© Author: A. Olesya Valerievna, candidate of medical sciences, practicing physician, teacher at a medical university, especially for SosudInfo.ru (about the authors)
Arterial hypertension (AH) is one of the most common diseases of the cardiovascular system. According to various sources, about a quarter of the entire world population suffers from it, and at least 7 million deaths are associated with its manifestations. In 9 out of 10 patients, the cause of hypertension cannot be found, but approximately 10% of cases are secondary hypertension, which is a symptom of another disease.
Secondary hypertension is considered a manifestation of the pathology of organs involved in maintaining normal blood pressure (BP), therefore, if they are damaged, its fluctuations are possible. With this form of pathology, a malignant and progressive course, poor response to therapy, and persistent high blood pressure are more often observed.
Symptomatic hypertension is more often recorded in young people 30-40 years old. According to estimates, it accounts for about half of the cases of high blood pressure in this age group, so it is extremely important to promptly suspect the secondary nature of the pathology and find its cause.
Analyzing clinical data, experts have identified up to 70 different diseases that can be accompanied by symptomatic hypertension , so the search for a specific cause is often difficult and takes time. Meanwhile, hypertension progresses, leading to irreversible changes in organs and disruption of endocrine metabolic processes, which further aggravates the patient’s condition.
The development of new approaches to identifying the disease, the use of more advanced methods of laboratory and instrumental examination have made it possible to increase the level of diagnosis and speed up the prescription of specific treatment, which is extremely important for symptomatic hypertension, because without eliminating the root cause, one can fight secondary hypertension for a long time and unsuccessfully with the risk of dangerous complications.
Classification of the disease by severity
Depending on the level of blood pressure, the persistence of its increase and changes in the heart and fundus of the eye, 4 degrees of severity of hypertension are distinguished:
- Transitional. At this stage, there is no sustained increase in pressure levels, and there are no changes in the blood vessels of the eyes and heart.
- Labile. In this case, an increase in blood pressure values is detected, but they do not decrease on their own. There is a change in the left ventricle (its insignificant increase) and narrowing of the vessels of the eyeball.
- Stable. Persistence of high blood pressure, enlargement of the left ventricle, changes in the blood vessels of the eyes.
- Malignant. Develops quickly, high blood pressure numbers (diastolic pressure increases greatly), changes in the heart (myocardial hypertrophy), brain, blood vessels and fundus.
Features of treatment
Symptomatic arterial hypertension is only a sign of an underlying disease. For successful treatment it is necessary to identify the cause and eliminate it. For some pathologies, this means removal of the tumor, for others, hormone replacement therapy. However, it is not always possible to carry out etiotropic therapy, and therefore blood pressure is corrected with antihypertensive drugs: ACE inhibitors, calcium and aldosterone antagonists, diuretics, beta-blockers. In this case, the choice of drug is determined by its effectiveness in influencing the central link in the pathogenesis of the development of hypertension in a specific endocrine disease.
Consequently, endocrine symptomatic hypertension is a complex of pathologies that directly affect the increase in blood pressure. Standards of treatment for primary hypertension in this case will be ineffective - first you need to influence the human endocrine system. Only by adjusting the hormonal levels can progress in therapy be achieved.
Difference between secondary hypertension and primary
For effective treatment of secondary endocrine hypertension, it is necessary to know the signs of its difference from primary hypertension. This is very important, since standard treatment for hypertension is not effective in this case.
- Hypertension appeared suddenly, the pressure was high and stable.
- Hypertension develops quite quickly.
- Age also matters a lot. Endocrine arterial hypertension occurs in young (under 20 years) and elderly (after 60 years) people.
- The level of pressure does not decrease when taking antihypertensive drugs, and their maximum doses do not give a satisfactory result (pressure decreases slightly and for a short time).
- Diastolic pressure is quite high.
- Symptomatic hypertension leads to the development of a panic attack.
Treatment of symptomatic hypertension
Treatment of secondary hypertension involves an individual approach to each patient, because the nature of the prescribed medications and procedures depends on the primary pathology.
With coarctation of the aorta, valvular defects, and anomalies of the renal vessels, the question is raised about the need for surgical correction of the changes. Tumors of the adrenal glands, pituitary gland, and kidneys are also subject to surgical removal.
In case of infectious and inflammatory processes in the kidneys, polycystic disease, antibacterial, anti-inflammatory drugs, restoration of water-salt metabolism are needed, in severe cases - hemodialysis or peritoneal dialysis.
Intracranial hypertension requires the prescription of additional diuretics; in some cases, anticonvulsant therapy is necessary, and large processes (tumor, hemorrhage) are removed surgically.
Antihypertensive therapy involves prescribing the same groups of drugs that are effective in the case of essential hypertension. Shown:
- ACE inhibitors (enalapril, perindopril);
- Beta-blockers (atenolol, metoprolol);
- Calcium channel antagonists (diltiazem, verapamil, amlodipine);
- Diuretics (furosemide, diacarb, veroshpiron);
- Peripheral vasodilators (pentoxifylline, sermion).
It is worth noting that there is no single treatment regimen for secondary hypertension in all patients , since drugs from the list prescribed for the primary form of the disease may be contraindicated in patients with pathology of the kidneys, brain or blood vessels. For example, ACE inhibitors cannot be prescribed for renal artery stenosis, which has led to renorenal hypertension, and beta-blockers are contraindicated in persons with severe arrhythmias due to heart defects and coarctation of the aorta.
In each case, the optimal treatment is selected based on the manifestations, first of all, of the causative pathology, which determines the indications and contraindications for each drug. The choice is made by the joint efforts of cardiologists, endocrinologists, neurologists, and surgeons.
***
Secondary arterial hypertension is a pressing problem for doctors of many specialties, because not only its identification, but also the determination of the cause is a complex and often lengthy process that requires numerous procedures. In this regard, it is very important that the patient sees a specialist as early as possible and outlines in as much detail as possible all his symptoms, the nature of the development of the pathology, medical history, family cases of certain diseases. Correct diagnosis of secondary hypertension is the key to successful treatment and prevention of its dangerous complications.
Causes of secondary endocrine hypertension
The endocrine system helps maintain and regulate the balance of the internal environment of the human body. This is accomplished by hormones produced by the endocrine glands. The following endocrine glands take part in the regulation of blood pressure: the thyroid gland, adrenal glands and pituitary gland.
There are two main reasons that contribute to increased blood pressure in diseases of an endocrine nature:
- water and salt retention occurs in the body;
- an increase in hormone levels, which leads to increased work of the sympathetic nervous system.
Activation of the sympathetic nervous system promotes changes in the cardiovascular system (narrowing of the lumen of blood vessels, increased heart rate, heart contraction with greater force). All these changes contribute to the development of secondary hypertension.
Prevention measures
It is necessary to observe preventive measures aimed at preventing the development of arterial hypertension caused by disorders of the endocrine system. Important measures include the following:
- adherence to daily routine;
- avoidance of stressful situations;
- proper nutrition;
- weight control;
- playing sports;
- refusal of salt;
- walks in the open air.
It is worth giving up salt, as the product has the property of accumulating liquid. This causes blood pressure to rise. If you follow all preventive measures, you can significantly reduce the risk of disease and improve your well-being. When the first signs of endocrine symptomatic hypertension, dangerous to human life, appear, urgent consultation with a specialist is needed. It is important to start treatment on time.
Acromegaly
Acromegaly most often occurs due to a tumor of the pituitary gland. It occurs in middle-aged people (from 30 to 50 years old). With this disease, the level of growth hormone increases. It has a great impact on the sodium level in the body, leading to its increase. When the level of sodium in the blood increases, fluid retention occurs, which, in turn, helps to increase the volume of blood circulating in the human body. All these disorders lead to persistent hypertension.
In a person with this disease, external characteristic changes can be observed:
- increase in brow ridges;
- fingers become thick;
- the size of the foot increases noticeably;
- lips, tongue and nose are large.
All these changes occur under the influence of growth hormone. They develop rather slowly, so differences can only be noticed when comparing photographs from different years.
This diagnosis is made based on examination, the presence of hypertension, and laboratory data. A person’s blood must be taken to determine the level of growth hormone after a glucose load. Computed tomography and magnetic resonance imaging will help identify a pituitary tumor.
Acromegaly is treated with surgery. An operation is performed to remove the pituitary tumor through the nasal passages. It gives a positive result and leads to a gradual decrease in the level of growth hormone (it decreases over 2 years). If surgery is not possible, then radiation therapy is prescribed. Drug treatment is auxiliary and is carried out before and after surgery.
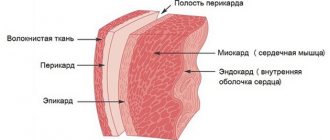
Description of the pathology
Arterial hypertension is a persistently elevated blood pressure level of 140/90 mm Hg. Art. According to statistics, 80-90% of patients have primary (essential) hypertension, the remaining 5-10% have secondary (symptomatic) hypertension. Symptomatic arterial hypertension is based on diseases of various internal organs, which can even indirectly affect blood pressure levels. In such a situation, hypertension is not a separate disease, but only pronounced symptoms of another pathology.
Symptomatic hypertension is divided into 4 main types: renal, hemodynamic, central and endocrine. With the development of endocrine diseases, the amount of hormones produced changes, which affects the change in readings on the tonometer. Often, with diseases of the endocrine system, the patient experiences not only an increase in blood pressure, but also hypertensive crises, which are very dangerous.
Symptomatic arterial hypertension is distinguished by a persistent course of the disease and resistance to hypotonic drugs. It also negatively affects target organs: heart, kidneys.
Symptomatic hypertension has a number of differences:
- Involves the age category of people under 20 and over 60 years old.
- Characterized by a sharp rise in blood pressure and its persistent consolidation at high levels.
- Intensive progression of the disease with malignant manifestations.
- The onset of periodic panic attacks.
- Lack of positive response to antihypertensive drugs.
- Increased lower values in the presence of renal hypertension.
- Detection of causative pathologies in the history taking.
Distinctive symptoms contribute to the establishment of a rational diagnosis and correct treatment.
Endocrine hypertension can develop against the background of the following pathologies:
- malfunction of the adrenal glands (pheochromocytoma, Conn's syndrome);
- excess amount of thyroid hormones (hypothyroidism, thyrotoxicosis);
- disorders of the pituitary gland (acromegaly, Cushing's disease).
With the development of these pathologies, hypertension is a symptom of the underlying disease and has high rates (from 160/100 mm Hg).
Itsenko–Cushing disease and syndrome
Another pathology that develops due to a pituitary tumor is Itsenko-Cushing disease. The syndrome occurs in the presence of tumors in the adrenal glands. In these diseases, there is an increased production of glucocorticosteroid hormones (cortisol). A person experiences the development of hypertension, activation of the sympathetic nervous system and mental disorders (psychosis). Symptomatic hypertension in this disease is malignant in nature, and the increase in blood pressure is persistent. The symptoms of this disease are quite varied:
- the formation of excess adipose tissue on the torso, face and neck;
- eye pathology (cataracts);
- cheeks acquire a bright blush;
- presence of follicles;
- increased hair growth (coarse and dark) in women according to the male type;
- stretch marks and decreased skin turgor in the abdominal area;
- weakness of muscle tissue;
- presence of hematomas;
- increased bone fragility;
- development of diabetes mellitus;
- problems in women with the menstrual cycle.
To make this diagnosis, it is necessary to undergo an examination, which includes a blood test for hormones (determining the level of cortisol in the blood), an MRI (to detect tumor formations of the pituitary gland) as well as computed tomography and ultrasound (to help find an adrenal tumor).
Treatment is aimed at removing tumor-like formations in the pituitary gland and adrenal glands. For Itsenko-Cushing disease, radiation therapy is performed. Drug treatment is not effective enough, so it is used as an adjuvant therapy in the treatment of Itsenko-Cushing syndrome and disease. X-rays will help in diagnosing pituitary adenoma. In this case, a picture of the sella turcica area is taken.
Manifestations and methods for diagnosing secondary hypertension
The symptoms of secondary hypertension are closely related to the disease that caused the increase in blood pressure. The main symptom that unites the whole mass of these ailments is considered to be a persistent increase in blood pressure, which is difficult to treat. Patients complain of a constant headache, noise in the head, pain in the occipital region, palpitations and chest pain, flashing “spots” before the eyes. In other words, the manifestations of secondary hypertension are very similar to the essential form of pathology.
Symptoms of pathology of other organs are added to high blood pressure. So, with renal hypertension, swelling, changes in the amount of urine excreted and its nature are a concern, fever, and lower back pain are possible.
Diagnosis of renal forms, as the most common ones, includes:
- Urine examination (quantity, circadian rhythm, character of sediment, presence of microbes);
- Radioisotope renography;
- X-ray contrast pyelography, cystography;
- Renal angiography;
- Ultrasonography;
- CT, MRI for probable space-occupying formations;
- Kidney biopsy.
Endocrine hypertension, in addition to the actual increase in pressure, is accompanied by sympathoadrenal crises, weakness in mice, weight gain, and changes in diuresis. With pheochromocytoma, patients complain of sweating, attacks of trembling and palpitations, general anxiety, and headache. If the tumor proceeds without crises, then fainting conditions are present in the clinic.
Damage to the adrenal glands in Conn's syndrome causes, against the background of hypertension, severe weakness, excessive amounts of urine, especially at night, and thirst. The addition of fever may indicate a malignant tumor of the adrenal gland.
Weight gain in parallel with the appearance of hypertension, decreased sexual function, thirst, itchy skin, characteristic stretch marks (striae), and carbohydrate metabolism disorders indicate a possible Itsenko-Cushing syndrome.
Diagnostic search for endocrine secondary hypertension implies:
- Complete blood count (leukocytosis, erythrocytosis);
- Study of carbohydrate metabolism indicators (hyperglycemia);
- Determination of blood electrolytes (potassium, sodium);
- Blood and urine tests for hormones and their metabolites in accordance with the suspected cause of hypertension;
- CT, MRI of the adrenal glands, pituitary gland.
Hemodynamic secondary hypertension is associated with pathology of the heart and blood vessels . They are characterized by an increase in predominantly systolic pressure. An unstable course of the disease is often observed, when an increase in blood pressure is replaced by hypotension. Patients complain of headache, weakness, discomfort in the heart area.
To diagnose hemodynamic forms of hypertension, the entire range of angiographic studies, ultrasound of the heart and blood vessels, and ECG are used; a lipid spectrum is required if atherosclerosis is suspected.
A large amount of information in such patients is provided by routine listening to the heart and blood vessels, which allows one to determine the characteristic murmurs over the affected arteries and heart valves. If neurogenic symptomatic hypertension is suspected, a thorough neurological examination is carried out, information about past injuries, neuroinfections, and brain surgeries is clarified.
Symptoms of hypertension in such patients are accompanied by signs of autonomic dysfunction, intracranial hypertension (headache, vomiting), and possible convulsions. The examination includes CT, MRI of the brain, assessment of neurological status, electroencephalography, possibly ultrasound and angiography of the cerebral vasculature.
Pheochromocytoma
During normal functioning of the adrenal glands, the hormones adrenaline and norepinephrine are produced. Pheochromocytoma is a disease associated with the uncontrolled production of adrenal hormones. This is caused by adrenal tumors. Malignant tumors occur in 8–10% of cases.
A feature of hypertension in pheochromocytoma is the frequent occurrence of hypertensive crises caused by a tumor (it releases substances into the blood that contribute to a sharp increase in pressure). During a crisis, a person experiences fear, panic attacks, nausea and vomiting.
In most cases, there is no sustained increase in blood pressure. Arterial hypertension is manifested by the following symptoms:
- headaches;
- pale skin;
- rapid, strong heartbeat;
- panic attacks.
Symptoms of the disease are varied, including nausea, pain in the abdomen and chest, slight tremors in the hands (tremor), decreased blood pressure with a sudden change in body position (to an upright position from a lying position), and decreased body weight.
Pheochromacytoma may be suspected if a person with hypertension does not progress on at least three blood pressure-lowering medications.
Diagnosis of the disease consists of blood and urine tests (large amounts of catecholamines are determined in it), biochemical analysis, ultrasound and computed tomography to detect a tumor.
It is necessary to constantly monitor the blood pressure level, since with this disease not only hypertension is observed, but also strong fluctuations in blood pressure values.
The only treatment that gives a positive result is surgery. Difficulties during surgical treatment are sudden jumps in blood pressure. After removal of the tumor, all symptoms quickly regress and a complete cure occurs. However, in 20–25% of patients after surgical treatment, the pressure level remains elevated. The reason for this may be the presence of primary arterial hypertension and nephropathy in patients.
“Not a disease, but a symptom”: what is symptomatic arterial hypertension?
Hypertension is one of the most common “diseases of civilization.” Its leading manifestation is an increase in blood pressure. However, there is a group of diseases that are also accompanied by high blood pressure.
With Nina Ananyevna Polyntsova, cardiologist at Clinic Expert Voronezh, we are talking about symptomatic arterial hypertension.
— Nina Ananyevna, what is symptomatic arterial hypertension?
-This is an increase in blood pressure, which is not an independent disease, but a symptom of diseases of other organs. These are the organs involved in regulating blood pressure. Symptomatic hypertension is also called secondary hypertension.
Symptomatic arterial hypertension is an increase
blood pressure, which is not independent
disease, but a symptom of diseases of other organs
— Is symptomatic arterial hypertension reflected in ICD-10?
- Yes. It is designated by code I15.
I15.0 – renovascular increase in blood pressure;
I15.1 – arterial hypertension in other kidney diseases;
I15.2 – secondary hypertension in endocrine pathology;
I15.8 – all other diagnosed types of secondary hypertension.
— How common is symptomatic arterial hypertension?
— According to statistics, it accounts for 5-10% of all cases of increased blood pressure.
— What types of symptomatic arterial hypertension are known?
— There are many symptomatic arterial hypertension. There are about 70 diseases manifested by high blood pressure. Some of them are more common, while others the doctor encounters very rarely in his practice.
According to the domestic classification, symptomatic arterial hypertension is divided into renal (nephrogenic), endocrine, hemodynamic, neurogenic, and iatrogenic.
- Renal (nephrogenic). It is divided into two options: with damage to the kidney tissue and kidney vessels. The first group includes pathologies such as pyelonephritis, glomerulonephritis, polycystic kidney disease, kidney damage due to diabetes mellitus (diabetic nephropathy), urolithiasis and a number of others. Pathologies of the renal vessels include stenosis (narrowing) of the renal artery (particularly due to atherosclerosis), fibrovascular dysplasia, and renal artery vasculitis.
What is the cause of increased blood pressure in renal pathology? With the fact that when this organ is damaged, substances (in particular renin) are produced that cause an increase in blood pressure.
— Endocrine symptomatic arterial hypertension. They, in turn, are divided into several subgroups:
a) adrenal gland. This organ secretes a number of hormones, the increased production of which can also cause an increase in blood pressure. Pathologies include Cushing's syndrome, hyperaldosteronism, pheochromocytoma;
b) pituitary: Cushing's disease;
c) thyroid (related to the thyroid gland). An increase in blood pressure in this case is associated with a disease such as thyrotoxicosis;
d) menopause (due to a lack of female sex hormones). It should also be noted that in the age period during which menopause occurs, hypertension is statistically more common. Therefore, it is not always easy to quickly determine whether we are talking about hypertension or symptomatic arterial hypertension caused by menopause.
What happens to a woman’s body after 40 years? Read about age-related changes in women through the eyes of a gynecologist in our article
— Hemodynamic arterial hypertension. They are associated with damage to certain vessels and the valvular apparatus of the heart. Increased blood pressure is caused by poor circulation.
Among the diseases are coarctation (narrowing) of the aorta at a certain level, heart defects (aortic valve insufficiency, patent ductus arteriosus), complete transverse heart block (one of the types of arrhythmias - heart rhythm disturbances).
More information about arrhythmias can be found here
— Neurogenic arterial hypertension. They are associated with damage to the central nervous system. Occurs with encephalitis, after traumatic brain injury, with severe disturbances in the circulation of cerebrospinal fluid.
— Iatrogenic arterial hypertension. They are caused, in particular, by taking medications. Some examples of such medications: nasal vasoconstrictor drops; inhalers that relieve bronchospasm; glucocorticoids; non-steroidal anti-inflammatory drugs; contraceptives (with long-term use) and others.
— How do symptomatic arterial hypertension manifest itself?
- Signs can be varied. Conventionally, two groups of manifestations can be distinguished:
- increased blood pressure and associated symptoms - such as nonspecific headaches, dizziness, palpitations, etc.;
- symptoms of the underlying disease.
Symptomatic arterial hypertension is observed more often in young people (younger than 20-30 years), or suddenly develops in old age (after 55-60 years).
These hypertensions are characterized by a rapid onset, a crisis course, or an initially persistent increase in blood pressure. Medicines that lower blood pressure are ineffective. According to statistics, among treatment-resistant, aggressive hypertension, 20% are symptomatic arterial hypertension.
There are high numbers of both systolic (upper) and diastolic (lower) pressure. However, there is also isolated systolic hypertension, when the upper pressure is increased, and the lower pressure is either normal or even less than normal. For example, such isolated low diastolic pressure occurs with aortic valve insufficiency: the more severe the insufficiency, the lower the diastolic pressure (in this case, there is an increase in the so-called pulse pressure - the difference between systolic and diastolic).
— How can symptomatic arterial hypertension be detected?
— Diagnostics is based on data obtained during a detailed interview and examination of the patient, and the results of laboratory and instrumental research methods.
Usually, tests such as a general clinical blood test, urine test, some parameters of a biochemical blood test (in particular, glucose, creatinine, cholesterol, potassium), ECG, EchoCG (ultrasound of the heart), and ultrasound of the kidneys are always prescribed.
Depending on the specific manifestations of the underlying disease, appropriate additional examinations are prescribed. For example, renal arterial hypertension can be suspected by a history of kidney pathology, changes in blood tests, and urine tests. According to the doctor's decision, instrumental diagnostics are also used: ultrasound, CT, MRI of the kidneys, intravenous urography, kidney biopsy.
If, against the background of high blood pressure, the patient complains of severe muscle weakness, a tingling sensation, goosebumps, thirst, and the release of large amounts of urine, hyperaldosteronism can be suspected. With it, in addition to the potassium level, it is necessary to study the content of sodium, renin and aldosterone. Ultrasound, CT, and MRI are also performed to detect pathological changes in the adrenal gland.
If the patient has lost weight, is bothered by trembling in his hands, has a sparkle in his eyes, and has bulging eyes, then thyrotoxicosis can be suspected. In this case, an ultrasound examination of the thyroid gland is performed to determine the level of a number of hormones - in particular TSH (pituitary hormone), triiodothyronine (T3) and thyroxine (T4) (thyroid hormones).
Suspicion of hemodynamic arterial hypertension may arise when a systolic murmur is detected during listening (auscultation) of the precordial region. With coarctation of the aorta, the upper part of the human body is well developed, while the lower part is worse, this difference is visible to the eye. With aortic valve insufficiency, high pulse pressure is observed. Cardiac ultrasound and ECG are of great help in establishing and clarifying the diagnosis.
The range of necessary studies in each specific case is determined by the doctor.
— How is symptomatic arterial hypertension treated?
— All patients receive medications that lower blood pressure. Today there are several groups of such drugs. Their choice depends on the underlying disease against which arterial hypertension developed. In addition, treatment of the underlying disease itself is carried out, including, if indicated, surgical treatment (for example, removal of a tumor of the adrenal cortex). If the cause is eliminated, blood pressure may return to normal.
Patients with symptomatic arterial hypertension must be treated by a cardiologist, and in addition to him, a doctor who treats the underlying disease
— Who treats symptomatic arterial hypertension?
— Treatment of symptomatic hypertension is the responsibility of different specialists. Such patients must be treated by a cardiologist, and in addition to him, a doctor who treats the underlying disease. This could be a urologist, nephrologist, endocrinologist, or surgeons of various profiles.
You can make an appointment with a cardiologist and other specialists here
ATTENTION: the service is not available in all cities
Interviewed by Enver Aliyev
The editors recommend:
Speculation about hypertension
The Ultimate Guide to High Blood Pressure: Frequently Asked Questions
When is daily blood pressure monitoring prescribed?
For reference:
Polyntsova Nina Ananyevna
Graduate of the Faculty of General Medicine of the Voronezh State Medical Institute in 1979.
In 1980, she completed an internship in surgery, and in 1986, a clinical residency in therapy.
In 1990, she underwent professional retraining in cardiology.
Doctor of the highest category.
Currently, he is a cardiologist at Clinic Expert Voronezh. Receives at the address: Pushkinskaya St., 11.
Primary hyperaldosteronism
In this case, there is an increase in the production of aldosterone in the adrenal glands. The causes of hypertension in this pathology are water retention in the body, which results in an increase in BCC (circulating blood volume).
Permanent hypertension, which is practically uncorrectable with conventional medications used to treat high blood pressure. It appears in 9% of patients suffering from this pathology.
This endocrine disease is characterized by weakness of muscle tissue, cramps, frequent and excessive urination.
The diagnosis is made on the basis of blood tests (the quantitative content of sodium, potassium, aldosterone in the blood is determined). The adrenal glands are examined using ultrasound and computed tomography.
Treatment of primary hyperaldosteronism is carried out with the drug Veroshpiron (Spironolactone). The dosage of the drug is determined by the attending physician. If the cause of the disease is a tumor formation, then surgical treatment is performed.
Pathology of the thyroid gland
This organ of the endocrine system produces the hormones thyroxine and triiodothyronine, which affect the growth of cellular structures and metabolism in general. An increase in blood pressure occurs both with increased thyroid function and with its decrease, but in both cases it has its own characteristics.
Hypothyroidism. A condition caused by insufficient production of thyroid hormones, the main causes of which are autoimmune damage, insufficient intake of iodine in the body, as well as partial or total removal of the thyroid gland due to injury or other pathological processes.
With hypothyroidism, there is an increase primarily in diastolic pressure, including at night, which is caused by a decrease in cardiac output, a decrease in heart rate, an increase in vascular resistance, and retention of water and sodium ions in the tissues. The clinical picture also reveals increased body weight, swelling, dry skin, hair loss, shortness of breath, drowsiness, decreased mood, attention, memory, interruptions in heart function, constipation, decreased libido.
With this disease, blood tests reveal a decrease in the concentration of thyroxine, triiodothyronine, and an increase in TSH.
Thyrotoxicosis. The main pathogenetic moment in the development of hypertension in this case is the formation and circulation in the blood of a large amount of thyroid hormones, causing an increase in cardiac output and an increase in heart rate. A feature of thyrotoxicosis is an almost isolated increase in systolic blood pressure with unchanged or decreased diastolic pressure.
Mental disorders are noteworthy: emotional instability, tearfulness, irritability, resentment, insomnia. Sexual dysfunction and other symptoms of metabolic disorders occur: sweating, weight loss, hair loss, exophthalmos, arrhythmias, palpitations, hand tremors, diarrhea.
Diagnosis is based on determining elevated levels of thyroid hormones in the blood.
Thyrotoxicosis
This disease is characterized by excess production of thyroid hormones. Causes of thyrotoxicosis:
- DTZ (diffuse toxic goiter);
- toxic adenoma;
- thyroiditis.
These hormones have a great influence on the heart and blood vessels. Which leads to tachycardia (increased heart rate), narrowing of the lumen of blood vessels. All these changes lead to the development of persistent symptomatic hypertension. The following symptoms are identified:
- irritability;
- sleep disturbance in the form of insomnia;
- weight change (weight loss);
- increased sweating;
- feeling of heat in the body;
- tremor of fingers.
A blood test for the hormones TSH, free T3 and free T4 will help confirm the diagnosis.
Once a diagnosis is made, drug treatment is prescribed. Treatment with thyreostatics is carried out. If conservative treatment is ineffective, treatment with a radioisotope or surgery is performed.
Neurogenic arterial hypertension;
ETIOLOGY AND PATHOGENESIS
TYPES OF ARTERIAL HYPERTENSION
According to the criteria of the initial pathogenetic link, changes in cardiac output, the type of increase in blood pressure and the nature of the clinical course, arterial hypertension is divided into several types. The initial link of the development mechanism. According to this criterion, general and local arterial hypertension are distinguished.
• General (systemic) arterial hypertension:
♦ Neurogenic arterial hypertension. Among them, a distinction is made between centrogenic and reflex (reflexogenic).
♦ Endocrine (hormonal). They develop as a result of endocrinopathies of the adrenal glands, thyroid gland, etc.
♦ Hypoxic (metabolic). There are ischemic (renal ischemic, cerebroischemic), venous-congestive and hypoxic (without a primary disturbance of hemodynamics in organs and tissues).
♦ Hemic (“blood”). Develop due to an increase in blood volume or viscosity.
• Local (regional) arterial hypertension. Change in cardiac output. There are hyper-, hypo- and eukinetic arterial hypertension.
• Hyperkinetic. Increased cardiac output (with normal or even decreased peripheral resistance).
• Hypokinetic. Cardiac output is reduced (with a significantly increased peripheral vascular resistance).
• Eukinetic. Normal cardiac output and increased
Type of blood pressure increase. Systolic, diastolic and mixed (systolic-diastolic) arterial hypertension are differentiated.
The nature of the clinical course. There are malignant and benign arterial hypertension.
• “Benign.” Occurs with slow development, an increase in both systolic and diastolic blood pressure; usually eukinetic.
• “Malignant.” Progress rapidly, with a predominant increase in diastolic blood pressure; as a rule, hypokinetic, less often - hyperkinetic (at the initial stage).
Risk factors for arterial hypertension: family history, obesity, diabetes, kidney disease, alcohol abuse, excessive consumption of table salt, stress, physical inactivity, smoking, patient's personality type.
These hypertensions are characterized by either an increase in hypertensive neurogenic effects, or a decrease in hypotensive neurogenic effects, or a combination of both. Neurogenic hypertension accounts for approximately half of all arterial hypertension. They are divided into reflex (reflexogenic) and centrogenic. Centrogenic arterial hypertension can occur either due to violations of the IRR or due to organic lesions of the brain structures that regulate systemic hemodynamics.
• Arterial hypertension caused by disorders of the internal nervous system (neurosis) is the result of repeated and prolonged stress with a negative emotional connotation, which causes a chain of interdependent progressive changes. The most important are:
♦ Overstrain and disruption of the main cortical nervous processes (excitation and active cortical inhibition), disruption of their balance and mobility.
♦ Development of a neurotic state and the formation of a cortical-subcortical excitation complex (excitation dominant).
This complex includes the sympathetic nuclei of the posterior hypothalamus, adrenergic structures of the reticular formation and the cardiovasomotor center.
♦ Increased tone of the walls of arterial and venous vessels, as well as the work of the heart, under the influence of catecholamines.
♦ At the same time, the hypothalamus-pituitary-adrenal system is activated. This is accompanied by an increase in the production and concentration in the blood of hormones with hypertensive effects (ADH, ACTH and corticosteroids, catecholamines, thyroid hormones).
♦ These substances potentiate the degree and duration of narrowing of arterioles and venules, increasing blood volume and cardiac output. This leads to a persistent increase in blood pressure—arterial hypertension develops.
The links in pathogenesis described above are also characteristic of the initial stages of hypertension.
• Arterial hypertension caused by damage to brain structures involved in the regulation of blood pressure.
♦ The most common causes: brain injury, encephalitis, strokes, tumors of the brain or its membranes, and impaired blood supply to the brain (cerebroischemic hypertension).
♦ General pathogenesis. These causes directly damage the structures involved in the regulation of blood pressure (sympathetic nuclei of the hypothalamus, reticular formation, cardiovasomotor center). Subsequent links of pathogenesis are similar to the mechanisms of development of arterial hypertension in neuroses.
Reflex arterial hypertension can develop on the basis of conditioned and unconditioned reflexes.
• Conditioned reflex arterial hypertension.
♦ Cause: repeated combination of indifferent (conditioned) signals (for example, information about an upcoming public speech, an important competition or event) with the action of agents that cause an increase in blood pressure (for example, caffeine, alcohol or drugs). After a certain number of combinations, an increase in blood pressure is registered only in response to an indifferent signal and a persistent increase in blood pressure may develop.
• Unconditioned reflex arterial hypertension.
♦ Cause: chronic irritation of extra- and intrareceptors, nerve trunks and nerve centers (for example, with long-term causalgic syndromes, encephalitis, brain tumors). These conditions contribute to the cessation of “depressor” afferent impulses to the cardiovasomotor (pressor) center. An increase in the tone of the latter causes a persistent increase in blood pressure.
Hyperthyroidism
Causes of hyperthyroidism:
Diffuse toxic goiter.
Consequences of treatment of diffuse toxic goiter.
Incorrect calculation of the dosage of drugs with thyroid hormones (overdose).
The clinical picture of hyperthyroidism is quite diverse. A person may complain of palpitations, shortness of breath, as well as increased fatigue and weakness. There is hyperactivity, mood swings, increased appetite and at the same time weight loss. Women experience menstrual irregularities – oligomenorrhea (increased interval between menstruation).
The following objective signs are distinguished:
- cardiopalmus;
- increased blood pressure;
- increased body temperature;
- skin moisture;
- the upper eyelid may lag behind when looking down;
- pulsation in the region of the heart.
Patients with hyperthyroidism may develop complications such as myocardial infarction, angina pectoris and atrial fibrillation.
The diagnosis is made based on complaints, examination, auscultation, palpation and laboratory blood tests.
Treatment is carried out in two directions - correction of endocrine functions and symptomatic treatment.
Kidney type
As the name suggests, they talk about dysfunction of the excretory system as the basis of the disease.
In itself, this type of symptomatic increase in blood pressure is not uniform. Careful division makes it possible to name two more subtypes.
Renovascular hypertension
Occurs most often. Caused by a decrease in the quality of blood flow. The amount of liquid connective tissue reaching the kidney decreases. Filtration intensity is insufficient.
The body seeks to compensate for the violation. Excess prehormone renin is produced. Together with angiotensin and aldosterone, it acts as a regulator of blood pressure.
Excessive amounts of this substance lead to vasospasm. The lumen of the arteries narrows, making it more difficult for blood to move. The tonometer readings are growing significantly.
Among the reasons for the violation are:
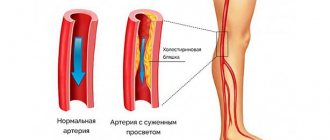
- Atherosclerosis. The most common option. It consists of low vascular patency due to blockage by cholesterol plaques.
- Thrombosis. The process is similar, only the occlusion is observed not by lipid structures, but by blood clots.
- Inflammation of the renal parenchyma and pelvis. We can talk about both classic pyelonephritis and autoimmune processes. Diagnosis of such conditions is not difficult.
Slightly less common is compression of the renal arteries by tumors, space-occupying formations, and vasculitis (inflammation of the walls of blood vessels and their subsequent scarring, or even fusion).
Clinical signs are characteristic:
- Strong headache. In the back of the head. Accompanies all forms of hypertension, so it is impossible to say exactly what was the cause without a thorough, thoughtful diagnosis. The intensity of the syndrome is extremely high. The patient takes a forced lying position in order to somehow alleviate the condition.
- Nausea, vomiting. Negative sign. Indicates increasing ischemic phenomena in cerebral structures.
- Weakness, drowsiness. General asthenia. They accompany the patient constantly, again directly indicating a violation of normal trophism of the brain.
- The small difference between the upper and lower pressure is 10-20 mmHg. Art.
Usually, this is where the neurological symptoms end, apart from rare exceptions.
Almost always there are renal manifestations, such as pain, disturbances in normal urination, and others.
Typical signs of the renovascular form of hypertension: early onset in women (before 30 years) and later in men (after 50), absence of a crisis course, approximate evenness of the patient’s condition throughout the process, resistance to treatment, predominant increase in lower (diastolic) pressure.
Both forms of secondary arterial hypertension can acquire a malignant course. A kind of ongoing crisis.
Standard therapeutic methods do not make sense; intensive treatment of the root cause is required.
Read more about the renovascular form of hypertension here.
Renoparenchymatous form
It occurs much less frequently.
The fundamental difference from the previous one is the lack of connection with the amount of blood entering the kidney. An increase in renin concentration is due to the inflammatory process.
Only a specialist can distinguish one from the other, and not immediately, but based on the results of a laboratory evaluation of urine, ultrasound diagnostics, scintigraphy, and possibly MRI.
The clinical picture is identical: there is a persistent increase in blood pressure against the background of renal symptoms: edema, lower back pain, and disturbances in the urination process.
Both varieties are dangerous to health and life. Urgent treatment is required to avoid complications. These include stroke (in 80% of cases) and heart attack. Against the background of a pronounced disorder, extensive types of deviations are likely.
In both cases, the treatment is inpatient. With the use of large combined doses of antihypertensive drugs, surgical intervention if necessary).
Antibiotics, diuretics, and hormonal drugs (Prednisolone, Dexamatezone) are used. Hospitalization lasts until the condition is completely corrected.
Hypothyroidism
A noticeable increase in diastolic pressure is observed in 15–20% of cases of hypothyroidism. To identify this disease, electrocardiography is performed, which detects specific changes, and also determines the level of hormones in the blood (increased TSH levels).
Levothyroxine is prescribed to treat hypothyroidism. Thyroid hormones are used to correct symptomatic arterial hypertension. If blood pressure does not decrease with prescribed treatment, it is recommended to take diuretics and angiotensin-converting enzyme inhibitors.
Neurogenic form
Partially overlaps with the endocrine one, but not always. A classic example of adjacent symptomatic hypertension is a tumor or mass in the chiasmal-sellar region.
For example, adenoma, germinoma, glioma of the posterior pituitary gland, craniopharyngioma, Rathke's pouch cyst and others.
A dual process develops: on the one hand, the neoplasm itself compresses the cerebral structures, provokes an increase in intracranial pressure, and hence unstable hormone production, on the other, key centers are involved that produce specific substances to stimulate the activity of the entire endocrine system.
Secondary arterial hypertension is not always caused by tumors; infections of cerebral tissues (encephalitis, meningitis) and previous injuries are possible.
The presence of vascular protrusions (aneurysms) and arteriovenous malformations affects.
The symptoms are pronounced, clearly visible and extremely varied. Typical manifestations of hypertension are identical: from headache to nausea, vomiting, weakness. The difference is in the nature of the pain syndrome.
If the mass formation reaches a significant size and begins to compress the brain tissue, the intensity is higher.
Third-party manifestations have several levels: mental disorders (apathy, depressive mood, emotional lability, mental impairment, memory lapses or problems with remembering), a neurogenic component (in addition to those already mentioned - focal signs, depending on the location of the lesion, for example, when the occipital region is involved lobes, visual dysfunctions occur, etc.).
Therapy is mainly surgical when it comes to tumors. When symptoms appear, there are not many options left.
Compression is taking place, the expansive spread of the mass effect will only increase. Removal of the tumor is required.
In the case of prolactinomas (pituitary adenomas that produce the hormone of the same name), medications can be used. Often such neoplasia regresses against the background of conservative intervention.
Inflammatory processes are eliminated with large doses of antibiotics. The blood-brain barrier causes variable effectiveness of treatment tactics for encephalitis or meningitis.
Hyperparathyroidism
This disease has no specific symptoms. It is manifested by weakness, fatigue and disruption of the digestive tract. Very often, secondary hypertension is the only manifestation of the disease. An increase in blood pressure occurs due to an increase in calcium levels in the blood. Parathyroid hormone levels are reduced.
Treatment is surgical - the parathyroid gland is removed. The blood pressure normalizes when the calcium and parathyroid hormone levels in the body normalize.
Neurogenic arterial hypertension
These hypertensions are characterized by either an increase in hypertensive neurogenic effects, or a decrease in hypotensive neurogenic effects, or a combination of both. Neurogenic hypertension accounts for approximately half of all arterial hypertension. They are divided into reflex (reflexogenic) and centrogenic. Centrogenic arterial hypertension can occur either due to violations of the IRR or due to organic lesions of the brain structures that regulate systemic hemodynamics.
• Arterial hypertension caused by disorders of the internal nervous system (neurosis) is the result of repeated and prolonged stress with a negative emotional connotation, which causes a chain of interdependent progressive changes. The most important are:
♦ Overstrain and disruption of the main cortical nervous processes (excitation and active cortical inhibition), disruption of their balance and mobility.
♦ Development of a neurotic state and the formation of a cortical-subcortical excitation complex (excitation dominant).
This complex includes the sympathetic nuclei of the posterior hypothalamus, adrenergic structures of the reticular formation and the cardiovasomotor center.
♦ Increased tone of the walls of arterial and venous vessels, as well as the work of the heart, under the influence of catecholamines.
♦ At the same time, the hypothalamus-pituitary-adrenal system is activated. This is accompanied by an increase in the production and concentration in the blood of hormones with hypertensive effects (ADH, ACTH and corticosteroids, catecholamines, thyroid hormones).
♦ These substances potentiate the degree and duration of narrowing of arterioles and venules, increasing blood volume and cardiac output. This leads to a persistent increase in blood pressure—arterial hypertension develops.
The links in pathogenesis described above are also characteristic of the initial stages of hypertension.
• Arterial hypertension caused by damage to brain structures involved in the regulation of blood pressure.
♦ The most common causes: brain injury, encephalitis, strokes, tumors of the brain or its membranes, and impaired blood supply to the brain (cerebroischemic hypertension).
♦ General pathogenesis. These causes directly damage the structures involved in the regulation of blood pressure (sympathetic nuclei of the hypothalamus, reticular formation, cardiovasomotor center). Subsequent links of pathogenesis are similar to the mechanisms of development of arterial hypertension in neuroses.
Reflex arterial hypertension can develop on the basis of conditioned and unconditioned reflexes.
• Conditioned reflex arterial hypertension.
♦ Cause: repeated combination of indifferent (conditioned) signals (for example, information about an upcoming public speech, an important competition or event) with the action of agents that cause an increase in blood pressure (for example, caffeine, alcohol or drugs). After a certain number of combinations, an increase in blood pressure is registered only in response to an indifferent signal and a persistent increase in blood pressure may develop.
• Unconditioned reflex arterial hypertension.
♦ Cause: chronic irritation of extra- and intrareceptors, nerve trunks and nerve centers (for example, with long-term causalgic syndromes, encephalitis, brain tumors). These conditions contribute to the cessation of “depressor” afferent impulses to the cardiovasomotor (pressor) center. An increase in the tone of the latter causes a persistent increase in blood pressure.
93.79.221.197 © studopedia.ru Not the author of the materials posted. But it provides the opportunity to use it for free. Is there a copyright violation? Write to us | Feedback.
Disable adBlock! and refresh the page (F5)
very necessary
How does SAG manifest?
The most indicative symptom of hypertension is persistently high blood pressure or frequent pressure surges. All other symptoms are secondary, and different patients exhibit their own set of symptoms. For example, one person simply experiences increased pressure, a headache, and an inexplicable feeling of anxiety. Another person, in addition to increasing values on the tonometer, experiences nausea and even vomiting, his face turns red, and his fingers tremble.
Common symptoms of SAH include:
- Dizziness that occurs suddenly;
- Constant feeling of fatigue, weakness, powerlessness;
- The appearance of attacks of obsessive nausea and, in some cases, vomiting;
- Development of pain in different parts of the head;
- Psycho-emotional status disorders;
- An increase or, conversely, a decrease in body temperature;
- Pain behind the sternum;
- Tinnitus (in one ear);
- Swelling of the face;
- Rapid pulse.
Surveys of patients show that they sometimes suffer from panic attacks - they are overcome by the fear of death, they sweat intensely, and their heartbeat increases. Panic attacks are not unique to hypertension, but, of course, this symptom cannot be ignored.
Like a rapid pulse, it is too common a symptom to make any diagnoses based on it alone. Sometimes it's just excitement, and sometimes it's a really worrying sign. But it shouldn’t scare you: fear doesn’t solve anything, but a timely trip to the doctor can save you from serious problems.
Pathology of the adrenal glands
Hypertension caused by diseases of the adrenal glands accounts for at least half of all endocrine hypertension, since the hormones they produce - catecholamines and corticosteroids - are directly involved in the regulation of blood pressure. Among the diseases of the adrenal glands that cause secondary hypertension are the following:
Pheochromocytoma. This is a tumor formed from the adrenal medulla (less often from chromaffin cells located outside the adrenal glands), producing catecholamines (adrenaline and norepinephrine) - hormones that are of paramount importance in the regulation of blood pressure, increasing the tone of the vascular wall, causing vasoconstriction, and an increase in cardiac output. This type of tumor rarely causes hypertension, in less than 0.2 percent of clinical cases.
Increased pressure in pheochromocytoma often has a crisis course, in some cases - against the background of permanently increased pressure. Crises with pheochromocytoma are caused by a sharp release of large amounts of hormones into the blood and occur with intense headaches and tachycardia. As a rule, they are provoked by a stressful situation, heavy food intake and are accompanied by a feeling of palpitations, increased sweating, changes in complexion (redness or paleness), hand tremors, fear of death, psychomotor agitation, abdominal and lower back pain. Arterial hypertension in this disease often cannot be corrected with medications.
Preeclampsia: SAH with alarming frequency
Preeclampsia, otherwise called late toxicosis, is a common and dangerous complication of pregnancy. It is very difficult to predict this pathology - there are, of course, categories of expectant mothers who are more susceptible to it, but absolutely no one is immune.
You can understand what kind of complication this is by answering the most common and important questions:
- How is gestosis related to increased blood pressure? Often, high blood pressure is the only obvious sign of gestosis. For some time, the woman herself does not understand what is happening to her - she feels bad, her heart beats faster, her face turns red, there is a noise in her ears, and her head begins to hurt. And if a one-time incident does not worry much, then a recurring condition already worries the pregnant woman. It is not so rare to discover gestosis by accident: during each visit to the gynecologist, the patient’s blood pressure is measured, and if the numbers on the tonometer are high, the doctor will first of all suspect gestosis.
- What other symptoms indicate gestosis? Protein in the urine is detected during testing; this is the first sign of nephropathology. Weight gain is also a symptom, and women who enter pregnancy with excess weight are already at risk. Swelling of peripheral tissues is not always associated with gestosis, but still very common, so as not to consider this option.
- Why is it dangerous? Because it develops differently. There are mild degrees of gestosis, and there are also deadly ones. For example, dropsy is easy to treat - apart from swelling, the woman actually does not complain about anything else. But with nephropathy, you need to act quickly and accurately so that this borderline stage does not develop into preeclampsia. In this state, the pressure increases significantly, and the pregnant woman suffers from headaches. Blood flow in the brain is disrupted; the pregnant woman's muscles may contract convulsively, which can lead to premature birth.
- Preeclampsia and eclampsia - what is the connection? Eclampsia is the most severe form of gestosis. If the patient does not receive emergency medical care, even death is possible. Loss of consciousness, leading to a comatose state of the pregnant woman, is possible. High blood pressure threatens placental abruption, as well as serious pathologies of the liver and kidneys.
The only way to reliably cure gestosis is to deliver the patient. And if in mild forms there is no urgency in this, then threatening conditions force doctors to take this measure. As a rule, after childbirth the blood pressure returns to normal. If a pregnant woman's blood pressure rises, this does not mean that she has become a chronic hypertensive patient. This is precisely symptomatic hypertension, a secondary disease caused by malnutrition of cells and tissues.
Diagnostics
The presence of stable hypertension implies a complete examination of the patient immediately after diagnosis to exclude symptomatic hypertension. If the diagnosis of symptomatic arterial hypertension confirms suspicions, it is necessary to determine the stage of hypertension, the degree of risk and the form of the underlying disease. The examination takes place in two stages.
At the first stage, the patient undergoes mandatory studies, including assessment of the degree of organ damage, methods for excluding secondary hypertension, diagnosis of accompanying clinical manifestations and possible cardiovascular complications.
- Taking an anamnesis is a thorough interview of the patient who has been diagnosed with hypertension for the first time, and analysis of all information about previous diseases and existing pathologies, namely:
- the duration of arterial hypertension in the anamnesis and the maximum pressure values, the results of past therapy, the presence of hypertensive crises in the anamnesis;
- information about the presence of signs of coronary artery disease (coronary heart disease), gout, central nervous system lesions, heart failure, diabetes mellitus, lipid metabolism disorders, peripheral vascular lesions, broncho-obstructive and renal diseases;
- information about medications taken to treat existing diseases, especially if they can provoke an increase in blood pressure;
- search for specific symptoms characteristic of secondary hypertension (youth, sweating, tremor, increased creatinine, retinopathy, spontaneous hypokalemia);
- gynecological history of the patients: increased blood pressure as a result of menopause, pregnancy, hormonal contraception or hormone replacement therapy;
- analysis of the patient’s lifestyle, this includes assessment of physical activity, quantitative assessment of tobacco smoking, alcohol consumption, fatty and salty foods, collection of data on weight fluctuations throughout life;
- personality and mental characteristics, level of education, family and work environment and other external factors that cannot be excluded when identifying the causes of hypertension;
- family history of hypertension, coronary artery disease, stroke, kidney disease, lipid metabolism disorders, diabetes mellitus.
- Objective research consists of several steps:
- calculating body mass index, which will require the patient’s weight and height;
- assessment of the size of the heart, the general condition of the cardiovascular system, the presence of murmurs, signs of coarctation of the aorta or heart failure (swelling of internal organs, enlarged liver, wheezing in the lungs), palpation of the pulse in the peripheral arteries;
- palpation of the kidneys, detection of noise in the arteries and search for space-occupying formations.
- Laboratory and instrumental studies in the diagnosis of symptomatic arterial hypertension:
- general analysis of urine and blood;
- blood test for cholesterol, glucose, potassium, creatinine;
- chest x-ray;
- ECG;
- Ultrasound of the abdominal organs;
- fundus examination.
As for the second stage, the form of symptomatic arterial hypertension is specified here.
- Special examinations to establish secondary hypertension.
- Additional methods assessing the degree and risk factors, as well as damage to certain organs. They are used if the risk is reduced as a result:
- Ultrasound of peripheral vessels;
- EchoCG – most accurately detects left ventricular hypertrophy, and the method is used only if X-ray examination and ECG fail;
- determination of triglyceride levels and lipid spectrum.
Treatment of SAH
Arterial hypertension, due to its symptomatic nature, requires not only therapy aimed at stabilizing blood pressure, but also parallel treatment of the disease that provoked this problem.
- Etiological treatment is to eliminate the cause of hypertension. The operation is indicated in the presence of coarctation of the aorta, pathology of the renal vessels, and hormonally active adrenal adenoma. Specifically, this applies to diagnoses such as pheochromocytoma, corticosteroma, adrenal adenocarcinoma, hypernephroid kidney cancer, and aldosterone-producing adenoma. Pituitary adenoma requires active intervention through laser treatment, radiotherapy and x-ray therapy, and sometimes surgery is indicated. Drug therapy aimed at eliminating the underlying disease (erythremia, urinary tract infection, periarteritis nodosa, congestive heart failure, etc.) usually shows a favorable prognosis for hypertension.
- Antihypertensive drug therapy – in conjunction with eliminating the etiology, treatment with antihypertensive drugs should be carried out. Persistent hypertension in combination with kidney damage is treated with diuretics (Furosemide, Hypothiazide, Triampur Compositum, Triamterene) along with ACE inhibitors. Insufficient hypotensive effect that can compensate for peripheral vasodilators and p-blockers. Combination treatment, combining several drug groups, can only be used for stable hypertension of any origin. A sharp decrease in pressure during prolonged arterial hypertension is contraindicated for elderly people due to the possible deterioration of renal, cerebral and coronary circulation. You can normalize cerebral vascular tone and improve the regulation of nervous processes with the help of caffeine and cordiamine, especially in the morning, when blood pressure has not yet increased too much.
Differential diagnosis
To identify the cause of symptomatic hypertension, the doctor needs to collect as accurately as possible an anamnesis of the patient’s illness and life (identify information about previous diseases, injuries, hereditary predisposition). Blood pressure measurements should be taken repeatedly (at home and in the hospital), and the patient should keep a special diary in which he records blood pressure readings.
To identify the cause of a rise in blood pressure, the patient may be prescribed the following types of laboratory and instrumental studies:
- Analysis of urine;
- general and biochemical blood tests;
- blood test for hormones;
- ECG;
- Ultrasound of the kidneys and renal vessels;
- Echo-CG;
- vascular angiography;
- CT.
After identifying abnormalities and analyzing the diagnostic results, the patient may be prescribed additional research methods:
- electroencephalography;
- rheoencephalography;
- Ultrasound of cerebral vessels;
- intravenous urography;
- radiography of renal vessels;
- isotope renography;
- selective phlebography of the adrenal glands;
- kidney biopsy;
- study of daily excretion of potassium and sodium in urine;
- blood tests to determine the level of angiotensin and renin;
- urine culture according to Gould et al.
Prevention of SAH
Secondary hypertension can also be prevented, and there is nothing difficult or impossible in preventing the disease.
7 points for the prevention of secondary arterial hypertension:
- Rules for healthy eating instead of diets. First, it is recommended to take a test for overeating: perhaps the fact is that you do not have the principle of moderation in eating. Then you have to determine how many meals a day you should have: some people eat strictly three times a day, no snacking, and that's fine. There should always be breakfast - don't replace it with a cup of coffee. Breakfast is always hearty and nutritious, but it is not the same as fatty and heavy. A complete lunch: protein and vegetables. Dinner is the same: raw vegetables, grilled, or in a salad, plus lean protein (chicken, turkey, beef, rabbit) or any fish or seafood.
- Must-haves to fuel the body. This can include various bioactive complexes and biological food additives. Today, it's easy to find lists specifically for women that include curcumin, fish oil, raw probiotics, collagen, etc. There are lists for maintaining men's health - these are sunflower lecithin, Omega-3, vitamin D, etc. Vitamin-mineral complexes and dietary supplements, when chosen wisely, help to avoid age-related diseases, deterioration of the condition of tissues and organs, and immune failures.
- Sports and physical education are our everything. For many, the topic of healthy lifestyle is unpleasant to the point of grinding teeth, but there is no need to treat it as something intrusive and complicated. 7000-8000 steps a day, which you record with a pedometer - and you are already on the move, already “running away” from hypertension. Find your version of physical activity.
- To give up smoking. No matter how much we talk about it, in the minds of many people this question is impenetrable. Today, people in their early thirties are forced to take blood thinners because their body has wasted its resources prematurely due to smoking.
- Ability to withstand stress. This was mentioned above, but it can be repeated - stress is not just a bad mood, apathy, or a pessimistic scenario. These are special reactions in brain structures that lead to disruptions in the regulation of important processes in your body.
- Timely diagnosis. This point has nothing to do with well-being. Both people of modest means and wealthy patients often equally dislike visiting doctors. Even when nothing worries you - just getting tested, appearing to specialists is something extremely complicated for them. But this is an indicator of immaturity and irresponsibility. And your state of health will definitely remind you of this.
- Life is like joy. Not a single physician would argue with the fact that recovery and the ability to maintain one’s health capital also depend on the patient’s worldview, sense of humor, and ability to correctly live through various situations. Some give up even before they start treatment - they become depressed from completely treatable diagnoses, feel sorry for themselves and do not take constructive steps. And doctors will also note that cheerful people who know how to treat themselves and the world around them with irony endure even complex treatment more easily, they are more active and less fixated on living through their suffering.
Probably, you can add a few more points to this list, but even if you think carefully about each of them, you will push the danger of developing hypertension a little away from yourself.
Neurogenic type
Causes
This type of symptomatic hypertension is very similar to endocrine hypertension. Increased pressure can be caused by tumors or neoplasms in the pituitary gland.
The tumor affects the cerebral structures, leads to an increase in intracranial pressure, the thyroid gland begins to produce hormones with disturbances, which leads to a persistent increase in blood pressure.
Neurogenic symptomatic hypertension can be triggered by infectious diseases of cerebral structures and brain injury.
A pituitary tumor can cause neurogenic hypertension
Symptoms
The neurogenic type of symptomatic hypertension is easily recognized by its characteristic symptoms:
- neuropsychiatric disorders;
- apathy;
- depression;
- unstable mood;
- disturbance of mental activity;
- memory loss;
- neurogenic disorders.
The symptoms are clearly manifested; in addition to the specific symptoms, general symptomatic manifestations of high blood pressure are added: headaches, vomiting, loss of strength. Pain in neurogenic symptomatic hypertension is more pronounced.
Diagnosis and treatment
Treatment of symptomatic arterial hypertension of the neurogenic type requires surgical intervention. Any tumors must be excised so that blood pressure returns to normal.
In case of adenoma or hormonal imbalances, the doctor prescribes hormonal medications. Antibiotics are prescribed for inflammation.