Malformation - what is it?
In this pathological condition, additional formation of vessels occurs in the organ, which connect the arterial, venous and lymphatic parts of the blood supply system. The result of such deformation is the discharge of blood and disruption of the nutrition of the area located just below the affected area.
One of the most common diagnoses in medicine is AVM—arteriovenous malformation of cerebral vessels. This disease is characterized by disruption of the connections between arteries and veins, resulting in impaired blood flow. Additional connections look like saccular nodes, and capillaries are completely absent, which leads to accelerated blood supply.
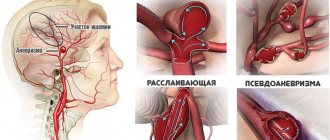
This anomaly occurs with continuous expansion, and subsequently possible damage to blood vessels. When they reach critically large sizes, a threat to the normal functioning of the brain arises.
The disease has the appearance of large pulsating vessels. The size of the vascular malformation may vary in each individual case.
This pathology most often manifests itself in men over 30 years of age.
Classification
Vascular malformation located in the brain can consist only of veins, arteries, or be a combination. The last option, arteriovenous, is the most common.
Based on the type of structure, cerebral AVMs are divided into:
- Racemose (account for ¾ of the total) - a branched vascular conglomerate.
- Fistulous - is a massive shunt between large vessels.
- Cavernous - a cluster of thin-walled cavities that externally resemble mulberries (diagnosed in 11% of AVM cases).
- Micromalformation is a small-sized formation.
Among the isolated ones, venous malformation, arterial, and telangiectasia are distinguished. Anomalies are also distinguished by size. The diameter of small ones does not exceed 30 mm, medium ones - 60 mm, and large ones are tangles larger than 6 cm. The localization of the defect is important for diagnosis and treatment: in mild cases they are located outside functionally significant areas, which include the brain stem, temporal and occipital lobes , thalamus, sensorimotor cortex, speech area, Broca's area. The nature of drainage is also important, that is, the presence of access to large veins.
The listed classification parameters are important for determining the risk in the event of surgery. Each of them (location, type of drainage, size) is assessed on a three-point scale, and depending on the amount of points scored, the operational risk is determined. Low is 1, and five means increased technical complexity of the intervention, a high probability of disability or death.
Forms of the disease
Modern medicine divides brain malformation into several forms:
- Arteriovenous malformation is a type of disease characterized by a complete absence of capillaries connecting the venous and arterial networks.
- Lymphatic pathologies are disorders in which the patient has problems with the lymph nodes. The peculiarity of this form is the frequent absence of a tumor.
- Arnold-Chiari malformation is characterized by displacement of the cerebellum towards the foramen of the occipital lobe, resulting in compression of the medulla oblongata.
Where can an AVM be located?
Cerebral arteriovenous malformations can originate and develop in any part of the brain, both on its surface and in deep areas. In addition, the onset of pathology can occur between the pulmonary trunk and the aorta.
Spinal cord AVM
This disease most often originates in the lower parts of the spine. In the initial stages it is asymptomatic, but after a while it can result in severe loss of sensation in the back area. Can lead to hemorrhage in the spinal cord.
Arteriovenous malformation between the pulmonary trunk and the aorta
The pulmonary trunk is one of the largest blood vessels in humans, starting from the right ventricle, and the aorta is a large unpaired arterial vessel of the systemic circulation.
The embryo must have connections between the heart and blood vessels - the arterial flow. After birth, it begins to overgrow, and if this does not happen, then the unovergrown arterial flow is considered a congenital heart defect.
The disease, which originates and develops in this part of the body, provokes the most painful manifestations and complications.
Indications and choice of treatment method
To date, three methods of treating AVMs are used: direct microsurgical removal, endovascular embolization and radiation treatment. Indications for the use of each method have been sufficiently developed. In some cases, a combination of techniques is used. To determine the possibility of direct microsurgical excision of the malformation, the Spetzler-Martin classification is used, which takes into account the size of the AVM, its localization in relation to functionally important areas of the brain and the characteristics of blood drainage.
| Classification of Spetzler-Martin AVMs | |
| Feature being assessed | Points |
| Size Small (<3 cm) Medium (3-6 cm) Large (>3 cm) | 1 2 3 |
| Localization (by functional significance) Insignificant Significant | 0 1 |
| Type of venous drainage Only into superficial veins Also into deep veins | 0 1 |
The size of the AVM is determined by the maximum size of the tangle in centimeters. Functionally important areas include areas of the brain, damage to which is likely to lead to severe, persistent neurological deficits. Venous drainage is assessed as “superficial” if all drainage is into the cortical veins or sinuses. If at least one of the drainage veins flows into the network of deep veins, then the outflow is considered “deep”. The Research Institute of Neurosurgery has developed the following tactics for treating patients with AVM after hemorrhage. For patients with hemispheric AVMs SM 1-3, excision of the malformation is indicated. If necessary, the stroma is first embolized and available afferents are switched off. AVMs localized in functionally significant areas or deep structures are sent for irradiation. Patients with SM 4-5 AVMs are referred for radiation therapy or observation. In some cases, patients with SM 4 AVM can undergo removal of the malformation. AVM embolization can be considered as an independent method in a small group of patients with small compact AVMs that have one or more large afferents. For unruptured AVMs, management tactics are more conservative. If there are no or minimal clinical symptoms, observation is warranted. In the case of convexital AVMs SM 1-3 in young and middle-aged patients, “active” tactics are possible - embolization followed by removal or irradiation of the AVM. Radiation treatment can be recommended for patients with SM 1-3 AVMs localized in functionally significant areas. Patients with AVM SM 4-5 remain under dynamic observation. In elderly patients, observation is usually limited.
Causes
This pathology is congenital, and the reliable and exact causes remain unknown to modern medicine. The main assumption is that trauma and intrauterine malformations of the fetus have a negative impact on the formation and structure of blood vessels.
Medical specialists were able to identify risk groups:
- male gender, since the vast majority of the disease affects men;
- genetic mutations;
- infectious diseases that the mother suffered during pregnancy;
- bad habits that a woman suffers from during pregnancy, such as smoking, excessive consumption of alcohol and medications;
- fetal injuries.
These are the main factors influencing the possibility of developing pathology.
Symptoms that should alert you
The size of the malformation can vary from small to large. The largest lesions can cause large hemorrhages and epileptic seizures in humans. If the lesions are small, then the symptoms do not manifest themselves and do not make themselves felt for a long time.
The most common symptoms of this disease:
- frequent attacks of headache;
- partial or complete loss of vision;
- loss of sensation in the limbs;
- muscle weakness;
- frequent convulsions, possible loss of consciousness;
- speech problems;
- lethargy, general malaise, inability to work.
Variants of manifestation of the disease
Doctors distinguish the following groups of the disease according to the clinical picture:
- The torpid nature of the course is characterized by headaches, frequent dizziness, and nausea. Since such manifestations also apply to many other diseases, it is impossible to determine problems with the blood vessels of the brain from them. The affected area is located in the cortical areas of the brain.
- Hemorrhagic character is inherent in 75% of patients suffering from this pathology. The hemorrhage may be small, and in this case there will be no significant symptoms. However, if the hemorrhage turns out to be massive, then vital brain centers will be at great risk of disruption. Symptoms may include the following: impaired speech and coordination, impaired hearing and vision. The worst option is death.
- Neurological character occurs with spinal cord injuries. The vessels, expanding, compress the nerve roots and endings. The result is pain in the back and lumbar region, as well as numbness of all extremities and decreased sensitivity of the skin.
Manifestation of the disease in a child
It is difficult to identify such a disease in young children, because at an early age it is practically asymptomatic, but there are some signs that may indicate the development of malformation in a child:
- speech defects, decline in intelligence, unstable gait, frequent convulsions;
- loss of coordination, shifty eyes, decreased muscle tone;
- partial visual impairment.
Radiation treatment of brain AVM
| Leksell Gamma Knife |
Radiation therapy (gamma knife, proton beam irradiation) is most effective for small compact malformations with a diameter of no more than 3 cm. Thus, with malformations less than 1 cm in diameter, complete obliteration can be achieved in almost 90% of cases, and with malformations with a diameter of more than 3 cm only - up to 30%. The negative side of radiation therapy for AVM is that obliteration of the AVM vessels occurs 1–3 years after treatment. Recent studies have shown that pre-embolization of AVM reduces the effectiveness of radiosurgery. According to the Research Institute of Neurosurgery, after stereotactic irradiation, complete obliteration can be achieved in more than 70% of cases. In 10% of patients, a decrease in the size of the AVM and a reduction in blood flow is observed.
Diagnostics
Vascular malformation can be diagnosed during examination by a neurologist. He prescribes several types of examinations and then makes a final diagnosis.
The following methods are used to diagnose the disease:
- Arteriography is the most common examination method. This procedure involves inserting a special instrument in the form of a tube containing a contrast agent into the femoral artery. The tube passes into the blood vessels of the brain. The chemical compound contained in the device allows you to determine the current state of the blood vessels.
- Computed tomography is often used in conjunction with arteriography, in which case the procedure is called angiography. The diagnostic picture is revealed in a similar way: through x-rays and chemical compounds, the condition of the blood vessels can be revealed.
- When it comes to arteriovenous malformation, magnetic resonance imaging is considered the most effective. For diagnostics, not X-rays are used, but magnetic particles.
How to identify arteriovenous malformation?
Diagnostics begins with:
- careful determination of neurological status;
- blood pressure measurements;
- assessing the condition of the skin and gait;
- patient complaints;
- survey regarding the course of pregnancy.
Persons with this pathology are advised to:
- Doppler ultrasound. Allows you to evaluate the structure of veins and arteries, blood circulation in them;
- radiographic angiography. To visualize the vessels, a contrast agent is injected, which “illuminates” them;
- computed angiography. With its help, you can recreate a 3D picture of human blood vessels;
- magnetic resonance angiography. A high-precision method for determining arteriovenous malformation allows you to evaluate the shape, structure, and blood circulation in damaged vessels;
- ultrasound examination of the heart. For the diagnosis of patent ductus arteriosus. You can also evaluate the ejection fraction; if it is more than 70%, then this indirectly allows us to judge the presence of malformation.
Treatment
The method of treatment depends on the location of the pathology, its type, severity of symptoms and individual characteristics of the patient. Any of the methods is aimed at achieving complete blockage of blood vessels in order to prevent hemorrhage.
If a patient suffers from frequent and severe headaches, he should be prescribed painkillers.
If the patient is bothered by incessant seizures, then doctors select appropriate anticonvulsant therapy to avoid brain swelling and death of nerve cells.
There are cases when it is enough for a patient to be examined by a neurologist and take prescribed medications that reduce the risk of choroid plexus rupture. However, this option is possible only in the absence of severe symptoms and complaints from the patient.
In all other cases, doctors resort to surgery. Pathological foci are removed, the vascular walls, where there were improperly fused vessels, are soldered. This is done to normalize blood flow and circulation in the brain.
There are 3 surgical methods in total:
- Surgical resection is one of the most effective types of surgery to get rid of malformation. This neurosurgical procedure is complex and is prescribed mainly in situations where the pathological choroid plexus is located shallowly and is small in size.
- Embolization is a procedure performed before surgery, which is used for deep-lying abnormal vascular plexuses and large pathologies. With this method, a special substance is injected into the vessel to block blood flow.
- Radiosurgery destroys damaged vessels and completely eliminates the malformation. The operation does not require the use of a surgical knife, since it involves irradiating the patient with protons. This eliminates possible infection of the patient. The procedure is used if the pathology is small in size and located at great depth.
About complications
Complications include:
- Rupture of arterial and venous malformations, leading to bleeding and circulatory impairment. The result is an increased load on the vascular walls, and this can lead to a hemorrhagic stroke.
- Due to abnormal vascular plexuses and impaired blood circulation, a lack of oxygen in the brain tissue can occur, and as a result, their gradual death occurs. This will lead to a cerebral infarction.
- If strong compression occurs by a large choroid plexus, the possibility of paralysis increases.
To avoid complications, it is necessary to begin a course of treatment for malformation as quickly as possible.
Why is arteriovenous malformation dangerous?
It is a very dangerous and insidious disease, since its complications are always sudden and with a high probability can cause death or disability of a person. There are:
- intracerebral, intraventricular and subarachnoid (in the cavity between the arachnoid and soft membrane) hemorrhages. Occurs in 55 - 65% of cases. Symptoms are similar to those of a stroke: numbness of the limbs, difficulty speaking, impaired vision and coordination, sudden onset of severe headache;
- epileptic seizures in about 25 - 40% of cases;
- disruption of adequate blood supply to the brain leads to the death of a significant part of the neurons and, as a consequence, this leads to significant impairments in speech, intellectual abilities, and in some cases to paresis or paralysis of various parts of the body.
Arteriovenous malformations of internal organs are rarely complicated; an asymptomatic course of the disease is more typical for them.
Forecast
The prognosis for arteriovenous malformation of the brain depends on the location of the pathology, its size and the stage at which it was detected.
How to live with this disease?
You can live normally with this pathology, but only if it is diagnosed in time and appropriate treatment is carried out.
Prognosis for brain AVM
Statistics show that in more than 50% of cases the first symptom is hemorrhage, as a result of which 15% of patients die and 30% become disabled.
At an early stage, the disease is detected extremely rarely, since it is not accompanied by any other symptoms.
Diagnosis is possible only by undergoing a preventive examination. The likelihood of hemorrhage is high even if the patient has no complaints. The possibility of hemorrhagic stroke increases every year.
Consequences and forecasts
The most likely outcome of the malformation is its rupture with all the specific symptoms and consequences of a hemorrhagic stroke. The degree of disability and the likelihood of death depend on the volume and location of the hemorrhage. Repeated ruptures increase the mortality rate. However, it is possible to live to an advanced age without surgery, which is observed in approximately half of AVM cases.
If characteristic brain symptoms appear in the form of headaches, epileptic seizures, contacting a neurologist and starting treatment will help avoid complications. What is the recovery rate after surgery? Radiosurgical and classical removal – 85%, embolization – about 30%. In combination, these techniques are more effective and give almost one hundred percent results. The most likely postoperative complication is stroke.