Venipuncture is a puncture of a vein to draw blood, inject medicinal solutions into the vein, transfuse donor blood, administer concentrates for angiography and scintigraphy, and feed the patient with protein mixtures.
During the procedure, the patient's hand should be in a stable position with the palm up. An oilcloth pillow is placed under the elbow. A tourniquet is applied to the middle third of the shoulder. The patient clenches his fist several times to better palpate the vein, and the puncture site is wiped with alcohol. The puncture itself is carried out as follows:
- the needle cut is directed upward;
- angle relative to the skin surface 45 degrees;
- there should be a feeling of “falling” into a vein;
- you can pierce the skin and the vein at the same time, or after piercing the skin, turn the needle so that it enters from the side of the vein;
- after correct venipuncture, blood appears on the needle cannula; if there is none, then you need to turn it without removing the needle from the skin to puncture again.
Blood for analysis is poured into a test tube; when bleeding, one end of a rubber tube is attached to the needle, and the other is directed into a tray; when administering drugs, a system is used. When finished, the tourniquet is removed, the needle is removed, and a cotton ball with alcohol is clamped in the crook of the elbow.
A common site for venipuncture is the vein in the cubital fossa. Additionally, you can use the superficial hands or forearms, lower extremities, and large branches.
In newborns and infants, the veins of the scalp are punctured; at older ages, the vessels of the upper extremities, legs and feet can be used. If the veins are poorly identified, venipuncture of large vessels is performed - subclavian, jugular or femoral veins.
For venipuncture, the donor's two elbows are treated twice in an area of at least 7-8 cm in diameter, the vein is pierced and about 5 mm is passed along its course. After blood appears in the tube, the needle is advanced half its length and is fixed throughout the blood collection.
Venesection is the opening of a vein using an incision; it is performed for poorly defined superficial vessels in patients who require long-term intravenous administration of medications. The veins selected are the same as in venipuncture. The mini-surgery is performed by a surgeon, not a nurse or paramedic.
The vein is removed from the surrounding tissue, 2 catgut nodes are placed on it, and the vein between them is opened. Then the catheter is inserted into the hole and secured with threads. After suturing the skin, the system is connected and, by pulling the threads by the removed ends, the vessel is freed from the knots.
The standard kit includes the following sterile items: a syringe with a needle, a tray, tweezers, cotton balls, gloves and a mask, a hemostatic tourniquet, a pad, ethyl alcohol and a second tray for used materials. For venesection you additionally need: a scalpel, clamps, scissors, needle holders, anatomical and surgical tweezers, catgut, silk, novocaine for pain relief.
Read more about venipuncture, venesection, as well as possible complications afterward in our article.
Indications for venipuncture
A vein puncture may be prescribed in the following cases:
- taking blood for research, autohemotherapy (injection into the buttock) or donation;
- the need for bloodletting (stagnation of blood in severe right ventricular failure, pulmonary edema, excessive formation of blood cells - polycythemia, poisoning with hemolytic poisons);
- intravenous injections for emergency or planned therapy, general anesthesia for operations;
- carrying out infusions - infusion of solutions through a dropper;
- infusions of blood, fresh frozen plasma, red blood cell suspension or its components;
- administration of radiopaque or radiopharmaceuticals during angiography, scintigraphy;
- parenteral nutrition with protein mixtures when the usual intake of food is impossible.
We recommend reading the article about vein catheterization. From it you will learn how to select a catheter, the Seldinger technique, rules for caring for the catheter and how to remove the catheter from the vein. And here is more information about the injection in the heart.
Peripheral vein puncture technique
The basic rule for performing vein puncture is to maintain complete sterility. To do this, you need to wash and dry your hands, put on sterile gloves and a mask. It is necessary to lay the patient down or sit in a chair so that the hand is in a stable position with the palm up. An oilcloth pillow covered with a sterile napkin is placed under the elbow. The nurse applies a tourniquet to the middle third of the shoulder, or a blood pressure monitor cuff can be used.
The patient clenches the hand into a fist several times to better contour the vein. After palpating the vessel, the puncture site is treated twice with alcohol from bottom to top. The skin on the elbow is stretched and the vein is fixed. The puncture itself is carried out according to the following rules:
- the needle cut is directed upward;
- the angle relative to the skin surface is 45 degrees;
- there should be a feeling of “falling” into a vein;
- you can pierce the skin and the vein at the same time, or after piercing the skin, turn the needle so that it enters from the side of the vein;
- after correct venipuncture, blood appears on the needle cannula; if there is none, then you need to turn it without removing the needle from the skin to puncture again.
If blood is needed for analysis, then place a test tube under the outer end of the needle or immediately attach a syringe. When performing bloodletting, the needle is connected to a rubber tube, the other side of which is lowered into the tray. A graduated vessel can also be used to measure the amount of blood released.
Watch the video about puncture and catheterization of peripheral veins:
If the patient is receiving an intravenous solution, then an infusion system and a syringe with medication are connected. For blood transfusion, a special infusion kit is used. After the necessary materials are installed, the venous tourniquet is removed.
At the end of the manipulations, the needle is removed, and a cotton ball moistened with alcohol is applied to the puncture site. To stop bleeding more quickly, the patient bends his arm at the elbow joint as much as possible. If necessary, a pressure bandage is applied to the puncture area.
Locations
The most common place for venipuncture is the vessels that are located in the cubital fossa. The most convenient of them are v. basilica or v. cephalica. They have the shape of the letter V, are close to the surface of the skin, move little, and have a fairly wide opening.
Projection onto the skin of the ulnar veins, which are most often punctured
In addition, puncture can be performed on the following vessels of the venous network:
- superficial veins of the hands or forearms;
- lower extremities;
- large branches - subclavian, femoral or jugular for long-term therapy and installation of a venous catheter.
There is a special group of patients for whom there are exceptions to the general rules. If it is necessary to connect to a device for artificial blood purification, a connection between a vein and an artery is created. The formed arteriovenous fistula should be used only for hemodialysis, and for tests or intravenous injections, the veins of the non-working arm are selected on the back of the forearm or hand.
In newborns and infants, the veins of the scalp are punctured; at older ages, with good peripheral circulation, the vessels of the upper extremities, legs and feet can be used for short-term therapy. If the veins are poorly defined, long-term therapy or the introduction of irritating, concentrated solutions is necessary, then venipuncture of large vessels - subclavian, jugular or femoral veins - is performed.
What it is
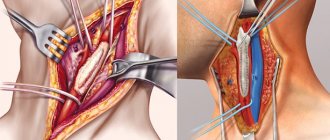
Translated from Latin vena – “vein” and sectio – “cut”. That’s right: during venesection, an incision is made on the wall of the vein, into which a cannula connected to a catheter is then inserted. Intravenous infusions (infusions) are administered through it. But it is impossible to cut a vein directly through the skin. Therefore, a small operation is first performed, exposing the vessel. To do this, they shallowly excise the skin and subcutaneous tissues with a scalpel, pry off the vein and begin to work with it directly.
Venesection has the following indications:
- a pronounced layer of subcutaneous fat;
- very low patient pressure (impossible to find a vein and get into it);
- Anatomically, the veins lie very deep.
Contraindications are problems on the skin at the site of excision. These are burns, fungal or purulent infections, unhealed wounds. A relative contraindication is thrombophlebitis: in this case, the advisability of venesection is decided, because sometimes this procedure is vital.
When performing venesection, they try to isolate large vessels so that the catheter can be freely installed. The following veins are best suited for this:
- ulna (on the inner bend of the elbow);
- internal and external jugular (in the neck);
- subclavian (in the area of the collarbone);
- femoral (in the lower leg area).
Features of the donor
When performing a vein puncture to donate blood, the requirements for sterility increase many times over. The procedure is carried out in specially equipped rooms; it is not allowed to use any consumables without checking the labeling and expiration date.
Pre-treat two elbow bends with antiseptics in an area of at least 7-8 cm in diameter twice. The puncture begins no earlier than 30 seconds after treatment. If a non-sterile object accidentally touches the puncture site, the disinfection procedure is repeated again.
A needle from a polymer container is used to pierce a vein and pass about 5 mm along its course. Then, after blood appears in the tube, the needle is advanced half the length and fixed throughout the entire blood sampling. It is necessary to achieve a fairly rapid flow of blood into the container. If this does not happen, then the following measures are taken:
- change the position of the needle cut;
- reinstall the tourniquet (it remains on the shoulder throughout the blood draw);
- use the other hand.
If repeated venipuncture is unsuccessful, the donor is removed from donating blood.
Complications
During the operation, complications such as bleeding and damage to neighboring nerves are possible. A little later, the following consequences are possible:
- thrombosis;
- phlebitis;
- cannula blockage;
- wound infection.
Complications during venesection are most likely an exception if the procedure is performed by qualified medical personnel.
Differences between venipuncture and venesection
Venesection is the opening of a vein using an incision. It is indicated for poorly defined superficial vessels in patients who require long-term intravenous administration of medications. For this, you can select the same veins as for puncture. But if a regular puncture can be performed by a nurse or paramedic, then venesection is a mini operation. It is performed only by a surgeon under local anesthesia.
The vein is removed from the surrounding tissue, 2 catgut nodes are placed on it, and the vein between them is opened. Then the catheter is inserted into the hole and secured with threads.
Venesection scheme
After suturing the skin, connect the infusion system and, by pulling the threads by the removed ends, free the vessel from the knots.
Technique
Venesection is performed under local anesthesia, usually done with novocaine. After anesthesia and treatment of the skin, an incision is carefully made above the vein and any bleeding from the subcutaneous vessels is stopped. Using clamps, a thread (catgut) is placed under the vein and the vein, or rather its distal segment, is ligated. Then a catheter is opened and inserted into it towards the center, which is tied with the ends of catgut, the skin over the vein is sutured.
The catheter can be left in place for several days by securing it to the skin with a bandage. It is necessary to flush the catheter daily to prevent blood clots from forming in it. The wound is treated daily. Skin sutures are removed on days 6-7.
We also recommend reading: Tracheostomy care algorithm
The technique of performing venesection can be found in the video if you want to get a more detailed understanding of this procedure.
Set for venipuncture and venesection
A standard set for vein puncture includes the following sterile items: a syringe with a needle, a tray, tweezers, cotton balls, gloves and a mask. You also need a hemostatic tourniquet, a pad, ethyl alcohol and a second tray for used materials.
For venesection you additionally need: a scalpel, clamps, scissors, needle holders, anatomical and surgical tweezers, catgut, silk, novocaine for pain relief. The prepared kits are sterilized and stored in separate boxes.
Venesection instrument set
Needle
For venipuncture, needles are used that meet the following requirements:
- short cut and large lumen so as not to destroy red blood cells and not injure the opposite wall of the vein;
- have no deformations or nicks on the tip;
- completely passable.
Regular needles can be used for saline infusions, but larger needles are needed for blood, plasma replacement, or parenteral nutrition solutions.
Dufault needle for blood collection and transfusion
Tourniquet
The use of a tourniquet during venipuncture allows you to create blood flow into the vein for better identification. It is installed at a distance of no closer than 10 cm from the bend of the elbow. There should be a sleeve of clothing or a napkin on the body. It is necessary to ensure that the tourniquet does not pinch the skin. The knot is tightened with a loop down and the free ends up. This is important to prevent the tourniquet from touching the area treated with alcohol.
After installation, it is imperative to feel the pulse on the radial artery or another peripheral one during venipuncture outside the ulnar vein. Prolonged or strong compression of blood vessels and soft tissues should be avoided. Sometimes, instead of a tourniquet, a blood pressure cuff is used; by pumping air into it, you can regulate the intensity of compression of the limb.
Using a tourniquet for venipuncture
Difference from venipuncture
Venipuncture is a routine medical procedure that can be performed by a nurse. It is carried out not only to install a catheter, but also for the purpose of a single administration of a drug through a vein or to collect venous blood. Unlike venesection, venipuncture is much easier and faster to do. And after the procedure, you don’t need to suture anything: you just need to press the wound caused by the syringe needle or catheter for a few minutes.
Another key difference: venesection must be performed with local anesthesia. Venipuncture does not require anesthesia. In rare cases (for example, children), superficial anesthesia is given with external drugs.