If, during examination of the patient, signs of insufficient myocardial nutrition are revealed, but there are no symptoms similar to angina pectoris, then a diagnosis of silent ischemia is made. It is accompanied by metabolic disorders, decreased contractile function and electrical activity of the heart muscle. It is found in cases of rhythm disturbances, high blood pressure, as well as in smokers and diabetics.
Features of the pathology
Asymptomatic myocardial ischemia is a fairly common pathology, affecting almost 35% of the entire world population. Painless cardiac ischemia, like angina, can occur due to combinations of a variety of reasons. This can be either stenosis or problems with platelet aggregation.
Important! Each patient with painless ischemia is diagnosed with multiple lesions of the coronary arteries of extremely severe form.
Silent myocardial ischemia is diagnosed in:
- 55% of patients with stable angina;
- 75% of patients with unstable angina;
- 60% of patients with congestive heart failure of ischemic origin;
- 60% of smokers, while for non-smokers this figure is only 35%;
- 30% of patients with diabetes.
Risk groups are divided into those who:
- suffered a myocardial infarction;
- has several risk factors for coronary artery disease, especially with severe episodes of CAD;
- suffers from coronary artery disease and hypertension;
- has diabetes;
- suffers from coronary artery disease and chronic obstructive pulmonary pathology;
- works in risky and stressful jobs, such as drivers, pilots or doctors, etc.
Symptoms
The main sign of silent myocardial ischemia is the absence of pain in the heart. Sometimes it is possible to suspect the presence of a circulatory disorder of the heart muscle based on the following general signs:
- pulse disturbances: increased frequency, decreased frequency, arrhythmia;
- weakness in left arm;
- cyanosis of the skin;
- decreased blood pressure;
- dyspnea;
- heartburn.
When conducting an ECG or Holter ECG for preventive purposes or during examination for another disease, such patients may experience frequent extrasystoles.
Silent ischemia can manifest itself with a variety of symptoms, and experts identify four main variants of the course of this condition.
Option I
This course of painless ischemia of the heart muscle is most often observed. In patients, it occurs against the background of angina pectoris and is detected in approximately 20-40% of patients. Moreover, almost 75% of angina attacks are not accompanied by pain, and the remaining 25% are expressed in cardialgia, characteristic of this disease.
Option II
Patients do not feel the presence of ischemia of the heart muscle or signs of myocardial infarction. They are not bothered by pain in the heart, and often the already occurring myocardial necrosis is revealed in them only after an ECG.
The first signs of myocardial infarction in such patients may be arrhythmias or the onset of sudden coronary death. According to some studies, a similar course of silent ischemia leading to necrosis of the heart muscle is observed in 12.5% of patients.
Option III
In such patients, episodes of myocardial ischemia are asymptomatic, and only when a heart attack occurs do they feel pain in the heart. Such a violation of the blood circulation of the heart muscle can go unnoticed for a long time or is accidentally detected when performing a Holter ECG or stress tests. Experts suggest that this clinical manifestation of ischemia may be associated with an increase in the pain threshold and patients simply do not feel less severe pain in the heart area.
IV option
Painless ischemia occurs infrequently in this form, but recently the number of such cardiologist patients has begun to increase. In them, signs of insufficient blood supply to the heart muscle are revealed only during an in-depth preventive examination using stress tests.
Reasons for development
Silent ischemia can be provoked by tandems of various factors. However, the main ones are:
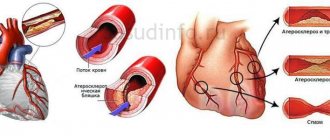
- Coronary stenosis, which most often occurs due to atherosclerosis in the arteries of the heart. It is diagnosed in half of patients with BIM, only the severity varies. It may also be a consequence of systemic vasculitis or cancer.
- Angiospasm of the coronary arteries, which occurs when the production of vasodilating substances by the vessels decreases with an increase in the release of vasoconstrictor substances. More often during stress or heavy physical activity.
- Coronary artery thrombosis, resulting from ulceration of atherosclerotic plaques in the vascular system, blood clots, problems with platelet clotting. With partial occlusion of the vascular lumen, signs of ischemia occur with or without pain, and with complete occlusion, myocardial infarction occurs.
Forms
To assess the condition of patients in BIM, both at the stage of diagnosis and for treatment, cardiologists use the following division of pathology into forms:
- The first, which has an accurate diagnosis, and the patient does not have attacks of pathology. The heart rhythm has no pathologies, like congestive heart failure.
- The second, in which there is no concomitant type of angina, but with a history of myocardial infarction.
- The third, having both angina and vasospasms. In such patients, within 24 hours, both an attack of painful ischemia and a painless one may occur.
Classification of the disease
Experts distinguish 2 main forms of silent ischemia:
A feature of the pathology is that the patient feels healthy. He may not be aware of the problem until complications begin to develop.
In some cases, the disease is accompanied by:
Usually patients do not pay attention to a symptom that manifests itself once!
Meanwhile, the pathology is progressing! It can transform into a new form and clearly manifest itself with attacks of pain.
Complications of the disease include:
heart rhythm disturbances;
chronic heart failure;
In some cases, ischemia causes sudden death. Medical professionals assess the prognosis of pathology without adequate therapy as unfavorable. This is due to the fact that the mortality rate reaches 35%.
Manifestations
The danger of pathology lies in the absolute absence of symptoms. A patient or doctor can identify this phenomenon only if there is diagnosed angina, coronary artery disease and/or myocardial infarction in the medical record or by discovering it by chance. More often this is shown by a planned ECG. In 70% of people after myocardial infarction or with coronary artery disease, 4 attacks of silent ischemia occur for every painful one.
How is it diagnosed?
Diagnosis of pathology is based on instrumental methods that provide clear information about ischemic damage to the heart muscle. The diagnosis of “silent myocardial ischemia” is made based on the results of:
- ECG when the patient is completely calm and relaxed. This technique is simple, accessible, and effective. The device shows changes in the functioning of the heart that are characteristic of coronary artery disease. The downside of the technique is that accurate data can only be obtained if the patient is at rest, because often BMI occurs purely during physical exertion.
- Holter-type ECG monitoring provides more information than the previous method, since it can be used in the patient’s usual activities. It will show not only the episodes of painless ischemia themselves, but also their duration, taking into account any activity and emotional state.
- Bicycle ergometry records ECG and blood pressure with a systematic increase in load. The higher the heart rate, the more oxygen the body needs, and with ischemia, the blood supply is disrupted, which will be recorded by the electrocardiograph.
- Coronary angiography is the main technique for BIM, as it provides information both about the pathology and its connection with the coronary arteries. This helps in determining the nature of the disease, how narrowed the cardiac arteries are and the degree of damage to the vascular bed, which will allow you to select the desired method of therapy.
- Stress echocardiography, which reveals heart problems during stress on the body, showing the asynchrony of myocarditis with other parts of the heart.
- SPECT of the myocardium is an emission-type CT scan, which evaluates the blood supply to the myocardium at the microcirculatory level, how damaged the myocytes are, and whether there are scars.
- PET-CT informs about the depth and area of blood supply pathologies in the myocardium, even at the level of the smallest endothelial functions, which is typical for hidden atherosclerosis.
Also read: What are the signs of angina?
Diagnostic measures
To diagnose this disease, many reliable laboratory and instrumental techniques are used. Most hospitals use a primary medical examination and patient interview, which allows one to suspect ischemic changes in the heart and identify specific symptoms and symptomatic complexes.
When listening to the patient's chest, rhythm and conduction disturbances can be detected, indicating a pathological process occurring in the body.
To confirm the diagnosis, the following laboratory methods are used:
- a general analysis of urine and blood with determination of the number of platelets allows us to judge disorders in the hematopoietic system and bone marrow pathology;
- biochemical analyzes provide information about the main markers of myocardial necrosis: troponins, myoglobin, creatine phosphokinase fraction. You also need to measure the main indicators of the liver and observe them over time;
- A coagulogram and hemostasiogram are used to determine blood clotting time and diagnose disorders in the blood coagulation system.
Of the instrumental methods, electrocardiographic examination of the heart is most widely used. An ECG is taken at the time of an attack, with the participation of stress tests (pharmacological tests, cold and heat tests, stress test, through esophageal stimulation of the ventricles, bicycle ergometry), and 24-hour ECG monitoring, otherwise called Holter, is also very informative.
Myocardial ischemia on the ECG is manifested by ST segment elevation above the isoline.
X-ray examination of the chest in both projections reveals an increase in the size of the ventricles, which indicates a functional overload of certain parts of the heart. You can also see changes in the aorta: this vessel is most susceptible to changes.
On phonocardiography, you can see changes in heart sounds, the appearance of pathological noises, indicating rhythm and conduction disturbances, as well as indicating heart defects.
An echocardiogram of the heart or ultrasound allows you to see the size of the heart cavities, the thickness of the walls, determine the location and nature of the location of necrosis, and pathological changes in the myocardium.
It is a highly sensitive research method that minimizes the risk of making an incorrect diagnosis with these initial data.
Treatment
Therapy is based on a combination of conservative treatment, medication and surgery. The latter is used only in severe cases.
Conservative
The doctor’s first recommendation for such an illness is a complete cessation of physical activity and balancing of the emotional state.
In this case, physical activity should be, the doctor will decide what its level will be. Changes in diet will definitely follow in order to normalize carbohydrate and fat metabolism, which means carbohydrates and animal fats need to be significantly reduced.
At the same time, it is necessary to increase the consumption of dairy products, fish, vegetable and fruit dishes. If obesity is diagnosed, you will need to control your caloric intake to reduce body weight. Complete cessation of smoking and alcohol.
Medication
To prevent disability, doctors use medications to try to maintain myocardial function at the proper level. For this use:
- Beta blockers, which reduce heart rate, help the myocardium better tolerate physical activity and have a pronounced antianginal effect. With them, attacks of any type of ischemia become less frequent, which gives a good prognosis to the patient.
- Calcium antagonists, which lead to normalization of heart rhythm by dilating coronary and peripheral arteries and reducing heart rate. By inhibiting metabolic processes, they increase the heart’s tolerance to any physical activity.
- Nitrates, which make resistance in the coronary arteries less. This leads to stimulation of collateral blood flow with its transfer to the affected areas of the myocardium. The lumen in coronary vessels becomes wider, leading to a cardioprotective effect.
- Nitrate-like vasodilators that stimulate the release of nitric oxide, which dilates blood vessels and arteries. This leads to improved blood supply to the myocardium, but does not treat the cause of the pathology.
- Statins affect atherosclerosis, which often leads to silent ischemia.
- ACE inhibitors with pronounced cardio and vasoprotective properties, bringing the myocardial oxygen demand and its supply into a balanced state.
- Antiplatelet agents that prevent the formation of thrombosis. They are prescribed primarily after myocardial infarction and with an established diagnosis of “painless ischemia” and during a hypertensive crisis.
Surgical
This technique is designed to restore normal or close to normal myocardial function. For this purpose, CABG or stenting of coronary arteries is used.
Which technique the doctor will choose depends on the current condition of the patient, how affected the arteries of the heart are and their extent, whether there are concomitant pathologies, and whether the area of ischemia in the myocardium is large.
After the procedure, the risk of relapse is 30% lower and the risk of death due to pathology is reduced by a quarter.
TRANSIENT MYOCARDIAL ISCHEMIA OR POSTHYPOXIC
CARDIOVASCULAR SYSTEM DYSADAPTATION SYNDROME.
L.V. Simonova, N.P. Kotlukova
Department of Childhood Diseases No. 2 of the Faculty of Pediatrics with a course of gastroenterology and dietetics of the Federal University of Internal Medicine, Russian State Medical University.
Transient myocardial ischemia (posthypoxic syndrome of disadaptation of the cardiovascular system) is a complex of functional, metabolic and hemodynamic disorders that occur in the body of a newborn as a result of perinatal hypoxia, characterized by an increase in the activity of cardiac-specific enzymes, disturbances in the neuro-humoral regulation of cardiac activity and energy metabolic processes , leading to a decrease in myocardial contractility, atrioventricular valve insufficiency, and sometimes to signs of heart failure.
“Transient myocardial ischemia” (TIM) is a pathology characteristic of the period of adaptation of a newborn. Subsequently, in the presence of clinical signs, data from laboratory research methods (increased activity of cardiac-specific enzymes), as well as the results of additional research methods (changes in the ECG, decreased ventricular ejection fraction, insufficiency of atrioventricular valves, etc.), the term “ posthypoxic syndrome of disadaptation of the cardiovascular system" (DM CVS).
IMT, like posthypoxic CVD, is characterized by a benign course and residual manifestations in the form of minimal signs of pulmonary hypertension, the formation of autonomic dysfunction and atrioventricular valve insufficiency.
According to domestic and foreign authors, IMT occurs with a frequency of 40 to 70% of children who have suffered perinatal hypoxia. IMT is associated with a temporary decrease or cessation of blood circulation in certain areas of the heart muscle, leading to a decrease in its functional activity. The duration of such time periods of acute myocardial ischemia according to Prahov A.V. (1996) ranges from 10 to 25 minutes per hour, depending on the severity of hypoxia.
The cardiovascular system of a newborn has anatomical and physiological features, among which the main ones are:
1. Embryonic structure of the myocardium. The cardiac muscle is presented in the form of undifferentiated fibers with weakly expressed transverse striations, which is due to a smaller number of myofibrils. They are dominated by the B-isomer of myosin with low ATPase activity and insufficient function of calcium channels. The connective tissue of the stroma is represented in a larger volume, but it has few elastic fibers, as a result of which the myocardium is less pliable.
2. In a newborn child, 30% of all cardiomyocytes are involved in contraction, while in an adult – 60%.
3. In the mitochondria of cardiomyocytes, the number of which is also reduced, there is a very low content of a vitamin-like substance responsible for the oxidation of free fatty acids - carnitine. Carnitine deficiency is most pronounced in premature newborns, but also occurs in full-term infants in the first days of life. During perinatal hypoxia, the maturation of the endogenous carnitine synthesis system slows down significantly.
4. The predominance of carbohydrate metabolism in the cardiomyocyte is characteristic of all newborns.
5. The right parts of the heart predominate over the left, and the younger the child’s gestational age, the more pronounced this predominance is. The left chambers of the heart begin to develop postnatally under the influence of mechanical stress, which increases significantly after birth.
6. A feature of the coronary circulation is a large number of anastomoses between the right and left coronary arteries. This vascular architecture, which persists in the first 2 years of a child’s life, allows for collateral blood flow and supply the myocardium with the necessary amount of oxygen and nutrients.
7. The ratio of the sizes of arteries and veins in newborns is 1:1, which ensures low blood pressure and easier development of vascular collapse.
8. A feature of the nervous regulation of the cardiovascular system in healthy newborns is the predominance of the sympathetic part of the nervous system. This ensures a primary increase in heart rate in response to stress. With hypoxia, in approximately 10% of fetuses, the development of cholinergic and, especially, adrenergic nerve plexuses, which have their endings in the sinus and atrioventricular nodes, lags behind.
9. A special role is played by the pulmonary circulation, where the pressure in the period of early adaptation is 25-65 mmHg. This is due to the greater muscle mass of the arteries and the mechanisms of regulation of vascular tone - the dominance of sympathetic influences in response to birth stress.
Thus, the above anatomical and physiological features of the cardiovascular system cause less inotropic activity of the heart muscle than in other age periods and rapid dilatation of the heart chambers with the development of relative insufficiency of the atrioventricular valves.
The pathogenesis of hypoxic damage to the cardiovascular system has been well studied in relation to acute hypoxia. As a result of severe oxygen deficiency in the cardiomyocyte, aerobic glycolysis is inhibited and a transition to anaerobic glycolysis is observed, as a result of which energy deficiency develops; accumulation of under-oxidized products occurs, the permeability of membranes and the function of electrolyte pumps are disrupted. Acidosis leads to severe cellular dysfunction, including cell death. Violation of the rheological and coagulation properties of blood against the background of hypercatecholaminemia leads to the effect of erythrocyte sludge and the development of stasis and microthrombi in the small vessels of the heart and other organs. Microcirculation disorders are mainly diffuse in nature, but are most often recorded in the subendocardial areas of the myocardium.
In recent years, much attention has been paid to the influence of chronic intrauterine hypoxia (CIH) and compensatory processes developing in the fetus. According to Tsyvyan P.B. et al. (1998) CVH can influence the genetic program of heart development, disrupting the rate of migration of neural crest cells, thereby slowing down the calcium current in the membranes of cardiomyocytes and leading to a decrease in myocardial contractility. In response to long-term chronic hepatitis, the intracellular renin-angiotensin-aldosterone system is compensatory activated, which has a number of effects, such as the development of cardiomyocyte hypertrophy, spasm of local coronary vessels and proarrhythmogenic effects. Thus, under conditions of prolonged chronic hepatitis, the fetus can develop a fundamentally different heart: with hypertrophy of the heart muscle, including the walls of the ventricles and the interventricular septum, but a reduced ejection fraction.
With chronic hepatitis, the maturation of many enzyme systems is delayed, including mitochondrial enzymes and endogenous carnitine synthesis, responsible for the β-oxidation of free fatty acids. If in a healthy newborn the process of maturation of the above systems takes 2-4 days, then in a child who has suffered perinatal hypoxia, this process takes several weeks. Partial carnitine deficiency accompanies the child throughout the entire first year of his life.
The most important sign of chronic hepatitis is underdevelopment of the pulmonary vessels, expressed in hypertrophy of the muscular layer of the arteries of the pulmonary circulation. In response to birth stress, the latter spasm and, thus, increased pressure in the pulmonary artery system will maintain blood flow through the fetal communications. This condition is called neonatal pulmonary hypertension. Prolonged functioning of a patent ductus arteriosus can lead to hemodynamic disturbances, which, in combination with an energy-metabolic imbalance, can lead to the development of heart failure.
Clinical signs
CVD diabetes is nonspecific and occurs in various pathological conditions of the neonatal period. The clinical picture of this pathology in the acute period is polymorphic and is often disguised as other diseases, and the severity of the condition ranges from minimal to severe. The main clinical manifestations of hypoxic damage to the cardiovascular system in newborns can be considered pallor of the skin and acrocyanosis, the presence of a “marble” pattern, tachypnea, muffled or muffled heart sounds, emphasis of the second tone over the pulmonary artery, systolic murmur of atrioventricular valve insufficiency, expansion of the boundaries relative cardiac dullness, cardiac arrhythmias. Monitoring of patients at the Perinatal Cardiology Center in Moscow made it possible to identify three clinical and pathogenetic variants of CVD diabetes:
1. Neonatal pulmonary hypertension and persistence of fetal communications;
2. Transient myocardial dysfunction (with normal, increased or decreased contractility of the heart muscle);
3. Heart rhythm and conduction disorders;
In practice, a combination of several variants of CVD is often encountered.
Neonatal pulmonary hypertension and persistence of fetal communications are characterized by the existence of two clinical types, depending on the pressure in the right ventricle (RV) - pulmonary artery (PA) system, and, accordingly, on the direction of blood flow through the fetal communications.
The first type [high pressure in the pulmonary circulation and right-to-left shunting of blood through a patent foramen ovale (PFO) and patent ductus arteriosus (PDA)] is characterized by the clinical picture of blue-type congenital heart disease, manifested by arterial hypoxemia syndrome. Diffuse bluish discoloration of the skin is present from birth, tests performed with oxygen (hyperoxic and hyperoxic-hyperbaric) are ineffective. Cyanosis increases when the baby cries and feeds. Upon examination, it is possible to identify a moderate expansion of the boundaries of relative cardiac dullness. Heart sounds, as a rule, are well audible; there is an accentuation of the second tone over the pulmonary artery. In the second intercostal space to the left of the sternum, a systolic murmur of patent ductus arteriosus is heard, which can also be heard well from the back. The diastolic component is usually absent. X-ray examination of the chest organs reveals a moderate increase in the cardiothoracic index up to 65% (normal up to 60%) and varying degrees of depletion of pulmonary blood flow. This X-ray picture corresponds to the precapillary form of pulmonary hypertension according to N.G. Zernov. and Kuberger M.B. (1977), which occurs in 40% of patients with posthypoxic CVD. The ECG in this group of children is characterized by specific signs: an increased amplitude of the P wave (a sign of overload of the right atrium), as well as disturbances of intraventricular conduction along the system of the right bundle branch - from nonspecific conduction disturbances to complete block. ST-T segment changes are rare. Doppler echocardiography allows you to determine the pressure in the cavity of the right ventricle, which is always elevated and amounts to 35-65 mmHg. (normal up to 30 mmHg), as well as right-left discharge of blood through fetal communications and their size. Subsequently, in such children, the discharge of blood from the right to the left first becomes bidirectional (bidirectional), then a left-to-right discharge of blood can be detected, both through the patent ductus arteriosus and through the open oval window.
The second type is characterized by a predominance of left-to-right shunting of the blood, which initially occurs much less frequently - in 10% of cases and can lead to impaired lung function up to pulmonary edema. The X-ray picture of this type of pulmonary hypertension (capillary form according to N.G. Zernov and M.B. Kuberger) is characterized by an increase in the cardiothoracic index, a flattened heart waist, and moderate hypervolemia in the lungs. Differential diagnosis must be made with congenital heart defects of the pale type. This disorder of adaptation of the cardiovascular system can be considered a risk factor for the formation of such a heart defect as patent ductus arteriosus. The timing of its spontaneous closure is significantly extended - up to 2-10 months of age; its surgical correction is possible.
Follow-up observations of children who have had CVD in the form of neonatal pulmonary hypertension indicate the presence of deviations on radiographs of the chest organs in the form of an increase in the cardiothoracic index by 6-10%, an increase in the pulmonary pattern in the root area and its depletion in the periphery, which corresponds to minimal signs of pulmonary hypertension. In many patients with abnormalities on radiographs, it is possible to detect conduction disorders along the right bundle branch system on the ECG with various types of response to the treatment: from the disappearance of conduction disorders to complete refractoriness to the therapy. The latter implies the formation of the morphological substrate of such conduction disorders.
Thus, the causes of conduction disorders in the system of the right bundle branch, detected in preschool children and considered a normal variant, should be sought in the perinatal period in the form of neonatal pulmonary hypertension.
Transient myocardial dysfunction with normal or increased contractility of the heart muscle is most difficult to diagnose clinically. Signs that deserve attention include pallor of the skin, cyanosis of the nasolabial triangle that occurs during crying and feeding, moderate expansion of the boundaries of relative cardiac dullness, muffled or dull heart tones, transient murmurs of atrioventricular valve insufficiency. The lack of expression of noise leads to such an auscultatory phenomenon as impurity of tones. In such cases, the most important information is provided by an electrocardiographic study, and during the period of adaptation of the newborn, ECG changes are more pronounced and occur much more often. According to the observations of A.V. Prakhov, several variants of pathological changes in the ventricular QRST complex are identified, indicating certain disorders in the contractile myocardium - ischemic changes in the final part of the ventricular ST-T complex and transient changes in the ventricular QRS complex. ST-T changes are observed in all children with IMT. The peak of manifestations is the first 2 days of life, then rapid positive dynamics are characteristic. Ischemic changes in the QRST complex are predominantly localized in certain areas of the ventricular myocardium - the lateral wall of the right ventricle, the anteroseptal and posterodiaphragmatic wall of the left ventricle and in the region of the apex of the heart. Transient focal changes in the ventricular QRST complex are in most cases recorded in the form of a pathological QS complex, less often in the form of an electrocardiographic “off” phenomenon, which is characterized by a significant decrease in the amplitude of the main waves of the QRS complex in one or more adjacent precordial leads. Transient focal ischemic changes are most often localized in the V5-V6 region, as well as in II, III, aVF, less often in V1-V2 leads.
A.V. Prakhov (1996) identified 4 variants of the “natural evolution” of ECG changes in the ventricular QRST complex during the course of IMT. The first evolution option, which occurs most frequently (42%), is characterized by transient focal changes in the ST-T complex, which are more often recorded in the early neonatal period and disappear on the ECG within 2-3 weeks after birth. It is observed in newborns who have suffered moderate hypoxia and has a favorable prognosis. The second option (26%) – against the background of ST-T disturbances, transient changes in the QRS complex occur. This option is typical for newborns who have suffered severe hypoxia, but also has a favorable prognosis. The third option is characterized by slow dynamics of ischemic changes in the QRS complex, which do not disappear during the neonatal period. The fourth option, which occurs most rarely, is characterized by ischemic QRS complexes from the first days of life and throughout the entire neonatal period. The last two variants of IMT have a less favorable prognosis.
Doppler echocardiography allows us to determine the ejection fraction of the ventricular myocardium, the presence or absence of hypertrophy, which is important for determining and correcting therapeutic measures in this group of patients. At the same time, increased contractility of the heart muscle (70-76% with a norm of 60% according to Teinholz) should not please the doctor, since excessive compression of the smallest coronary vessels during systole contributes to self-sustaining myocardial ischemia. It is in children with increased contractility that the longest lasting ST-T changes are possible - from 2.5 to 8 months. The addition of intercurrent diseases that aggravate hypoxia leads to rapid decompensation of cardiac activity due to a drop in ventricular ejection fraction. An even more serious situation arises in children in whom a decrease in myocardial contractility and relative insufficiency of the atrioventricular valves are already detected in utero. The occurrence of even mild asphyxia in the intranatal period leads to disaster. At birth, there is a picture of cardiogenic shock with marbling of the skin, low blood pressure, and severe multiple organ disorders. On the part of the heart, cardiomegaly, significant dullness of heart sounds, systolic murmur of atrioventricular valve insufficiency at the corresponding points of auscultation, signs of circulatory failure, and a pronounced decrease in the contractility of the heart muscle are detected. Subsequently, in such children, myocardial contractility, even against the background of therapy, does not reach the required values and remains at subnormal values (55-56%).
Diagnosis of post-hypoxic damage to the cardiovascular system in the acute period includes an ECG, chest x-ray, Doppler echocardiography, and determination of the activity of cardiac-specific enzymes, such as CF-CPK and LDH1. Elevated levels of CF-CPK and LDH1 depend on the severity of hypoxia and are determined over a long period of time - up to 2 months of life, even in the absence of clinical manifestations and ECG changes.
In follow-up, using cardiointervalography, a syndrome of autonomic dysfunctions is revealed, characterized by pathological types of autonomic reactivity - hypersympathicotonic (mainly in children who have suffered moderate hypoxia) and asympathicotonic (the group of the most severe patients). The latter is known to be a preclinical marker of autonomic dysfunction syndrome.
The third clinical and pathogenetic variant of CVD is cardiac arrhythmias, a common pathology in newborns who have suffered hypoxia, especially in combination with birth trauma. Among cardiac arrhythmias, sinus tachycardia deserved priority as a natural response to hypoxia and birth stress. However, long-term sinus tachycardia must be considered as pre-heart failure due to shortening of diastole, a decrease in the volume of blood entering the ventricular cavity in diastole and, as a consequence, deterioration of coronary blood flow. The second most common cardiac arrhythmia is extrasystole. In the vast majority of cases, supraventricular extrasystoles occur - single, bigeminy, trigeminy, paired extrasystoles. A dangerous type of cardiac arrhythmia - supraventricular paroxysmal tachycardia - is a common phenomenon in the neonatal period, due to the presence of additional pathways and ectopically active foci. This cardiac arrhythmia is characterized by rapid development of signs of heart failure. The clinic notes a sharp deterioration in the child’s condition, vomiting “fountain”, refusal to eat, severe lethargy and drowsiness of the child. Some children develop an urgent situation with cardiac and respiratory arrest. There may be cases of atrial flutter, which are more easily tolerated by the child, as well as non-paroxysmal supraventricular tachycardia, paroxysmal ventricular tachycardia, i.e. almost all types of heart rhythm disturbances found in adults. It is necessary to take into account the close connection between cardiac arrhythmias in a newborn child and damage to the central nervous system, especially in the form of hyperexcitability syndrome, hypertensive-hydrocephalic and convulsive syndromes, and the presence of birth trauma.
Differential diagnosis
should be carried out with congenital heart defects of the blue (transposition of the great vessels) and pale (OOO, coarctation of the aorta) types, cardiomyopathies, myocarditis.
EchoCG almost immediately makes it possible to exclude congenital heart defects, such as transposition of the great vessels, coarctation and/or stenosis of the aorta, congenital pathology of the mitral valve (the presence of left ventricular hypertrophy in a newborn requires the exclusion of these particular defects).
If a reduced ejection fraction is detected, a moderate decrease in contractility of the heart will indicate in favor of hypoxic damage to the heart up to 40-45%, followed by rapid positive dynamics during therapy, in contrast to dilated cardiomyopathy and myocarditis, in which there is a pronounced decrease in the contractility of the heart and torpidity to treatment .
Often a diagnosis of exclusion is congenital carditis, especially when cardiomegaly is accompanied by signs of cardiac decompensation and cardiac arrhythmias. The absence of other clinical signs of congenital infection in a child and such widely used methods as examination for opportunistic infections, a biochemical blood profile, including CRP, acute phase proteins of inflammation, and a clinical blood test over time help to remove this diagnosis. Hypoxic damage is also supported by rapid positive dynamics in response to therapy.
Basic principles of therapy
for the syndrome of disadaptation of the cardiovascular system of hypoxic origin are: correction of hemodynamic disorders, improvement of metabolic processes in the myocardium, relief of arrhythmia, symptomatic therapy. In the presence of an urgent situation and the need for rapid correction of disorders (severe acute circulatory failure of the left ventricular type), it is advisable to use intravenous drip administration of dopamine for the purpose of inotropic support in newborns. The dose of the drug ranges from 2 to 8 mcg/kg per minute, administered in a 10% glucose solution at a rate of 3 ml/hour.
With a decrease in the contractility of the heart muscle and signs of NK, digoxin can be the drug of choice, although the question of its use against the background of hypoxia and ischemia is still debatable. In order to prevent the development of side effects, it is advisable to prescribe digoxin in maintenance doses without saturation, i.e. 0.01 mg/kg per day in two doses every 12 hours under heart rate control.
Reducing the hemodynamic load on the heart is achieved by using diuretics - furosemide (1-4 mg/kg), veroshpiron (2-3 mg/kg), triampur (2-3 mg/kg), etc. With adequate therapy, signs of circulatory failure in most newborns quickly stop.
In the presence of rhythm disturbances, the tactics for their relief are determined by the severity of the condition and the degree of hemodynamic disturbances. The presence of an attack of paroxysmal tachycardia requires its drug relief. Unlike older children, in whom ATP is used, regardless of the mechanism of tachycardia, this drug is not used in newborns and children in the first year of life due to the high risk of developing asystole. In addition, at an early age, tachyarrhythmia, once occurring, tends to recur. Therefore, before medicinal relief of tachycardia paroxysm, premedication is necessary. For this purpose, Finlepsin, Phenibut, Relanium, and GHB are prescribed in age-specific dosages. ATP can be used to relieve an attack only in a specialized intensive care unit with premedication. For recurrent tachyarrhythmias, the most effective are cordarone and digoxin, both separately and in combination, as well as finlepsin at a dose of 10 mg/kg per day. Digoxin is used in a maintenance dose of 0.01 mg/kg/day. Cordarone is first prescribed at a saturation dose of 10-15 mg/kg/day for 7-10 days, followed by a maintenance dose of 5 mg/kg/day. If cordarone is ineffective, propafenone (ritmonorma) can be used at a dose of 10 mg/kg/day. The duration of antiarrhythmic therapy is determined individually, averaging 3-6 months. The drugs are discontinued gradually after 3-6 months after stable normalization of the heart rhythm.
Particular attention is paid to normalizing cerebral circulation in newborns. For this purpose, Cavinton, 25% solution of magnesium sulfate, cinnarizine, trental, etc. are prescribed.
For heart rhythm disturbances: the use of neurometabolic therapy is justified. Nootropic drugs with a sedative effect (phenibut and pantogam) and a stimulating component of action (picamilon, pyriditol, aminalon, glutamic acid) are used, which contributes to the correction of cortical-subcortical relationships, the formation of the protective function of the sympathetic-adrenal system, and has a trophic effect on autonomic regulation centers . Essential properties of drugs in this group are also enhancing the bioenergetics of the nerve cell, mobilizing the energy reserves of neurons without depleting them, protecting the brain from hypoxia, and increasing tolerance to exogenous stress agents.
It is advisable to prescribe antioxidant therapy and membrane stabilizers, in particular vitamins A, C, E, and the microelement selenium, taking into account the fact that membrane dysfunction plays a significant role in the pathogenesis of heart rhythm disorders. Ubiquinone (coenzyme Q10, kudesan) has a good membrane-stabilizing effect, the use of which not only helps reduce the level of toxic lipid peroxides, but also stabilizes the balance of essential microelements (zinc, iron, copper, selenium).
Along with drugs that have a positive inotropic effect, in the treatment of dysadaptation syndrome of the cardiovascular system, cardiotrophic metabolic therapy is used, primarily Actovegin, Cytomac, -carnitine, which stimulates and supports the carbohydrate component of metabolism in cardiomyocytes, beta-oxidation of free fatty acids. Follow-up observations show that in most cases, when using Actovegin, Cytomac and -carnitine, normalization of heart size and myocardial contractility occurs much faster than when using only inotropic support (digoxin, dopamine). According to M.Ya. Ledyaeva et al. (2003) the use of β-carnitine (Elcar) at a dose of 50 to 100 mg/kg body weight for 3-4 weeks contributed to the achievement of an anabolic effect even in children with UVR combined with hypoxia. Such drugs as Riboxin, Panangin, Asparkam, KKB, etc. have found widespread use in practice.
In general, subject to adequate and timely treatment, posthypoxic syndrome of disadaptation of the cardiovascular system has a favorable course. In order to timely identify patients with scanty and nonspecific clinical symptoms, it is advisable to conduct an ECG examination of all newborns who have suffered perinatal hypoxia either before discharge from the maternity hospital or in the first month of life. In some patients, during follow-up observation, residual effects of transient myocardial dysfunction are revealed, which can persist up to the age of three (decrease in ejection fraction to 46-56%, insufficiency of atrioventricular valves, minimal signs of pulmonary hypertension, increase in heart size, disturbances in its rhythm, etc.) .d.). In this regard, this group of children requires clinical observation for the presence of a risk of developing myocardial dystrophy, autonomic dysfunction syndrome. Dispensary observation of children who have had CVD should be carried out according to form 30 up to 3 years of age.
Surveillance tactics include:
— examination by a pediatric cardiologist at least once every 3 months;
- conducting an ECG once every 3 months, after 1 year of life - lying and standing in 12 leads;
— Doppler echocardiography at least once every 6 months with mandatory determination of the size of the heart cavities and the contractility of the ventricular myocardium;
— consultations with specialists (neurologist, immunologist);
- if necessary, conduct courses of cardiotrophic and metabolic therapy with the inclusion of drugs such as actovegin, L-carnitine, ubiquinone, cytomac or cytochrome C, riboflavin mononucleotide, lipoic acid, B vitamins.
Complications and prognosis
Patients with silent ischemia should not expect a completely favorable prognosis. If left untreated, disability is guaranteed, as is sudden coronary death.
Statistics say that this pathology leads to the development of arrhythmia and chronic heart failure by at least 2 times, and death by 6 times. This leads to the fact that cardiologists pay maximum attention to problems, since timely detection of the disease gives a good chance of saving a person’s life, and prevention helps to eliminate it.
The pathology is no less dangerous than its painful relative, since the coronary bed is disrupted in both cases. But the secretive course leads to insidious pathology and a sad outcome in the future. The patient is not even aware of the problem, which significantly delays treatment. This threatens the development of:
- angina pectoris;
- severe arrhythmia;
- heart failure;
- sudden death.
Causes of asymptomatic myocardial ischemia
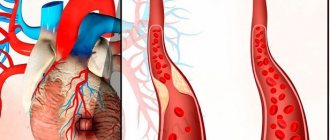
The main causes of silent ischemia are atherosclerotic vascular lesions.
Plaques on the walls narrow the blood vessels. This leads to disruption of the blood supply to the heart. Ischemia can also occur against the background of coronary vascular spasm. The development of pathology can be provoked by:
- high blood pressure;
- obesity;
- frequent stress;
- diabetes;
- sedentary lifestyle;
- bad habits;
- high blood cholesterol levels, etc.
Experts have found that the hereditary factor also has a great influence on the development of pathology. Particular attention should be paid to health if someone in the family already suffers from coronary heart disease.
Prevention
The sooner the pathology is detected, the higher the patient’s chances of life. Therefore, the best prevention of the disease is regular examinations by a cardiologist, especially after 45 years. If an ischemic episode is detected early, therapy will reduce the heart rate and the disaster it can lead to.
Give up bad habits, lead a healthy lifestyle and eat a balanced diet, this will help in the prevention of silent ischemia. Children with heart pathologies must be under strict medical care, since they are at risk, just like older people. Parents have a heavy burden to ensure that their children have a normal life.