Key diagnostic points
It is very important that the abdominal form of myocardial infarction is recognized as quickly as possible.
The main confirmation of this diagnosis is provided by an ECG. The ambulance crew must have a portable electrocardiograph. The appearance and size of pathological waves on the cardiogram can indicate the location and size of the affected lesion. If the results of a mobile examination show a disturbance in the conduction of the heart muscle, the patient must be urgently hospitalized.
The gastralgic variant of MI in the hospital is clarified and finally confirmed using laboratory rapid tests. Damage to the heart muscle is indicated by the presence of cardiac markers in the blood:
- myoglobin and troponins - proteins of muscle cells, they are released into the blood when the integrity of the membranes is violated;
- AST and ALT are enzymes, an increase in the level of which indicates damage to internal tissues.
It is also advisable to do coronary angiography.
In this situation, you need to follow a clear algorithm of actions:
general information
For individuals suffering from chronic gastrointestinal ailments, pain in the abdominal area, upset stool, and nausea do not cause concern, since they consider these phenomena to be completely natural, given the existing pathology. However, such signs may indicate an abdominal form of myocardial infarction. Most often, the gastralgic type occurs with a diaphragmatic heart attack. Males are more susceptible to it. The danger is that the symptoms are similar to intoxication, i.e., with a clinic atypical for a heart attack. Unlike other forms, the abdominal one goes through only two stages - the most acute (lasting no more than two hours), which is characterized by pronounced necrosis of the heart muscle, and acute (lasting no more than twelve hours), when the intensity of the symptoms decreases.
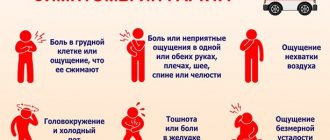
The main syndrome of the abdominal form of acute myocardial infarction is severe pain in:
- epigastric region;
- right hypochondrium;
- right half of the abdomen.
It is burning, sharp in nature and does not go away after taking Nitroglycerin.
First aid
Providing primary care to a patient who is suspected of having an atypical myocardial infarction is no different from emergency care for any heart disease.
The only difficulty arises in the fact that it is almost impossible to diagnose this disease on your own; the patient’s complaints do not correspond to the typical symptoms characteristic of a heart attack.
The main task when providing first aid is to calm the patient and call a medical team as soon as possible. At the first signs of an atypical development of the disease, you should:
- Remove from the person all constricting objects (tie, neckerchief, belt) that interfere with breathing, loosen or unfasten clothing.
- Sit in a comfortable position on a chair or armchair, leaning your torso against the back. You can place the patient on his side with his knees bent.
- Open the window, directing a stream of fresh air towards the patient.
- Give the person a nitroglycerin tablet or offer to take aspirin (at least 300 mg), after dissolving it in a small amount of water.
- Call an ambulance, clearly explaining the symptoms of the disease to the dispatcher.
- If medical care is delayed, take the patient to the nearest medical facility yourself.
Also read: Stroke and heart attack - what is the difference?
This algorithm of action can save the patient’s life; this pathology is often accompanied by cardiac arrest. The high mortality rate from an atypical form of heart attack is due to difficulties in diagnosing and late seeking medical help.
Uncharacteristic development of myocardial infarction
The increase in the number of atypical variants of the disease is associated with a change in the age structure of patients. On the one hand, heart attacks often affect young citizens, and on the other hand, they are increasingly observed in older people. In this case, it is often repeated and develops against the background of various concomitant pathologies. The last factor affects the course and clinical picture of the disease. All variants of heart attack that have an uncharacteristic onset are conventionally divided into painless and painful. Atypical myocardial infarction of the abdominal form refers specifically to pain. This phenomenon causes some difficulties in diagnosis, since the localization of the pain syndrome is atypical. The individual mainly feels pain in the epigastric, iliac, umbilical (umbilical) region, as well as in the hypochondrium. Therefore, the person is sure that the pain is caused by problems with the gastrointestinal tract. There are many cases where a heart attack of this form provoked an exacerbation of acute pancreatitis, cholecystitis, appendicitis and other diseases. For timely and reliable diagnosis of the gastralgic form of infarction, it is necessary to take into account that the predominant localization of pain in such patients is the abdominal area. The abdominal form of myocardial infarction, as well as other variants that have an atypical onset, is most often the lot of elderly citizens with signs of atherosclerosis and a hereditary predisposition.
Diagnosis of atypical heart attack
Differential diagnosis of atypical infarction and acute pathologies of the peritoneal cavity involves a thorough analysis of the patient's anemnesis. In the presence of ulcerative and inflammatory lesions of the gastrointestinal tract or angina attacks, suspicions arise about the progression of gastrointestinal diseases or the development of a heart attack.
With biliary colic, pain in the right hypochondrium appears after eating fatty foods or spicy foods, and is often accompanied by nausea. During a heart attack, wave-like pain usually spreads beyond the sternum and into the area of the left arm.
Pain radiating to the right side of the body is characteristic of biliary colic. An enlarged gallbladder and pain during palpation are signs of acute cholecystitis. Abdominal muscle spasms during a heart attack become less intense when the patient's attention is diverted. This does not happen with pathologies of the digestive tract.
Incorrect assessment of patients' sensations sometimes leads to medical errors. Diagnosis is complicated by the fact that nonspecific symptoms of a heart attack (fever, increased levels of neutrophils in the blood) can accompany exacerbation of chronic forms of pathologies of the digestive tract.
A special role is given to electrocardiographic research. If there is any doubt about the diagnosis, it should be done as soon as possible. Approximate information can be obtained using a hemostasiogram (blood clotting indicators).
Causes
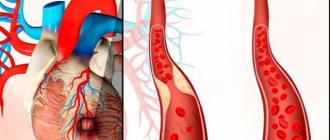
The gastralgic form occurs in the case of pathological narrowing of blood vessels as a result of their damage by a mixture of fats, i.e., atherosclerotic plaques. The peculiar clinical picture is due to the close location of the dead area to the diaphragm. In addition to atherosclerosis, the causes of heart attack are:
- abuse of alcoholic beverages;
- smoking;
- obesity;
- angina pectoris;
- pericarditis;
- diabetes;
- heredity.
Failure of blood circulation in coronary artery disease contributes to the formation of necrosis in the heart muscle. In the acute course of this process, a condition called a heart attack occurs. The anterior wall of the left ventricle is most often affected. But the abdominal form of myocardial infarction is characterized by necrosis in the posterior wall of the muscle of the main human organ, which is quite close to the diaphragm. The uniqueness of this pathology is that the patient is bothered by pain in an atypical place - in the epigastric region and under the ribs on the left side. Unfortunately, a blurred or unclear clinical picture is the cause of an error in making the initial diagnosis.
Causes
Abdominal infarction is caused by external and internal factors. Impaired blood supply and cell death can provoke:
- Damage to the coronary arteries of the heart by atherosclerotic plaques. This pathology often develops against the background of high levels of low-density lipoproteins in the blood. Lipids are deposited on the walls of the arteries, harden and increase in size. Plaques can block the lumen of the vessel, impeding blood flow.
- Smoking. Promotes vascular damage and the development of atherosclerosis.
- Obesity.
- Hypertension.
- Presence of angina pectoris.
- Drinking alcohol regularly over a long period of time.
- Endocrine disorders (diabetes mellitus).
- Errors in nutrition (predominance in the diet of fatty foods and foods rich in simple carbohydrates).
- Inflammatory diseases (arteritis).
- Blockage of the coronary arteries by a thrombus or embolus.
- Anomalies in the development of blood vessels that supply the heart.
- Stress.
- Physical inactivity (lack of physical activity).
Diagnostic measures
For the purpose of differential diagnosis, a troponin test is performed at the prehospital stage. It shows the presence of elements of myocardiocyte breakdown in the blood. At later stages of infarction, C-reactive protein and moderate leukocytosis are detected. And the activity indicators of liver cells are subject to changes both in pancreatitis and hepatitis, and in the abdominal form of myocardial infarction. Therefore, this variety almost always causes difficulties in differential diagnosis.
The main clinical feature is pain in the abdominal area, or more precisely, in the epigastric region or left hypochondrium. Often there is a false diagnosis of pancreatitis. Abdominal pain is characteristic of posterior localization of the infarction. In this case, the diaphragmatic muscles are partially involved in the process.
Location of pain
The localization of pain is usually observed in the upper abdomen (especially with a posterior infarction). Patients mainly complain of pain in the epigastric region, but a detailed survey reveals pain in the chest and in the area of the heart. To accurately determine the location, the doctor asks the patient to indicate with his hand the place where the pain occurs.
If attacks do not occur for the first time, the main symptoms of the abdominal variant of myocardial infarction change in character. The patient may note that the pain has become stronger, heavier or squeezing; previously taking nitroglycerin helped, but now it doesn’t, etc.
Any changes in the specifics of pain (different nature, spread to certain places) require a thorough diagnosis. The main task of the doctor is to differentiate between a heart attack and diseases of the abdominal organs.
Pain usually appears after physical exertion and emotional stress; it can occur during eating. Gastric pain syndrome has a wave-like character - it increases gradually and reaches a peak approximately an hour after the onset of the attack. This condition is often accompanied by panic and fear of death. Taking nitroglycerin provides temporary relief.
Myocardial infarction is usually accompanied by a state of shock, cardiac asthma, sudden rhythm disturbances, loss of consciousness
The pain may be accompanied by nausea, and in rare cases, single vomiting. As practice shows, pain, regardless of the initial location, eventually flows beyond the sternum, closer to the heart.
When interviewing a patient, you should not ask about feelings of fear and panic, unless the patient himself says so. Focusing on the psycho-emotional state can only aggravate the condition, and with new attacks the patient will artificially attach such sensations to himself.
Read also: Exercise therapy for myocardial infarction exercises
Upon examination, pale skin, blue lips are noted, anxiety is reflected on the face, and the patient is worried about shortness of breath. The skin is covered with perspiration, but is cold to the touch. The tongue is moist and clean.
When listening, disturbances in heart rate and tachycardia are observed. The borders of the heart are expanded, the tones are muffled (up to complete disappearance). Sometimes a friction noise of the pericardial sac is heard. Blood pressure is low, at the initial stage it can be normal or even elevated.
You can learn about the main markers of myocardial infarction from this article.
When examining the abdomen, it is necessary to pay attention to muscle tension, the presence of hepatic dullness, bloating, involvement in the breathing process, symmetry, localization of pain, and the presence of symptoms of peritoneal irritation.
With an infarction of the posterior wall from the abdominal organs, incomplete paralysis of the stomach, bloating, abdominal wall tension and pain may be observed. Stool disorders are usually not observed. An increase in these symptoms during a heart attack is not observed.
- Laboratory manifestations such as an increase in the concentration of leukocytes, a shift of the leukocyte formula to the left, the presence of c-reactive protein, an increase in the content of sialic acids are not among the distinctive diagnostic indicators, and therefore cannot be used for differentiation in emergency diagnosis.
- Considerable importance is attached to the analysis of enzymes to distinguish diseases that have symptoms of an “acute abdomen”. Blood tests for abdominal infarction, such as the study of aspartate and alanine aminotransferase, are not always informative.
- An increase in the concentration of creatine phosphokinase and a change in the content of lactate dehydrogenase are also observed in pancreatitis and require a lot of time for analysis, which does not allow their use in a specific patient. Approximate information can be obtained from coagulogram data.
- Typical signs of dying areas of the heart muscle are observed on the electrocardiogram, but they appear only the next day.
- The abdominal form of a heart attack is difficult to distinguish from pathologies of the abdominal organs. Pain in the epigastric region or in the upper abdomen on the right, accompanied by nausea and vomiting, makes one think about acute gastritis, pancreatitis, cholecystitis, and exacerbation of cholelithiasis.
- The listed diseases, as well as a heart attack, can be accompanied by an increase in temperature and an increase in the concentration of leukocytes. A carefully collected anamnesis is of great importance in differentiating a heart attack and exacerbation of diseases of the abdominal organs. The presence of angina attacks, exacerbation of cholecystitis or pancreatitis allows one to lean towards one or another disease.
- With hepatic colic, pain appears after eating spicy and fatty foods. They are noted in the right hypochondrium and become intense from the first minutes. This condition may be accompanied by nausea.
- During a heart attack, pain is rarely localized only in the right hypochondrium or epigastric region; it usually radiates to the sternum. Repeated examinations after half an hour or an hour often reveal pain in the heart and left arm.
- What distinguishes a heart attack from hepatic colic is that the pain with it increases gradually and has a wave-like character. Hepatic colic is characterized by pain spreading to the right shoulder and scapula, which is not typical for a heart attack.
- Acute cholecystitis is indicated by an enlarged and painful gallbladder, painful “vesical” and “liver” points on palpation. During a heart attack, the abdominal muscles are not so tense. Gallstone disease is confirmed by the appearance of jaundice.
- In hepatic colic, ALT is higher than AST, and an increase in alkaline phosphatase is also noted. A heart attack is characterized by an increase in LDH, which is not observed in hepatic colic. Also, during a heart attack, CPK increases sharply, which practically does not change during exacerbation of cholelithiasis.
- Of particular importance are the ECG results, which confirm or deny the presence of a heart attack. In case of doubt regarding the diagnosis, it should be carried out as quickly as possible.
The set of first aid measures always includes taking an electrocardiogram, and if the doctor for some reason refuses the study, the patient must insist on having it performed.
Differential diagnosis of abdominal form of myocardial infarction
Due to atypical symptoms, it is performed with such pathologies as:
- appendicitis;
- perforated ulcer;
- cholecystitis;
- toxic food infection;
- intestinal obstruction;
- pancreatitis.
After collecting the anamnesis of the whole family, the individual’s complaints and examination, a preliminary diagnosis is made, and an accurate diagnosis is made only after laboratory and instrumental examinations. In differential diagnosis, the result of an ECG taken in the first minutes of the onset of pain and a survey of the individual are important.
Signs
Symptoms of the abdominal form of myocardial infarction appear in the first hours of the disease. Pain (stinging), which appears unexpectedly against the background of emotional or physical stress, is considered the main symptom. Often a person is not able to describe the nature of the pain syndrome, since there is no clear localization, and the intensity weakens after taking Drotaverine or Nitroglycerin. And changing the position of the body does not have any effect on it.
Cold sweat, low blood pressure, pallor of the dermis - these are all companions of gastralgic pain. In addition, the individual has the following clinical picture:
- bloating;
- nausea and vomiting;
- dermis moist and cold;
- stool disorder;
- heart rate becomes erratic;
- cardiac sounds are dull, systolic murmur and additional sounds appear;
- cardiac asthma;
During an attack, the patient has a fear of death.
Symptoms of the abdominal form of myocardial infarction most often appear after eating. This phenomenon is associated with poor blood supply to the heart muscles during gastrointestinal tract activity. When examining the abdomen, there is no tension. There is also no temperature observed during the acute period. After a few hours, the pain syndrome moves to the chest area.
Treatment of acute myocardial infarction in the first 48 hours
If, despite all the contradictions in the clinical picture, the patient is still diagnosed with myocardial infarction, treatment for this pathology no longer raises questions. Any form of this disease should be considered as acute necrosis of the heart muscle. This approach will make it possible to begin specialized measures from the first minutes of the development of the disease.
There is a clear division of drugs according to their use in the acute period of the pathological process and their further use in long-term therapy. From the first seconds of myocardial infarction, the following must be done:
- First of all, relieve pain. This will help avoid the development of painful shock, which can lead to severe cardiac failure. Narcotic analgesics, mainly morphine, are usually used. Taking 2 - 5 mg every 30 minutes of this drug will not only reduce pain, but also help dilate the coronary veins.
- Nitrates, in particular nitroglycerin, are good for angina attacks, but cannot relieve pain due to necrosis of the heart wall. The lack of response of the patient's body to these drugs is already a clinical symptom of a heart attack.
- Much attention has recently been paid to the use of anticoagulants for the treatment of necrosis of the heart wall. Currently, most cardiology clinics are moving away from the use of heparin and clexane and are focusing on the use of streptokinase and the rapid administration of alteplase and urokinase. Scientific evidence suggests an 8-12% reduction in mortality when using these drugs.
- Combating oxygen deficiency in tissues is one of the top five resuscitation measures for acute myocardial infarction; it is extremely important to ensure its access to the patient’s tissues.
The percentage of patient recovery depends on the emergency start of rescuing a patient with acute necrosis of the heart muscle.
Abdominal form of myocardial infarction: first aid
Individuals with severe gastralgic symptoms, which are not typical for the picture of an “acute abdomen,” are hospitalized in the cardiology department to determine the final diagnosis. Until the doctors arrive:
- The patient is placed in a horizontal position.
- It is advisable to provide fresh air.
- If possible, measure your pressure. If the numbers are high, it is allowed to give the medicine that the patient had previously taken.
To exclude erroneous hospitalization in an infectious diseases or surgical healthcare facility, the patient is given an ECG before his hospitalization. In the gastralgic form, the results obtained after recording cardiac activity are correlated with a lower (posterior) infarction.
After diagnosis (in the absence of restrictions and contraindications), thrombolysis is allowed at the prehospital stage. In addition, Heparin and antiplatelet agents must be administered. In case of cardiogenic shock, infusions of infusion solutions are indicated.
After analgesia, the individual is taken in a supine position to a multidisciplinary inpatient healthcare facility. Where additional laboratory and hardware types of examinations are performed. The choice of treatment method - angioplasty, bypass surgery, stenting of coronary vessels - is determined by the attending doctor.
Location and nature of pain
In the abdominal form of myocardial infarction, the pain is localized in the upper abdomen. However, patients feel it both in the heart area and behind the sternum. With a repeated heart attack, the nature of the pain and its irradiation changes. Therefore, the factors that caused it must be differentiated.
Basically, pain occurs after emotional or physical stress and can coincide in time with eating. It increases gradually, becoming strongest thirty to sixty minutes after the onset of the attack. Often the individual is seized with panic and feels the fear of death. Taking Nitroglycerin alleviates it for a certain period. The pain is accompanied by nausea, vomiting is quite rare.
Prevalence of the disease
The abdominal form of myocardial infarction, the symptoms of which are extremely atypical, has difficulties with diagnosis.
Therefore, to make an accurate diagnosis, it is necessary to carry out differential diagnosis with certain diseases of the gastrointestinal tract, especially with pancreatitis and cholecystitis. In addition to interviewing and examining the patient, a very important point in such a diagnosis is an examination of the abdomen, during which the doctor identifies the degree of pain and tension in the abdominal wall. It is also necessary to conduct some laboratory tests, the results of which will allow an accurate diagnosis to be made. Such studies include:
- ECG and EchoCG;
- coronary angiography;
- MSCT;
- troponin test;
- Ultrasound of the heart;
- blood tests.
Also an indicator of the abdominal form of myocardial infarction is the presence of hemorrhagic shock, which is observed in almost all patients with this disease. Therefore, if a person, in addition to severe pain, has low blood pressure, tachycardia and acute hypoxia, then we can say with a high degree of confidence that the patient has necrosis of the heart muscle.
The abdominal form is observed in heart patients prone to high cholesterol levels. The disease is distributed evenly across age groups and is equally common in both adults and elderly people.
Based on some factors, the disease has differences based on the patient’s gender. Example: due to dietary habits, men are more often susceptible to this pathology. They are more addicted to alcohol, which damages the heart and leads to excessive obesity (especially if it is beer), and also abuse fatty foods.
The main difficulty of an abdominal infarction is its similarity to a completely different problem in the body: a disorder of the digestive functions. If the illnesses are confused, the patient will face inevitable death if the operation is incorrect or greatly delayed.
The main method of preliminary diagnosis is simple palpation of the abdomen, during which slight pain may be felt. It allows you to understand which area of the body is in pain and whether there is swelling in certain areas.
In the presence of a heart attack, no serious abnormalities are found in the abdominal cavity, but severe and, at first glance, causeless pain in the diaphragm is detected. This observation allows us to move on to the main diagnostic method - coronary angiography.
Symptoms of myocardial infarction can be generalized and affect the entire body or focus on one body system. Necrosis of the heart muscle does not always have typical symptoms, such as chest pain, dizziness, fear of death, etc., which significantly complicates diagnosis.
In this regard, the following atypical forms of the disease are distinguished:
- Abdominal. Pain occurs in the epigastrium, which causes spasm of the abdominal muscles and eating disorders. Accompanied by hiccups, nausea, vomiting, diarrhea, flatulence. The abdominal variant in its course resembles acute inflammation of the pancreas.
- Asthmatic. If you have seen a person suffocating from a spasm of the respiratory tract, then you can easily imagine what a myocardial infarction looks like in this form. Expiratory shortness of breath, increasing and accompanied by pain in the heart, indicates the development of a necrotic process.
- Brain. Symptoms resemble those of cerebral ischemia. There is clouding of consciousness, decreased concentration, and possible fainting. Such a person does not understand well what is happening around him and cannot express any complaints.
- Collaptoid. There is a rapid decrease in blood pressure, cold sweat, and darkening of the field of vision. Another name for this condition is defined as cardiogenic shock. Often accompanied by arrhythmia.
- Peripheral. When pain first occurs in areas of the body distant from the heart region. This could be the lower jaw, left arm, spine, etc.
During prolonged attacks of a heart attack, significant swelling may occur, accompanied by shortness of breath, malaise, and in severe cases, ascites due to acute right ventricular failure. These forms can be combined with each other; less often, myocardial ischemia is asymptomatic.
The abdominal form is characterized by symptoms reminiscent of poisoning. It occurs with diaphragmatic infarction, so you should be especially careful in the differential diagnosis. This form most often affects men.
Therapy
Treatment of the abdominal form of myocardial infarction is carried out in a 24-hour hospital for 25-35 days. This is necessary for constant monitoring of the individual’s condition. The patient must remain in bed and avoid any situations that could provoke overexertion. Pharmacotherapy is aimed at eliminating symptoms and preventing the development of complications. Doctors recommend taking medications belonging to the following pharmacological groups:
- ACE inhibitors;
- calcium blockers;
- nitrates;
- sedatives;
- analgesics;
- thrombolytics;
- beta blockers;
- disaggregants;
- anticoagulants.
In the abdominal form, symptoms similar to a malfunction in the gastrointestinal tract are observed, so the patient is prescribed medications to prevent the secretion of bile, reduce acidity, and increase intestinal efficiency.
If there are complications and concomitant ailments, other medications may be prescribed.
During inpatient treatment, the individual must perform special exercises to return to their previous physical condition. The course of physical therapy is designed for the entire recovery period, i.e. from six to twelve months.
In addition, dietary nutrition is necessary, since the abnormal process is accompanied by dyspeptic symptoms.
Treatment
In case of myocardial infarction (abdominal form), treatment begins immediately after the diagnosis has been clarified. Therapy is aimed at reducing myocardial oxygen demand, restoring vascular patency, eliminating risk factors, relieving pain and preventing complications. Patients with a heart attack are hospitalized.
The main aspects of therapy are:
- Taking medications.
- Easier breathing.
- Cardiopulmonary resuscitation. Required in the absence of consciousness, disappearance of the pulse and cessation of breathing.
- Defibrillation. Performed in case of cardiac arrest.
- Relieving pain syndrome.
- Surgical intervention.
- Following a strict diet. In case of atherosclerosis, fatty dishes and foods, sweets, mayonnaise, pickles, smoked meats and alcohol are excluded from the menu.
- Rehabilitation activities (gymnastics, massage, physiotherapy).
Medication
For abdominal (abdominal) myocardial infarction the following are used:
- Narcotic painkillers (Fentanyl).
- Neuroleptics (Droperidol).
- Nitrates. They must be administered intravenously.
- Beta-blockers (medicines based on metoprolol, bisoprolol and atenolol). Indicated for increased blood pressure and heart rhythm disturbances.
- Statins. Prescribed for heart attack due to dyslipidemia and atherosclerosis.
- Thrombolytics (Streptokinase).
- ACE inhibitors (Captopril, Enap).
- Calcium antagonists (Verapamil).
- Antiarrhythmic drugs (Lidocaine, Amiodarone).
- Potassium (Panangin) and magnesium preparations. Panangin is prescribed after a heart attack.
- Antiplatelet agents and anticoagulants.
Operation
In severe cases of abdominal infarction, installation of metal structures (stents) into the lumen of the coronary arteries or bypass surgery is required. When aneurysms form, they require excision. In case of severe cardiac arrhythmia, a pacemaker is installed for the person.
Prevention of the abdominal variant of myocardial infarction comes down to giving up cigarettes and alcohol, limiting fatty and sweet foods on the menu, timely treatment of atherosclerosis and thrombosis, normalizing weight, eliminating stress and stabilizing blood pressure.
Abdominal heart disease requires surgery and the use of certain medications. Injections of adrenaline (temporary measure) and thrombolotics (substances that help cope with blockage of blood vessels) are taken as means of restoring blood circulation.
- Eliminate the focus of necrotic changes.
- Restore blood circulation (by eliminating a blood clot or transplanting a vessel).
- Identify capillaries and veins in the myocardium area so as not to lead the body to excessive bleeding.
- Make the incision correctly and then suture it, the periosteum and the chest.
Suitable instruments for the operation are an electric scalpel and a regular scalpel, clamps. Obese people or patients with high cholesterol should first perform an indirect cardiac massage without cutting the chest.
With abdominal lesions, necrosis can be transmitted from the myocardium to the diaphragm. In this case, this part of the body is also operated on in order to eliminate dead tissue, and the operation becomes urgent.
After the operation, it is very important to correctly fasten all the incised elements. Due to its heavy weight and low flexibility, the chest is connected with wire. Epithelial tissue - the outer layer, which is easiest to restore, is stitched with self-absorbable threads. The periosteum is connected using reinforced threads.
When treating this form of myocardial infarction, the same drugs are used as for typical manifestations. The pain is not relieved by nitroglycerin, so if it occurs, it is worth resorting to narcotic analgesics.
Due to the ambiguity of symptoms, the disease should be differentiated from:
- acute pancreatitis;
- acute cholecystitis;
- poisoning;
- inflammation of the appendix;
- intestinal obstruction.
To prevent recurrent attacks, the following is prescribed:
- beta blockers;
- calcium antagonists;
- sedatives;
- anticoagulants;
- angioprotectors.
It is necessary to exclude excessively fatty and fried foods, excessive physical activity, and bad habits. If doctors' recommendations are not followed, myocardial infarction is characterized by relapses. Maintaining a healthy lifestyle will help avoid recurrent attacks.
Preventive actions
To prevent a recurrent heart attack, doctors advise:
- lead an active lifestyle;
- give up cigarettes and alcohol;
- visit a cardiologist annually;
- control blood pressure and cholesterol levels;
- undergo the necessary examinations, including cardiac angiography, ECG and others;
- adjust the diet - exclude fried and fatty foods, enrich it with cereals and legumes, fish, nuts, vegetables, lean meats;
- stick to a daily routine;
- sign up for a pool or cardio workout;
- take medications prescribed by the doctor - angioprotectors, beta-blockers, anticoagulants, calcium antagonists, sedatives;
- treat associated ailments.
Failure to comply with the above recommendations is fraught with relapses.
Disease prevention
Preventive measures are aimed at preventing the development of a typical myocardial infarction. To do this you need:
- Monitor the condition of the heart muscle. To do this, it is enough to undergo an examination by a cardiologist.
- Monitor cholesterol and blood pressure; if they increase, they need to be reduced.
- Monitor your diet, that is, reduce your fat intake by replacing them with protein foods, such as lean meat, as well as beans, cereals, nuts, vegetables and fish.
- Monitor your physical fitness, that is, get rid of obesity.
- Regularly devote time to physical activity, especially cardio training: running, swimming, etc.
It is also important to completely quit smoking and limit the amount of alcohol consumed as much as possible, since these products have a greater impact on the development of a heart attack.
Complications
The abdominal form of myocardial infarction, the clinical picture of which is described in the article, if misdiagnosed and treated, is complicated by the following pathological conditions:
- rupture of cardiac tissue;
- acute heart failure;
- pericarditis;
- post-infarction syndrome;
- thrombosis;
- arrhythmias;
- neurotrophic disorders;
- aneurysms.
Sudden coronary death overtakes an individual if timely assistance is not provided. In addition, you should definitely take a rehabilitation course.