General information
In cardiology, the term myocardial dystrophy (myocardial dystrophy) combines a group of non-degenerative and non-inflammatory lesions of the myocardial cardiac muscle.
The code for myocardial dystrophy according to ICD-10 is I42.8 Other cardiomyopathies (dishormonal refers to I42.9 Cardiomyopathy, unspecified). The pathology is characterized by significant changes in metabolic processes and a pronounced decrease in the contractile function of the myocardium. Cardiac dystrophy is always a secondary process that combines electrolyte, dysmetabolic, neurohumoral, enzymatic and autonomic disorders. Dystrophy of the left ventricle of the heart is characterized by changes both in the myocytes themselves and in the structures of the conduction system of the heart, which leads to disturbances in the basic functions of the myocardium:
- excitability;
- conductivity;
- automatism;
- contractility.
Dystrophic degeneration of the myocardium, especially at the initial stage, is usually reversible, which greatly distinguishes it from the degeneration that occurs with cardiac amyloidosis and hemochromatosis .
Why does atrophy occur?
Atrophy of the ventricle of the heart, what it is, is not known to everyone.
The left ventricle, which has a cone shape, with walls three times thicker than the walls of the right ventricle, is one of the four chambers of the heart. It begins a large circle of blood circulation, and, accordingly, nutrition of the whole body. As statistics indicate, the mortality rate for left ventricular hypertrophy is about 4%. Let's consider the features of this disease.
Hypertrophy provokes a significant thickening of the wall of the left ventricle, and this thickening does not occur due to the characteristics of the internal space, which does not undergo changes.
Quite often, hypertrophy leads to modification of the septum located between the right and left ventricles. Due to the ongoing hypertrophic changes, the wall loses elasticity, while its thickening can occur both uniformly and in specific areas of localization.
All these features directly affect the course of the disease.
What is noteworthy is that left ventricular hypertrophy is often observed among young people, and often in itself it is not even a disease, nor is it a diagnosis, representing only one of the possible symptoms of any type of heart disease.
As we have already noted, left ventricular hypertrophy can develop due to hypertension. In addition, predisposing factors include various types of heart defects, frequent and significant stress.
Pathogenesis
metabolites accumulate . As a result of changes in biochemical processes in the myocardium, the contractility of muscle fibers is disrupted, heart failure arrhythmias develop .
Myocytes are able to fully recover after eliminating the influence of negative factors. However, too long an exposure can lead to partial death of cardiomyocytes, which are subsequently replaced by connective tissue. cardiosclerosis is formed .
Post-rehabilitation period
A proper post-rehabilitation period can stop the dystrophic changes that start in the body with the development of diffuse myocardial dystrophy. You can also strengthen the body and carry out high-quality prevention. When diagnosing myocardial dystrophy, you must adhere to the following rules:
- resort and sanatorium treatment with balneotherapy and physiotherapy;
- treatment of pathologies that affect the thyroid gland;
- normalization of metabolism;
- taking vitamins and minerals that are necessary for normal heart function;
- long and leisurely walks in the fresh air;
- conducting routine ultrasound and ECG for early detection of disease progress;
- mandatory treatment of the underlying disease that led to myocardial dystrophy, especially for ischemic heart disease, which leads to the development of ischemic dystrophy.
Classification
Pathological changes in the heart are classified according to the causes of their occurrence, which will be listed below in the appropriate section, by stages and by the speed of development.
By stages
- Compensation stage . At this stage, all changes are reversible. Gradually, foci of dystrophy form in the heart muscle, which are noticeable at the microscopic level. Symptoms are minimal or completely absent.
- Subcompensation stage . All changes in cardiomyocytes are still reversible. Confluent foci of dystrophy are formed. All changes are visible at the macroscopic level, the chambers of the heart begin to enlarge. Symptoms are increasing.
- Stage of decompensation . The changes become irreversible. necrosis occurs with their gradual replacement by connective tissue, which is unable to perform the normal functions of cardiomyocytes. The structure of the heart changes, symptoms increase sharply, and the patient’s condition worsens significantly.
Classification by speed of development
- Acute form . It occurs abruptly against the background of intense exposure to negative factors ( pulmonary embolism , severe physical overexertion, complicated hypertensive crisis ).
- Chronic form . It is formed under prolonged exposure to internal and external factors of moderate strength (frequent acute infections, chronic intoxication).
Causes of atrophic changes in the heart
All the reasons why cardiac muscle dystrophy can develop can be divided into two categories - congenital and acquired. A direct change in the cellular structure of heart cells is observed in congenital cardiomyopathies, the origin of which has not yet been sufficiently studied.
There are also a number of pathological processes underlying the development of myocardial dystrophy, which arise in the process after birth. These include:
- Intoxication. Occurs as a result of acute or chronic poisoning of the body with tobacco, alcohol, drugs, medications, poor-quality food products, industrial substances and other toxic compounds that enter the body.
- Infection. Often, atrophy of the heart muscle occurs against the background of an acute viral (influenza, Coxsackie virus) or chronic infection. Especially often, heart complications result from constant inflammatory processes in the nasopharynx.
- IBS. It occurs as a result of chronic myocardial ischemia against the background of severe coronary atherosclerosis.
- Excessive overload (in athletes and people with physical labor). Appears as a result of constantly increased load on the heart, which it cannot cope with. This is expressed in impaired oxygen metabolism, including in cardiomyocytes.
- Deviations in the functioning of endocrine organs (thyrotoxicosis, hypothyroidism).
- Chronic anemia, vitamin deficiency, starvation.
- Metabolic disorders and obesity.
- Physical inactivity.
- Pathological processes in the liver and kidneys.
- Psychosomatic abnormalities.
- Disorders of the digestive system (liver cirrhosis, hepatitis, pancreatitis).
Causes
Myocardial dystrophy can develop under the influence of a variety of internal and external factors that disrupt the flow of metabolic and energy processes in the heart muscle.
Degenerative changes can form under the influence of acute and chronic exogenous intoxications (drug, industrial, alcohol), various physical agents (overheating, vibration, radiation).
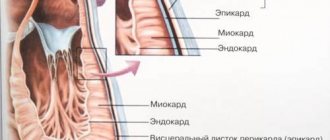
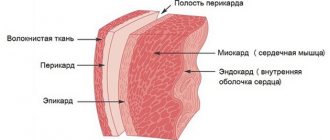
The structure of the myocardium
Quite often, changes in the heart muscle are formed as a result of:
- metabolic and endocrine disorders (pathological menopause, Itsenko-Cushing syndrome , vitamin deficiency , obesity , diabetes mellitus , hyperparathyroidism , hypothyroidism , thyrotoxicosis );
- infections (chronic tonsillitis );
- systemic diseases (neuromuscular dystrophy, collagenosis);
- diseases of the digestive tract ( pancreatitis , cirrhotic liver disease , malabsorption syndrome ).
In newborns and young children, myocardial dystrophy can develop as a result of intrauterine infection , perinatal encephalopathy , and cardiovascular maladaptation syndrome due to hypoxia .
Pathological changes in the heart can also be observed in athletes, which is associated with excessive physical overload ( pathological athletic heart ).
Dishormonal myocardial dystrophy
It is diagnosed mainly in women aged 45-50 years. Occurs as a result of disturbances in the estrogenic functions of the ovaries. Dyshormonal cardiodystrophy occurs extremely rarely in men aged 50-55 years as a result of disturbances in the production of the hormone testosterone .
Main complaints:
- pain in the heart area during hot flashes;
- sensations of heat in the chest;
- increased sweating;
- feeling of rapid heartbeat.
If the patient has concomitant hypertension , heart failure may develop as a complication.
The dyshormonal form of myocardial dystrophy also includes changes in the heart muscle caused by disturbances in the functioning of the thyroid gland.
Cross-section of the heart with myocardial dystrophy
With thyrotoxicosis (hyperfunction of the thyroid gland), metabolism accelerates, which leads to weight loss, rhythm disturbances, insomnia , thirst, increased excitability of the nervous system and excessive nervousness.
With hypothyroidism, metabolism slows down. Patients complain of low blood pressure , swelling, a feeling of chilliness, and aching chest pain.
Fatty degeneration of the myocardium
With severe metabolic disorders, fats begin to be deposited in the heart muscle, completely replacing the cytoplasm of cardiomyocytes over time. Fatty degeneration of the myocardium leads to a significant decrease in the contractility of the heart.
Patients complain of severe shortness of breath and aching pain in the area where the heart is located. In more advanced cases, swelling of the lower extremities occurs. Such patients are primarily indicated for lifestyle correction in parallel with drug therapy.
Dysmetabolic myocardial dystrophy
What is dysmetabolic myocardial dystrophy and when does it develop?
This pathology is observed in patients suffering from diabetes. It occurs as a result of metabolic disorders, which leads to damage to the coronary arteries . Patients complain of chest pain, simulating angina . The pain is not relieved by Nitroglycerin and is less intense.
Myocardial dystrophy of mixed origin
Several factors contribute to the development of this pathology.
What is it and how does it manifest itself? Most often, mixed myocardial dystrophy is observed in children suffering from chronic anemia . In young patients, neuroendocrine myocardial dystrophy develops, and electrolyte metabolism changes. A similar disease can also occur in adults. The very first diagnostic signs on the ECG are dysfunction of contraction (especially in the left ventricle). In the absence of adequate timely therapy, the negative effect on the heart is aggravated, disturbances begin to be registered in relation to automaticity, excitability and conductivity of the heart. And as a complication, the patient develops an acute hemodynamically significant pathological disease.
Myocardial dystrophy of complex origin
This variant is characterized by a more severe course. The disease is provoked by a systematic disturbance in the metabolism of organs and tissues, which leads to systemic changes. The first symptoms of the disease are nonspecific, which makes early diagnosis difficult. In more advanced cases, patients complain of respiratory disorders, arrhythmias, and increases in blood pressure.
Alcoholic cardiac dystrophy
It is generally accepted that this form develops with systematic, daily consumption of alcohol for 10 years. However, with a hereditary deficiency of specific enzymes that are responsible for processing ethanol, the disease can develop within 3 years. Most often, males aged 25-55 years are affected.
Myocardial dystrophy with anemia
When hemoglobin decreases below the level of 90-80 g/l, hemic hypoxia , which is accompanied by an energy deficiency in the heart muscle. The disease develops against the background of chronic blood loss, hemolytic and iron deficiency anemia, and DIC syndrome .
The mechanism of pathology development
Myocardial dystrophy is caused by a variety of reasons. Therefore, the process itself progresses or originates in different ways.
In any case, the basis of the disease is a violation of metabolic processes in the cardiac structures.
The approximate development scheme includes three stages:
- The emergence of a primary, provoking factor. This could be due to endocrine deviation, intoxication, or other issues.
- Impact on the muscle layer of the organ. The normal supply of oxygen and nutritional compounds is blocked. Trophy at the local level drops significantly.
- “Consolidation” of the result. There is a chronic deficiency of necessary substances and stabilization of dystrophic phenomena (thinning of the muscle layer of the myocardium).
The process can develop over a week, month or years. Depends on the aggressiveness of the pathology.
Destruction occurs gradually, not in one second. Typically, from the moment the first symptoms appear until a clear clinical picture emerges, it takes from 6 to 24 months. This gives hope for high-quality diagnosis and comprehensive treatment.
Symptoms of myocardial dystrophy
The symptoms of myocardial dystrophy directly depend on its stage. In the early stages of development, cardiac complaints may be absent. Patients experience decreased performance, rapid fatigue, and poor tolerance to habitual physical activity.
Later, as the disease progresses, patients begin to complain of prolonged, aching pain in the heart area that is not associated with physical activity and does not stop after taking Nitroglycerin . But at the same time, emotional and physical stress can provoke chest pain in such patients, but after a certain time. Most often the pain is causeless.
Often there is a feeling of rapid heartbeat, a feeling of lack of air, and shortness of breath. At later stages, swelling appears in the lower extremities, arrhythmias , and shortness of breath appears at rest. During an objective examination, you can hear a weakening of the first sound above the apex of the heart, tachycardia and a short systolic murmur.
Clinical symptoms largely depend on the cause that led to changes in the heart. With menopausal pathology, patients complain of a feeling of heat, frequent “hot flashes”, excessive sweating, and a feeling of paresthesia in the extremities. With thyrotoxicosis , rhythm and conduction disturbances develop quite quickly, and with anemia , the symptoms of heart valve defects are simulated (a pathological systolic murmur appears, characteristic of insufficiency of one of the valves: aortic, tricuspid or mitral).
What is pathology
Atrophy of the ventricle of the heart, what it is, is not known to everyone. The left ventricle, which has a cone shape, with walls three times thicker than the walls of the right ventricle, is one of the four chambers of the heart. It begins a large circle of blood circulation, and, accordingly, nutrition of the whole body.
Under the influence of certain factors, hypertrophy of the muscles of the organ occurs: thickening of the walls, loss of elasticity of the septum between the right and left ventricles, which leads to atrophy of the organ. The development mechanism is as follows. More blood begins to flow into the cavity of the left ventricle of the heart. Muscles overcome more resistance. Overload begins due to the resulting pressure and volume. Response to overload: lengthening, increasing muscle mass, increasing the total mass of the myocardium.
As muscles increase, they become denser and their need for oxygen increases. But the body is no longer able to provide the organ with the required volume. Oxygen starvation develops, further modification of the structure.
Types of atrophy
The disease has several types, regardless of the reasons for its development:
- Fat atrophy. Occurs against the background of lipid metabolism disorders, hypoxia, cardiovascular pathologies, alcohol intoxication or blood diseases.
- Dishormonal. When the hormonal system malfunctions. Often develops during menopause.
- Ischemic. Result of the coronary crisis. The condition is dangerous and provokes heart failure.
- Diffuse. Appears against the background of frequent inflammatory processes.
- Grainy. Provoking atrophy is a disorder of protein metabolism.
Left ventricular atrophy is a common occurrence in people who play sports professionally. Systematic physical activity and unbalanced nutrition lead to muscle wasting.
Causes of atrophy
Pathology develops for the following reasons:
- abnormalities of heart development;
- heredity;
- food and industrial poisoning;
- excessive physical activity;
- metabolic disease;
- anemia (low hemoglobin content in the blood);
- thyroid diseases;
- avitaminosis;
- myopathy (chronic progressive hereditary muscle disease associated with metabolic disorders in muscle tissue);
- stressful conditions;
- malnutrition (diet, fasting with lack of normal amount of protein food);
- obesity;
- alcohol abuse;
- cardiosclerosis (characterized by oxygen starvation of tissues, metabolic disorders).
- high blood pressure;
- hypertrophic cardiomyopathy (a hereditary disease in which the myocardium thickens);
- mitral valve stenosis (a disease characterized by narrowing of the left atrioventricular valve);
- aortic stenosis (during the disease, the passage of the aorta narrows, preventing the free flow of blood);
- pathologies of the respiratory system: lead to impaired lung function;
- cardiac ischemia;
- hypertension in late stages.
All of the above factors cause changes in the muscles of the left ventricle, which, in turn, causes organ dysfunction. Left ventricular atrophy is a dangerous disease that can result in death if not treated promptly.
Tests and diagnostics
In the anamnesis, patients with myocardial dystrophy reveal various pathological conditions and diseases, which are manifested by disturbances in metabolic processes and tissue hypoxic syndrome. Objectively, when examining the heart, you can hear a weak systolic murmur, a weakening of the first sound at the apex of the heart, muffled heart sounds and irregular rhythm.
The electrocardiogram records nonspecific changes in the myocardium, disturbances in repolarization processes, arrhythmias, and signs of decreased myocardial contractile function.
Drug and stress tests give a negative result (coronary artery disease is excluded).
When performing phonocardiography , the ratio of the duration of electrical and mechanical systole changes.
Echocardiography confirms the expansion of the cavities of the heart, changes in the structures of the heart muscle are recorded. In this case, no organic pathology is observed.
If chest x-ray a myopathic configuration of the heart , then this indicates deep damage to the myocardium.
Using scintigraphy, you can assess the perfusion and metabolism of the heart muscle, detect diffuse/focal changes, which will indicate a decrease in the number of normally functioning cardiomyocytes.
In extremely doubtful cases, they resort to myocardial biopsy , when all non-invasive studies performed have not yielded any result. Differential diagnosis is carried out with such diseases as:
- myocarditis;
- IHD;
- cor pulmonale;
- cardiosclerosis;
- heart defects.
UAC indicators are usually normal.
Briefly about the structure of the myocardium
The myocardium is the middle (muscular) layer of the heart and consists of specific cells - cardiomyocytes. It also contains fibers of the conduction system that generate impulses for contraction of the organ. Among them:
- sinoatrial node (Kisa-Fleck);
- atrioventricular node (Aschoff-Tavara);
- right and left bundle branches;
- Purkinje fibers.
The myocardium of the ventricles and atria is separated from each other, due to which they are able to contract unsynchronously. The muscular layer of the ventricles is more developed and can reach 11 mm for the left and 5 mm for the right. This is due to the fact that they do more work. The thickness of the walls of the atria ranges from 2 to 3 mm.
Myocardial functions
- contractility, due to which blood is distributed throughout the body;
- excitability - the ability to contract in response to internal or external stimuli;
- conduction of an impulse through the fibers of the conductive system;
- automatism - the ability to relax and contract independently without external stimulation.
For muscle cells to contract, the following conditions are necessary:
- mitochondria must produce sufficient energy;
- cardiomyocytes, with a normally functioning conduction system, are required to capture the nerve impulse;
- Sufficient potassium levels must be maintained.
With myocardial dystrophy, the contraction process is noticeably disrupted, which leads to poor circulation, and all organs and tissues of the body do not receive the necessary nutrients and oxygen.
Treatment of myocardial dystrophy with folk remedies
Traditional methods of treatment can only be an addition to the main therapy, but not replace it.
Rosehip flower tincture
The prepared solution helps to normalize cardiac activity, even out heart rhythm during arrhythmia, and replenish the lack of vitamin C.
Pour two cups of boiling water over 2 tablespoons of rosehip flowers and let it brew for an hour. The prepared infusion should be taken before meals, 1 tablespoon.
Lemon harvest
Citrus collection will help normalize heart function and strengthen the heart muscle. To prepare a thick paste, you need to grind 150 grams of fresh figs and 250 grams of lemon in a meat grinder. Then add 50 grams of vodka and 100 grams of liquid bee honey to the resulting consistency. Lemon infusion should be taken three times a day, 1 teaspoon.
Honey-beet tincture
To improve blood circulation in the heart muscle and get rid of tachycardia, honey-beetroot tincture is recommended. Additionally, the solution has a sedative effect.
To prepare, stir 1 teaspoon of bee bread in 100 ml of a mixture of beetroot juice and honey (50/50). Let sit in the refrigerator for 3 hours. The resulting infusion should be taken three times a day, 3 tablespoons.
Folk remedy for shortness of breath
A frequent companion to myocardial dystrophy is shortness of breath . Breathing practices help combat it. Additionally, you can use proven traditional methods.
Squeeze the juice out of 10 whole heads of garlic and 10 lemons, and mix the resulting solution with 1 liter of bee honey. Place the finished mixture in a container, seal it tightly, and place it in a cool, dark place for 7 days. You need to take 4 teaspoons of the mixture daily for two months. The mixture should not be swallowed immediately; try to dissolve it slowly.
Vitamin cocktail
One of the primary tasks in the treatment of heart pathology is the general strengthening of the body and acceleration of metabolism. A healthy vitamin cocktail will solve these two problems at once.
Mix the juice of 1 grapefruit, 2 kiwis and 4 oranges. Pour a glass of rose hips into a liter of water and cook for 20 minutes. Let cool, then strain with cheesecloth and add to the berry mix. Additionally, grate the ginger root and add 1 teaspoon of honey to the resulting mixture.
Healing herbal tea
The presented recipe will allow you to prepare a collection that has a positive effect on the functioning of the cardiovascular and endocrine systems.
You'll need:
- 2 tbsp. spoons of oregano and valerian;
- 1.5 tbsp. spoons of adonis flowers and mint leaves;
- 1 tbsp. a spoonful of motherwort herb, juniper and dill fruits.
Pour boiling water over everything at the rate of 1 tbsp. spoon of herbal mixture per 1 liter of water. Bring the infusion to a boil and let it sit for 24 hours. You need to take the resulting solution before meals, 100 g.
Prevention
Lifestyle is of great importance in the prevention of myocardial dystrophy. Almost all preventive measures are aimed at correcting an existing lifestyle.
It is recommended to stop drinking alcoholic beverages and smoking. It is necessary to promptly treat all identified pathological changes in the heart muscle and various infectious diseases.
It is important to monitor the correct functioning of the endocrine system. obese people - dietary. Weight correction is important.
It is better to avoid excessive physical activity so as not to force the heart once again. When playing sports, you must take into account your physical fitness. Don't forget about warming up, which allows you to balance physical activity. Try to refuse to work in hazardous industries - health is more valuable than any money.
Main aspects of the prevention of myocardial dystrophy
- sanitation of foci of infection;
- complete, healthy, balanced diet;
- timely maintenance drug therapy (if cardiac pathology is detected, especially with dystrophic changes in the myocardium).
Diagnostic approaches
Diagnosis of cardiac pathologies is varied. A patient examination always begins with a visual examination of the patient and an analysis of his complaints. During the examination, the doctor performs percussion (tapping with fingers) and auscultation (listening with a phonendoscope). Percussion allows you to determine the boundaries of the heart muscle, which expand during myocardial dystrophy. However, the percussion method cannot be called indicative in comparison with more modern diagnostic methods - ECHO-CG, MRI and others.
Auscultation helps to identify the presence of a heart murmur, muffled first tone, and disturbed rhythm.
The basis of any cardiac examination is always the ECG. This is an accessible and very informative diagnostic method, which allows not only to identify pathologies in the functioning of the heart, but also to determine the further scenario for examining the patient.
Chest X-ray, MRI, stress tests are prescribed by a cardiologist to clarify the diagnosis after an ECG.
Additionally, laboratory tests are carried out, in particular, a biochemical blood test, tests for thyroid hormones, and a general blood test are important.
Other complex diagnostic procedures - scintigraphy, coronary angiography, ultrasound of the heart are prescribed strictly individually, after a recommendation from a cardiologist is given for this.
In children
In children, myocardial dystrophy can develop as a result of hypervitaminosis , rickets , chronic dietary disorders, bacterial and viral infections. Often this pathology is observed at an early age due to lack of physical activity, or, on the contrary, due to excessive force overload.
In pediatric practice, myocardial dystrophies that developed as a result of drug poisoning were observed.
Most often, the cause of the disease is vegetative, nervous and endocrine disorders.
The main symptoms in children consist of:
- asthenia;
- shortness of breath with minimal physical activity;
- weakening the sonority of heart sounds.
Anatomical and functional features of the heart
The heart is one of the vital organs that performs the function of blood supply to the body. It has 4 cameras, which are presented as:
- right atrium;
- right ventricle;
- left atrium;
- left ventricle.
Due to their alternate contraction, blood is able to move through the blood vessels according to two circles of blood circulation (small and large). If we talk about numbers, then the average number of contractions of the heart muscle per minute reaches 70 beats, and the total average daily number is 100,000.
During pregnancy
The most common myocardial disease in pregnant women is myocardial dystrophy.
Gynecologists quite often have to deal with this diagnosis in everyday practice, although it is not always justified. If we move away from all cases where myocardial dystrophy borders on other organic heart diseases ( valvular defects , myocarditis , etc.), then only those pathological changes that occur with anemia, vitamin deficiency, intoxication, overwork can be attributed to cardiac muscle dystrophy. pregnant women.
For pregnant women who suffer from myocardial dystrophy, according to the Institute of Obstetrics and Gynecology of the Academy of Medical Sciences, the following are typical: the addition of late toxicosis (35%), premature rupture of water (28%), weakness of labor (12%), perinatal mortality (6%).
Therapy for pregnant women with myocardial dystrophy consists of eliminating the underlying disease that caused this pathology, compensating for cardiac activity and eliminating pregnancy complications. Termination of pregnancy is not necessary in most cases.
Treatment of myocardial atrophy
Today, the main treatment strategy for atrophic changes in the myocardium is to prevent its further progression. Unfortunately, as practice has shown, there are currently no effective drugs that can restore myocardial cells. Trimetazidine (preductal) did not live up to the hopes placed on it. The effectiveness of mesidol and riboxia has not yet been proven. And according to a number of notes in the official medical literature, it can be considered controversial
Therefore, now all therapy comes down not to treating the disease muscle atrophy, but to correcting its consequences. The first known drugs that significantly stop the processes of dystrophy and subsequent atrophy of cardiomyocytes are diuretics and beta blockers. They have been successfully used for more than 50 years in different countries of the world. Currently used ACE inhibitors are able to stop the atrophy process only in a number of patients. Sartans and calcium blockers have been used quite successfully over the last decade. But this period is not enough to decide which treatment for heart muscle atrophy is most appropriate at a particular stage.
Diet for myocardial dystrophy
Diet for heart failure
- Efficacy: therapeutic effect after 20 days
- Timing: constantly
- Cost of products: 1700-1800 rubles. in Week
Diet for vegetative-vascular dystonia (VSD)
- Efficacy: Healing effect
- Timing: constantly
- Cost of products: 1500-1600 rubles per week
Basic rules in nutrition:
- restriction in salt consumption (no more than 3 g per day);
- counting calories consumed;
- drinking enough liquid;
- weight control;
- eating foods rich in potassium, magnesium and fiber;
- consumption of multivitamins and fortified foods;
- avoidance of coffee and alcohol-containing products.
Consequences and complications
Dangerous complications and consequences of an untreated disease:
- Chronic heart failure. Manifested by swelling, severe shortness of breath and general weakness. Initially, symptoms appear only during exercise, in more advanced cases - at rest and with minimal physical activity. Without adequate therapy, CHF progresses quite quickly and leads to death.
- Rhythm and conduction disorders . Changes concern the generation and conduction of nerve impulses through the heart muscle. It all can start with rare, seemingly harmless extrasystoles . Further, the disease progresses and affects conduction, provoking sinoatrial and atrioventricular blockades. Atrial fibrillation is often recorded . Patients complain of loss of consciousness, shortness of breath, and a feeling of arrhythmia. Treatment can be medication or emergency surgery (EC implantation).
- With severe hemodynamic disturbances, blood clots , which can travel through the bloodstream to the brain, kidneys, eyes, etc.
Mechanism of hypertrophic changes
The left ventricle, like the muscles of skeletal muscles, trains in response to increasing load, muscle fibers increase in volume.
Initially, the thickened wall provides a more powerful contraction of the left ventricle of the heart, but later the increase in the wall is no longer compensatory, but pathological.
Coronary capillaries cannot supply the enlarged left ventricular wall with oxygen, and some muscle cells are in a state of ischemia. Left ventricular hypertrophy provokes disruption of coronary blood flow and can lead to a heart attack, which is facilitated by hardening of blood vessels.
Due to ischemia, the nutrition of cardiomycetes is destroyed, some of them are replaced by connective tissue. In the thickness of the LV myocardium, the fibrin content increases, which reduces the ability of the myocardium to contract.
Over time, atrophy develops in the left ventricle due to chronic ischemia - a condition in which cardiomycetes are depleted, which leads to a decrease in the thickness of the heart.
In hypertrophied myocardium it is noted:
- decreased force of ventricular compression;
- increasing the duration of contraction;
- dilatation - expansion of the cavity;
- decreased compliance, which impairs ventricular filling;
- a decrease in coronary reserve - the volume of blood that the ventricle is able to additionally push into the bloodstream under load.
Forecast
The prognosis is considered favorable for stages I and II. Heart functions can be fully restored after the cause-and-effect factor is eliminated. The duration of the recovery period is largely influenced by the general condition of the body (the fastest recovery is observed at a young age and in the absence of concomitant pathology), the time of initiation of therapy (the earlier competent treatment is prescribed, the faster the disease regresses). The duration can range from 1 year to several years.
At stage III, the prognosis directly depends on the presence of complications and the severity of already formed changes. When changes in the heart muscle are diagnosed, the emphasis is not on the patient’s well-being and restoration of normal heart parameters, but on reducing the rate of progression of chronic heart failure and restoring the rhythm. In the third stage, lifelong therapy is required. In the absence of adequate treatment, the life prognosis is extremely unfavorable.
Clinical forms
In addition, a number of clinical specialists distinguish forms of myocardial dystrophy depending on the clinical manifestations. Among them:
- cardialgic. Manifested by pain in the chest of an aching, pinching nature, not dependent on physical or emotional stress, taking nitroglycerin or other nitrates, not radiating (not radiating) to the area of the shoulder blade or left arm, passing on its own; chilliness of the upper or lower extremities; rapid fatigue; general weakness; low physical endurance; dizziness;
- arrhythmic. Characteristic: attacks of pre-fainting or fainting, sensations of improper functioning of the heart, a feeling of lack of air, increased heart rate (patients feel them at a frequency of more than 90 per minute), pain in the chest;
- stagnant. It is formed in chronic heart failure and manifests itself in the form of swelling of the legs, feet, thighs, less often of the upper limbs and face, a non-productive cough due to stagnation of blood in the pulmonary circulation; increase in liver size; swelling of the neck veins; hydropericardium or hydrothorax - accumulation of fluid between the layers of the outer membrane of the heart or the pleural membrane of the lungs;
- combined. It occurs most often and is a combination of various forms of the disease.
Myocardial dystrophy has a long, slowly progressive course; decades can pass from the beginning of the first stage to the last.