopidogrel (warfarin, Xarelto, etc.) are used.
Before a planned operation, the patient must perform the necessary research methods to clarify the degree of vascular damage, as well as assess the contractile activity of the myocardium, the ischemic zone, etc.
For this, the patient is prescribed CAG, ultrasound of the heart (echocardioscopy), standard and stress ECG, transesophageal electrical stimulation of the myocardium (TEPS - transesophageal electrophysiological study).
After all diagnostic methods have been completed, the patient is hospitalized in the clinic where the operation will be performed.
The evening before the operation, a light dinner is allowed. It is likely that some cardiac medications will need to be discontinued, but only as directed by the attending physician. Breakfast before surgery is not allowed.
Stenting itself is performed under local anesthesia. General anesthesia, dissection of the chest and sternum, and connection of the heart to a heart-lung machine (ACB) are not required.
At the beginning of the operation, local anesthesia of the skin is performed in the projection of the femoral artery, which is accessed through a small incision. An introducer is inserted into the artery - a conductor, through which a catheter with a stent installed at the end is brought to the affected coronary artery.
Under the control of X-ray equipment, the exact position of the stent at the site of stenosis is monitored.
Next, the balloon, which is always inside the stent in a compressed state, is inflated using air injection, and the stent, being a spring structure, is straightened out, tightly fixed in the lumen of the artery.
After this, the catheter with the balloon is removed, a tight aseptic dressing is applied to the skin incision, and the patient is transferred to the intensive care unit for further observation. The entire procedure lasts about three hours and is painless.
After stenting, the patient is observed for the first day in the intensive care unit, then transferred to a regular ward, where he remains for about 5-7 days until discharge from the hospital.
Possible complications
Thus, intraoperative (during surgery) complications are the occurrence of life-threatening arrhythmias (ventricular fibrillation, ventricular tachycardia), incision of the coronary artery (dissection), and extensive myocardial infarction.
Early postoperative complications are acute thrombosis (sedimentation of blood clots at the site of stent installation), aneurysms of the vascular wall with the possibility of rupture, and cardiac arrhythmias.
A late complication after surgery is restenosis, the growth of the inner lining of the vessel onto the surface of the stent from the inside with the appearance of new atherosclerotic plaques and blood clots.
Prevention of complications consists of careful X-ray monitoring of stent installation, the use of the highest quality materials, as well as taking the necessary medications after surgery to treat atherosclerosis and reduce blood clots.
The correct attitude of the patient also plays a significant role here, because in any field of surgery it is known that in positively minded patients the postoperative period proceeds more favorably than in persons predisposed to anxiety and restlessness.
Moreover, complications develop in less than 10% of cases.
Lifestyle after surgery
As a rule, in 90% of cases, patients note the absence of angina attacks. However, this does not mean that you can forget about your health and continue to live as if nothing had happened. Now you must take care of your lifestyle and, if necessary, correct it . To do this, just follow simple rules:
- Stop smoking and drinking strong alcoholic drinks.
- Follow the principles of healthy eating. There is no need to exhaust yourself with constant starvation diets in the hope of normalizing high cholesterol levels in the blood (as the basis for the development of atherosclerosis). On the contrary, you should get proteins, fats and carbohydrates from food, but their intake should be balanced, and the fats should be “healthy”. Fatty meats, fish and poultry should be replaced with lean ones, and fried foods and fast food products should be completely eliminated from the diet. Get more greens, fresh vegetables and fruits, dairy products. Also useful are cereal products and vegetable oils - olive, flaxseed, sunflower, corn.
- Take medications prescribed by your doctor - lipid-lowering drugs (if cholesterol levels are high), antihypertensive drugs, antiplatelet agents and anticoagulants (under monthly monitoring of blood clotting). Particular attention should be paid to prescribing the last group of drugs. So, in the case of installing a simple stent, “double prevention” of its thrombosis consists of taking Plavix and aspirin in the first month after surgery, and in the case of a drug-coated stent - in the first 12 months. Premature stopping of taking medications according to the regimen prescribed by the doctor is unacceptable.
- Avoid significant physical activity and sports. Loads adequate to the patient’s condition in the form of walking, light jogging or swimming are sufficient.
- After the operation, visit a cardiologist at your place of residence according to his appointments.
- Stenting is not a disabling operation, and if the patient remains able to work, he can continue to work.
Prognosis, life expectancy after surgery
Life expectancy also increases - more than 90% of patients live quietly in the first five years after surgery. This is also evidenced by reviews from patients whose quality of life improves significantly.
According to patients and their relatives, angina attacks almost completely disappear, the problem of constant use of nitroglycerin is eliminated, the patient’s psychological state improves - the fear of death during a painful attack disappears.
The patient’s relatives, of course, also become calmer, because the coronary vessels become patent, which means the risk of a fatal heart attack is minimal.
Where is stenting performed?
Currently, the operation is widespread and is performed in almost all major cities of Russia.
So, in Moscow, for example, today there are many medical institutions that practice stenting of heart vessels. Institute of Surgery named after. Vishnevsky, Volyn Hospital, Research Institute named after. Sklifosovsky, cardiac center named after.
Myasnikov, Federal State Budgetary Institution named after. Bakuleva is not a complete list of hospitals providing such services.
Stenting refers to high-tech medical care (HTMC), and can be carried out under the compulsory medical insurance policy (in an emergency) or under a quota allocated from the regional budget (in a planned manner).
To obtain a quota, you must submit an application to the regional department of the Ministry of Health, with attached copies of medical studies confirming the need for the intervention. If the patient can afford to pay for the operation, he can be operated on a paid basis.
Thus, the approximate cost of the operation in Moscow is: preoperative coronary angiography - about 10 thousand rubles, installation of an uncoated stent - about 70 thousand rubles, with a coating - about 200 thousand rubles.
Which is better - CABG or stenting?
Only a cardiac surgeon can answer this question regarding each specific patient with angina during an in-person examination . However, some benefits have been identified for both treatments.
Thus, stenting is characterized by a less traumatic operation, better tolerance by patients, and no need for general anesthesia. In addition, the patient spends fewer bed days in the hospital and can start working earlier.
Bypass surgery is performed using one’s own tissues (veins or arteries), that is, there is no foreign body in the body. Also, the likelihood of re-stenosis of a bypass is lower than that of a stent. If the patient has diffuse damage to the coronary vessels, bypass surgery can solve this problem, unlike a stent.
Source: https://otlichaem.ru/obshhestvo/chem-otlichaetsya-shuntirovanie-ot-stentirovaniya.html