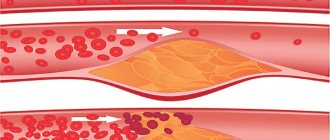
Changes in the structure of blood vessels are a sign of life-threatening processes for the patient, which are not always possible to diagnose in a timely manner. A pathology such as splenic artery aneurysm is poorly amenable to conservative treatment and in most cases is eliminated through surgery.
How operations to remove a splenic aneurysm are performed, what their cost is, and what doctors think about the future of patients who have undergone treatment - read further in the article.
What is a splenic artery aneurysm?
Local pathological dilatation of the vessel supplying the spleen is called a splenic artery aneurysm (SAA). In the structure of all aneurysms of visceral vessels, the ACA occupies up to 60% and affects women 4 times more often than men. Possible localization can be determined by:
- In the main trunk of the splenic artery;
- In its branches;
- In places of vascular branching.
The disease is the cause of death in 11% of patients with acute aneurysmal pathology and has a clinical picture that mimics many surgical diseases.
Aneurysm of the splenic artery is designated by the ICD-10 code - I72.8 (Aneurysm and dissection of other specified arteries).
All methods
The complexity of the operation depends on the location of the aneurysm. If the enlargement is located close to the spleen, doctors insist on splenectomy—removal of the organ along with the aneurysm. Such intervention does not affect the patient’s lifestyle.
If the aneurysm is located in areas distant from the spleen, due to the complexity of direct surgery, minimally invasive techniques are used.
Given that the spleen is well supplied with blood and has many sources of nutrition, blocking blood flow in the main artery does not impair the functionality of the organ. Therefore, whenever possible, doctors use methods that exclude the aneurysm from the general blood flow:
- Angioplasty and stenting (average price from 100 thousand rubles).
- Embolization (average price from 40 thousand rubles).
Angioplasty is a surgical method that allows you to expand the lumen of blood vessels for subsequent stenting. During the operation, a catheter equipped with an expanding balloon is inserted into a small incision. Once the catheter reaches the required area inside the vessel, the doctor expands the lumen by inflating the balloon.
The process is monitored through an X-ray monitor. The procedure is painless, since the inner wall of the vessels does not have nerve endings.
Then, to strengthen the stenotic effect, a catheter with a stent is inserted - a cylindrical wire frame covered with a sealed film. Doctors use balloon inflation to press the stent against the artery walls. Upon completion of the operation, the catheter with the balloon is removed from the vessel cavity.
When using the embolization method, a coil is placed in the cavity of the aneurysm, thrombosing it and isolating it from the main blood flow. The use of the method allows you to completely preserve blood circulation in the splenic artery. The lumen of the expansion closes, eliminating the possibility of its subsequent rupture.
Minimally invasive endovascular surgery to remove a splenic artery aneurysm can take from 45 minutes to 3 hours.
Types of ASA
Based on morphology, two groups of formations are distinguished:
- Saccular aneurysms of the splenic arteries - develop at the origin of the branches of the artery;
- Diffuse - in the area of its main trunk.
According to origin they are distinguished:
- True aneurysms are more common in women. Anatomically repeat the vessel wall;
- False (traumatic) – more common in men. Represented by connective tissue. Find out more about false and true aneurysms here.
In 80% of cases, one aneurysm develops. Multiplicity of lesions is observed in 20% of patients.
You can find out all the details about the types, location and methods of treatment, including clipping or removal of an aneurysm, in separate articles on the pages of our website.
What complications can there be?
The main danger is that the splenic artery may rupture. If the patient is not provided with first aid, this will lead to death. Basically, there are two types of rupture: complete and incomplete. In the first case, the wall of the vessel, which was deformed, is completely damaged, a hematoma is formed, and the person himself experiences severe pain and anemia at this time. If the aneurysm does not rupture completely, a hematoma forms behind the peritoneum and the bleeding stops for a while, and the patient’s blood pressure decreases. In any case, you should not hesitate to go to the hospital, where specialists will be able to diagnose and prescribe the correct treatment.
Causes and risk groups
Among the causes, the most probable (occurring in 70% of patients) and possible are distinguished. Most likely reasons:
- Muscular fibrous dysplasia;
- Hypertension in the portal vein system in combination with an enlarged spleen (splenomegaly);
- Liver transplantation;
- Vascular complications of pregnancy.
Possible reasons:
- Diseases of the endocrine glands;
- Atherosclerosis;
- Inflammatory diseases of the abdominal organs (pancreatitis, stomach ulcer);
- Hypertonic disease.
People at risk are:
- Suffering from bacterial endocarditis;
- Pregnant;
- Patients with alcoholism, drug addiction;
- Smoking abusers;
- Those who have suffered any types of trauma, including surgical interventions on the abdominal organs.
Up to 10% of ASA are infectious in nature. The pathology is found in 40% of pregnant women (with a third or more pregnancies), and in 20% of men after operations on the abdominal organs.
Main signs and distinctive symptoms
A feature of the disease is the variety of nonspecific manifestations. Some patients are asymptomatic. Signs differ in uncomplicated and complicated cases.
Symptoms in the uncomplicated form:
- Dull periodic or constant pain localized in the left hypochondrium;
- Pain may radiate to the left costovertebral angle;
- The pain increases in proportion to the size of the aneurysm.
The complicated course is acute and can mimic many surgical diseases . The following symptoms are observed:
- Cutting, cramping pain in the abdomen and lower back;
- Fever up to 38 degrees or higher;
- Increased breathing and heart rate;
- “Board-shaped” tense abdomen;
- Bloody stool;
- Local swelling in the lumbar region (appearance of retroperitoneal hematoma);
- Fall in blood pressure.
The complicated course of ASA in pregnant women imitates obstetric pathology:
- Placental abruption;
- Amniotic fluid embolism;
- Uterine rupture.
ASA is characterized by the phenomenon of “incomplete rupture”, observed in 25% of patients. At the time of rupture, only part of the aneurysm is damaged, which leads to a temporary stop of bleeding due to a compressive hematoma. During this period, most patients feel an improvement in their condition, but after 1-2 days the rupture becomes complete, which causes a repeated attack of “acute abdomen” and worsens the prognosis for life.
Danger and complications
The danger of the disease is expressed in the following:
- The clinic is nonspecific;
- An increase in education may not be accompanied by a deterioration of the condition for a long time;
- With large sizes, the blood supply to internal organs is disrupted.
The combination of these factors leads to the fact that the symptoms of complications may be the first and only manifestation of the pathology.
Without treatment, the following complications are likely:
- Aneurysm rupture:
- Hemorrhage into the abdominal cavity or retroperitoneal space;
- Development of arteriovenous fistula;
- Retroperitoneal hematoma;
- Pancreatic necrosis;
- Infection;
- Peritonitis.
The probability of rupture with a formation diameter of up to 2 cm is 5-10%, less than 2 cm - 2%.
Those at risk for a complicated course are:
- Pregnant women;
- Patients after liver transplantation.
After treatment as planned, no complications are observed. When treating complicated conditions, the following may develop:
- Bleeding from the pancreas or stomach;
- Secondary infection;
- Sepsis.
Diagnostics
Questioning, examination and objective research are ineffective. Auscultation can detect a systolic murmur over the area of the aneurysm only in 10-12% of cases.
Confirmation of the diagnosis is carried out using instrumental methods:
- Radiography . A specific symptom of ASA is a “calcified ring” - an area of the vessel that has undergone the deposition of calcifications. The symptom indicates atherosclerosis and a long course of the disease;
- Ultrasound . A round anechoic (dark) formation in the projection of the spleen or pancreas, filled with blood, is identified;
- Duplex scanning . The method is used to determine the diameter of the aneurysm and the nature of the blood flow in it;
- Selective angiography . The technique helps to detect thrombotic masses characteristic of this formation;
- CT allows one to differentiate an aneurysm from other diseases by the vascular structure of the wall, as well as by the connection with the splenic artery, which does not happen with tumors and cysts. A specific symptom is calcifications;
- MRI is used to differentiate aneurysms from cysts and other neoplasms. The method helps to determine compression of internal organs and retroperitoneal hematoma.
You will find complete information about vascular diagnostics in this article.
Often an aneurysm is discovered accidentally, during ultrasound diagnostics or x-ray examination. And it can arise in completely different places. Read about the manifestation of this formation in the following organs and parts of the body: heart, brain, carotid artery, neck, lungs, aorta (ascending, descending and thoracic) and lower extremities.
Treatment
If the size of the formation is up to 2 cm and there are no complaints, the patient is monitored dynamically:
- Periodic examinations by a vascular surgeon;
- Ultrasound once every 6 months.
Indications for surgical intervention:
- Diameter more than 2 cm;
- Presence of complaints;
- Pregnancy;
- Childbearing age (up to 45 years);
- Threat of rupture.
Operations can be endovascular and reconstructive.
The method of choice is endovascular occlusion (closing the lumen) of the splenic artery . The operation is performed on all patients whose aneurysm is not associated with inflammatory diseases of the pancreatic gland or stomach. The remaining patients undergo open surgery:
- Ligation (application of a ligature to a vessel);
- Removal of protrusion;
- Resection with removal of the spleen (if the formation is located at the distal part or at the hilum of the organ);
- Resection with removal of part of the pancreas (in case of inflammation spreading to the pancreas).
We bring to your attention 2 articles about the possibilities of diagnosing and treating splenic artery aneurysms:
- . Authors: M. B. Patsenko, V. A. Ivanov, A. V. Obraztsov, D. A. Mironenko, S. N. Kryzhov, N. V. Obraztsova, V. L. Smirnov.
- . Authors: M.V. Vishnyakova, A.I. Lobakov, A.V. Lerman, G.A. Stashuk, S.E. Dubrova, A.V. Vashchenko, I.N. Demidov, E.A. Stepanova, A.G. Platonov.
All about medicine
The prevalence of splenic artery aneurysms ranges from 0.1% to 2%. Although this disease is rare, it remains the most common (50 - 75%) among all visceral (related to internal organs) aneurysms. The predominance among women occurs in a ratio of 4:1.
The disease is often asymptomatic and is discovered during the diagnosis of some other disease or rupture, and this is already a life-threatening condition with a high mortality rate.
Currently, the threshold for treatment of asymptomatic patients is an aneurysm diameter greater than 2 cm. Additional factors that may require intervention include pregnancy, portal hypertension, cirrhosis, and patients requiring liver transplantation.
Pregnant women with a ruptured splenic artery aneurysm experience a high mortality rate of 70% to 90%. The critical period for them begins in the last trimester, especially during childbirth.
There are differences between true and false aneurysms. True aneurysm is often associated with hormonal changes and increased blood flow that occurs when physiological changes occur during pregnancy. On the other hand, pseudoaneurysm occurs when the arterial wall is damaged due to trauma or under the influence of enzymes in pancreatitis.
Aneurysm size is not clearly associated with the risk of rupture, and systematic treatment of all visceral aneurysms is recommended.
ENDOVASCULAR TREATMENT OPTIONS
Endovascular treatment has gained widespread acceptance mainly due to its high technical success rates coupled with significant improvements in patient outcomes and low mortality compared with open surgical repair.
The goal is to achieve complete occlusion (patency) of the vessel outside the aneurysm. The main techniques are angioplasty and stenting.
In angioplasty, the use of a guide catheter may be difficult to catheterize tortuous vessels and may therefore complicate balloon insertion in this anatomy. However, control of the delivery system using x-ray endovascular methods greatly simplifies the task.
In case of aneurysm of the splenic artery, a procedure with preservation of the parent artery is possible with the implantation of covered stents. The main limiting factor of this approach is the tortuosity of the artery. However, recent studies using low profile stent grafts offer new possibilities if the diameter of the artery itself is adequate. In addition to maintaining vessel patency, implantation of a stent graft has a number of advantages.
Classic transcatheter aneurysm embolization with coils is another option that is used to maintain blood circulation in the artery. The use of split spirals allows for more precise deployment. This approach is intended for patients with saccular aneurysms that have a narrow neck and in which deployment of the coil is associated with a low risk of coil displacement.
Percutaneous approach. In cases of difficult vascular access to the splenic artery (this may be due to its size, location, or vascular anatomy), a percutaneous approach may be considered. This can be done using ultrasound guidance.
NEW TECHNOLOGIES
The self-expanding stent has been approved in Europe in recent years for the treatment of peripheral vascular aneurysm. It is made of phynox and its design consists of a three-dimensional braided tube made of two layers interconnected. The multilayer configuration along with the three-dimensional geometry results in reduced velocity within the aneurysm sac while maintaining flow in the main artery and surrounding branches. A case of treatment of a hepatic artery aneurysm using such a stent was recently reported. Therefore, it can be assumed that such devices will be used for visceral aneurysms, including splenic artery aneurysm.
There are several endovascular approaches to the treatment of splenic artery aneurysms. These are reliable procedures with high technical success and low periprocedural morbidity. Treatment options depend on the location of the aneurysm, the patient's age, and physiological and clinical conditions.
The ISC Vascular Surgery Clinic uses various endovascular techniques, including installation of a stent graft in a peripheral artery.
False aneurysm of the splenic artery
False aneurysms are most typical for men and are represented by connective tissue sacs connected to the artery through a scar bridge. These are formations of scar etiology that develop after injury or against the background of a surgical disease. In 90% of patients they are a complication of pancreatic cysts.
Distinctive features:
- Long-term asymptomatic course;
- Less risk of ruptures and complications;
- There is a high probability of complete calcification.
The main manifestation is dull periodic pain in the left half of the back or left hypochondrium, which occurs during physical activity . Diagnosis is not difficult. The most effective are MRI and CT, through which they detect a scar formation that fills with blood through the connecting bridge with the splenic artery.
Treatment is surgical. The following types of interventions are performed:
- Ligation of the vessel with subsequent installation of drainage;
- Removal of a cyst or distal part of the pancreas;
- Suturing the artery wall.
. Authors: D.M.N., prof. S.S. Shestopalov, D.M.N., prof. S.A. Mikhailova, D.M.N., prof. A.N. Tarasov, A.P. Efremov, N.F. Zinich, K.M.N. B.H. Sarsenbaev.
ICD-10 code for cerebral atherosclerosis
Stopping blood flow in the area of cerebral vessels can cause deadly complications, so it is extremely important to detect cerebral atherosclerosis in a timely manner. In ICD 10, vascular pathology is classified in class IX, where all diseases of the cardiovascular system are systematized. Every doctor working with the International Classification of Diseases, 10th revision and using this section knows the code of the desired disease. If necessary, codes are used that indicate complications that arise against the background of cerebral atherosclerosis.
Cerebrovascular pathology
In ICD 10, all diseases associated with pathological changes in cerebral vessels are limited to codes I60-I69. Cerebral atherosclerosis has a separate code, designated as I67.2, but the doctor will make this diagnosis only after absolute certainty of the presence of the disease. Sometimes the designation of the disease will be preliminary: upon completion of a full examination, the diagnosis may be changed. The reason for this doctor’s tactics is easily explained - the symptoms of brain pathology do not always immediately indicate the presence of blockage of the arterial trunks of the brain. Therefore, the doctor selects section I67 “Other cerebrovascular diseases”, where general diagnoses are grouped. In addition, the following pathology is found in this section:
- dissection of cerebral vessels without threat of rupture (I67.0);
- cerebral aneurysm without rupture (I67.1);
- encephalopathy due to progression of vascular pathology (I67.3);
- encephalopathy
Forecasts
The prognosis is relatively unfavorable. Life-threatening conditions develop in only 2% of patients, but mortality from complications reaches 25%. Among pregnant women, mortality from complications reaches 70%. Postoperative mortality in complicated patients reaches 30%, but not in planned patients.
With timely detection and treatment of the disease, the duration and quality of life do not change.
Splenic artery aneurysm is a common type of vascular pathology of internal organs. The disease is characterized by frequent involvement of women and a possible asymptomatic course. At risk are pregnant women, as well as people suffering from surgical pathology of the abdominal organs.
If you experience pain in the left hypochondrium, you should immediately seek medical help. Timely instrumental diagnostics contributes to the selection of adequate treatment and the prevention of serious complications.
How does a false aneurysm manifest?
False aneurysm is rare, but is considered the most dangerous. The reason for the appearance of such an aneurysm may not be a deformed splenic artery, but a rupture of the vessel and the formation of a hematoma. The disease can be detected when the patient has bleeding from the upper intestine, and there will be no reason for the manifestation of this symptom.
A doctor can also diagnose a false aneurysm by the appearance of noise; it will intensify during pulsation and listening to noise in the internal organs.