Types of phlebography
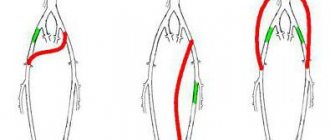
Depending on the method of carrying out, venography of the veins of the lower extremities is divided into two main types: ascending and retrograde. Ascending is used to determine the shape, size, location of venous vessels.
Retrograde venography is used to examine the valves that are located in the venous vessels. The peculiarity is that it is carried out with breath holding. In this case, valves that do not have defects in their operation retain contrast, and those that have any violations allow contrast to pass in the opposite direction.
How phlebography is performed - research technique
The algorithm for performing the manipulation in question will depend on the study area:
Phlebography of the lower extremities
Lasts, on average, about 30 minutes.
- The patient is placed on the couch.
- The contrast agent is administered through a vein in the foot or leg. If it is not possible to puncture a vein due to excessive swelling, it is cut, after first numbing the working area. The patient should try to relax as much as possible. In order for the specified substance to spread more actively, a tourniquet is applied to the limb.
- After taking targeted photographs, saline solution is poured through the same needle in order to completely wash out the coloring substance from the veins. Only after fluoroscopy confirms that there is no contrast agent in the veins is the needle removed.
- This procedure is completed by applying a bandage.
The patient may complain of slight malaise and loss of strength after phlebography of the veins of the lower extremities. This condition is a consequence of incomplete removal of the coloring substance from the body. To quickly return to normal, it is recommended to drink plenty of fluids.
Phlebography of the brain
It is carried out without the use of a contrast agent, so side effects, as a rule, do not occur after the study. The procedure lasts about 20 minutes and is similar to a standard MRI.
MR phlebography of cerebral vessels
The patient is placed on a movable couch, which gradually moves to the center of the magnetic ring.
The tomograph records signals emanating from the anatomical structures of the brain and creates a specific image, on the basis of which the doctor can confirm - or refute - the preliminary diagnosis.
Phlebography of the pelvic veins
It is considered an invasive procedure. It is also called transuterine venography.
- A contrast agent is injected into the wall of the uterus by puncturing it.
- To bring a catheter with a needle to the puncture area, a medical conductor made of fluoroplastic is used, which, unlike a metal medical instrument, is not capable of damaging the integrity of the uterus.
- A few seconds after the injection of the coloring agent, a series of photographs are taken.
In general, the described procedure lasts 20-30 minutes.
Phlebography for men
It is practiced for diagnosing and monitoring the effectiveness of treatment measures for varicocele. Due to the high risk of tissue injury, this technique is rarely used.
After using local anesthesia, a contrast solution is injected through a vein at the root of the scrotum. The doctor uses X-ray equipment to monitor the rate of spread of the drug in the groin area.
Using this type of diagnosis, it is possible to find out the exact diameter of the spermatic vein and its structure.
Video: Phlebography after sclerotherapy of the left testicular vein
Indications for use
Phlebography is a research method that is used for venous disease. It is mainly used for pathology of the veins of the lower extremities and pelvic organs. The main diseases requiring radiopaque venography include:
- varicose veins with ambiguous results of functional tests, which are carried out primarily in the diagnosis of varicose veins;
- postthrombophlebitic syndrome;
- recurrent varicose veins of the lower extremities;
- acromegaly (enlargement of the limbs due to increased production of growth hormone from the pituitary gland) for the purpose of visualizing the venous system of the legs;
- trophic ulcers as a consequence of varicose veins;
- as a control for sclerotherapy.
results
In both groups of patients, the main etiological factor in the development of VBT, VV and PV, according to the anamnesis, was pregnancy and childbirth. It was during pregnancy (primary or repeat) that women experienced PV and PV, and after childbirth, pelvic pain. The number of pregnancies and births in the groups did not differ statistically and ranged from 1 to 3. In table 1 presented
Table 1. Clinical characteristics of patients of groups 1 and 2 Note. Here and in the table. 2, 3: percentage in brackets. clinical characteristics of the examined patients.
Ultrasound examinations.
In group 1, 10 patients had valvular insufficiency of the left gonadal vein, 2 had bilateral lesions of the gonadal veins, and 1 had valvular insufficiency of the internal iliac veins (SIV). During ultrasound examination of the intrapelvic veins, no attempts were made to assess the condition of the parietal tributaries of the SVC (obturator, internal pudendal and inferior gluteal veins), since, firstly, their visualization is associated with significant time costs, and secondly, ultrasound examination seems to be a low-informative way to assess the valvular apparatus of the tributaries The SVC and, thirdly, all patients were scheduled to undergo radiocontrast venography, which is still considered the most accurate method for studying the intrapelvic veins, including the tributaries of the internal iliac veins. Pathology of the main superficial veins of the lower extremities was not detected in any observation (Table 2).
Table 2. Results of ultrasonography of the veins of the pelvis, perineum and lower extremities in patients of groups 1 and 2.
PPR in the 1st group was found in 16.6% of patients, in the 2nd - in 100%.
Phlebographic studies.
No complications were recorded during or after phlebography. The duration of the diagnostic procedure was 20-30 minutes.
1st group.
Valvular insufficiency of the gonadal veins was detected in 100% of patients: 10 (83.3%) were diagnosed with left-sided lesions, 2 (16.6%) - right-sided. In none of the cases, according to phlebography, was an anatomical connection established between the ovarian and superficial veins of the perineum or lower extremities (Fig. 1).
Rice.
1. Phlebograms. a — valvular insufficiency of the left gonadal vein (1); b — valvular insufficiency of the pampiniform venous plexus (2), parametric (3) and uterine (4) veins (indicated by arrows). Retrograde contrasting of parametric veins was found in all patients, uterine veins - in 8 (66.6%). Reflux of the contrast agent along the trunk of the left SVC was recorded in 2 (16.6%) women, along the left obturator vein - in 2 (16.6%) (Fig. 2).
Rice. 2. Pelvic venogram. Reflux of contrast agent along the left internal iliac (1) and left obturator (2) veins (indicated by arrows).
It should be noted that visualization of this parietal inflow was obtained in one woman with valvular regurgitation of the left SVC and in one without it. In the remaining patients, even selective catheterization of the SVC tributaries was not accompanied by visualization of the SPV, i.e., no reflux of the contrast agent was recorded from the internal tributaries into the superficial veins of the perineum, including 2 patients with VV.
In one case, a uretero-ovarian conflict was detected when the right ureter was compressed by the right gonadal vein, which was accompanied by impaired urine passage and pyelectasis (Fig. 3).
Rice. 3. Ovaricogram. Right ureter (1) and right gonadal vein (2), right-sided pyelectasis (3) (indicated by arrows).
Compression of the left common iliac vein by the right common iliac artery (May-Turner syndrome) was diagnosed in 2 patients (Fig. 4).
Rice. 4. Pelvic venogram. Compression of the left common iliac vein by the right common iliac artery (indicated by an arrow).
Thus, the results of the use of OGTF in the group of patients with VBT and TVP proved that this method is necessary to confirm the diagnosis, identify the features of the anatomical structure of the gonadal and intrapelvic veins, pelvic arteriovenous and ureterovenous conflicts. This is extremely important for the choice of treatment method and the order of surgical interventions.
2nd group.
Valvular insufficiency of the left gonadal vein was found in 15% of patients. An anatomical connection between the gonadal and superficial veins of the perineum and lower extremities was not identified in one of the observations. Reflux of contrast agent through the parametric veins was diagnosed in 100% of those examined, and through the uterine veins - only in 10%. Retrograde contrast of the trunk of the left SVC was recorded in 3 (15%) patients, the left obturator vein - in 2 (10%), and the left internal pudendal vein - in 1 (5%) patient (Fig. 5).
Rice.
5. Pelvic venogram. Catheterization of the trunk of the left internal iliac vein. Contrasting the internal pudendal (1) and obturator (2) veins (indicated by arrows). It should be noted that reflux of contrast agent along the SVC tributaries was detected only in the case of their selective catheterization. When contrast was introduced into the trunk of the SVC on the left and right and a Valsalva maneuver was performed with a breath hold for at least 5 s, no retrograde flow of contrast into the parietal tributaries of the SVC was detected. Visualization of the internal pudendal and obturator veins did not show further spread of the contrast agent into the superficial veins of the perineum or lower extremities, i.e., according to the results of phlebography, there was no obvious connection between the intrapelvic, vulvar and perineal veins, which means there was no continuous, permanent PPR.
Arteriovenous and ureterovenous conflicts were not identified in this group of patients.
The results of ultrasound and venographic studies showed comparable, almost identical results (Table 3).
Table 3. Results of ultrasound and radiological methods for studying the veins of the pelvis, perineum and lower extremities in patients of the 1st and 2nd groups
Contraindications for carrying out
Since venography is a radiopaque and invasive research method, there are a number of contraindications to its use. Moreover, a person may experience both conditions that prohibit the administration of contrast, and those that exclude the use of x-rays in principle.
The main contraindications include:
- Allergic reaction to contrast. In most cases, an iodinated contrast agent is used, and if the patient is allergic to iodine, the contrast can be replaced with gadolinium.
- Chronic diseases in the stage of decompensation.
- Acute infectious diseases.
- Severe renal or liver failure. With these pathologies, it is difficult to remove the contrast agent from the body.
- Pregnancy is a contraindication to any x-ray examination, since x-rays have a detrimental effect on the fetus.
- Conditions in which bleeding may develop when contrast is administered: hemophilia, thrombocytopenic purpura.
- The presence of inflammation in the area of trophic disorders.
- Senile age (relative contraindication).
Contraindications
Contraindications are divided into relative and absolute. With the latter, no research is carried out. Relative – a reason for a thorough analysis of the situation and making a decision based on the patient’s condition.
Relative contraindications include:
- age over 60;
- pregnancy;
- sensitization of the body.
To absolute:
- pathology of the kidneys and liver in the acute stage;
- tumor growth;
- blockage of a vessel;
- individual intolerance to the drug;
- serious condition of the patient;
- skin lesions in the area of access to the vein.
The essence of the method
The presence of contrast, which fills the veins and is visible under the influence of x-rays, allows the radiologist to see the shape and location of the veins, the presence of a defect in them, a violation of blood flow, which the specialist will describe as a “contrast filling defect.”
What can be seen using phlebography of the veins of the lower extremities and pelvis? It allows you to diagnose:
- the presence of an embolus in the veins;
- blockage of veins with blood clots;
- anomalies in the structure of blood vessels of both congenital and acquired origin;
- disturbances in the functioning of venous valves, their patency, diameter;
- number and structure of communication veins.
In most cases, venography is not the diagnostic method of choice; it is performed after unclear and questionable results of non-invasive examination methods. It is used not only for diagnosis, but also as one of the preparatory methods before surgery. For example, to visualize a vein before bypassing it.
To reduce the radiation exposure to the patient, it is possible to use a large-frame fluorograph, which allows you to reduce the procedure to one minute, taking up to 9 pictures during this time.
Interpretation of results
All X-rays, MRI or CT images obtained as a result of the examination should be interpreted only by a radiologist. The resulting conclusion is transferred to the patient’s attending physician, who referred him for the venography procedure.
example of the results of CT phlebography of the legs, done for more effective preparation for phlebectomy surgery
In the protocol of venography of the lower extremities with a normal X-ray picture, you can see phrases such as the function of the valvular apparatus of the veins is preserved, the patency of the veins is normal, no filling defects or “breakage” of the contrast were detected. In the case of thrombosis, these changes are present due to complete or partial obstruction of the venous lumen for contrast.
Regarding MRI phlebography of the brain, we can say that the examination protocol is complex, with many nuances that are understandable only to specialists. In the absence of pathological formations, the corresponding phrase is indicated in the conclusion; if present, the location, size and topographic relationship of the pathological formation and healthy tissue are indicated.
When performing transuterine venography, varicose veins of the small pelvis can be identified, and then their detailed characteristics are also given. The development of thrombophlebitis and phlebothrombosis is also manifested by a break and a defect in contrast filling.
Preparing for the examination
Since the method is invasive (using X-ray radiation), phlebography of the lower extremities requires careful preparation. The main activities are:
- Refusal to eat at least 4 hours before phlebography; only water is allowed to drink.
- Before the administration of a contrast agent, an allergy test is performed 1-2 days using subcutaneous injection of 0.1 ml of contrast and subsequent observation of the skin reaction. The presence of any signs of allergy (itching, rashes, redness) is a contraindication to the administration of an iodine-containing contrast agent.
- A few days before the examination, a coagulogram (determination of blood clotting), a general blood and urine test, and an electrocardiogram are performed.
- Right before the procedure, the patient must empty his bladder, undress completely, and put on a hospital gown.
- If the patient is very afraid of the procedure and is anxious, the doctor may prescribe sedatives.
- If pain occurs during the procedure, the patient is given sedatives or analgesics.
How to prepare for phlebography, and what preparation program will be prescribed before the procedure?
Shortly before the procedure, the doctor should talk with the patient to identify contraindications. If there are any allergic reactions, the patient must notify the doctor.
The doctor should also inform you in advance about possible negative phenomena that may occur during phlebography: nausea, itching, squeezing sensations in the chest and/or throat. Any discomfort in such a situation should be reported to the doctor immediately.
After receiving all the necessary information, the patient must sign a consent document for the specified type of study.
In addition, before this procedure, you should take a blood test for coagulation .
On the day of phlebography, you should adhere to the following recommendations:
- Do not eat anything 4-6 hours before the procedure. This minimizes the risk of developing nausea at the time of the study. You are allowed to drink non-carbonated water. There are no such restrictions when performing phlebography of cerebral vessels.
- Remove metal objects located in the research area . When examining the condition of the veins of the lower extremities, you must take off your clothes and put on a robe. In the case of diagnostic measures aimed at studying the blood vessels of the brain, the patient should take care in advance of removing jewelry, removable dental structures, hearing aids - and other items that the doctor will tell you about.
- Before the procedure you need to go to the toilet.
If the patient is too suspicious, he is given sedatives (in the absence of contraindications).
Methodology
How is phlebography done? Position of the patient in the X-ray room: horizontal, on the back, on a hard surface. There should be nothing under your feet; they should lie flat and motionless. Next, a tourniquet is applied to the ankle for better contrast administration.
After applying a tourniquet, an injection of novocaine solution is given to relieve vasospasm. Next, the X-ray table is installed in a vertical position and saline is injected into the dorsal artery of the foot, followed by a slow injection of contrast for 1-1.5 minutes. If it is not possible to puncture a vein, then a small incision is made (venesection). The doctor should warn the patient about possible reactions to the administration of contrast: nausea, burning, dizziness, etc. If they occur, the patient should immediately inform the doctor.
Once the contrast is injected, the radiologist watches the contrast agent spread through the veins and takes the necessary pictures. When the result is obtained, a special solution is injected to remove the contrast. Only when fluoroscopy shows that the contrast has been completely removed, observation is stopped and the needle is removed.
At the end, it is necessary to apply a pressure bandage to the limb at the site of contrast injection and wrap the leg with an elastic bandage. The doctor should warn the patient that he should not move the limb for the next couple of hours.
When to examine with MRI and how
Tomography can be used on any part of the body if contrasting of blood vessels is not possible, and it is also the main way to diagnose diseases of the venous system of the brain.
Before an MRI, the patient must remove all metal objects and lie on his back on the scanning bed. Place a small pillow under your head and bolsters under your feet. The head is placed in the direction of the magnet. The couch is pushed into the apparatus, and the center of the beam is fixed above the study area.
The entire procedure does not take more than 20 minutes and is not accompanied by any discomfort. Refers to the most accurate methods of diagnosis.
Watch the video about magnetic resonance venography in the diagnosis of venous outflow disorders:
Possible complications
As a rule, phlebography of the veins of the lower extremities goes well. However, sometimes unwanted side reactions and complications may occur:
- inflammatory diseases at the injection site (abscess, skin cellulitis);
- inflammation of the venous vessels (phlebitis);
- allergic reactions to the administration of a contrast agent - from mild (urticaria, redness of the skin, itching) to severe (anaphylactic shock, Quincke's edema);
- development of renal failure;
- blood clotting disorder (formation of blood clots and blockage of blood vessels by them);
- in a patient with acute viral diseases, the condition may worsen.
Possible complications during and after the procedure
The most dangerous condition is an anaphylactic reaction to a contrast agent. It is manifested by severe swelling, agitation, fear of death, darkening of the eyes, a drop in blood pressure, and an attack of suffocation. Can have serious consequences on the patient's life if help is not provided immediately.
As the contrast agent passes through the vessels, there is nausea, a feeling of warmth or slight tingling, and sometimes slight pain is noted. When administered intravenously, perforation of the vein and development of phlebitis at the injection site may occur.
The intraosseous method is more dangerous due to the occurrence of osteomyelitis or areas of bone necrosis. Intrauterine contrast in rare cases results in uterine perforation and endometritis. MRI diagnostics are not accompanied by noticeable side effects or complications.
Phlebography of the pelvic veins
Although most people associate venography only with the diagnosis of pathology of the veins of the lower extremities, it is also used to detect disturbances in blood flow in the veins of the pelvis. It is most often used in gynecology. It allows you to evaluate not only the veins of the pelvis, but also the venous bed of the uterus. The method allows you to diagnose varicose veins of the first degree, a characteristic feature of which is the corkscrew-like course of blood vessels.
Dilatation of the pelvic veins is an early sign of the development of valve insufficiency long before the appearance of any symptoms. If dilation or ectasia of the veins is not diagnosed in time, varicose veins or dilation and inflammation of hemorrhoidal veins may develop in the future.
Phlebography results
The following conclusions can be considered a normal examination protocol:
- the valves of the veins are not changed, their function is preserved;
- vascular patency is not impaired;
- There are no defects in vein filling or image interruption.
When pathology is detected, the localization of blood clots, the degree of varicose veins, and weakness of the valve apparatus are described. MRI scanning confirms or removes the assumption of vein thrombosis, compression from the outside. If an abnormal formation is detected, it is fixed, the size is measured and the location is noted.
Modern methods of phlebography
Medicine is improving every day, including phlebography. One of these modern methods is CT venography. Although this method also refers to X-ray, it is more advanced. The main advantages of CT venography:
- is carried out using a special device - a tomograph, which makes it possible to more accurately visualize the vessels and take a large number of pictures at once from different angles;
- three-dimensional image allows you to examine the vein in detail from different sides;
- less radiation exposure due to a more advanced CT scanner mechanism;
- does not require hospitalization of the patient in a hospital and further observation.
CT venography does not allow one to see changes in the veins over time, but it helps in diagnosing damage to the veins of the pelvis, retroperitoneum, and chest. Another highly effective method for visualizing veins is MRI venography.
Phlebography of the brain
Application
phlebographic visualization of veins and venous sinuses of the brain
Phlebography (venography) of the brain is performed exclusively using an MRI or CT scanner, without the introduction of a radiocontrast agent. This is due to the fact that obtaining a series of targeted images, performed layer by layer, is sufficiently informative even without introducing contrast.
This type of study allows you to confirm or exclude pathology of the venous sinuses, as well as the superficial and deep veins of the brain. This pathology can be caused by various diseases (inflammatory - meningoencephalitis, tumors, brain injuries, diseases of the blood system), but their danger lies in the occurrence of thrombosis of the veins of the specified localization. As a rule, phlebography examines the venous sinuses of the brain, the vein of Galen, and the internal veins of the brain.
Preparation for the procedure
No special preparation is required for MRI venography of the brain. You are allowed to eat at any time, including breakfast on the day of the study. The only thing a patient should take care of before an MRI is to remove all metal objects (watches, jewelry, glasses), and also leave credit cards, removable dentures, ballpoint pens, hearing aids and some others outside the office items. In the case where the patient has implanted ferromagnetic (capable of magnetization when exposed to a strong magnetic field) medical supplies, for example, pacemakers, stents, vascular clips, hearing aids, MRI venography is absolutely contraindicated for him. In this case, it is possible to perform a study using a CT machine.
How is the research conducted?
Cerebral venography is performed as a routine examination using a tomograph. The patient is invited to enter the room with the MR unit and is placed on a movable table, which will gradually move to the center of the ring formed by the magnet. At this time, special equipment catches and records signals reflected from the internal structures of the brain, including from blood vessels, resulting in the formation of a certain picture that allows one to confirm or exclude a preliminary diagnosis. In general, the study does not cause discomfort to the patient and takes from 20 to 30 minutes.
MRI venography: features
The main advantage of this method of examining veins is the possibility of performing it in patients with allergies to iodine-containing contrast agents, since it is possible to perform MRI venography of veins without the use of contrast.
Also, this research method excludes radiation, since it is not x-ray. The essence of MRI is the reaction of the electromagnetic field to the concentration of hydrogen ions in tissues. Since different tissues contain different amounts of hydrogen ions, they will be visible in different colors on MRI. The main contraindication is the presence of any metal objects in the body (pacemaker, prosthetic joints, clips on blood vessels).
Venography results
With a normal structure of the vessels and the absence of their pathology, phlebography of the veins of the lower extremities shows that the dye quickly and evenly fills the lumen of the vessel. If filling with contrast slows down or stops altogether, or if a filling defect is observed, then the patient may have an obstruction to the flow of blood through the venous vessels (thrombosis, embolism).
At the moment, traditional X-ray contrast venography is used less and less, giving way to more modern examination methods: CT, MRI venography, ultrasound examination of blood vessels. However, venography is a method that is still widely used in many treatment and diagnostic centers due to its availability and low cost.
Pelvic venography
Previous14Next
Pelvic venography was introduced into clinical practice in 1946-1950. de la Pena, Amselem, Guilhem et Baux, etc. Her technique was based on the classic venographic studies of the anatomist Batson, published in 1940. Batson showed that contrast fluid, when injected into the deep dorsal vein of the penis, quickly and easily performs venous pelvic plexuses.
The first published work on the clinical use of pelvic venography belongs to Estella (1947). In the domestic literature, the first report on pelvic venography was made in 1960 by G. I. Mgaloblishvili, who presented an analysis of pelvic phlebograms performed in the urological clinic of the II Moscow Medical Institute. To date, 212 intraosseous phlebographies of the pelvis have been performed in this clinic. Over the last decade, pelvic venography has found frequent use not only in urological, but also in gynecological practice, especially for recognizing tumors of the bladder and internal genitalia (G. I. Mgaloblishvili, 1960, 1963; Oliver, 1951; Zeman, 1955; Kucera, 1956 , 1957; Fischer, Dalali, 1954; Diaz Bruzual, 1961; L. A. Rozneritsa, 1963; I. M. Gryaznova et al., 1964).
The main routes of administration of radiopaque fluid for pelvic venography are intravenous and intraosseous. Intravenous tracts include the femoral veins, the deep and superficial dorsal veins of the penis or clitoris, and the venous vessels of the corpora cavernosa of the penis. The intraosseous tracts include the bone marrow veins of the pelvic bones (pubic, ischial, iliac and sacral) and the trochanters of the femur. Since when injecting contrast fluid into the superficial dorsal vein of the penis, it is not possible to sufficiently fill the venous plexuses of the pelvis, including the venous plexuses around the bladder, it is preferable to inject the contrast agent into the deep dorsal vein of the penis.
Before performing phlebography, it is necessary to test the patient’s sensitivity to iodine preparations in order to avoid a possible allergic reaction (on the eve of the study, 1 ml of a radiopaque contrast agent, the same one intended for phlebography, is injected intravenously).
Injection of contrast fluid into the deep dorsal vein of the penis . Once the bladder is filled with 200 ml of oxygen, a small incision of skin and tissue is made under local novocaine anesthesia in the middle of the dorsal surface of the penis, approximately 1.5-2 cm from the root. Having found v. dorsalis penis profundae, first 10 ml of a 0.5% novocaine solution is injected into it, and then 20 ml of 50-70% triiotrast or cardiotrust. The first image is taken at the moment of administration of the contrast agent, the second immediately after its administration, the third after 3-5 seconds, the fourth after 10 seconds.
Injection of contrast fluid into the corpora cavernosa of the penis - cavernosography . Under local novocaine anesthesia, the corpora cavernosa of the penis are punctured and a physiological solution of table salt is slowly injected into them. If the saline solution passes freely into the corpora cavernosa, then 15-20 ml of a 50% solution of a triatomic radiopaque substance is injected through the same needle, at the end of the infusion of which three radiographs are taken.
This method of pelvic venography for recognizing diseases of the pelvic veins is used very rarely. It is used primarily to clarify the localization of areas of fibroplastic induration of the penis (Hirtl, 1962), as well as before plastic surgery on the penis for the so-called fracture of the penis, its injuries.
Injection of contrast fluid into the bone marrow of the horizontal branch of the pubic bones . Over the past 7 years, we have exclusively used this method, since it is the best for recognizing blastomatous lesions of the bladder, prostate and main veins of the pelvis. Many urologists and surgeons share the same opinion (Salzman, Weise, 1960; Diaz Bruzual, 1961; Olsson, 1962, etc.).
Once the bladder is filled with oxygen (200 ml), a Dufaux needle with a mandrin using a hammer is injected into both pubic bones under local novocaine anesthesia, or a needle is inserted using a Kirschner drill. After removing the mandrin, a little blood is sucked out of the bone marrow with a syringe, which serves as proof that the needle is in the bone marrow. First, a 0.25% solution of novocaine with heparin is injected into the bone marrow, and then a contrast agent. For pelvic venography, it is most advisable to puncture the bone marrow of the pubic bones using a special apparatus - a pulse solenoid (G. I. Mgaloblishvili, L. P. Panin and G. I. Karvatsky, 1960). The advantage of this device is that the needles are painlessly and instantly inserted into the bone to the required depth.
Stepping 2 cm outward from the middle of the symphysis, feel the most protruding part of the pubic bone on each side and in this area anesthetize the skin, tissue and periosteum with a 0.25% solution of novocaine. Then, in a strictly perpendicular direction, using the above-mentioned pulse solenoid, needles containing side holes are inserted to a depth of 2.5-3 cm. Having established by aspiration the presence of blood in the syringe, which indicates that the needles are in the spongy substance, they are inserted slowly into the syringe. bone marrow on each side, 15 ml of 0.5% novocaine solution, and then 10 ml of heparin solution (1:1000). This prevents blood clotting and vasospasm. Then, 15 ml of 70% triyotrast or cardiotrust is quickly injected into the pubic bones on each side and images are taken. During the administration of the contrast agent, the patient is asked to take 2 deep breaths and, after inhaling, hold his breath and strain. This increases the pressure in the inferior vena cava system and facilitates the penetration of the radiopaque solution into the venous plexuses of the pelvis.
The first image is taken immediately after the contrast agent is introduced into the spongy substance of the pubic bones, the second - after one second, and the third - after 3 seconds. If it is necessary to have an excretory urogram, then a picture is taken 5 minutes after intraosseous administration of a contrast agent, and if a descending cystogram is necessary, a picture is taken 15-20 minutes later. After removing the needles, place a bag of ice on the area of the pubic bones for 2 hours.
The advantage of the intraosseous phlebography method over the intravenous method is as follows:
- thanks to the bilateral injection of a contrast agent into the pubic bones, it is possible to obtain a more intense and uniform filling of the venous plexuses of the pelvis and, therefore, a significantly better image of them;
- the intraosseous method is technically simple and, therefore, more accessible;
- there are no complications with it.
In addition, in women, the intraosseous phlebography method is almost the only one, except for the possibility of introducing a contrast agent into the cavernous bodies of the clitoris.
Indications for pelvic venography . Phlebography is performed to determine the degree of growth of the bladder by a malignant tumor, as well as its infiltration of the peri-vesical tissue and neighboring organs. This is necessary to resolve the issue of the possibility of performing a particular operation, for example, extended resection of the bladder with ureterocystoneostomy, cystectomy (G. I. Mgaloblishvili, 1960; Guilhem et Baux, 1954; Zeman, 1955; Garlsson et al. 1961). The same applies to prostate cancer. Thanks to phlebography, it is possible to determine the presence or absence of metastatic lymph nodes in the area of large venous vessels of the pelvis, as well as to identify the recurrence of a malignant tumor of the bladder and its spread. Phlebography makes it possible to establish the cause of venous stasis in the pelvic region and lower extremities, to recognize a blood clot, its location and extent in the large pelvic veins (Kahr, 1953; Salzman and Weise, 1960; Diaz Bruzual, 1961)
On venograms, especially those performed by the intraosseous method, it is possible to obtain a good image of the visceral and parietal veins of the pelvis: the obturator venous plexus, the system of suprapubic and retropubic veins, the veins of the Santorini plexus, the main trunks of the hypogastric veins, the common iliac veins, the lower segment of the vena cava, the system of sacral veins, iliolumbar vein. In addition, it is sometimes possible to obtain an X-ray image of the internal pudendal veins, sciatic and gluteal veins, as well as the proximal segments of the femoral veins.
When interpreting pelvic venograms depending on the route of administration of the radiocontrast agent, it is necessary to take into account:
- degree and shape of the plexus vesico-prostaticus image;
- venous drainage from this plexus through the lateral veins of the pelvis;
- filling of the transverse presacral veins and main veins of the pelvis, retrograde outflow through the system of the femoral and gluteal veins.
With pelvic intraosseous phlebography, the contrast agent from the very beginning performs the venous obturator plexus, the cystic plexus (plexus Santorini) with the veins surrounding the neck of the bladder and being in connection with the plexus prostaticus and plexus pudendalis, which drain blood into the internal iliac veins. As a result of filling the bladder with oxygen, a good expansion of the veins of the paravesical venous plexus is achieved. When comparing the right half of the pelvic venous vessels with the left half, a more complex venous outflow on the left side is revealed. On the right, the venous outflow is simpler; in addition to filling with contrast fluid vv. obturatoria, hypogastrica, plexus Santorini, v. iliaca ext., v. cava inferioris, sometimes an image of the presacral veins is revealed on the radiograph. On the left, in addition to the similar veins just listed, presacral anastomoses are filled with contrast fluid, functioning from left to right. This circumstance is important in the diagnosis of vein thrombosis and in recognizing advanced cancerous infiltration of the bladder walls.
In Fig. 76, 77, 78, 79 show normal pelvic venograms with various types of radiocontrast agent administration.
Rice. 76. Pelvic venogram. Normal architecture of the pelvic veins. A contrast agent is injected into the deep dorsal vein of the penis (shown by an arrow).
Rice. 77. Normal pelvic venogram. A contrast agent of 60 ml was injected into both pubic bones.
1 - plexus Santorini; 2 - v. obturatoria; 3 - v. hypogastrica; 4 - v. iliaca externa;
5 - v. iliaca communis.
Rice. 78. Normal pelvic venogram. A contrast agent in an amount of 60 ml was injected into both ischial tuberosities. 1 - plexus Santormi; 2 - v. obturatoria; h - v. iliaca communis.
Rice. 79. Normal pelvic venogram. A contrast agent in an amount of 30 ml was injected into the corpus cavernosum of the penis.
7 - v. obturatoria; 2 - v. hypogastrica; 3 - v. iliaca externa; 4 - v, iliaca communis;
5 - plexus presacralis.
It should be noted that even normally, it is often not possible to obtain a clear image of such visceral plexuses of the pelvis as the posterior vesical and sacral on venograms. But you always get a clear image of the Santorini plexus, especially its anterior section, and the parietal plexuses of the pelvis.
On phlebograms in the case of a bladder tumor infiltrating its walls, it is possible to see weak filling of the venous network corresponding to the tumor area, compression of the veins and the development of a small venous network around the tumor. When comparing one side to the other, a significantly pronounced asymmetry of venous architectonics is revealed. However, phlebography is not able to reveal the degree of germination of the bladder by the tumor when it is localized on the anterior wall and in the area of the apex of the bladder.
As is known, the greatest difficulties in establishing indications for radical surgical treatment for malignant neoplasms of the bladder occur in cases where the tumor is located at the bottom of the bladder, in the area of the ureteral orifices, involving them in the blastomatous process. In such difficult cases, pelvic venography helps solve this problem, and this is its great advantage over other x-ray diagnostic methods. Pelvic venography may also be useful when prescribing radiation therapy to patients with cancer of the bladder and other pelvic organs in cases where it is necessary to determine the exact location of the lymph nodes affected by local stasis.
To study the relationship between the lymphatic and venous vascular systems of the pelvis and inguinal areas, Battezzati, Belardi, Donini and Becchi (1963) proposed combined lymphophlebography using the following method. 8-10 ml of an oily radiopaque substance is injected into the lymphatic collectors of the foot and dorsum of the penis. The injection is performed under pressure at a rate of 0.3 ml per minute. By the end of the injection, 2 x-rays of the pelvis are taken in direct and oblique projections. Then they begin pelvic phlebography: under local novocaine anesthesia, a water-soluble contrast agent in an amount of 15-20 ml is injected through a needle inserted into the pubic bone 1 cm below the upper edge and 1 cm lateral to the symphysis for 10-15 seconds. Towards the end of the injection, 2 pictures are taken within 15 seconds.
Previous14Next
Date added: 2016-07-11; views: 2423; ORDER A WORK WRITING