The increase in cases of vascular diseases, heart diseases, and atherosclerosis of the aorta requires a constant search for a solution to this problem, so scientists and doctors are actively working on the invention of new diagnostic and treatment methods. In addition to traditional drug treatment and standard recommendations for controlling the progression of the disease, endovascular surgical methods have now been widely introduced into everyday medical practice.
Their meaning is the non-invasive delivery of a drug or a special device for the purpose of embolization of a vessel, restoration of its lumen, removal of thrombotic masses, as well as in oncology for targeted effects on the tumor using chemotherapy and radiation therapy.
Indications and contraindications
Medical removal of a cerebral aneurysm is possible only in a few cases.
Indications for the most common type of surgery – clipping: aneurysm larger than 7 mm, predisposition to rupture of the swollen sac. Before surgery, you must ensure that there are no contraindications. Surgeries cannot be performed if there are blood diseases. Interventions are prohibited in case of decompensation of diabetes, as well as in acute inflammation or infection of various etiologies.
Clipping of cerebral arteries is prohibited if the pathology is deep.
Intervention is not allowed in cases of exacerbation of chronic diseases, as well as in severe cases of bronchial asthma.
Indications for trepanation
The reasons for the operation are conditions, diseases in which the functioning of the brain and blood circulation are disrupted due to pathologies that compress the brain structures and blood vessels:
- traumatic brain injuries;
- inflammatory processes;
- increased intracranial pressure;
- blood clots, emboli, aneurysm of cerebral vessels;
- hemorrhages;
- abnormalities of the skull;
- tumors;
- cavities with blood clots and other fluid.
What is the danger of a cerebral aneurysm?
Pathophysiology determines several locations of the aneurysm:
- abdominal aorta (the vast majority of all aneurysms);
- thoracic aorta;
- cerebral vessels;
- heart;
- peripheral arteries on the extremities (in very rare cases);
- aneurysm of the splenic branch of the aorta.
The severity and consequences of aneurysm rupture depend entirely on the location of the affected vessel.
Causes
The appearance of a vascular aneurysm can be caused by a number of reasons:
- infectious diseases, in particular syphilis;
- atherosclerosis is the most common cause that affects older people;
- blunt abdominal trauma (abdominal aortic aneurysm);
- hypertonic disease;
- smoking and drug use (especially cocaine);
- menopause in women;
- myocardial infarction.
Statistics show that aneurysm develops in adults over 30 years of age. Women hold the championship. Among them, the mortality rate is also higher.
What are the causes of rupture of an aneurysm? This could be a stressful situation, a sharp jump in blood pressure, increased physical activity, heavy lifting, or the condition of the aneurysm itself. It can burst in people under the influence of alcohol or at a very high body temperature.
Signs of the development of an aneurysm are not always obvious, especially in the early stages, which allows a person to feel well and not see a doctor. This is precisely the insidiousness of the disease. Painful sensations begin to appear as it grows, as it begins to put pressure on surrounding tissues.
Abdominal
With the growth of an abdominal artery aneurysm, periodic pain occurs in the left hypochondrium, which can radiate to the back. Other signs of abdominal aortic pathology:
- pulsation in the area of the buttocks and thoracic region;
- cyanotic feet as a result of the formation of blood clots that clog peripheral vessels, as a result of which blood circulation in the lower extremities worsens;
- weight loss, accompanied by a feverish state caused by inflammation in the pathologically altered aorta.
Small aneurysms of this location rarely rupture. If the diagnosis is made in a timely manner and adequate treatment is prescribed, then there is nothing to fear.
Thoracic
If the formation is located in the thoracic region (thoracic aneurysm), then as it grows, the following appears:
- difficulty breathing and swallowing;
- cough;
- loss of voice;
- heavy snoring;
- dull pain in the chest, radiating to the back.
Cerebral
Brain aneurysms (cerebral) are manifested by more serious signs that cannot be ignored:
- double vision;
- pain behind the eyeballs;
- partial loss of sensation and limitation of movements;
- eyelid ptosis;
- ringing in the ears.
The signal symptom is prolonged headaches that do not stop for several days. They say that the vessel can burst at any moment. This condition requires immediate medical attention.
Thinning vessel walls can allow microscopic blood leaks into the surrounding nerve tissue, causing irritation. People suffering from vascular aneurysms can suffer up to two dozen minor hemorrhages throughout their lives. Sometimes these symptoms are not clearly expressed and may be attributed to another neurological pathology.
Heart
Protrusion of the heart wall is typical for people who have had a heart attack or have weakened heart muscles due to persistently high blood pressure. The causes of an aneurysm are post-infarction scars and areas of dead tissue as a result of oxygen starvation. Pathology of the heart wall has two forms - acute and chronic.
- interruptions;
- dyspnea;
- soreness.
Cardiac aneurysm can be congenital and is diagnosed in newborns. The first examination by a cardiologist reveals pathology.
The following symptoms can indicate a suspicion of rupture of a cerebral aneurysm:
- sudden severe headache;
- photophobia;
- nausea and vomiting;
- confused consciousness and its loss;
- visual impairment;
- increased tone of the neck muscles.
The consequences of a ruptured abdominal aortic aneurysm can be very serious. It can be recognized by the following symptoms:
- a sharp drop in blood pressure;
- pale skin;
- loss of consciousness;
- strong heartbeat.
The severity of the condition is due to hemorrhagic shock. Blood under pressure is poured into the abdominal cavity, and also enters the esophagus, trachea and pleural cavity. The only salvation in this case is urgent surgery.
Rupture of a thoracic aneurysm is often fatal. The aorta is the largest vessel in the body and bleeding from it is usually massive, under high pressure. If a rupture occurs in the abdominal cavity, the person simply dies from blood loss. Symptoms:
- sharp pain throughout the abdomen;
- anemia;
- pallor;
- drop in blood pressure;
- shock;
- collapse.
When hemorrhage into the retroperitoneal cavity, the hematoma compresses the iliac arteries, which causes ischemia of the lower extremities with loss of temperature and pain sensitivity. When the vessels supplying the spinal cord are compressed, ischemia may occur.
The radical way to treat an aneurysm is surgery. However, the risk of surgery is quite high, so small aneurysms are not treated in this way. You just need to see a doctor and, if possible, eliminate the causes that may cause its growth.
To avoid rupture of a cerebral aneurysm, patients with an already established diagnosis are prescribed treatment aimed at minimizing this risk. It helps to stop the growth of pathology and consists of taking medications that normalize blood cholesterol, blood pressure and heart rate.
If the aneurysm does burst, then treatment is similar to the treatment of hemorrhagic stroke. In some cases, surgery is required. It is aimed at excluding the aneurysm from the bloodstream. If this is not done, the patient usually dies from repeated hemorrhages within a year.
Modern medicine has not yet found methods for preventing aneurysm. The best way is a healthy lifestyle, stress control and regular preventive medical examinations.
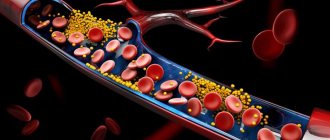
Approximately the same thing happens to the artery wall during an aneurysm. A thinned area forms on it, it bulges in the form of a “hernia”. The chamber of the ball is stretched due to high air pressure inside, the wall of the vessel is stretched due to high blood pressure.
Aneurysms occur not only in the brain, but also in other vessels. There are aneurysms of the thoracic and abdominal aorta, and cardiac aneurysms. They are all very dangerous.
Frequent locations of aneurysms in the brain
The exact causes of the development of intracranial aneurysms are not fully known. It is more appropriate to talk about risk factors - conditions that increase the risk of weakening and stretching of a section of the artery wall.
All risk factors can be divided into congenital and acquired.
Often, a baby is initially born with an abnormality in the artery wall. The following congenital factors contribute to the occurrence of cerebral aneurysms:
- Polycystic kidney disease is an inherited disease in which cysts form in both kidneys. Gradually the kidneys enlarge. In many patients, polycystic disease is asymptomatic, in some it is accompanied by some clinical manifestations, in particular, increased blood pressure, including in the vessels of the brain. This contributes to the formation of aneurysms.
- Hereditary disorders of connective tissue. One example is Ehlers-Danlos syndrome. Connective tissue is present in the walls of arteries and normally gives them strength. If its properties are violated, the vascular wall is also weakened.
- Arteriovenous malformations of the brain are “irregular” tangles of blood vessels in which arteries are directly connected to veins, without capillaries.
- Coarctation (narrowing) of the aorta after the arteries supplying the arms and head depart from it. As a result, little blood flows into the lower part of the aorta and into the vessels that supply many organs, and blood pressure rises in the vessels of the head and arms.
- Family history. If your immediate family (parents, children, siblings) has been diagnosed with an aortic aneurysm, your risk is also increased.
The occurrence of cerebral aneurysms can be provoked by head injuries, infections, cancer, drug use (in particular cocaine), atherosclerosis, smoking, and alcohol abuse. Some scientific studies have found evidence that the risks are increased when using oral contraceptives. Cerebral artery aneurysms occur more often in older people than in younger people. The pathology occurs more often in women than in men.
A cerebral aneurysm is a time bomb that a person carries in his body, often without even knowing it.
A cerebral aneurysm is dangerous because it does not make itself felt until it grows too large or ruptures. It can only be diagnosed by accident, when a person is examined for another pathology.
Current methods for diagnosing cerebral aneurysms
About 60-70% of cerebral aneurysms occur without severe symptoms. At the slightest suspicion of the presence or rupture of an aneurysmal sac, a full examination of the vascular system of the brain is performed. There are several ways to verify ABGM.
Selective cerebral angiography
This diagnostic technique is recognized as the most informative for the timely detection of brain pathologies: venous anastomosis, arterial aneurysms, occlusions, stenosis of certain areas of the vascular system. This study involves the introduction of a contrast iodine-containing solution, followed by recording its spread using X-ray equipment. There are several types of angiography:
Access to the target vessels is made through the right femoral artery. A specially shaped catheter is inserted through an introducer (anti-trauma tube with a valve) into the main arteries supplying the brain. Modern installations make it possible to obtain high-quality three-dimensional images of the vascular bed in real mode. When changing the projection (C-arm position), the integrated volumetric model will deviate accordingly on the demonstration monitor, helping to visually assess the real state of the vascular tree and find aneurysmal lesions.
Rotational angiography with 3D reconstruction is the most accurate method that helps to choose angulation with optimal display of the aneurysm neck and adjacent vessels, to build the right tactics for further treatment of intracranial aneurysmal formations of complex shape and difficult localization.
Examinations before surgery
The choice of type of operation is influenced by the test results. It is also necessary to undergo them to exclude contraindications:
- general blood test and biochemistry;
- Analysis of urine;
- X-ray examination;
- MRI, in which the aneurysm will be larger than 3 mm;
- computed tomography for a tumor over 5 mm - done to determine blood clots and other defects inside the tumor;
- cardiogram;
- examination by other doctors depending on the symptoms of the disease;
- angiography – detects tumors up to 3 mm.
The reliability of the results obtained is the key to a successful operation and the absence of serious consequences after its implementation. Before the procedure itself, they also visit the surgeon and anesthesiologist, and agree on the date of the intervention.
12-16 hours before admission to the surgical department, a person must refuse to eat, and before the operation itself, he must not drink (the doctor will prescribe the exact time intervals).
After open surgery, the body needs 2 to 4 months to fully recover and eliminate the consequences. When treating an arterial aneurysm endoscopically, the recovery time is significantly reduced. Recovery Features:
- for several days there is pain in the area of intervention, when the wound begins to heal, itching appears;
- in some cases, the consequence after removal of the aneurysm is swelling and numbness in the suture area;
- within 2 weeks, it is considered normal for headaches, fatigue and anxiety to persist;
- up to 8 weeks, similar symptoms persist during open surgery;
- During the year, the patient should not engage in contact sports or lift weights exceeding 3 kg;
- You can’t sit for a long time.
After 6 weeks, the patient is allowed to start work if it does not involve physical activity.
As prescribed by the doctor, it is necessary to undergo MRI and CT, as they help monitor postoperative recovery.
After completion of the rehabilitation period, there remains a need for MRI every 5 years to exclude re-formation of the aneurysm. In general, reviews after surgery are positive. The most common side effects include deterioration of well-being due to sudden changes in weather.
Treatment
The only effective method is surgical treatment. All patients with aneurysms should be subject to it, regardless of their size, structure, structural features of the wall, or how old the aneurysm is. The choice of surgical treatment depends on the localization of the pathology, the presence or absence of aneurysm rupture, the time elapsed since the rupture, the general condition of the patient, the presence of complications and the necessary equipment, and the qualifications of the surgeon. In case of multiple aneurysms, it is advisable to remove them on the same day.
Patients with an unruptured aneurysm do not undergo emergency removal. The operation is carried out as planned (the timing is determined in advance, the patient is prepared), since the risk of spontaneous rupture of the aneurysm does not exceed 2-5% per year. Patients with a ruptured aneurysm require prompt surgical treatment to stop blood flow to the defect. This is due to the rapid development of complications, with a 20-25% chance of developing a re-rupture within the next 14 days. Each repeated rupture becomes more and more difficult.
Timing of the operation
In the next 3 days and within 2 weeks from the moment of hemorrhage, surgical intervention is indicated for all patients without complicated vascular pathology. The operation can be performed only when the patient’s condition is compensated, in persons with a high risk of re-bleeding, or with severe spasm of the cerebral arteries. The choice of surgery depends on the severity of oxygen deficiency in the brain. If the patient's condition is satisfactory, surgery can be performed immediately after diagnosis. If compensation is incomplete, observation of the patient is indicated followed by a decision to perform surgery; if there is improvement, surgery can be performed. In case of decompensated condition, surgery is postponed until the condition improves.
If there is a high risk of death, all patients with acute compression (compression) of the brain due to the presence of a hematoma, severe impairment of the outflow of brain fluid from the ventricles of the brain, displacement of the brain stem, and large areas of impaired blood flow to the brain tissue are subject to surgery. For such patients, surgical intervention is a vital step in the provision of resuscitation care. In these patients, the probability of death without surgery is 90-95%.
After 2 weeks from the moment of rupture of the aneurysm (delayed period), patients with a complicated course of the disease due to spasm of the cerebral arteries, those in serious condition, and patients who have suffered hemorrhage and those in a stable condition are subject to surgery. Also during this period, surgical removal of aneurysms located in hard-to-reach places can be performed. In the delayed period, preference is given to operations with the least trauma, since the risk of death has already been minimized.
The result of treatment depends on how quickly and completely it was possible to stop the flow of blood to the aneurysm. For treatment, one of two surgical options is used: open microsurgery or endovascular (transvascular) intervention. In rare cases, when patients are in serious condition, they resort to combination treatment. It consists of endovascular embolization (blockage) of the lumen of the artery, which provides blood flow to the aneurysm. After the patient's condition improves, open surgery is performed.
Types of operations
An open microsurgical operation is performed under anesthesia using a special microscope and microsurgical equipment. The effectiveness of stopping the blood supply to an aneurysm during open surgery is 95-98%. The essence of the operation:
- Craniotomy – opening of the skull;
- Opening of the dura mater;
- Dissection of the arachnoid membrane and isolation of large blood vessels of the base of the brain and aneurysm;
- Stopping blood flow to the aneurysm using clipping;
- Layer-by-layer elimination of tissue defects.
If it is not possible to perform open intervention, when the aneurysm is localized in a hard-to-reach place, in elderly patients, the aneurysm can be treated endovascularly. After surgery, it is possible to exclude the defect from the bloodstream in 86-88% of cases. The essence of the intervention is the introduction into the cavity of the aneurysm of a special detachable catheter-balloon or electrically detachable microscopic platinum spirals. The balloon leads to a mechanical cessation of blood flow, and the coil leads to the formation of blood clots that prevent the flow of blood into its cavity.
Postoperative period
After the operation is completed, regardless of the patient’s condition, he is transferred to the neuro intensive care unit, where he is under constant monitoring. The patient is prevented from complications. If within 24 hours after surgery the patient’s condition remains satisfactory or moderate, he is transferred to the neurosurgery department. If the condition worsens, an emergency computed tomography (CT) scan of the brain is performed. After receiving the results of the examination, the issue of subsequent treatment tactics is decided.
Consequences
Surgical removal of the aneurysm before it ruptures and compliance with all operating rules allows you to minimize the likelihood of adverse effects and complications.
The average postoperative mortality does not exceed 13%.
Possible consequences after surgery:
- Increased thrombus formation;
- Development of cerebral edema;
- Attachment of infection;
- Stroke;
- Epilepsy;
- Convulsive syndrome;
- Speech disorders;
- Vision problems;
- Memory impairment;
- Impaired balance and coordination of movements;
- Decreased mental capacity.
Embolization of neoplasms
Embolization of a cerebral aneurysm is an endovascular surgical penetration into the skull, the purpose of which is to separate the neoplasm from the general bloodstream:
- a part is inserted into the vessel - a hose through which neurosurgical instruments are immersed;
- using an instrument, the doctor cuts off the blood supply to the aneurysm;
- using guides and catheters, they manipulate instruments, and also use neurosurgical video equipment;
- To separate the tumor, special balloons are used, thanks to which embolization of the cerebral aneurysm is successful;
- when the balloon is in the right place, it is filled with a special solution;
- once inflated, the balloon reliably protects the aneurysm from the flow of additional blood;
- After some time, the blocked vessel heals and the aneurysm passes.
Endovascular treatment of arterial cerebral aneurysms is a minimally invasive technique, but it is carried out only under general anesthesia. There is no need for stitches afterwards, and infection is not a common consequence of the procedure. The only remaining risk, as with other surgical interventions, is that the procedure is performed incorrectly.
Another consequence of endovascular treatment of arterial cerebral aneurysms is damage to the walls of the tumor. However, the complication in this case occurs directly in the operating room and can be treated by surgeons.
Osteoplastic trepanation
Unlike decompression trepanation, in this case there is no typical location for removing the bone fragment. The hole is made in the part of the skull in which the path to the pathological formation will be the shortest. At the first stage, dissection of soft tissues is also performed. It is best to cut the skin flap in a horseshoe shape to make it easier to stitch it back in the future.
At the next stage, the surgeon creates an osteoperiosteal flap. Here, the neurosurgeon also drills holes in the skull, between which sections of bone are subsequently cut out using a special saw. Since restoration of the bone area will be planned at the final stage, one “bridge” is not sawed off, but broken, so as not to damage the periosteum that feeds the bone.
Stages of osteoplastic trepanation
After this, the surgeon dissects the duramater and enters the cranial cavity, where he performs all the necessary manipulations. When the main operation is completed, all tissues are sutured in reverse order.
Who is at risk?
Cerebral aneurysm can occur at any age. This disease is more common in adults than in children and is slightly more common in women than men. People with certain inherited diseases are at higher risk.
The risk of cerebral rupture and hemorrhage exists with all types of cerebral aneurysms. There are about 10 reported aneurysm ruptures per year for every 100,000 people, which is about 27,000 people per year in the United States). Most often, aneurysm affects people aged 30 to 60 years.
Other factors that can contribute to aneurysm rupture are hypertension, alcohol abuse, drug addiction (especially cocaine use), and smoking. In addition, the condition and size of the aneurysm also influence the risk of rupture.
Top
Consequences after craniotomy
The severity of the consequences in the postoperative period depends on the reason for the operation, the age of the patient, and the presence of concomitant diseases. If neurological disorders were not immediately detected after trepanation, this does not mean that they will definitely not arise in the future. If the cerebral cortex is damaged, hearing and vision impairment of varying severity, up to complete loss, may occur.
The consequence may be a stroke due to thrombosis or thromboembolism. During trephination for abscesses, pathogenic flora may spread through the membranes of the brain, which will lead to meningitis and encephalitis. After many hours of anesthesia, disorders of the respiratory and cardiovascular systems are possible. If the neurovascular bundles are damaged, numbness, complete loss of sensitivity, and movement of certain areas of the skin, muscles, and limbs are possible. Postoperative consequences can manifest themselves in the form of mental and behavioral disorders.
Aneurysm clipping
Clipping of a cerebral aneurysm is performed on an open organ. The process requires craniotomy. The purpose of such an intervention, as with embolization, is to disconnect the neoplasm from the blood supply. The effectiveness of open intervention is much higher, but the operation cannot be performed if the aneurysm is deep.
When opening the skull, the doctor finds a bag filled with blood, and a clamp is applied to it. The process is controlled by an endoscope, and all manipulations are carried out with microsurgical instruments. The probability of complications after surgery does not exceed 8%, but the possibility of damage to the aneurysm sac is almost completely eliminated.
Features of the postoperative period
Brain surgery always causes consequences for the body. However, with proper rehabilitation and following the doctor’s recommendations, they can be overcome. Here's how the process begins:
- after the surgery department, the person is transferred to the neuro intensive care unit for several days;
- every day the surgeon examines the patient, studies the emerging consequences and prevents complications;
- if adverse symptoms occur, a computed tomography scan is performed;
- the most common consequences are vascular spasms and hypoxia of brain cells, sometimes hemorrhages occur under the arachnoid membrane;
- in the absence of exacerbations, clipping and other operations do not lead to death;
- if a large aneurysm was located near the basilar area, the risks increase;
- Also, the risk of mortality is high in people admitted with hemorrhage.
Disability after embolization of a cerebral aneurysm occurs only in 4% of cases. Statistics show that 8 out of 10 patients return to their normal lives, but only 4 of them begin working.
Complications after artery clipping occur in approximately 10% of cases. This 10% includes consequences such as:
- disturbance of attention, concentration;
- constant headaches;
- minor and significant speech problems;
- ischemia, pulmonary edema - in rare cases.
Mortality occurs only in very difficult situations. If possible, you should not refuse the operation.
In the first days after the intervention, to prevent the consequences of the operation, the patient is monitored by medical personnel. It is important to notice bleeding and other symptoms in time.
In the first days of recovery, the patient is prescribed nootropics, analgesics, diuretics and neuroprotectors if bleeding occurs.
Open trepanation and operations near brain tissue are complicated by additional consequences:
- repeated hemorrhages;
- infections and inflammations (in very rare cases);
- neurological disorders;
- necrosis of nervous tissue and neurological deficit - vasospasm.
During rehabilitation, the patient uses different methods: physiotherapy, massage, exercise therapy. After endoscopic clipping, you can return to your normal life within a week. At the same time, there is no need for complex physiotherapeutic procedures.
Under the constant supervision of specialists, the patient undergoes courses of massage, exercise therapy and physiotherapy, and also takes preventive medications.
To prevent consequences after surgery, it is also necessary to follow a diet. Doctors recommend sticking to it for the rest of your life:
- You should not eat animal fats, including lard and large amounts of butter;
- sharply limit fatty dairy products: cheeses, ice cream, processed cheeses, condensed milk, cream, cottage cheese and milk with high fat content;
- you cannot eat more than 2-3 yolks per week;
- minimize the consumption of fatty fish, canned food, squid, oysters and caviar;
- It is forbidden to eat a lot of sweets and starchy foods;
- Restrictions include polished rice and semolina;
- It is better to completely exclude peanuts, hazelnuts and pistachios from the diet;
- vegetables cooked with fat, only a little olive oil is allowed;
- store-bought sauces, spices;
- tea and coffee with cream, alcohol and soda.
During the diet, lean meat is consumed, and the skin is removed from fish and chicken. Stewed, boiled and steamed dishes are used. You should also minimize the amount of salt.
Technique for endovascular surgical interventions
If there is a narrowing of a vessel area that threatens the development of a stroke, restoration of its patency with the help of medical instruments is indicated. For this procedure, the patient is placed under general anesthesia and a contrast agent is injected intravenously.
At this time, he is on the operating table, the puncture site of the femoral vein is specially treated with antiseptic agents and covered with sterile sheets. An infusion catheter is placed in a peripheral vein, most often in the elbow area, so that solutions and anesthesia can be administered.
Vital signs are monitored using special equipment that is connected and records heart rate, blood pressure, electrocardiogram, and degree of blood oxygen saturation.
The operating room must have an X-ray unit, which can be used to monitor the progress of the catheter through the vessels to the designated area of the vessel. Then, a special occlusion device is placed into the vessel through the free end of the boat, or it must be secured in advance. Make sure that it is installed securely; one of the criteria is the complete restoration of blood flow.
Treatment of cerebral aneurysms is carried out using a spiral, the effect of which is opposite. Fibrin threads and blood cells settle on it, and thus a thrombus gradually forms, blocking the flow of blood and further enlargement of the aneurysm.
Endovascular embolization of a cerebral aneurysm has a similar effect, the drugs for which are delivered in the same way, through a catheter. After the site of protrusion or vascular malformation has been reached, a sclerosing substance, for example, alcohol-based, is injected.
A burn occurs on the inner surface of the vessel and the walls stick together. Blood flow through the pathologically altered vessel is stopped, the progression of the growth of the wall defect is stopped, and the likelihood of rupture and the occurrence of massive intracerebral bleeding is prevented.
Another, no less effective, method of treating vascular aneurysms is stereotactic radiosurgery. The procedure for exposing pathologically altered vessels to x-ray radiation absolutely does not require any incisions or punctures. A beam of gamma radiation passes through the tissue exactly to the location of the aneurysm. This is possible thanks to special calculations carried out by radiation therapy doctors; the radiation is not actually scattered, minimizing the impact on surrounding healthy tissue.
The patient's head is placed in a special fixing frame. It is secured with special screws. Before installation, the scalp is numbed on the forehead and back of the head. This installation guarantees reliable immobilization of the patient’s head and prevents accidental involuntary twitching. This also improves the accuracy of the gamma rays. As a result, thickening of the vessel wall also occurs, and complete occlusion can be achieved after several years; sometimes a repeated X-ray endovascular procedure is required.
After the manipulation is completed, a series of photographs are taken after a certain time in order to ensure the reliability of the blockage of the vessel. The catheter is carefully removed, and the puncture site is treated and sealed with a bandage, or a pressure bandage is applied. The duration of the operation, depending on the complexity, is about 30-40 minutes. After it, the patient is given bed rest for eight hours.
Cost and direction
Patients with an aneurysm apply for free surgery, either endoscopically or by opening the skull. To do this, you need to contact regional or district clinics, which are then referred to larger medical centers.
Surgery to remove an aneurysm is also available for a fee. An open one costs 20-50 thousand rubles, and an endovascular one costs from 15 thousand. But in Moscow and some large cities
The price usually includes consumables and payment for the work of all medical staff. Separate payments may be required for medications and time spent in a private room.
In general, the prognosis after removal of an aneurysm is favorable: 80% of patients recover successfully and do not suffer from severe consequences. When bleeding occurs, the mortality rate can reach 50%.
Signs of a ruptured aneurysm
- difficulties with perception and processing of information;
- decreased visual sharpness, the appearance of “blind spots”;
- difficulty moving, convulsions and involuntary movements;
- tingling, numbness, decreased sensitivity of different parts of the body;
- difficulty swallowing food;
- speech disorders;
- epileptic seizures;
- character changes, pronounced apathy or aggressiveness may appear;
- pain syndrome in different parts of the body;
- problems with bowel movements.
| Symptoms of hemorrhagic stroke | Symptoms of ruptured cerebral aneurysm |
| · Confusion or loss of consciousness. · Nausea, vomiting. · Sudden, severe headache. · Numbness, weakness (paresis) or paralysis in the right or left side of the body. · Dizziness, loss of balance. · Convulsions. · Disorientation. · Speech and swallowing problems. | · Sudden, very severe headache. · Nausea, vomiting. · Neck muscle tension. · Visual impairment, double vision. · Convulsions. · Increased sensitivity to light, photophobia. · Loss of consciousness. |
In both cases, not the entire set of symptoms may be present. In both cases, the patient's life is in danger and he needs immediate medical attention. If the person next to you complains of a sudden severe headache (the sensation is often compared to being hit on the head with a hammer) or loses consciousness, you should immediately call an ambulance.
After aneurysm rupture, the prognosis depends on several factors:
- Age and general health of the person.
- Pre-existing neurological pathologies.
- Location of the aneurysm.
- Bleeding intensity.
- The time elapsed from the moment the aneurysm ruptures until the start of medical care.
According to statistics, about 40% of patients after an aneurysm rupture die in the first 24 hours. Up to 25% die from complications within 6 months. The recovery period can last from several weeks to several months. Among the survivors, some recover almost completely, while others retain neurological disorders, sometimes very pronounced.
Factors that increase the risk of complications
Craniotomy always carries a certain risk of complications, but there are factors that can significantly increase it, as well as the risk of complications during the recovery period. To somehow compensate for this, it should be taken into account that the following are in danger:
- Elderly people. Worn-out vessels of the heart and brain may not withstand the load of general anesthesia, decreased vitality and metabolic rate can significantly affect the success of the recovery process, concomitant diseases (and in old age they develop even in the healthiest and most successful people) can affect the outcome of the operation.
- Children. The compensatory mechanisms of the child’s body are not yet sufficiently developed, as is his immunity, therefore any surgical intervention poses a significant risk for children. In addition, it is impossible to explain to a small child the need to adhere to the regime after craniotomy; he can harm himself.
- People who have already experienced skull surgery in their lives. Often, after the first operation, adhesions form between the membranes of the brain and its substance, pressing against the part of the bone that was once opened. With repeated intervention there is a high risk of damaging the entire structure.
- People suffering from blood diseases. Hemophilia, anemia - any diseases that affect the rate of blood clotting significantly increase the likelihood of bleeding during surgery and add problems in order to somehow compensate for it.
- People suffering from diabetes. Due to the specific features of this disease, all blood vessels are damaged to one degree or another, which significantly complicates the recovery period.
- People suffering from any immune deficiency syndromes. If they are present, the likelihood of developing an infectious inflammatory process as a result of surgery increases significantly. If possible, doctors avoid prescribing craniotomy to patients in this group - but if it is still necessary, great efforts are required to compensate for the disease.
However, even if a person is completely healthy, the recovery process will be long and there is no way to insure against the development of complications.
Features of the postoperative period
The prognosis after a ruptured aneurysm depends largely on the person's age, general health, other underlying neurological conditions, location of the aneurysm, the extent of bleeding (and rebleeding), and the time from the rupture to medical attention. The two most important factors are early diagnosis and treatment.
Patients treated for an unruptured aneurysm will require less rehabilitation therapy and recover faster than those with a ruptured aneurysm. Recovery from treatment or rupture can take several weeks to months.
Top
Top
If the procedure for clipping a cerebral aneurysm was successful, and during rehabilitation the patient followed the doctors’ recommendations, life expectancy is not reduced. If treatment is refused, the tumor enlarges, rupture and hemorrhage occur.
Additional factors also influence the consequences and life expectancy:
- single micro-formations are easier to treat and have minimal consequences;
- small aneurysms do not cause serious symptoms and occur without rupture;
- the location of the pathology affects the course of the disease and treatment;
- at a young age, surgery is easier to tolerate, and the prognosis for patients is more favorable;
- with connective tissue diseases, the consequences may be more serious;
- diseases of organs and systems can delay surgical treatment or worsen the prognosis.
It is very important to follow the doctor’s instructions, and then the risks will be minimal.
Lifestyle
Of course, an operation to eliminate an aneurysm in the vast majority of cases leads to its complete exclusion from the bloodstream, and there is no risk of its rupture with hemorrhage in the brain tissue. But this does not mean that after the operation the patient can immediately resume the usual lifestyle that he led before the intervention. Yes, life changes dramatically after surgery, and every patient should take this into account before surgical treatment. Often, after surgery, many people have to relearn how to walk, eat, talk, read and write. But this does not mean at all that you should refuse to clip the aneurysm, since its rupture without surgical treatment can cause death.
After discharge from the hospital where the operation was performed, the patient is sent for further treatment and rehabilitation to the clinic at the place of residence. At this stage, the patient is treated by a neurologist, a neurosurgeon (if there is a clinic on staff) and an epileptologist (if the patient has had or is experiencing symptomatic epilepsy). In addition, an important role in rehabilitation is played by a rehabilitation doctor, exercise therapy doctor, speech therapist, psychologist and other specialists.
Disability due to aneurysm
Assignment of disability after open surgery occurs after a socio-medical examination. Only in 7-10% of cases the patient is given one of the categories of disability.
The appointment is due to functional imbalance, partial incapacity. Temporary disability is also prescribed if the patient needs long-term rehabilitation.
The disability group is given depending on the symptoms and consequences:
- The first is prescribed if the patient needs outside care and supervision. At the same time, he cannot provide for himself, incapacity is given, and a guardian is assigned to the person.
- The second group is given for partial impairment of functionality. Sometimes they are given partial incapacity.
- The third group is established for moderate dysfunction. This may include partial hearing loss, paralysis or disorientation. At the same time, the possibility of self-service remains 100%.
The decision to undergo surgery is made by the patient, but it should be based only on the consultation and decision of the neurosurgeon. Ideally, you should obtain multiple opinions from leading physicians in the field. The consequences after surgery to remove an aneurysm are minor in 80% of cases and disappear within a year.
What is a cerebral artery aneurysm?
Some types of aneurysms—especially very small aneurysms—do not cause bleeding or other complications. A cerebral aneurysm can occur in any area of the brain, but is usually located where branches of an artery arise, between the undersurface of the brain and the base of the skull.
Top
Other causes of cerebral aneurysm include head trauma or injury, high blood pressure, infections, tumors, atherosclerosis (vascular disease accompanied by the deposition of cholesterol on the walls of blood vessels) and other diseases of the vascular system, as well as smoking and drug use. Some researchers believe that taking oral contraceptives may increase the risk of developing an aneurysm.
An aneurysm that occurs due to infection is called an infected (mycotic) aneurysm. Aneurysms associated with cancer are often associated with primary or metastatic tumors of the head and neck. Drug use, particularly frequent use of cocaine, can damage blood vessels and lead to the development of a brain aneurysm.
Top
Top
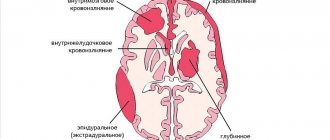
Most often, the rupture leads to a subarachnoid hemorrhage (bleeding into the cavity located between the cranial bone and the brain). A dangerous consequence of subarachnoid hemorrhage is hydrocephalus, which is characterized by excessive accumulation of cerebrospinal fluid (CSF) in the ventricles of the brain, which, under its influence, expand and put pressure on brain tissue.
Another complication can be vasospasm, in which blood vessels narrow, limiting blood flow to vital areas of the brain. A lack of blood supply can lead to stroke or tissue damage.
Top
Symptoms of a cerebral aneurysm include pain in the eye area, numbness, weakness or paralysis of one side of the face, dilated pupils and blurred vision.
When a cerebral aneurysm ruptures, a person may experience a sudden and very severe headache, double vision, nausea, vomiting, neck stiffness, and possible loss of consciousness. People commonly describe this condition as “the worst headache of their life,” which tends to be severe and intense.
Other symptoms of a ruptured brain aneurysm include: nausea and vomiting accompanied by severe headache, drooping eyelid, sensitivity to light, changes in mental status or anxiety level. Some patients experience seizures. Loss of consciousness and, in rare cases, coma are also possible.
If you are suffering from an acute headache, especially in combination with the other symptoms mentioned above, you should consult a doctor immediately.
Top
Through certain diagnostic methods, information about the aneurysm and the most appropriate treatment method can be obtained. These tests are usually performed after a subarachnoid hemorrhage has occurred to confirm the diagnosis of a cerebral aneurysm.
Angiography is an x-ray examination of blood vessels, which is performed using contrast agents. An intracerebral angiogram can reveal how narrowed or damaged arteries or blood vessels in the brain, head, or neck are, and can also identify changes in an artery or vein, including a weak point, such as an aneurysm.
This method is used to diagnose cerebrovascular accidents, and also allows you to accurately determine the location, size and shape of a brain tumor, aneurysm or burst vessel.
Angiography is performed in specially equipped X-ray rooms. After administering a local anesthetic, a flexible catheter is inserted into the artery and advanced to the affected vessel. A small amount of radiopaque contrast agent is released into the bloodstream and spreads through the vessels of the head and neck, after which several x-rays are taken, which can help diagnose an aneurysm or other circulatory problems.
A computed tomography (CT) scan of the head is a quick, painless, non-invasive diagnostic test that can detect the presence of a cerebral aneurysm and, for a ruptured aneurysm, determine whether there is bleeding in the brain as a result of the rupture. As a rule, this is the very first diagnostic procedure prescribed by a doctor if he suspects the possibility of rupture.
The X-rays are processed by computer as two-dimensional cross-sectional images of the brain and skull. Sometimes contrast agents are injected into the bloodstream before a CT scan is performed. This process, called computed tomographic angiography (CT angiography), provides clearer, more detailed images of the blood vessels in the brain. CT scans are usually performed on an outpatient basis in specialized laboratories or clinics.
Magnetic resonance imaging (MRI) uses computer radio waves and a powerful magnetic field to produce detailed images of the brain and other organs. Magnetic resonance angiography (MRA) provides even more detailed images of blood vessels. The images can be viewed as three-dimensional images or two-dimensional cross-sections of the brain and blood vessels. This painless, noninvasive procedure can show the size and shape of an unruptured aneurysm and determine if there is a brain bleed.
If a ruptured aneurysm is suspected, the doctor may refer the patient for a cerebrospinal fluid test. After applying a local anesthetic, a small amount of cerebrospinal fluid (which protects the brain and spinal cord) is removed from the subarachnoid space, which is between the spinal cord and the surrounding membranes, using a surgical needle.
Top
There are two types of surgical treatment for cerebral aneurysms: aneurysm clipping and occlusion. These operations are among the most complex and risky operations (other blood vessels may be damaged, a recurrent aneurysm may form, and there is also a risk of a postoperative attack).
Endovascular embolization is an alternative to surgery. This procedure is performed more than once during a person's lifetime.
Top
Top
Top
Top
Diagnostics
Diagnosis of aneurysms in 98% is based on instrumental studies. To determine pathology use:
- Ultrasound (ultrasound) with transcranial (transcranial) Dopplerography - allows you to visualize the pathologically altered area of the vessel, determine the size of the aneurysm, and the features of its walls. Small aneurysms are difficult to see;
- CT – computed tomography. Allows you to better visualize the vessels, the affected area, and more accurately determine the size of the aneurysm, its structure, and the features of the walls. You can also evaluate the severity of blood flow through the artery, its features, and create a 3-D model of the affected vessel. The study involves exposure to radioactive radiation;
- MRI – magnetic resonance imaging. In terms of diagnostic capabilities, it is not inferior to CT. The action is based not on the influence of radioactive radiation, but on the principles of magnetism;
- Cerebral (cerebral) angiography. The method is based on the passage of X-ray radiation, which visualizes a special contrast agent introduced into the vascular bed. Allows you to diagnose an aneurysm with a 98% guarantee. Recognized as the “gold standard” in the diagnosis of pathology. Allows a comprehensive assessment of the condition of the vessels of the head;
- EEG – electroencephalography. Allows you to evaluate the electrical potentials of the brain and determine the depth of the lesion, symptoms, and make a treatment prognosis.
Useful: Atmospheric pressure: normal for humans