Features of the disease
Hemorrhages into the subarachnoid space (the gap between the meninges) occur spontaneously in most cases. The person then feels a sudden headache and nausea. Some people start vomiting, others lose consciousness.
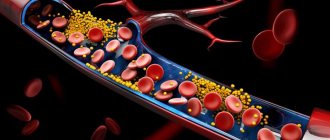
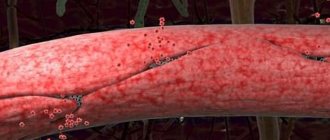
Subarachnoid hemorrhage occurs due to complete rupture of blood vessels or partial tear of a cerebral artery . The reason for this is various pathological processes, most often aneurysms (protrusions of the walls of blood vessels) and traumatic lesions.
Blood accumulates in the area of the basal cisterns, so the disease can be called basal subarachnoid hemorrhage. Aneurysm ruptures cause blood to leak into the cerebrospinal fluid . In this case, a pronounced spasm of the arteries of the brain is observed, its edema develops, and neurons begin to die.
How to diagnose
Subarachnoid bleeding can be diagnosed only with the help of a complex of neurological studies, which are carried out in paid clinics. First, the doctor interviews the patient: questions are asked about how long ago the symptoms appeared, whether there were injuries or pressure surges, and whether the patient has bad habits. Then the patient is examined in order to detect signs of neurological disorders, and also to assess the patient’s level of consciousness.
Next, a blood test is taken to determine blood clotting. A lumbar puncture is then performed. To do this, take a special needle and make a puncture of a few millimeters in the lumbar region, extracting a few milliliters of cerebrospinal fluid. If there is a small amount of blood (clots) in the cerebrospinal fluid, there is a hemorrhage in the subarachnoid space. To study the structure of the brain and locate the site of hemorrhage, computed tomography and magnetic resonance imaging are performed.
Echoencephalography can detect intracranial subarachnoid hemorrhage, which can displace the brain. Transcranial Doppler ultrasound can assess blood flow in the arteries of the brain. This will help determine where the vasoconstriction occurs. Using magnetic resonance angiography, you can evaluate the integrity of the cerebral arteries and their conductivity.
Prevalence of the disease and stages of its development
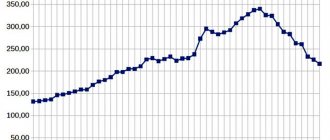
Among all forms of circulatory disorders in the brain, SAH occurs in 1-7% of cases . Spontaneous subarachnoid hemorrhage occurs in 8-12 people out of 100 thousand annually. Its traumatic form is more common. Depending on the situation, the frequency of subarachnoid hemorrhages in traumatic brain injuries varies from 8 to 59%.
Older patients are more likely to develop this condition. Alcohol intoxication is also a risk factor.
Almost 85% of cases occur due to rupture of the cerebral arteries, which are located in the circle of Willis. About half of subarachnoid hemorrhages are fatal. Of these, 15% of patients do not have time to get to the hospital .
There are 3 stages of development of traumatic subarachnoid hemorrhage.
- The blood that has entered the subarachnoid space begins to spread through the cerebrospinal fluid channels. In this case, the volume of cerebrospinal fluid increases and intracranial hypertension develops.
- In the cerebrospinal fluid, the blood begins to coagulate and clots form. They block the liquor pathways. As a result of this condition, liquor circulation is disrupted, and intracranial hypertension begins to increase.
- The dissolution of clotted blood is accompanied by the appearance of meningeal syndrome and signs of the onset of aseptic inflammation.
Subarachnoid hemorrhage
SAH is a subtype of hemorrhagic stroke, which is classified into a separate group based on the location of the hematoma. A brain hematoma in the subarachnoid space increases the volume of fluid in it, which increases intracranial pressure.
The presence of blood in the subarachnoid space leads to irritation of the pia mater and the development of aseptic meningitis. Reactive reflex spasm of cerebral vessels causes insufficient blood circulation and the development of ischemic stroke.
The frequency of subarachnoid hemorrhage among all acute cerebral hemorrhages is 10%. Up to 80% of subarachnoid bleeding occurs in people 40-65 years old.
Classification of severity of conditions
Doctors use three methods to assess the severity of the lesion. When classified according to Hess and Hunt, 5 levels are distinguished :
- Asymptomatic or minor symptoms such as mild headache and neck stiffness. The survival rate for this condition is 70%.
- Moderate or severe pain, severe stiffness of the neck muscles, paresis of the nerves of the skull. The chances of survival do not exceed 60%.
- Neurological deficit in minimal manifestations, stunning. Only 50% of patients survive.
- Stuporous state, manifestations of moderate or severe hemiparesis, autonomic disorders, signs of decerebrate rigidity. The probability of survival does not exceed 20%.
- Agony, deep coma, decerebrate rigidity. In this condition, 90% of patients die.
The Fisher scale , modified by Claassen et al, is based on computed tomography findings. It distinguishes 4 degrees of damage:
- The first level is assigned when the hemorrhage is not visualized.
- We are talking about the second level in cases where the thickness of the lesion is less than 1 mm.
- At the third level, the thickness exceeds 1 mm.
- The fourth level of SAH is diagnosed in cases where intraventricular hemorrhages or their extension to the brain parenchyma are visualized, regardless of thickness.
The World Federation of Neurological Surgeons uses the Glasgow Coma Scale to assess focal neurological deficits:
- At level 1 there is no neurological deficit, GCS score is 15 points.
- To assign level 2 according to the GCS, there must be from 13 to 14 points and the absence of neurological deficit.
- If there are signs of damage to the central or peripheral nervous system and 13-14 points on the GCS, level 3 is established.
- The GCS score is 7-12; the presence of focal neurological deficit is not important.
- According to the GCS, less than 7 points were assigned.
Classification of subarachnoid hemorrhage
SAH is classified according to three factors:
- by etiology;
- according to the severity of the patient’s condition (Hunt and Hess scale);
- by the volume and extent of the hematoma and the degree of visualization on CT (Fisher scale);
According to the etiological factor, hemorrhagic stroke with hemorrhage into the subarachnoid space is divided into 2 types:
- post-traumatic (due to mechanical damage to the vascular network due to trauma, a subdural hematoma of the brain appears);
- spontaneous (usually due to aneurysm rupture).
Based on location, isolated and combined hemorrhages are distinguished.
With combined SAH, after entering the subarachnoid space, blood spreads through the cerebrospinal fluid channels and enters other areas of the brain. Divided into 3 types:
- subarachnoid-ventricular;
- subarachnoid-parenchymal;
- subarachnoid-parenchymal-ventricular.
According to Hunt and Hessom:
- 1 point - asymptomatic, mild headache, slight stiffness of the neck muscles. Survival rate - 70%.
- 2 points - headache of moderate or high intensity, stiffness of the neck muscles. The only neurological symptoms are cranial nerve palsy. Survival rate - 60%.
- 3 points - change in consciousness, state of stupor, minor neurological manifestations. Survival rate - 50%
- 4 points - state of stupor, moderate or severe hemiparesis, decerebrate rigidity (increased tone of extensor muscles), autonomic disorders. Survival rate - 20%.
- 5 points - deep, agony. Survival rate - 10%.
According to Fisher's classification:
- 1 point - no blood.
- 2 points - the thickness of the hematoma is less than 1 mm, there are no blood clots.
- 3 points - the thickness of the SAH is more than 1 mm or there are clots in the blood.
- 4 points - hemorrhage into the parenchyma and ventricles.
The Generalized SAH severity classification scale for predicting stroke outcome, proposed by Ogilvy and Carter, takes into account the presence or absence of five factors:
- Age over 50 years.
- 4-5 points on the Hunt and Hess scale.
- 3-4 points on the Fisher scale.
- Presence of aneurysm >10 mm.
- The presence of an aneurysm in the posterior circulatory (vertebrobasilar) circulatory system of the brain measuring >25 mm.
Causes and risk factors
SAH occurs due to disruptions in the integrity of the walls of the arteries that run inside the skull. They are located on top of the hemispheres of the brain or at its base. The following are the causes of arterial damage:
- traumatic lesions: traumatic brain injuries, in which brain contusion and arterial damage are diagnosed;
- spontaneous violations of the integrity of the walls;
- aneurysm ruptures;
- ruptures of arteriovenous malformations.
In most cases, non-traumatic subarachnoid hemorrhage occurs due to the sudden rupture of an aneurysm in the arteries of the brain.
Experts include the following risk factors:
- use of alcohol and drugs;
- high blood pressure;
- vascular atherosclerosis;
- infections that damage the cerebral arteries (syphilis).
Treatment
Drug treatment
After a subarachnoid hemorrhage occurs, some of the blood vessels near the ruptured aneurysm may go into spasm. This condition is known as cerebral vasospasm, and it can lead to further bleeding, causing brain damage.
To prevent this, the patient may be prescribed a drug called nimodipine (Nimotop) , which must be taken for three weeks. Nimodipine was originally used to treat high blood pressure, but was found to be more useful in preventing cramps. Side effects of nimodipine include:
- increased sweating;
- nausea;
- swelling of the legs, ankles;
- stomach upset.
morphine , can be used to relieve symptoms of severe headaches . paracetamol can be used as an alternative .
Neurosurgical clipping
Neurosurgical clipping is a procedure performed under general anesthesia (when the patient is put to sleep). During the procedure, an incision is made in the scalp and a small piece of bone is then removed to expose the brain.
A neurosurgeon (a specialist in brain and nervous system surgery) will carefully look for the aneurysm and, once located, will close it with a tiny metal clamp. After replacing the “bone flap,” the neurosurgeon will sew the scalp back together.
Neurosurgery is an incredibly complex and difficult procedure, and success can never be guaranteed.
However, neurosurgical clipping has a relatively good success rate, with 70% of people achieving significant or even complete recovery after surgery.
Endovascular coil embolization
Endovascular coil embolization is a procedure in which a tiny plastic tube or catheter is inserted into an artery in the leg or groin. The tube is then guided through a network of blood vessels into the head and finally into the aneurysm.
Tiny platinum coils are then passed through the tube into the aneurysm. These coils block the flow of blood into the aneurysm and thus prevent further bleeding.
Endovascular coil embolization is becoming an increasingly preferred treatment option as it has a higher success rate, with 77% of people achieving significant improvement or complete recovery after surgery.
Additionally, due to the less invasive nature of endovascular coil embolization compared to neurosurgical clipping, recovery time is typically faster.
Clinic: symptoms and signs
It is necessary to call an ambulance for subarachnoid hemorrhage if, against the background of normal health, a person has:
- headache that gets worse with any activity;
- nausea and vomiting;
- the appearance of psycho-emotional disorders: fear, drowsiness, increased excitability;
- convulsions;
- disturbance of consciousness: stupor, fainting or coma appears;
- the temperature increased to febrile and subfebrile values;
- photophobia.
Symptoms persist for several days.
Separately, there are signs that arise when the functioning of the cortex and nerves of the brain is disrupted . This is evidenced by:
- loss of skin sensitivity;
- speech problems;
- the appearance of strabismus.
A few hours after the effusion of blood, symptoms of meningitis appear:
- Kernig's sign (a person is unable to straighten a leg that is bent at the same time at the knee and hip joints);
- stiffness of the neck muscles (the patient does not reach his chin to his neck).
Traumatic subarachnoid hemorrhage due to traumatic brain injury requires monitoring for signs of damage to different brain regions.
Problems with the frontal lobe will be indicated by:
- speech disorder;
- cramps in the fingers;
- unsteady gait;
- speech disorders;
- behavior changes.
When the temporal lobe , hearing is lost, memory impairment, auditory hallucinations and tinnitus appear.
Impaired reading ability, loss of tactile sensations, and ability to navigate indicate problems in the parietal lobe .
Damage to the occipital lobe results in visual impairment and visual hallucinations.
With a relapse, existing symptoms intensify and new ones appear. For some, blood pressure rises, arrhythmia begins, pulmonary edema occurs and the heart stops.
Symptoms
Signs of SAH occur suddenly. The clinical picture of the disease is characterized by a sharp and acute headache that cannot be tolerated. For a large number of people, headache is the only symptom of the disease. But pain can also appear with other brain diseases.
The remaining signs are divided as follows:
| Symptoms | Characteristic manifestations |
| Psychomotor |
|
| Neurological |
|
Most often, subarachnoid hemorrhage occurs against the background of physical or emotional outbursts.
Diagnostics and first aid
The doctor assesses the patient's condition and prescribes a computed tomography scan. Using CT:
- the area where the bleeding occurred is identified;
- data on the liquor system is obtained;
- it is checked whether there is cerebral edema.
High-precision CT angiography allows you to find out where the source of bleeding is . Negative CT results are associated with insignificant amounts of hemorrhage. They also occur when diagnostics are carried out at a later date.
If negative results are obtained, a lumbar puncture and cerebrospinal fluid examination are prescribed. SAH is indicated by an increasing concentration of red blood cells.
If the disease occurs due to an aneurysm, then vascular angiography . A radiopaque contrast agent is injected into them and X-rays are taken. Endovascular surgery is performed on damaged areas.
First aid is aimed at stabilizing the patient's condition. He needs to be taken to the hospital when the first symptoms appear .
Treatment is carried out to stop the bleeding and eliminate its source. It is important to prevent the development of complications and relapses.
Treatment methods
Subarachnoid hemorrhage in the brain is treated according to the following principles:
- stabilize the patient's condition;
- prevent relapses of SAH;
- normalize homeostasis;
- carry out preventive therapy for cerebral vascular spasms and the development of ischemia.
Drug treatment
Conservative treatment includes basic and specific therapy.
Basic therapy is aimed at normalizing cardiac and respiratory activity and relieving symptoms. When hydrocephalus increases, diuretics (Glycerol, Mannitol) are prescribed.
Symptomatic treatment includes:
- anticonvulsants (Lorazepam, Valproic acid) for seizures;
- sedatives (Diazepam, sodium thiopental) for psychomotor agitation;
- Metoclopramide and Domperidone are prescribed for frequent vomiting.
Specific therapy is aimed at minimizing the degree and consequences of vasospasm:
- use of nimodipine (calcium antagonist);
- ZH-therapy (hypertensive hypervolemic hemodilution) to maintain hypervolemia (excess blood volume), controlled hypertension and hemodilution (dilution of blood with plasma replacement fluid) - this helps improve blood flow and microcirculation.
Surgery
Unconscious patients are intubated and connected to a ventilator.
If conservative therapy does not produce results, cerebral edema progresses or CT scan reveals massive hemorrhage, decompression craniotomy is performed, hemorrhagic contents are removed, and external ventricular drains are installed.
If a rupture of a cerebral aneurysm is detected, specific surgical treatment is performed aimed at excluding it from the bloodstream.
The main methods are:
- clipping of the aneurysm neck;
- endovascular occlusion (introduction of a balloon catheter filling the aneurysm cavity).
For decompensated vasospasm, stenting or vascular angioplasty is indicated.
Treatment tactics
Patients with SAH are immediately prescribed medications that normalize intracranial and blood pressure . If the patient is unconscious, then the trachea is intubated and a ventilator is connected.
People with massive hemorrhages undergo emergency surgery to remove the hemorrhagic contents . The rest are receiving therapy that should reduce the risk of recurrent bleeding.
The doctor faces the following tasks:
- achieve stabilization of the condition;
- prevent relapses;
- normalize homeostasis;
- minimize the manifestations of the disease that led to the lesion;
- treat and prevent vascular spasms and cerebral ischemia.
Patients are given pain relief using means that provide minimal sedation.
This allows you to control their consciousness. Checking water balance and assessing kidney function is carried out using a urinary catheter. People with SAH are fed using a nasogastric tube or parenterally. Compression garments help prevent vein thrombosis.
If the cause of the disease is an aneurysm, then during angiography the problematic vessel may be clipped or clogged .
is also carried out :
- patients who experience seizures are prescribed anticonvulsants;
- people with cerebral edema are given diuretics;
- for repeated vomiting, give antiemetics.
How is the treatment carried out?
Emergency care for a person with such bleeding can only be provided by doctors using intravenous injections to reduce agitation and headaches. Self-administration of any medications can aggravate the situation (for example, aspirin is contraindicated in patients).
If bleeding is suspected, the patient must be taken to the hospital. Therapeutic actions should begin to be carried out by the ambulance team at the prehospital stage. Subarachnoid hemorrhage is fatal in 50% of cases, and a third of patients die in the ambulance.
The patient is taken to the neurological, neurosurgical department or intensive care unit.
After the diagnosis is established or confirmed, the patient is prescribed drugs that increase blood clotting and drugs that lower blood pressure.
Drug therapy
Drug treatment includes the primary stage (stopping bleeding) and eliminating headaches.
If the course of the disease is accompanied by convulsions or seizures, medications can be used to reduce these manifestations of the disease.
During drug treatment, the following drugs are prescribed:
- reducing arterial spasms;
- laxatives and diuretics (help reduce edema of the brain);
- painkillers;
- reducing cramps;
- antiemetics;
- tranquilizers.
Surgical intervention
Brain surgeries are performed in cases where intracerebral hemorrhage is caused by an aneurysm, as well as in case of massive hemorrhage in the brain, characterized by impaired consciousness, loss of speech and motor function (in this case, the hematoma is removed).
There are two types of surgery:
- Neurosurgical clipping. The operation involves placing a metal clip on the aneurysm, which will prevent growth and rupture. The operation is performed on the open brain under general anesthesia, in the case of an aneurysm of the middle cerebral artery (occlusion has great risks, since access to the artery is difficult).
- Endovascular occlusion. The operation involves inserting a coil into the aneurysm, which, like a staple, prevents growth and rupture. The operation is performed on a closed brain (a coil is inserted through a catheter, which is led from the femoral artery through the carotid and vertebral arteries to the aneurysm) and under general anesthesia. This type of surgery is performed more often, especially in cases where the patient's condition is unstable and open-brain surgery may worsen it. Also, preference is given to occlusion in case of aneurysm of the basilar artery and posterior cerebral artery, since clipping in this case is impossible.
In case of aneurysm of the anterior cerebral and anterior communicating artery, both operations can be performed.
Surgery can also be called removal of a hematoma through holes in the skull. The operation is performed only if the blood clot is on the surface.
Expected prognosis and possible complications
The consequences of subarachnoid hemorrhage in the brain depend on the reasons that caused it, how quickly the patient was hospitalized, and how adequate the treatment was. The prognosis is influenced by the age of the patient and the amount of bleeding.
The most serious complication of subarachnoid cerebral hemorrhage is vasospasm. This vasospasm leads to ischemic brain damage. In severe cases, death is possible. Delayed ischemia occurs in 1/3 of patients , half of whom experience irreversible neurological deficit.
The development of vasospasm can be prevented by the introduction of calcium channel blockers. But for traumatic lesions such drugs are not used.
There are other consequences:
- Relapse. It happens both in the early period and after a certain period of time.
- Hydrocephalus - cerebrospinal fluid accumulates in the ventricles of the brain. Occurs in early and late periods.
- Pulmonary edema, ulcerative bleeding, myocardial infarction. These complications occur rarely.
Among the long-term consequences are:
- attention disorder;
- memory problems;
- fatigue;
- psychoemotional disorders.
People after SAH often complain of headaches, and sometimes pituitary and hypothalamic hormonal regulation is disrupted.
Causes
- Blood circulation.
Like all organs in the body, the brain needs blood to provide it with oxygen and other essential nutrients.
Our circulatory system consists of arteries and veins. Blood is pumped from the heart through the aorta (the main artery leading away from the heart) before passing through all the medium and small arteries that branch off from each other. The blood then enters the tiniest vessels known as capillaries, from where the oxygen in the blood is transferred to the cells that make up the tissues and organs of our body.
Capillaries then move the blood into veins, which return it to the heart. Veins are weaker and smaller than arteries, so capillaries must also reduce blood speed and pressure.
Subarachnoid hemorrhages are mainly caused by aneurysms and arteriovenous malformations, which occur due to defects and weaknesses of the blood vessels.
Preventative measures to prevent relapses
To minimize negative consequences, it is necessary to remember how to prevent subarachnoid hemorrhages:
- A nutritious diet, in which the body receives large quantities of fruits and vegetables, reduces the amount of fatty and fried foods.
- Refusal of drugs, alcohol, cigarettes.
- Gradual introduction of moderate exercise (swimming, race walking, jogging).
- Regular walks.
- Monitoring blood pressure (find out how to choose a tonometer for home use) and blood glucose concentration.
These preventive measures reduce the risk of subarachnoid hemorrhage.
A timely diagnosis and treatment measures allow patients to recover . But negative consequences of subarachnoid hemorrhage, which are life-threatening, occur in 80% of patients. The use of preventative measures will help prevent this.
This video presents a lecture on the treatment of subarachnoid hemorrhage:
What can cause it?
Subarachnoid hemorrhage is a type of hemorrhagic stroke in which blood is released into the subarachnodal space of the brain (the area between its cavities that is filled with cerebrospinal fluid).
The release can occur as a result of the development of vascular pathologies, head injuries, and blood clotting disorders. In this case, the patient experiences a severe headache. The frequent absence of other symptoms can make diagnosis difficult.
This condition also occurs as a result of damage to the brain parenchyma. In this case, specific neurological signs will be observed: disruption of the facial muscles (hemiparesis).
A complete list of possible causes of subarachnoid hemorrhage (SAH) is given in the table below:
| Traumatic | Spontaneous (non-traumatic) |
| Severe injury (TBI)/closed injury (CTBI). Brain contusion. | The most common reasons:
More rare causes:
|
The pathogenesis of hemorrhage can be described as the collection of fluid in the subarachnoid cavity - the space between the pia mater and the arachnoid membrane. This cavity contains cerebrospinal fluid, which rises from the spinal cord, wraps around both hemispheres of the brain and descends back.
When bleeding begins, blood flows to the basal cisterns (located at the base of the brain). And it begins to enter the cerebrospinal fluid, which leads to spasms of the arteries, death of neurons and swelling of the brain. The amount of cerebrospinal fluid increases due to the blood, which leads to an increase in pressure in the brain cavity and can contribute to its displacement.
Classification
In order to assess the patient's condition and the severity of the disease, several assessment methods have been developed using a scale and scoring system.
- Severity scale , which consists of five levels: from mild or asymptomatic to agonal and coma.
- The Fisher scale analyzes data obtained from a CT scan. It takes into account the visualization and volume of hemorrhage, as well as its spread to other areas of the brain.
- A combination of the classic Glasgow Coma Scale (assessing speech, motor responses and degree of eye opening) and focal neurological deficits (neurological signs that appear when certain areas of the brain are affected).
To establish the severity, the totality of the assessment results on all scales, as well as the location and size of the aneurysm, are taken into account.
Dyscirculatory encephalopathy of the 3rd degree is a serious disease in an advanced stage that threatens with disability and a high probability of death. More details in the article. The severe disease hydrocephalus in newborns can have the most dire consequences. Why is it so important to detect the disease early?
Prognosis for the patient
The overall mortality rate for subarachnoid hemorrhage is about 50%.
The likelihood of death is associated with the manifestations of the disease. If there are no symptoms, there is no mortality. With the appearance of stiff neck and neck muscles, as well as damage to the cranial nerves, the risk of death increases to 11%. If after an attack the patient experiences drowsiness, the probability of death is already 37%, and with the addition of hemiplegia (paralysis of half the body) – 71%. Prolonged coma is accompanied by 100% death.
The leading cause of death is recurrent hemorrhage, and it occurs within the first month after the first episode. If the patient does not die at this time, his subsequent probability of survival for a year is 90% or more.
After discharge, 25% of patients have neurological disorders that limit normal life, for example, paralysis persists. Only 20% of patients who have suffered subarachnoid hemorrhage do not have any consequences of this disease.
Factors that worsen the prognosis:
- late seeking medical care;
- misdiagnosis, for example, migraine;
- the presence of severe neurological disorders;
- high systolic blood pressure;
- previous subarachnoid hemorrhage or myocardial infarction;
- chronic liver diseases;
- a large volume of shed blood detected during tomography;
- aneurysm in the posterior part of the brain (vertebrobasilar);
- elderly age;
- development of delayed ischemia, intracerebral hemorrhage or hemorrhage into the ventricles of the brain;
- development of fever a week after the onset of the disease.
If the aneurysm is not found during tomography, or it is located in the middle cerebral artery, the prognosis is much better.
If subarachnoid hemorrhage complicates a traumatic brain injury, it increases the likelihood of neurological disorders and death of the patient. However, with a preserved level of consciousness, almost all such patients subsequently recover.
Rehabilitation
If treatment is carried out on time and the bleeding is successfully stopped, then the patient’s condition can be normalized. The recovery period takes at least 6 months. During the rehabilitation period, the patient must:
- take the medications prescribed by your doctor every day, without changing the dosage or skipping a dose;
- control the dynamics of brain recovery;
- Visit a neurologist regularly for examination.
The patient is strictly contraindicated to drink alcohol, drugs, or smoke. It is necessary to avoid stress and physical activity, to lead a calm and measured life.
Diagnostics
The examination is carried out urgently within the neurological hospital. Transportation is immediate; the sooner therapy is started, the higher the chances of a successful outcome.
There is no time for long research. If the patient is conscious, he is questioned for complaints. In case of fainting or coma, talk to relatives. Assessment of basic reflexes is mandatory.
Immediately after admission, doctors are looking for the possibility of conducting MRI diagnostics. This is the basis that allows you to visualize tissue, detect the location of hemorrhage, assess the size of the hematoma, and also work out treatment tactics and surgical access if there are indications for surgical treatment.
Verification is carried out using tomography, this is a key activity. However, it is not always possible to establish a diagnosis even in such a sensitive and informative way.
Then they resort to a spinal puncture. A typical sign of an emergency is blood in the fluid. Then measures are taken to stabilize the patient's position.
Once finished, you can look into it in more detail.
The following methods are shown:
- Reflex examination (routine neurological). Provides information on the safety of higher nervous activity.
- Repeat MRI if indicated.
- Questioning the patient if he is conscious about his current state of health.
The examination is carried out urgently. The likely outcome depends on the speed of detection of the pathological process. Typically, the diagnosis of SAH is assumed after routine measures; MRI puts everything in its place. There are no difficulties in identifying except for rare clinical cases.
What is subarachnoid hemorrhage (SAH), its symptoms and diagnosis
SAH is a hemorrhage in the space between the arachnoid and pia mater. The most common causes are a ruptured aneurysm or injury. Symptoms of hemorrhage appear without any prerequisites : the head suddenly begins to hurt, as if from a blow with a blunt object, a feeling of nausea appears, and the person repeatedly loses consciousness. The disease is diagnosed using computed tomography, less commonly, lumbar puncture .
Diagnosis of pathology
Subarachnoid hemorrhage belongs to the category of the most complex and life-threatening cases. Its diagnosis involves conducting a complex of hardware examinations of the patient in order to confirm the diagnosis, as well as determine the stage of development, localization of hemorrhage, and the degree of disorders in the vascular system and hemispheres.
The main examination procedures include:
- Initial examination of the patient, analysis of his complaints.
- Visual assessment of a person’s condition, monitoring of his consciousness and the presence of neurological abnormalities.
- A laboratory blood test that can be used to determine the criteria for blood clotting.
- Cerebrospinal fluid puncture. If about twelve hours have passed since the onset of hemorrhage, its results, namely the presence of blood in the cerebrospinal fluid, can confirm the progression of SAH.
- Magnetic resonance imaging or computed tomography can identify the presence and location of the effusion, as well as assess the general condition of the brain. CT is more informative in the situation with SAH, which is why this type of examination is often prescribed to patients.
- If there is a suspicion of brain displacement as a result of injury, echoencephalography is prescribed to confirm or refute this fact.
- Transcranial Doppler ultrasound is performed to monitor the quality of blood flow in the cerebral arteries and its deterioration as a result of narrowing of the blood vessels.
- Magnetic resonance angiography of the arteries helps to assess their integrity and patency.
Angiography
Based on the results of the study, the patient will be diagnosed in accordance with the International Classification of Diseases, Tenth Revision. SAH is classified in the section “Diseases of the circulatory system,” a subgroup of cerebrovascular diseases, and may have an ICD-10 code from I160.0 to I160.9, depending on the location of the source of the effusion.
Symptoms of cerebral hemorrhage
A third of patients with subarachnoid hemorrhage complain only of headache. It has features:
- occurs suddenly or less often after precursors - an attack of dizziness or noise in the head, spots before the eyes;
- sharp, intense, reminiscent of a blow to the back of the head;
- accompanied by a feeling of pulsation in the occipital region;
- occurs in the back of the head or forehead, and then spreads throughout the head, as well as into the neck and between the shoulder blades;
- sometimes accompanied by the sensation of hot liquid spilling.
If a person experiences such signs, he should immediately contact a medical facility. The risk of developing subarachnoid hemorrhage when complaining of such a headache is 10%.
Other possible signs of subarachnoid hemorrhage:
- repeated vomiting that does not bring relief;
- convulsions;
- loss of consciousness in 45% of patients, stupor, lethargy, coma;
- stiff neck;
- dilation of the pupils and lack of their reaction to light (with cerebral edema);
- hemorrhage into the internal media of the eye;
- drooping eyelid, deviation of gaze down and to the side;
- photophobia;
- motor restlessness, agitation;
- increase in body temperature.
This serious condition is accompanied by a stress reaction of the body. Adrenaline is released from the adrenal glands, resulting in an increase in blood pressure. A complication of the pathology may be cardiac arrhythmia or pulmonary edema. In 3% of cases, subarachnoid hemorrhage leads to rapid cardiac arrest and death of the patient.
Causes of subarachnoid bleeding
In most cases, the cause of subarachnoid bleeding is a ruptured aneurysm. This is due to weakness in the walls of the blood vessels passing through the brain. Most often, their damage occurs at the point where small vessels depart from the main trunk.
Doctors cannot say for sure why a person develops an aneurysm.
However, there are certain risk factors that can cause such a pathology:
- Arterial hypertension.
- Hereditary predisposition.
- Rare diseases of the body.
- Bad habits (smoking, alcohol and drug addiction).
One of the causes of the disease is arterial hypertension.
In addition to rupture of aneurysms, other causes can lead to such a condition as SAH:
- Injuries that may result in hemorrhage with blood entering the subarachnoid space.
- The development of a tumor in the brain, which leads to damage to nearby vessels. In this case, the nature of the neoplasm can be both malignant and benign.
Learn more about the symptoms of a brain tumor.
- Arteriovenous malformations are a congenital pathology, as a result of which veins and arteries become intertwined.
- Vasculitis is an inflammatory lesion of blood vessels caused by an infectious or autoimmune process.
- Infectious lesion of the brain (complication of purulent meningitis, encephalitis, etc.).
- Fibromuscular dysplasia.
- Moyamoya disease.