I67.9 Cerebrovascular disease, unspecified
- First aid kit
- Online store
- About company
- Contacts
- Publisher contacts:
- +7
- Address: Russia, 123007, Moscow, st. 5th Magistralnaya, no. 12.
Official website of the RLS ® company.
Home Encyclopedia of medicines and pharmaceutical assortment of goods of the Russian Internet. The directory of medicines Rlsnet.ru provides users with access to instructions, prices and descriptions of medicines, dietary supplements, medical products, medical devices and other goods. The pharmacological reference book includes information on the composition and form of release, pharmacological action, indications for use, contraindications, side effects, drug interactions, method of use of drugs, pharmaceutical companies. The medicinal reference book contains prices for medicines and pharmaceutical market products in Moscow and other cities of Russia. Transfer, copying, distribution of information without the permission of RLS-Patent LLC is prohibited. When quoting information materials published on the pages of the website www.rlsnet.ru, a link to the source of information is required.
Lots more interesting things
© REGISTER OF MEDICINES OF RUSSIA ® RLS ®, 2000-2019.
All rights reserved.
Commercial use of materials is not permitted.
The information is intended for medical professionals.
general information
Short description
The concept of “chronic cerebral ischemia” includes: “discirculatory encephalopathy”, “chronic ischemic cerebral disease”, “vascular encephalopathy”, “cerebrovascular insufficiency”, “atherosclerotic encephalopathy”. Of the above names, the term “dyscirculatory encephalopathy” is most often used in modern medicine [1-5]
Patient category: adults.
Users of the protocol: neurologist, therapist, general practitioner (family doctor), ambulance and emergency medicine doctor, psychotherapist, speech therapist, physiotherapist, physical therapy and sports doctor, psychologist, social worker with higher education, social worker with secondary education, paramedic .
Diagnostics
II. METHODS, APPROACHES AND PROCEDURES FOR DIAGNOSIS AND TREATMENT
— determination of glycosylated glucose.
— Doppler ultrasound of the cerebral vessels and brachiocephalic trunk.
- sensory impairments (visual, auditory, etc.).
— paroxysmal conditions (with circulatory failure in the vertebrobasilar system).
- determination of urea, creatinine, electrolytes (sodium, potassium, calcium) - identification of electrolyte imbalances associated with the use of dehydration therapy.
— X-ray of the chest organs (2 projections): changes in the configuration of the heart with valvular defects, expansion of the boundaries of the heart in the presence of hypertrophic and dilated cardiomyopathy, the presence of pulmonary complications (congestive, aspiration pneumonia, thromboembolism, etc.).
All codes associated with “aneurysm ICD 10”
- Cerebral without rupture I67.0
- Carotid artery I72.0
- Vertebrate I72.6
- Other precerebral arteries I72.5
- With I60.7 gap
Symptoms of unexploded A.
depends on its location and size. Small sizes do not cause any symptoms and do not manifest themselves in any way until A. grows enough to compress adjacent structures.
When it begins to “press,” the symptoms depend on its location.
Aneurysms of the right ICA affecting the perichiasmal region are characterized by the presence of right-sided nasal hemianopsia (loss of the nasal half of the visual field). Left ICA - left-sided nasal hemianopsia. Compression of A. ICA on both outer parts of the chiasm leads to bilateral binasal hemianopia (loss of both nasal halves of the visual field).
When A.’s pressure on the “oculomotor” group of cranial nerves leads to deprivation of movements of the eyeball, dilation of its pupil (mydriasis), and lack of reaction to light - when three motor nerves (III, IV, VI pairs) are involved in the pathological process.
A is characterized by the presence of epileptiform seizures and cluster headaches. In the presence of giant A in the area of the cavernous sinus, pain develops in the supraorbital region, which gradually increases, sensitivity in the facial area decreases and the oculomotor nerves are affected.
Localization
It is most often localized in the cerebral part of the internal carotid artery (ICA), where the posterior communicating artery (PCA) or ophthalmic artery (OA) arises from it.
Less commonly, in the anterior cerebral arteries (ACA), where the anterior communicating artery (ACA) is located.
Sometimes at the point where the middle cerebral artery (MCA) divides or at the basilar artery (BA) where it divides into the posterior cerebral arteries (PCAs).
In 80% of cases A are single and only 20% are multiple.
Basically, size A is up to 1 cm, less often up to 2 cm. There are A with a diameter of more than 2.5 cm - giant aneurysms.
Causes
A. appear due to congenital inferiority of the arterial wall. This is a predisposition to stretch the vessel wall.
With age, degenerative processes develop in the aneurysm - the vascular wall becomes thinner and stretches more, increasing the protrusion, complicated by ruptures.
If there is a predisposition, A. can form when:
- uncontrolled and persistent increase in blood pressure,
- atherosclerosis of cerebral vessels,
- injuries of the vascular wall,
- inflammatory and autoimmune processes (arteritis) in blood vessels,
- when using drugs,
- radiation exposure,
- pressure on the vessel of a space-occupying tumor, for example
With a gap
It all starts with sharp headaches, vomiting, loss of consciousness (in 55%) up to a coma, photophobia, addition of meningeal (stiff neck muscles, Kernig, Brudzinsky symptoms) and focal symptoms depending on the affected area. If the aneurysm is located in the MCA, then impaired blood circulation in the pool leads to hemiparesis and speech disorders, especially in the dominant hemisphere.
If in the PSA, then a bifrontal hematoma is formed, causing lower paraparesis. If the vertebral artery (VA) is dissected, Wallenberg-Zakharchenko syndrome is possible. During the first days, in patients with developed subarachnoid hemorrhage, body temperature and blood pressure rise to 38°C.
Symptoms of aneurysms
Rupture of A. is manifested by the clinical picture of hemorrhagic stroke. Unexploded A. causes symptoms when surrounding brain structures are compressed.
Why is it dangerous?
Dangerous due to rupture and asymptomaticity. That is, aneurysms may not manifest themselves at all before rupture. There are no symptoms or they are of little specificity and insignificant.
And when it ruptures, it manifests itself as a hemorrhagic stroke, a life-threatening condition, often with severe neurological disorders that require long rehabilitation.
It’s worth thinking about this if anyone in your family has had episodes of intracerebral hemorrhage, especially someone under the age of 40-50.
It is possible that aneurysms were the cause. In such a situation, contact a neurologist about undergoing an examination and identifying cerebral vascular diseases.
Source: https://zdorovoe-serdce.net.ru/anevrizmaticheskaya-bolezn-golovnogo-mozga-mkb-10/
Differential diagnosis
Differential diagnosis:
Get treatment in Korea, Israel, Germany, USA
Get advice on medical tourism
2) Diet: table No. 10 (restriction of salt, liquid).
- glycine, 20 mg/kg body weight (on average 1-2 g/day) sublingually for 7-14 days
- tolperisone hydrochloride, 50-150 mg 2 times a day for a long time (under blood pressure control).
Relief of an epileptic seizure or status epilepticus is carried out according to the clinical protocol “Epilepsy. Status epilepticus."
— vinpocetine – 5-10 mg in tablets 3 times a day/day; Tablets 5.10 mg, ampoules 2 ml; — nicergoline – 10 mg tablets 3 times a day, tablets; ampoules 5 mg, tablets 5, 10 mg; - bencyclane fumarate - iv slowly 50-100 mg/day, ampoules; 100 mg 2 times/day for 2-3 months, tablets. Ampoules of 2 ml, tablets of 100 mg.
- tolperisone - 100 mg/day - ampoules, tablets 50 mg - 50-150 mg/day.
Relief of an epileptic seizure or status epilepticus is carried out according to the clinical protocol “Epilepsy. Status epilepticus."
- gabapentin - capsules of 100, 300, 400 mg.
— Tolperisone – 50 mg tablets.
Drug treatment provided at the emergency stage:
— Epileptic seizures (see clinical protocol “Epilepsy”, “Status Epilepticus”).
The use of a special system of exercises to restore impaired motor functions and the formation of a compensatory stereotype.
Constant stimulation of motor and mental activity.
— Sanitary educational work aimed at educational, propaganda and propaganda activities that promote a healthy lifestyle.
Other cerebrovascular diseases (I67)
Excluded: consequences of listed conditions (I69.8)
Excludes: rupture of cerebral arteries (I60.7)
Brain:
- aneurysm NOS
- acquired arteriovenous fistula
Excluded:
- congenital cerebral aneurysm without rupture (Q28.-)
- ruptured brain aneurysm (I60.-)
Atheroma of the cerebral arteries
Excludes: subcortical vascular dementia (F01.2)
Non-purulent thrombosis:
- brain veins
- intracranial venous sinus
Excludes: conditions causing cerebral infarction (I63.6)
Acute cerebrovascular insufficiency NOS
Cerebral ischemia (chronic)
ICD-10 alphabetical indexes
External Causes of Injury - The terms in this section are not medical diagnoses, but rather a description of the circumstances under which the event occurred (Class XX. External Causes of Morbidity and Mortality. Heading Codes V01-Y98).
Medicines and chemicals - table of medicines and chemicals that have caused poisoning or other adverse reactions.
In Russia, the International Classification of Diseases
10th revision (
ICD-10
) was adopted as a single normative document for recording morbidity, reasons for the population’s visits to medical institutions of all departments, and causes of death.
ICD-10
introduced into healthcare practice throughout the Russian Federation in 1999 by order of the Russian Ministry of Health dated May 27, 1997 No. 170
The release of the new revision (ICD-11) is planned by WHO in 2022.
Abbreviations and symbols in the International Classification of Diseases, 10th Revision
NOS
- without other instructions.
NEC
— not classified in other categories.
ICD-10 code for cerebral ischemia
The use of the International Classification of Diseases (ICD-10) helps doctors more easily navigate the wide variety of pathologies of the human body. Modern medicine is able to determine a lot of diagnoses that are impossible to remember or learn. This is especially true for vascular pathology: there are quite a lot of different variants of serious diseases associated with acute or chronic circulatory disorders of organs and systems. In particular, cerebral ischemia belongs to the “Diseases of the circulatory system” (class IX) and is located in the section “Cerebrovascular diseases”. Each condition has a code that the doctor will use to diagnose and treat it.
ICD code cerebral ischemia
Cerebral ischemia is a disease that develops in newborns as a result of circulatory disorders and is characterized by insufficient (hypoxia) or completely stopped (anoxia) oxygen supply to the brain tissue.
Late diagnosis and late treatment of the disease lead to the development of metabolic disorders and the formation of various functional disorders, which in turn can cause bleeding, the appearance of foci of necrosis and other severe complications, including death.
In modern medicine, ischemia in a newborn is one of the most serious problems of perinatal neurology. This is due to the lack of sufficiently effective methods of treating the disease.
Therefore, pathology is one of the main causes of mortality and disability in children under one year of age. According to ICD 10, ischemia is coded P 91.0 – P 91.
9 depending on the degree of course, causes of development and clinical manifestations.
Classification of pathology
Experts distinguish two forms of the disease:
- Cerebral ischemia in newborns is a congenital pathology; its signs appear in the first days of a child’s life. And in 70 out of 100 infants it starts at the time of birth or in the later stages of gestation.
- The chronic form of coronary artery disease is diagnosed in patients of older, often retirement age.
Reasons for the development of the disease
In the vast majority of cases, the causes of ischemia in an infant are the formation of blood supply disturbances in the third trimester of pregnancy or directly during childbirth.
Causes of development of ischemia in the prenatal period
Fetal hypoxia in the last stages of gestation can develop for the following reasons:
- Violation of uteroplacental blood flow, which is most often provoked by the following factors:
- the age of the expectant mother is more than 35 years - in order to give birth to a healthy child at this age, you must follow all the doctor’s recommendations;
- the presence of endocrine diseases in a pregnant woman;
- development of toxicosis in the third trimester;
- maternal history of epilepsy or the presence of neurological disorders in close relatives;
- long-term treatment for infertility;
- bad habits (smoking, alcohol abuse, taking drugs, uncontrolled use of various medications);
- bearing several fruits at the same time.
- Impaired blood flow from the placenta to the fetus (fetoplacental). This may happen for the following reasons:
- placental abruption or disruption of its blood supply, which leads to vascular pathologies;
- entanglement of the umbilical cord around the fetal neck;
- intrauterine malformations and formation of the organs of the cardiovascular system of the unborn child;
- development of acute placental insufficiency.
Many disorders of the intrauterine development of a child, including changes in blood supply, can be determined using a timely ultrasound.
Factors provoking the development of brain hypoxia during childbirth
The main causative factors for the development of ischemia in a newborn are:
- Asphyxia during childbirth - it can be provoked by:
- long or too fast labor;
- clamping of the umbilical cord during contractions or pushing;
- an increase in body temperature above 38 degrees during childbirth due to an acute illness or exacerbation of a chronic one;
- childbirth at home without qualified medical care;
- heavy bleeding;
- emergency caesarean section;
- childbirth at less than 36 weeks and more than 42.
- The development of respiratory failure in the first days after birth occurs for the following reasons:
- the presence of congenital malformations of the cardiovascular system;
- disruption of the blood supply to the heart;
- severe birth injuries;
- RDS – fetal respiratory distress;
- depression of respiratory function for various reasons;
- periodically duplicating attacks of lack of breathing (apnea);
- the presence of congenital pneumonia or aspiration syndrome;
- development of respiratory failure in premature babies.
- A sharp decrease in blood pressure shortly after birth, which can be caused by:
- sepsis;
- development of heavy bleeding.
Clinical manifestations and diagnostic principles
Experts distinguish three stages of the disease in children: mild, moderate and severe. Each of them has its own symptoms.
Mild or first degree ischemia
The disease is characterized by mild damage to brain tissue and develops as a result of mild hypoxia or asphyxia experienced during childbirth.
The main symptoms of grade 1 cerebral ischemia in newborns are as follows:
- the presence of disturbances in the tone of the muscular system;
- increased motor activity, appearing with trembling of the chin and limbs;
- enhanced reflexes;
- restlessness - shallow sleep, unreasonable crying, sudden movements.
In prematurely born children, grade 1 ischemia is manifested by a syndrome of depression of the central nervous system, the signs of which are lethargy, low muscle tone, weakening of unconditioned reflexes (grasping, swallowing and sucking).
With a mild degree of pathology, clinical manifestations disappear within 5-7 days. In the vast majority of cases, they do not need to be treated.
Changes in laboratory and clinical research
A blood test can detect a decrease in oxygen levels (hypoxemia) and an increase in carbon dioxide (hypercarbia), and acidosis is also observed - a shift in the reaction to the acidic side. All instrumental studies were without pathological abnormalities.
Second degree of ischemia
The main causative factors are fetal hypoxia in the prenatal period, moderate asphyxia during childbirth, the presence of RDS or congenital pathologies such as heart disease, pneumonia.
Ischemia of the 2nd degree is manifested by the following symptoms:
- Syndrome of depression or excitation of the central nervous system - in some cases, their alternation is observed.
- Convulsions are single, short-term clonic in full-term infants, and frequent tonic or atypical in premature infants. Such convulsive manifestations include apnea, rowing movements with the arms and pedaling with the legs, and causeless shuddering.
- Increased intracranial pressure - it can lead to the development of hydrocephalus, characterized by an increase in the size of the head and opening of the sutures of the skull.
- The presence of vegetative-visceral disorders - marbled skin, dermographism, gastrointestinal dysfunction, consisting of frequent constipation, diarrhea, flatulence, increased regurgitation.
- Loss of consciousness or lightheadedness caused by changes in blood pressure.
Third degree of cerebral ischemia
The reasons for the development of the third and most severe stage of the disease are long-term intrauterine hypoxia or perinatal asphyxia of a high degree of complexity. A combination of these two reasons is also possible.
In addition, the development of grade 3 ischemia can also be caused by extracerebral diseases of the child, these include severe congenital pneumonia, malformations of the cardiovascular system, respiratory disorders, lack of water in the body, leading to hypovolemic shock.
The clinical manifestations of this stage are more difficult to treat than many diseases. The third degree of development of ischemia is manifested by the following signs:
- Profound depression of the central nervous system, which can develop in the first twelve hours of a baby’s life (often during this period the child is in a coma). Over the next 12 hours, there is a slight increase in the level of activity, and then, on the second - third days, again depression of the central nervous system up to coma.
- Frequently recurring seizures.
- Dysfunction of the brain stem, manifested by a violation of the rhythm of the respiratory and oculomotor functions, a disorder of the normal reaction of the pupil to light.
- The presence of vegetative and visceral disorders - bluish or marbled skin, pronounced dermographism.
- Increased intracranial pressure.
- In some cases, the severe stage of the disease is characterized by a complete absence of unconditioned reflexes and reactions to various stimuli.
- With large areas of damage, the newborn takes a forced posture of decerebration and decortication, in which the limbs and body are extended, the arms are turned inward, the pupils are dilated, and the eyes roll down.
- The extreme degree of manifestation of central nervous system depression is a comatose syndrome, characterized by a sharp decrease in the tone of all muscle fibers and blood pressure, disturbances in the rhythm of breathing and heartbeat, and the presence of functional disorders of the gastrointestinal tract and urinary system. In this case, the eyes and mouth are open, and the eyeballs are not fixed (float).
Source: https://eltransteh.ru/kod-mkb-cerebralnaja-ishemija/
Classification of acute cerebral ischemia
Vascular pathology of the brain, caused by a sudden and severe disruption of arterial blood flow, is allocated to a separate group of ICD-10. All variants of cerebral infarction are divided into parts, each of which indicates the level of vascular pathology:
- difficulty in blood circulation occurred at the level of vessels located outside the brain (precerebral arteries);
- cerebral blood flow is impaired;
- a blood clot formed in the cerebral veins.
ICD-10 codes I63.0 to I63.2 indicate cerebral infarction caused by thrombosis of the precerebral arteries, I63.3 to I63.6 - occlusion of the cerebral arteries and veins. The I64.0 code encrypts a stroke in which there is no bleeding into the brain structures.
This group of ICD-10 codes does not include complications and consequences arising from acute ischemic attack.
Symptoms
In most cases, a slight expansion of the artery section does not manifest itself in any way. Such an aneurysm is most often discovered by chance or during a routine examination. When clinical signs appear, they are divided into tumor-like or apoplectic. In the first case, the formation quickly increases in size, compressing nearby brain structures as it grows.
All symptoms add up to the standard clinical picture of the tumor and directly depend on the location of the protrusion. Typically, a tumor-like aneurysm is localized in the cavernous sinus or in the area of the chiasm, the intersection of the optic nerves.
A defect in the arterial wall located in the chiasmal region negatively affects visual function: visual acuity decreases and its fields are disrupted. A long-term and fairly large cerebral aneurysm often leads to nerve atrophy followed by complete blindness. If it is located in the cavernous sinus, which is located at the base of the skull and regulates venous outflow from the eye sockets and brain, cranial nerve palsy occurs. When the 3rd, 4th and 6th pairs are affected, oculomotor disorders such as strabismus and inability to focus on an object occur.
Damage to the branches of the trigeminal nerve is manifested by the characteristic symptoms of its neuralgia. In advanced cases, even the bone tissue of the skull is deformed, which is revealed during an X-ray examination.
When the disease proceeds according to the apoplexy type, any clinical signs are most often absent. An apoplectic aneurysm is discovered only after it has ruptured and hemorrhaged into the brain. Among the symptoms that may precede this, painful sensations in the area of the eye sockets and forehead are occasionally mentioned.
Coding options for chronic cerebral ischemia
All chronic conditions leading to ischemic changes in brain structures are encrypted in subsection I67. Frequent causes of long-term cerebral circulatory insufficiency are the following conditions:
- dissecting aneurysm of the cerebral arteries (I67.0);
- cerebral aneurysm without signs of rupture (I67.1);
- atherosclerotic lesions of cerebral vessels (I67.2);
- encephalopathy due to vascular causes (I67.3);
- encephalopathy due to arterial hypertension (I67.4);
- a rare vascular pathology of the carotid and cerebral arteries described as Moyamoya disease (I67.5);
- inflammatory damage to the veins and arteries of the brain, leading to impaired blood flow (I67.6 - I67.7);
- when it is difficult to identify the main causative factor, codes I67.8 - I67.9 are used, which indicate all unspecified variants of diseases.
All types of consequences of acute or chronic cerebral ischemia are encrypted in subsection I69.
Additional codes to indicate the reason
Often, the doctor needs to not only identify the underlying disease with a code, but also identify additional causative factors that led to ischemic conditions in the head. For this, ciphers from other subsections are used:
- arterial hypotension (I95);
- serious heart disease (I21, I47);
- blockage of individual non-cerebral arteries (I65);
- various types of cerebral hemorrhages (I60 - I62).
If it is necessary to indicate complications, the doctor can use the coding of other sections. In particular, if severe brain disorders such as dementia occur due to vascular causes, the code F01 can be used.
Treatment
An aneurysm is treated primarily surgically, since such a formation requires removal. However, if the protrusion is small in size and does not manifest itself clinically, then the neurologist is limited to systematic observation. A patient with this diagnosis is registered and examined regularly. Additionally, measures are being taken to eliminate the causes that provoked the pathology. If there is an increase in the brain aneurysm with a simultaneously increasing risk of its rupture, surgery is performed using one of the modern techniques.
General recommendations
The leading causes of this disease are atherosclerosis, hypertension, and diabetes. If there are chronic pathologies, it is necessary to treat them, as well as adjust your lifestyle. First of all, you should stop smoking and reduce your alcohol consumption. These bad habits have an extremely negative impact on the condition of blood vessels for all of the listed diagnoses.
The transition to a healthy diet is one of the most important conditions for stabilizing the condition and the effectiveness of drug therapy for major diseases. It is necessary to exclude unhealthy fatty foods from the diet, minimize sugar consumption, eat more fresh vegetables and fruits, lean meat, and dairy products. Heat treatment is also important: it is advisable to boil, stew or bake dishes, and avoid fried foods.
Use cases for ICD-10
The main purpose of using ICD-10 in the practice of any doctor is the ability to perform statistical analysis, both within one medical institution, and across the country and the world. In addition, the international classification allows all doctors in the world to use the same diagnoses, which helps to carry out treatment effectively and correctly.
If acute thrombosis or chronic ischemia of cerebral vessels is detected, the doctor conducts a course of therapy aimed at completely curing the patient from the pathology of the precerebral or cerebral arteries. If necessary, surgery may be performed. If the treatment was successful, then upon discharge the doctor will indicate the diagnosis in the form of an ICD-10 code. The disease code will be processed by the hospital's statistical service, sending the information to the region's medical information center. If, in addition to the main diagnosis, there are complications and consequences that require additional examination and treatment, the doctor will indicate the coding of these conditions using international classification codes.
All ischemic conditions of the brain can be encrypted using ICD-10. By using the International Classification of Diseases, 10th Revision, the physician will always use diagnoses that are used throughout the world. This will make it possible to correctly assess not only a person’s disease, but also to carry out effective treatment using modern and high-tech methods of global therapy.
Symptoms of an aneurysm
A ruptured cerebral aneurysm is diagnosed by symptoms similar to those of a stroke:
- Attacks of severe headache.
- Dizziness.
- Feelings of heat.
- Various cognitive disorders: memory loss, inability to perceive information, impaired logical thinking.
- The development of all kinds of psychological disorders, including constant mood swings, insomnia, increased anxiety, irritability.
- Behavioral disorders: excessive fearfulness, aggression, slow reaction.
- Reduced blood pressure.
- Photophobia and other visual impairments.
- Problems with urination or bowel movements (usually spontaneous).
- Sensitivity to loud and harsh sounds.
- Noise and ringing in the ears.
- Hearing loss in one ear.
- The occurrence of general weakness of the body.
- Nausea and vomiting.
- Due to the resulting muscle tone, it is difficult to turn your head or lower it down.
- Dehydration of the body.
The human body is 75% water. To replenish your body's water supply, consume foods high in water more often.
- Difficulty swallowing.
- Impaired perception of the surrounding world.
- Speech disorders.
- Impaired coordination of movements.
- Convulsions and paralysis.
- Loss of consciousness or falling into a coma.
How to provide first aid to a person in case of loss of consciousness before doctors arrive.
A symptom such as a headache can occur 1-2 days before the aneurysm ruptures.
Although there have been cases where the patient complained about them for several weeks before the hemorrhage.
Symptoms accompanying hemorrhage in most cases depend on the size of the formation and the location of the aneurysm, as well as the presence of associated complications.
When pathology occurs on the carotid artery, the patient experiences various visual impairments.
When it is located in the area of the anterior cerebral artery, the patient experiences mental disturbances and possible paralysis of the limbs. Aneurysm of the middle cerebral artery leads to hemiaparesis and speech impairment.
If it occurs in the vertebrobasilar system, it may develop trigeminal or facial nerve damage and other disorders such as dysarthria.
Localization in the cavernous sinus often leads to hemorrhage into the cavity of the cranium, because it is located behind the meninges.
If a person finds any of these signs in combination with a headache, then it is necessary to consult a doctor for a timely diagnosis and initiation of treatment, which will help prevent the negative consequences of aneurysm rupture with subsequent hemorrhage.
Hemorrhagic vasculitis
Hemorrhagic vasculitis is considered a disease that is a type of immune vasculitis of small vessels and is characterized by increased formation of immune complexes and increased permeability of vascular walls. This pathology can develop 2-3 weeks after acute tonsillitis, influenza or scarlet fever. Hemorrhagic vasculitis is more common in children than in adults. Children aged 4 to 12 years are especially susceptible to the disease. Boys get sick 2 times more often than girls.
Hemorrhagic vasculitis ICD 10 (according to the international classification of diseases, tenth revision) is included in the group of diseases under the code D69.0 Allergic purpura. Most photos of hemorrhagic vasculitis show that the main symptom of the disease is an allergic rash.
Etiology of the disease
The causes of hemorrhagic vasculitis in adults and children are divided into several types:
- complications after an infectious disease caused by viruses, bacteria or parasites;
- food or drug allergies;
- hypothermia or individual intolerance to the vaccine;
- genetic predisposition.
The most common causes of hemorrhagic vasculitis are associated with the influence of infectious agents.
Our readers successfully use Normaten to treat HYPERTENSION. Seeing how popular this product is, we decided to bring it to your attention. Read more here...
Operation clipping
Neurosurgical treatment is carried out in the first three days after the rupture of the aneurysmal sac, depending on the patient’s condition. An intracranial intervention is performed, exposing the blood vessel and “switching off” A from the circulation.
Some of them can be “turned off” using the endovasal method (filling the lumen of the aneurysm with balloon catheters inserted through a guide through the blood vessels under periodic X-ray control).
Early operations are aimed at preventing recurrent bleeding and removing blood from the subarachnoid space, which reduces the risk of arterial spasm in the future.
A week or two after the rupture, a late period begins when there is an increase in intracranial pressure (ICP), swelling of the brain, and increased vulnerability, which complicates the approach to A.
The choice of anesthesia method and surgical support plays an important role. They use lumbar puncture (reducing the volume of the brain), hyperventilation, protection against oxygen deficiency using barbiturates, lowering blood pressure down to 50 mmHg.
Clip on the aneurysm sac
In open surgery, careful access is provided in the form of frontotemporal (the scales and ridge of the wings of the main bone are resected) or basal (if A is located in the vertebrobasilar region).
To “neutralize” an aneurysm, the neurosurgeon has in his arsenal miniature clips that are applied to its base - the neck; they have a spring mechanism, which allows you to change their position.
Often, before applying clips, the aneurysm is opened and freed from thrombotic masses.
Clipping can be supplemented by applying special quickly hardening plastic substances to surface A.
Surgical treatment is necessarily complemented by conservative treatment. Bed rest, painkillers and sedatives, beta-blockers, calcium channel antagonists, drugs that improve blood clotting, cerebral circulation and vasodilators are provided.
In some cases, antitussive drugs are added to therapy to prevent cough shocks, which are accompanied by an increase in pressure in the blood vessels and the risk of repeated hemorrhages.
Hypertension code according to ICD 10
CARDIOLOGIST LEO BOCERIA ABOUT HYPERTENSION
The chief cardiac surgeon of the Ministry of Health of the Russian Federation states: “Hypertension is not a death sentence. The disease is truly dangerous, but it is possible and necessary to fight it. Science has stepped forward and medications have appeared that eliminate the causes of hypertension, and not just its consequences. Just enough... Read the article >>
People suffered from hypertension long before the invention of the first tonometer, but even then people knew how the disease manifested itself and could recognize it by its characteristic symptoms. The first thing we paid attention to was:
Since then, the symptoms have not changed, but the name has changed a little. It acquired an incomprehensible prefix of three letters and one number.
International Classification of Diseases
Hypertension code ICD 10 for an ordinary person sounds like something unusual and incomprehensible, because everyone is simply accustomed to hypertension. What does this code mean?
In modern realities, to ensure the development of medical science and the ability to manage healthcare throughout the world, it is necessary to constantly obtain, collect and store information about the health status of the population. For this purpose, back in 1989, the International Classification of Diseases was created. At the moment, the ICD 10th revision is in force.
Also, one of the goals of the ICD is to translate diagnoses (which sound differently in different languages) into a universal, international ICD code. This approach simplifies the process of classifying, storing and transmitting important medical information.
The diagnosis of hypertension is made when there is a persistent increase in blood pressure above normal levels (according to the WHO - 140/90) recorded during two medical appointments in a state of complete physical calm. This is important because blood pressure increases not only in pathology, but also normally during physical activity as an adaptive reaction of the body.
If the doctor’s office is not located on the first floor and there is no elevator to it, and in our country this is not uncommon, then after the patient has conquered all the steps, he and his cardiovascular system need time to return to normal. But if a person suffers from hypertension, then only antihypertensive drugs will help return to normal.
Hypertension code according to ICD 10 in the international classification occupies several positions at once, namely, it has codes starting from I10 to I15, although bypassing I14. Each code also has a third digit (except I10), which indicates a specific feature of the diagnosis.
Target organs
Like any other disease, hypertension has its own target organs - these are the organs that suffer first and foremost and more than others. In this case it is:
The heart muscle suffers as a result of impaired regulation of vascular tone by higher centers, which are located in the medulla oblongata and the hypothalamus. As a result, a huge cascade of complex reactions is launched, the result of which is stenosis of blood vessels, including arteries, which leads to complications of normal blood circulation along the riverbed.
The heart tries to adapt to new conditions, hypertrophy (increase in volume) of the left ventricle develops, which allows the force of cardiac contraction to increase, but not everything is so smooth, you have to pay for everything.
Hypertrophied muscle tissue requires more oxygen than normal and over time ceases to be fully supplied with O2, which, in combination with nutrient deficiency, leads to heart failure.
The renal arterioles are affected in the same way as other vessels; their lumen narrows in the same way. In this case, the blood supply to the kidney is disrupted, which can lead to complications in filtration in the parenchyma. To avoid this, specific hormones such as renin begin to be released into the blood, which triggers the renin-angeotensin system, the main task of which is to increase blood pressure levels.
The brain can be affected as a result of a persistent increase in pressure and, as a result, rupture of one of the brain vessels. Hemorrhagic stroke is one of the most serious complications of hypertension.
Causes
- Burdened heredity.
- Gender (men are more likely)
- Age>50-55 years
- Frequent stress
- Obesity
- Physical inactivity
- Bad habits
Forms, stages of development
Hypertension has two forms:
There is stage III arterial hypertension.
Cerebral aneurysm: causes, symptoms, diagnosis
Most of the blood flows into the brain through the unpaired basilar and internal carotid arteries. Inside the parenchyma, vessels form branches due to the microcirculation of many anatomical structures (cerebellum, medulla oblongata, ventricles).
At the level of the trunk, these arteries form a plexus (Circle of Willis). The cerebral arteries (anterior, middle, posterior) depart from the area. A large number of anastomoses ensure the preservation of circulation when a blood clot clogs one of the vessels - the carotid or basilar artery.
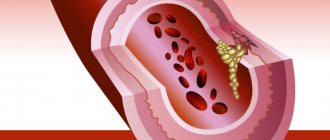
A cerebral aneurysm is a dissection of the arterial wall with a high risk of intravascular hemorrhage. The formation is not accompanied by clinical symptoms, and therefore creates difficulties in detection. Neuroimaging using radiation methods (CT and MRI) for other diseases detects pathology by chance.
CT scan of an internal carotid and anterior cerebral artery aneurysm
Large protrusions compress surrounding structures. Symptoms are due to the localization of aneurysmal expansion. In most cases, periodic headache and dizziness are observed.
Cerebral aneurysm
Due to the difficulties of detecting early development and the lack of clinical symptoms, it is difficult to reliably establish the frequency of the disease. About 50% of cerebral aneurysms are discovered by chance during postmortem examinations of people who died from intracerebral hemorrhage (hemorrhagic stroke).
Death occurs from aneurysm rupture with a frequency of 65% within three months after the onset of pathology. The probability of death immediately after a rupture is about 10%.
Arterial aneurysmal dilatations of the vessel wall are formed gradually. The decrease in microcirculation intensity develops consistently. The formation of vascular anastomoses and collaterals compensates for the lack of microcirculation. The absence of external manifestations of pathology at the beginning of development does not allow timely diagnosis.
Classification of cerebral aneurysms according to the ICD
The international classification has identified several types of aneurysmal protrusions of the arterial wall:
- Dissection of any part of the aortic wall - code “I71”;
- Ruptured thoracic aortic aneurysm – “I71.1”;
- Thoracic aortic aneurysm without precise localization of expansion – “I71.2”;
- Ruptured abdominal aortic aneurysm – “I71.3”;
- Aneurysm of cerebral vessels (cerebral) – “I67.1”.
The list of cerebrovascular diseases has an ICD code – “I60-69”. The section includes subarachnoid, intracerebral hemorrhages, cerebral infarctions, strokes, stenoses and blockages of cerebral arteries.
Anatomically, types of cerebral aneurysms:
- Lateral (tumor-like);
- Saccular;
- Fusiform.
The lateral variant has a tumor-like shape. The saccular appearance is rounded, which provides a connection between the neck and the trunk of the artery. The spindle-shaped variety occurs due to the expansion of the vessel in part of the trunk.
Size classification:
- Small – up to 11 mm in diameter;
- Medium – 11-25 mm in diameter;
- Giant - over 25 mm.
It is impossible to determine the relationship between etiology and form of pathology. The structure of the arterial bulge depends on the location of the injury.
Causes of cerebral aneurysm
To restore impaired blood circulation, intervascular anastomoses are formed inside the brain:
- Arteriolovenular - formed between arterioles and veins of different diameters. Collaterals provide direct drainage of blood from the site of arterial stagnation directly into the veins. The formation of anastomosis increases the likelihood of aneurysm formation by increasing pressure in the artery;
- Arterioarterial shunts create bypass pathways for blood outflow. The anastomosis does not always provide optimal blood flow due to blockage of the arteries by an embolus or thrombus;
- Venovenous anastomoses are formed through additional connections between different veins. Collaterals provide improved outflow to eliminate tissue hypoxia.
Anastomoses can be precursors to the formation of aneurysmal expansion or appear against the background of primary arterial protrusion.
Morphological basis of aneurysm formation
The wall of the vessel consists of three shells - inner, middle, outer. Blood comes into contact with the intima. When the inner wall is damaged, conditions are created for the formation of blood clots, atherosclerotic plaques, and emboli. Intimal fragility develops due to intoxication, infections, and poisoning.
The middle (intermediate) shell is represented by elastic connective tissue fibers that provide contraction and relaxation of the wall.
The outer part of the vessel contains veins, arteries, and nerve fibers. Increased strength allows you to maintain the size of the lumen and maintain its shape.
For an aneurysm to form, a defect in the middle and outer lining of the artery is required. Penetration of the intima outward promotes the formation of an additional cavity that accumulates blood. If the thin-walled cavity ruptures, an aneurysm ruptures, leading to a stroke. Destruction of the walls increases the likelihood of blood clots.
Local turbulence in the movement of blood in places of damage causes difficulties for microcirculation. Local stagnation promotes thrombosis. Long-term persistence of the condition causes the accumulation of cholesterol plaques in places of intimal destruction.
Atherosclerosis and high blood pressure create the preconditions for blockage of cerebral arteries when a fragment of a cholesterol plaque breaks off, a blood clot, and migrates to the brain.
Causes of vascular wall defects:
- Acquired - infectious conditions, connective tissue diseases, increased blood pressure, autoimmune destruction of the intima;
- Congenital - genetic predisposition to defects in the vascular stroma, weakness of connective tissue fibers.
Hereditary diseases that increase the risk of cerebral aneurysms:
- Essential hypertension;
- Alpha-1 antitrypsin deficiency;
- Polycystic kidney disease;
- Neurofibromatosis;
- Arteriovenous malformations;
- Sickle cell anemia;
- Fibromuscular dysplasia;
- Tuberculous sclerosis;
- Collagenosis with impaired formation of type III collagen;
- Ehlers-Danlos syndrome;
- Randu-Osler syndrome;
- Marfan syndrome;
- Systemic lupus erythematosus;
- Pseudoxanthoma elastica.
Separately, a nosology called “coarctation” should be highlighted. The condition is accompanied by a congenital defect of the aorta. Occurs in 8% of newborns. The nosology is combined with heart defects and is characterized by a violation of the movement of blood through the narrowed part of the vessel.
Aneurysmal dilatation in arterial hypertension
Persistent elevation of blood pressure is a chronic condition. The etiology of the nosology has not been established, but there are provoking factors that need to be eliminated during treatment.
Essential hypertension or essential hypertension is established when there is a persistent increase in blood pressure over 140 mmHg. mercury column.
An increase in intravascular pressure against the background of nosology leads to the destruction of the vascular wall, promotes the formation of blood clots, and expansion of the middle and outer lining of the artery.
Other provoking factors are inflammatory vascular processes, connective tissue diseases, hereditary predisposition, atherosclerosis.
Infectious causes of aneurysms
Bacterial pathogens cause intoxication and provoke direct tissue damage.
List of infectious diseases that contribute to the formation of aneurysm:
- Meningitis - inflammatory damage to the meninges with transition to the arterial membrane;
- Fungal infections with damage to the cerebral parenchyma;
- Bacterial endocarditis is characterized by blockage of cerebral vessels by blood clots that enter the cerebral arteries from the primary inflammatory focus, which is the heart valves and myocardium.
Aneurysmal cavities of the brain in traumatic brain injury
Closed TBI contributes to the destruction of the skull bones, which cause compression of the cerebral arteries. The pathology is localized inside the cortical parts of the cerebral arteries. An additional danger is rupture of the vessel by a bone fragment, which is formed during fractures.
Magnetic resonance imaging allows one to distinguish between false and true traumatic brain injuries. The first type is formed due to the penetration of blood through the membranes of the vessel, the second - due to the protrusion of the internal intima through the middle and outer wall.
Symptoms of cerebral aneurysms
Most forms occur hidden. Mild symptoms appear only in the presence of mild intracerebral hemorrhage (hemorrhagic permeation).
Focal neurological disorders form large intracerebral formations:
- Muscle cramps are formed by large expansions with compression of the hemispheres;
- Vision pathology is associated with damage to the optic nerve;
- Transient ischemic attack (TIA) is caused by a significant decrease in blood flow through the large cerebral arteries;
- Headaches are provoked by compression of the arachnoid and soft membranes, irritation of pain receptors by inflammation, swelling, and neoplasm;
- Pain in the facial area occurs when the cranial nerves that innervate the masticatory and facial muscles are damaged;
- Doubling of objects before the eyes is provoked by compression, damage to the optic chiasm inside the brain;
- Speech disorders.
Weak symptoms of the pathology develop when the wall of the carotid or vertebral artery expands.
Consequences of cerebral aneurysm
For a long time, aneurysmal expansion does not manifest itself clinically. It is possible to find out about the presence of a dangerous condition after performing a CT or MRI of the head or after a rupture.
In the first case, surgery to remove an aneurysm will save a person’s life, in the second, the consequences are sad. Approximately 50% die immediately or within three months.
25% of people with a ruptured aneurysm develop a disability.
Main consequences:
- Brain swelling;
- Increased intracranial pressure;
- Blockage of the cerebrospinal fluid pathways;
- Displacement of intracerebral structures;
- Subarachnoid hemorrhage;
- Cerebral vasospasm;
- Coma;
- Stroke (ischemic and hemorrhagic).
The risk of rupture of an aneurysmal protrusion of a cerebral artery is about 80%. If a small formation is detected at the beginning of development, negative consequences can be prevented using conservative methods.
Diagnosis of intracerebral aneurysms
Neuroimaging methods (computer and magnetic resonance imaging) help determine changes in brain structures, cerebral hemorrhages, hematomas, and pathology of the vascular wall.
What CT shows:
- Areas of compression of the brain parenchyma;
- Bag-shaped, spindle-shaped extensions;
- Intracranial hemorrhages;
- Bone destruction;
- Brain compression zones;
- Thrombophlebitis of the arteries.
What does an MRI show:
- Intracerebral hemorrhage;
- Pulsation of arteries;
- Expansion of the vascular wall;
- Compression of nerve trunks, medulla;
- Intra-arterial thrombi.
Contrast enhancement methods (arteriography, CT and MRI of cerebral vessels) are used to verify areas of vasoconstriction, atherosclerosis, and areas of circulatory disorders.
Additional diagnostic methods are transcranial ultrasound, positron emission tomography, radiography of the cervical spine, ECG, lumbar puncture, EEG (electroencephalography).
Source: https://mrt-kt-golovnogo-mozga.ru/article/anevrizma-sosudov-golovnogo-mozga