© Author: Z. Nelly Vladimirovna, doctor of the first qualification category, especially for SosudInfo.ru (about the authors)
Coronary heart disease (CHD) has become a serious social problem, because most of the world's population has one or another of its manifestations. The fast pace of life in megacities, psycho-emotional stress, and consumption of large amounts of fat in food contribute to the onset of the disease, and therefore it is not surprising that residents of developed countries are more susceptible to this problem.
IHD is a disease associated with changes in the walls of the arterial vessels of the heart by cholesterol plaques, which ultimately leads to an imbalance between the needs of the heart muscle for substances necessary for metabolism and the possibilities of their delivery through the heart arteries. The disease can be acute or chronic; it has many clinical forms, differing in symptoms and prognosis.
Despite the emergence of various modern treatment methods, IHD still occupies a leading position in the number of deaths in the world. Often, cardiac ischemia is combined with the so-called ischemic brain disease, which also occurs with atherosclerotic damage to the vessels that supply it with blood. A fairly common ischemic stroke, in other words, cerebral infarction, is a direct consequence of atherosclerosis of the cerebral vessels. Thus, the common causes of these serious diseases also determine their frequent combination in the same patient.
Main cause of coronary artery disease
In order for the heart to deliver blood to all organs and tissues in a timely manner, it must have a healthy myocardium, because many biochemical transformations necessary to perform such an important function occur there. The myocardium is equipped with vessels called coronary vessels, through which “food” and breathing are delivered to it. Various influences that are unfavorable for the coronary vessels can lead to their failure, which will lead to disruption of blood flow and nutrition of the heart muscle.
Modern medicine has studied the causes of coronary heart disease quite well. With increasing age, under the influence of the external environment, lifestyle, dietary habits, as well as in the presence of a hereditary predisposition, the coronary arteries are damaged by atherosclerosis. In other words, protein-fat complexes are deposited on the walls of the arteries, which over time turn into an atherosclerotic plaque, which narrows the lumen of the vessel, disrupting the normal blood flow to the myocardium. So, the immediate cause of the development of myocardial ischemia is atherosclerosis.
Video: IHD and atherosclerosis
Signs of prolonged asphyxia and severe ischemia in newborns
- Low Apgar scores (0-3) after the first 5 minutes of life
- Coma, absence of tendon reflexes and muscle tone
- Disorders of internal organs (kidneys, lungs, liver, heart)
The degree of cerebral ischemia is determined by the doctor after examining the child; this figure should appear in the discharge diagnosis. Initial data on the baby’s condition are obtained immediately after birth using the Apgar scale:
| Sign | 0 points | 1 point | 2 points |
| Heart rate | Absent | Slow (less than 100 beats per minute) | More than 100 beats per minute |
| Attempts to breathe | Absence | Weak squeaking, insufficient ventilation of the lungs | Strong scream |
| Muscle tone | Muscles are relaxed | Limbs are slightly bent | Limbs bend well, movements are active |
| Vivacity of reflexes (to irritation of the foot) | None | Grimaces on the face | Scream |
| Color of the skin | Blue, pale | Pink body, bluish limbs | The whole baby is pink |
The baby's condition is recorded 1 and 5 minutes after birth. After 1 minute, the need for resuscitation is determined by the number of points. Scores at 5 minutes reflect to some extent hypoxic brain damage (if any).
When do we take risks?
Risk factors are conditions that pose a threat to the development of the disease, contribute to its occurrence and progression. The main factors leading to the development of cardiac ischemia are:
- Increased cholesterol levels (hypercholesterolemia), as well as changes in the ratio of various lipoprotein fractions;
- Eating disorders (abuse of fatty foods, excessive consumption of easily digestible carbohydrates);
- Physical inactivity, low physical activity, reluctance to play sports;
- The presence of bad habits such as smoking, alcoholism;
- Concomitant diseases accompanied by metabolic disorders (obesity, diabetes mellitus, decreased thyroid function);
- Arterial hypertension;
- Age and gender factors (it is known that IHD is more common in older people, and also in men more often than in women);
- Features of the psycho-emotional state (frequent stress, overwork, emotional overstrain).
As you can see, most of the above factors are quite banal. How do they influence the occurrence of myocardial ischemia? Hypercholesterolemia, nutritional and metabolic disorders are prerequisites for the formation of atherosclerotic changes in the arteries of the heart. In patients with arterial hypertension, against the background of pressure fluctuations, vascular spasm occurs, which damages their inner lining, and hypertrophy (enlargement) of the left ventricle of the heart develops. It is difficult for the coronary arteries to provide sufficient blood supply to the increased myocardial mass, especially if they are narrowed by accumulated plaque.
It is known that smoking alone can increase the risk of death from vascular diseases by about half. This is explained by the development of arterial hypertension in smokers, an increase in heart rate, increased blood clotting, as well as increased atherosclerosis in the walls of blood vessels.
Risk factors also include psycho-emotional stress. Some personality traits that have a constant feeling of anxiety or anger, which can easily cause aggression towards others, as well as frequent conflicts, lack of mutual understanding and support in the family, inevitably lead to increased blood pressure, increased heart rate and, as a result, increased need myocardium in oxygen.
Video: occurrence and course of ischemia
Does everything depend on us?
There are so-called non-modifiable risk factors, that is, those that we cannot influence in any way. These include heredity (the presence of various forms of IHD in the father, mother and other blood relatives), old age and gender. In women, various forms of IHD are observed less frequently and at a later age, which is explained by the peculiar effect of female sex hormones and estrogens, which prevent the development of atherosclerosis.
In newborns, small children and adolescents, there is practically no sign of myocardial ischemia, especially those caused by atherosclerosis. At an early age, ischemic changes in the heart can occur as a result of spasm of the coronary vessels or developmental defects. Ischemia in newborns most often affects the brain and is associated with disturbances during pregnancy or the postpartum period.
It is unlikely that each of us can boast of excellent health, constant adherence to a diet and regular exercise. Heavy workload, stress, constant rush, inability to eat balanced and regularly are frequent companions of our daily rhythm of life.
It is believed that residents of megacities are more prone to developing cardiovascular diseases, including ischemic heart disease, which is associated with high stress levels, constant overwork and lack of physical activity. However, it would be nice to visit the pool or gym at least once a week, but most of us will find a lot of excuses not to do this! Some people don’t have time, others are too tired, and a sofa with a TV and a plate of homemade delicious food on a day off beckons with incredible force.
Many people do not attach significant importance to lifestyle, so clinic doctors need to promptly identify risk factors in patients at risk, share information about the possible consequences of overeating, obesity, a sedentary lifestyle, and smoking. The patient must clearly understand the outcome that can result from ignoring the coronary vessels, so as they say: forewarned is forearmed!
Cardiopathy - heart pathology in children
The term “cardiopathy” comes from the Greek words kardia - heart and pathos - disease.
There are two meanings of this concept: in the broad sense of the word, it means any cardiac pathology, including those of unknown origin. In the narrow sense, it is used most often to indicate disorders of myocardial development. In this regard, the diagnosis of cardiopathy is often made in children.
It is especially common in newborns (posthypoxic cardiopathy) and children 7–12 years old.
The causes of this disease are varied and depend on the type and form of the pathology. There are congenital and acquired cardiopathy. Congenital develops as a result of certain genetic disorders, which can phenotypically manifest themselves in the form of heart defects, connective tissue dysplasia, and systemic vasculitis.
Acquired cardiopathy is the result of exposure to unfavorable external factors: infectious agents (microorganisms that cause myocarditis, endocarditis, etc.), hormonal changes in the body, stress, excessive physical activity, etc.
The term “cardiopathy” comes from the Greek words kardia - heart and pathos - disease. There are two meanings of this concept: in the broad sense of the word, it denotes any cardiac pathology, including those of unknown origin. In the narrow sense, it is used, most often, to denote disorders of myocardial development. In this regard, the diagnosis of cardiopathy is often made in children. It is especially common in newborns (posthypoxic cardiopathy) and children 7–12 years old.
Prich
The symptoms of this disease are varied and depend on the type and form of the pathology. There are congenital and acquired cardiopathy. Congenital develops as a result of certain genetic disorders, which can phenotypically manifest themselves in the form of heart defects, connective tissue dysplasia, and systemic vasculitis.
Types and forms of coronary heart disease
Currently, many types of coronary heart disease are known. The classification of IHD, proposed in 1979 by a WHO expert working group, still remains relevant and is used by many doctors. It is based on the identification of independent forms of the disease, which have unique characteristic manifestations, a certain prognosis and require a special type of treatment. Over time and the advent of modern diagnostic methods, other forms of IHD were studied in detail, which is reflected in other, newer classifications.
Currently, the following clinical forms of IHD are distinguished, which are presented:
- Sudden coronary death (primary cardiac arrest);
- Angina (here we distinguish such forms as angina pectoris and spontaneous angina);
- Myocardial infarction (primary, repeated, small-focal, large-focal);
- Post-infarction cardiosclerosis;
- Circulatory failure;
- Heart rhythm disturbances;
- Painless myocardial ischemia;
- Microvascular (distal) ischemic heart disease
- New ischemic syndromes (“stunning” of the myocardium, etc.)
To statistically record the incidence of coronary heart disease, the International Classification of Diseases, X revision, is used, with which every doctor is familiar. In addition, it should be mentioned that the disease can occur in an acute form, for example, myocardial infarction, sudden coronary death. Chronic ischemic heart disease is represented by such forms as cardiosclerosis, stable angina, chronic heart failure.
Different stages of atherosclerotic lesions in cardiac ischemia
Overdiagnosis and ineffective therapy of ischemic encephalopathy
Pediatric neurology is one of the few areas of Russian medicine in which most doctors do not follow the latest recommendations for the diagnosis and treatment of PEDs. And if newborn babies with brain damage in our country are looked after very well, then the “consequences of PEP” are treated incorrectly and unreasonably.
- Newborn babies and children in the first 3-6 months of life have features that are mistaken for encephalopathy. For example, trembling, increased muscle tone, Graefe's symptom - all this is the norm for babies up to six months. Most pediatricians and neurologists, unfortunately, do not know about this.
- Examination of a frightened or sleepy baby is another reason for overdiagnosis of cerebral ischemia. In such cases, he may be overly excited or lethargic.
- Overdiagnosis usually results in the prescription of unnecessary medications. Such drugs do not help children with the real consequences of hypoxia, and they are not needed at all for healthy children.
A short list of unnecessary medications:
- Vascular drugs (Cavinton, cinnarizine, etc.) see drugs to improve cerebral circulation
- Actovegin, Cerebrolysin, Cortexin
- Nootropics: phenibut, piracetam, pantogam, picamilon
- All homeopathic medicines (see placebo effect)
- Herbal remedies (motherwort, valerian) see sedatives for children.
All of the above products do not have proven effectiveness and safety. At best, they will not help, at worst, they will cause various side effects.
Manifestations of myocardial ischemia
Symptoms of cardiac ischemia are varied and are determined by the clinical form that they accompany. Many people know such signs of ischemia as pain in the chest, radiating to the left arm or shoulder, heaviness or a feeling of compression behind the sternum, fatigue and shortness of breath even with minor physical exertion. If such complaints appear, as well as if a person has risk factors, he should be asked in detail about the characteristics of the pain syndrome, find out what the patient feels, what conditions could provoke the attack. Typically, patients are well aware of their disease and can quite clearly describe the causes, frequency of attacks, intensity of pain, their duration and nature depending on physical activity or taking certain medications.
Sudden coronary (cardiac) death is the death of a patient, often in the presence of witnesses, occurring suddenly, instantly or within six hours from the moment of the heart attack. It manifests itself as loss of consciousness, cessation of breathing and cardiac activity, and dilation of the pupils. This condition requires urgent treatment, and the sooner it is provided by qualified specialists, the greater the likelihood of saving the patient’s life. However, even with timely resuscitation measures, the incidence of deaths in this form of IHD reaches 80%. This form of ischemia can also be observed in young people, which is most often caused by a sudden spasm of the coronary arteries.
Cerebral ischemia in full-term and premature infants
The nature of brain damage due to asphyxia differs between children born at term and premature babies. The earlier a child is born, the greater the risk of periventricular leukomalacia (PVL). This term means necrosis of the white matter of the brain located near special cavities (ventricles). Cysts form in place of dead cells. It is PVL that is responsible for most cases of cerebral palsy and dementia in children born before 31 weeks of pregnancy.
In full-term infants, the cerebral cortex - the gray matter - is more often damaged. The health consequences will depend on the volume and location of damaged neurons. If the asphyxia was severe and acute, the brain stem, which is responsible for breathing and heartbeat, may be damaged. This poses a direct threat to the baby's life.
Angina and its types
Angina is perhaps one of the most common manifestations of myocardial ischemia. It usually occurs against the background of atherosclerotic damage to the heart vessels, but in its genesis an important role is played by the tendency of blood vessels to spasm and an increase in the aggregation properties of platelets, which entails the formation of blood clots and blockage of the artery lumen by them. Even with minor physical exertion, the affected vessels are not able to ensure normal blood flow to the myocardium, as a result, its metabolism is disrupted, and this is manifested by characteristic pain. Symptoms of coronary heart disease will be as follows:
- Paroxysmal intense pain behind the sternum, radiating to the left arm and left shoulder, and sometimes to the back, shoulder blade, or even to the abdominal area;
- Heart rhythm disturbances (increased or, conversely, decreased heart rate, the appearance of extrasystoles);
- Changes in blood pressure (usually increased);
- The appearance of shortness of breath, anxiety, pale skin.
Depending on the causes of occurrence, various variants of the course of angina pectoris are distinguished. This may be angina pectoris that occurs against the background of physical or emotional stress. As a rule, when taking nitroglycerin or with rest, the pain goes away.
Spontaneous angina is a form of cardiac ischemia that is accompanied by the appearance of pain for no apparent reason, in the absence of physical or emotional stress.
Unstable angina is a form of progression of coronary heart disease, when the intensity of painful attacks and their frequency increases, and the risk of acute myocardial infarction and death increases significantly. The patient begins to consume more nitroglycerin tablets, which indicates a worsening of his condition and a worsening of the disease. This form requires special attention and urgent treatment.
Read more about all types of angina and its treatment by following the link.
Dilated cardiomyopathy
https://www.youtube.com/watch?v=xfzJVZU0X1Q
It can be congenital or acquired. As a result of structural pathology of the myocardium, its contractility decreases and expansion (Latin: dilatatio) of the cavities of the heart occurs. Congestive heart failure develops.
May be congenital or acquired.
As a result of structural pathology of the myocardium, its contractility decreases and expansion (Latin: dilatatio) of the cavities of the heart occurs.
Congestive heart failure develops.
Myocardial infarction, what does this concept mean?
Myocardial infarction (MI) is one of the most dangerous forms of IHD, in which necrosis (death) of the heart muscle occurs as a result of a sudden cessation of blood supply to the heart. Heart attacks are more common in men than in women, and this difference is more pronounced in young and mature adults. This difference can be explained by the following reasons:
- Later development of atherosclerosis in women, which is associated with hormonal status (after menopause, this difference begins to gradually decrease and finally disappears by the age of 70);
- Greater prevalence of bad habits among the male population (smoking, alcoholism).
- The risk factors for myocardial infarction are the same as those described above for all forms of coronary artery disease, however, in this case, in addition to narrowing of the lumen of blood vessels, sometimes thrombosis usually occurs over a significant period.
In various sources, during the development of myocardial infarction, the so-called pathomorphological triad is distinguished, which looks like this:
▼
The presence of an atherosclerotic plaque and its increase in size over time can lead to its rupture and the release of contents to the surface of the vascular wall. Smoking, increased blood pressure, and intense exercise can contribute to plaque damage.
▼
Damage to the endothelium (the inner layer of the artery) when a plaque ruptures causes increased blood clotting and “sticking” of platelets to the site of damage, which inevitably leads to thrombosis. According to various authors, the incidence of thrombosis during myocardial infarction reaches 90%. First, the thrombus fills the plaque, and then the entire lumen of the vessel, and the movement of blood at the site of thrombus formation is completely disrupted.
▼
Spasm of the coronary arteries occurs at the time and place of thrombus formation. It can occur along the entire length of the coronary artery. Coronary spasm leads to a complete narrowing of the lumen of the vessel and the final stop of blood movement through it, which causes the development of necrosis in the heart muscle.
In addition to the reasons described, others play an important role in the pathogenesis of myocardial infarction, which are associated with:
- With a violation of the coagulation and anticoagulation systems;
- With insufficient development of “bypass” circulatory pathways (collateral vessels),
- With immunological and metabolic disorders at the site of damage to the heart muscle.
How to recognize a heart attack?
What are the symptoms and manifestations of myocardial infarction? How not to miss this formidable form of ischemic heart disease, which so often leads to the death of people?
Often, MI finds patients in a variety of places - at home, at work, on public transport. It is important to identify this form of IHD in time in order to begin treatment immediately.
The clinical picture of a heart attack is well known and described. As a rule, patients complain of acute, “dagger-like” chest pain, which does not stop when taking nitroglycerin, changing body position or holding their breath. A painful attack can last up to several hours, with anxiety, a feeling of fear of death, sweating, and cyanosis of the skin.
With the simplest examination, disturbances in the heart rhythm and changes in blood pressure (decrease due to a violation of the pumping function of the heart) are quickly revealed. There are cases when necrosis of the heart muscle is accompanied by changes in the gastrointestinal tract (nausea, vomiting, flatulence), as well as so-called “painless” myocardial ischemia. In these cases, diagnosis can be difficult and requires the use of additional examination methods.
However, with timely treatment, it becomes possible to save the patient’s life. In this case, at the site of the focus of necrosis of the heart muscle, a focus of dense connective tissue will appear - a scar (the focus of post-infarction cardiosclerosis).
Video: how the heart works, myocardial infarction
Classification
According to the pathology:
- Functional - occurs during systematic physical overload. During training, especially great demands are placed on the work of the heart, and in order to respond to them, the body is forced to adapt. As a result, myocardial metabolism changes, and over time, its structure;
- Secondary - appears against the background of another pathology. Cardiopathy often develops against the background of pulmonary pathology (pneumonia, bronchial asthma);
- Dysplastic cardiopathy - develops in children as a result of changes that occur with connective tissue dysplasia. Often morphologically manifested by mitral valve prolapse, additional chords, changes in the shape and position of the heart (teardrop-shaped, the heart axis is vertical). As a result of changes in the structure of the elastic tissue of the heart, it is excessively stretched in diastole and also contracts inadequately in systole, heart failure occurs;
- Cardiomyopathy is a congenital genetically determined myocardial pathology. There are 3 types of cardiomyopathy in children: dilated, hypertrophic and restrictive.
- functional cardiopathy complicates the course of early and prolongs the period of late postpartum adaptation of the circulatory system and the body of the newborn child as a whole;
- limit the volumes and speed of intravenously administered fluid during intensive infusion therapy;
- require differential diagnosis with such congenital heart diseases as congenital defects, cardiomyopathies, carditis;
- functional cardiopathy in some children ends with the formation of some minor anomalies in the development of the heart (insufficiency of the tricuspid and mitral valve, a functioning open foramen ovale);
- the appearance of early consequences (impaired myocardial metabolic processes and reduced LV systolic function during the first 3-6 months of life, various cardiac arrhythmias);
- the formation of long-term consequences during subsequent years of life (incomplete blockade of the right bundle branch, intraventricular blockade at the level of Purkinje fibers).
The true incidence of functional cardiopathy is unknown. Currently, quite a large amount of scientific material has been accumulated on this problem, which requires some systematization. In this regard, we propose a working draft classification of functional cardiopathy of the neonatal period, in which all disorders of the functional state of the heart are divided into 5 classes.
^ Working draft classification of functional cardiopathy of the neonatal period (A.V. Prakhov, 2007).I. Posthypoxic cardiopathy.II. Toxic-metabolic cardiopathy: 1. Functional cardiopathy with indirect hyperbilirubinemia (bilirubin cardiopathy); 2. Cocaine cardiopathy.III. Cerebrocardiac syndrome;^ IV.
Functional cardiopathy caused by endocrine pathology: 1. Diabetic cardiomyopathy of newborns; 2. Cardiopathy with congenital hypothyroidism; 3. Cardiopathy with congenital hyperthyroidism;^ V. Cardiopathy with respiratory distress syndrome. Posthypoxic cardiopathy occurs in newborns who have suffered perinatal hypoxia and is characterized by side of the heart by polymorphism of clinical manifestations, the consequences of which in some children may persist over the next several years of life.
The heart damage is based on transient posthypoxic myocardial ischemia, which occurs in the intrapartum period and in the first days of the early neonatal period. It is caused by post-hypoxic disturbances of microcirculation in the heart muscle with subsequent ischemia, as well as hypoxemia, changes in the rheological properties of blood, hemodynamic overload of the right or left heart, transient pulmonary vascular hypertension and hypoglycemia.
In a child with posthypoxic cardiopathy, early stages of heart failure are clinically diagnosed with a decrease in LV systolic function, focal changes in the ST-T complex on the ECG, in some children, lengthening of A-B conduction, hemodynamic overload of the right heart, tricuspid, less often mitral insufficiency, as well as various disorders heart rhythm.
Early consequences include decreased LV systolic function for 3-6 months after birth, incomplete right bundle branch block, intraventricular blocks at the level of Purkier fibers, mild pulmonary vascular hypertension, tricuspid regurgitation. Long-term consequences occur in the form of incomplete right bundle branch block. His, intraventricular blocks at the level of Purkinje fibers, tricuspid valve insufficiency.
Among toxic-metabolic cardiopathy, a distinction is made between functional cardiopathy with indirect hyperbilirubinemia and cardiopathy with prolonged use of narcotic substances by a woman during pregnancy.^ Functional cardiopathy with indirect hyperbilirubinemia (bilirubin cardiopathy). Occurs in the first 2-6 days after birth when the level of indirect bilirubin is more than 300 µmol/l.
The underlying mechanisms are the toxic effects of high concentrations of indirect bilirubin on the myocardium with blocking of intracellular enzyme systems of myocardial cells (NAD-dependent dehydrogenases, alcohol dehydrogenase, glutamate dehydrogenase, glyceral-3-phosphate dehydrogenase) with the subsequent formation of a deficiency of energy-intensive phosphates.
Clinically, the initial stages of acute heart failure can be determined with a decrease in LV systolic function, a violation of the ventricular repolarization phase in all precordial leads on the ECG. During the first two weeks of life, the majority of children have a restoration of LV systolic function, then by the end of the neonatal period, the indicators of the final part of the ventricular ST-T complex on ECG.
The early and long-term consequences of bilirubin cardiopathy have not been studied.^ Cocaine cardiopathy is formed in utero. The basis of cardiopathy is the regular use of narcotic drugs by a woman during pregnancy. After the birth of a child, cocaine cardiopathy is manifested by a high frequency of congenital minor anomalies of heart structures.
Episodes of respiratory and cardiac arrest are clinically determined. On the first day of life, the child exhibits functional cardiopathy with a decrease in the contractile and pumping function of the left ventricle. Early and long-term consequences are not known.^ Cerebrocardial syndrome (with hypoxic-ischemic damage to the central nervous system).
It is diagnosed from the first days of a newborn’s life. It is based on a violation of the central autonomic regulation of cardiac activity during perinatal hypoxic-ischemic damage to the central nervous system. Clinically, damage to the central nervous system significantly predominates over hypoxic damage to the heart. Most often, the arrhythmic variant is clinically manifested in the form of various cardiac arrhythmias - sinus tachycardia, sinus bradycardia, sinus arrhythmia, various extrasystoles.
During the first months of a child's life, various arrhythmias are diagnosed. Long-term consequences have not been studied. Currently, the most studied functional cardiopathy associated with endocrine pathology are diabetic cardiomyopathy, cardiopathy with congenital hypothyroidism and cardiopathy with congenital hyperthyroidism.
^ Diabetic cardiomyopathy of newborns arises in utero and clinically manifests itself immediately after the birth of the child if the mother has been treated with insulin for a long time. It is based on maternal hyperglycemia resulting from diabetes, fetal hyperinsulinism, hormonal placental dysfunction, disturbances in the hormonal regulation of interactions at the level of cell membranes, which ultimately leads to heart damage in the form of glycogen deposition in the myocardium and its subsequent hypertrophy.
It is characterized by asymmetric thickening of the heart septa, especially the interventricular septum and the wall of the left ventricle, dynamic subaortic stenosis, a decrease in LV diastolic filling, resulting in LV diastolic dysfunction and an increase in the size of the heart chambers. Clinical manifestations of diabetic cardiomyopathy usually disappear by the end of the first month of life, and pathological changes in the heart regress within 6-12 months after the birth of the child.
Long-term consequences have not been studied.^ Cardiopathy with congenital hypothyroidism occurs in utero. It is based on a deficiency of thyroid hormone in the body of the fetus. Clinically manifested by sinus bradycardia, early stages of heart failure. The ECG is characterized by low-amplitude ventricular complexes in the left precordial leads and an increase in the duration of the ventricular QRS complex in lead V3R-V2R-V1.
According to ultrasound examination of the heart, a moderate pericardial effusion can be detected. Thyroxine therapy leads to an improvement in cardiac function and electrocardiographic and echocardiographic parameters during the first months of life. Long-term consequences have not been studied.^ Cardiopathy with congenital hyperthyroidism occurs in utero.
It is based on transplacental transfusion of thyroid-stimulating immunoglobulin from mother to fetus. In the neonatal period, it is clinically manifested by sinus or supraventricular tachycardia, followed by a decrease in systolic function of the left ventricle and the addition of acute heart failure, as well as transient pulmonary vascular hypertension.
Normalization of thyroid function in the first months of a child’s life leads to regression of cardiac pathology. Long-term consequences have not been studied.^ Cardiopathy in respiratory distress syndrome occurs predominantly in premature infants after birth, due to systolic overload of the right heart due to high transient pulmonary vascular hypertension, which is the result of disseminated pulmonary atelectasis, hyaline membrane disease or edematous-hemorrhagic syndrome , as well as concomitant hypoxemia and hypoxia caused by acute respiratory failure.
Clinically manifested by various stages of acute heart failure, mainly of the right ventricular type. The ECG diagnoses systolic overload of the right ventricle, various rhythm and conduction disturbances. According to cardiac ultrasound, an increase in the diameter of the right ventricle, an enlargement of the right atrium is detected, and relative insufficiency of the tricuspid valve may occur.
With a decrease in pulmonary vascular hypertension and respiratory failure, the manifestations of cardiopathy disappear. The immediate and long-term consequences have not been studied. Thus, the proposed working draft of the classification of neonatal functional cardiopathy reflects the main disorders of the functional state of the heart in newborns that have been studied to date and can serve practitioners as a basis for diagnosis and differential diagnosis with other congenital cardiac pathologies .
Consequences and complications of coronary artery disease
Post-infarction cardiosclerosis
Post-infarction cardiosclerosis is one of the forms of coronary heart disease. A scar in the heart allows the patient to live for more than one year after a heart attack. However, over time, as a result of impaired contractile function associated with the presence of a scar, one way or another, signs of heart failure - another form of coronary heart disease - begin to appear.
Chronic heart failure
Chronic heart failure is accompanied by the occurrence of edema, shortness of breath, decreased tolerance to physical activity, as well as the appearance of irreversible changes in the internal organs, which can cause the death of the patient.
Acute heart failure
Acute heart failure can develop in any type of coronary artery disease, however, it most often occurs in acute myocardial infarction. So, it can manifest itself as a disruption of the left ventricle of the heart, then the patient will have signs of pulmonary edema - shortness of breath, cyanosis, the appearance of foamy pink sputum when coughing.
Cardiogenic shock
Another manifestation of acute circulatory failure is cardiogenic shock. It is accompanied by a drop in blood pressure and a pronounced disruption of the blood supply to various organs. The condition of the patients is severe, consciousness may be absent, the pulse is threadlike or not detectable at all, breathing becomes shallow. In internal organs, as a result of lack of blood flow, dystrophic changes develop, foci of necrosis appear, which leads to acute renal and liver failure, pulmonary edema, and dysfunction of the central nervous system. These conditions require immediate action because they directly pose a mortal danger.
Arrhythmia
Heart rhythm disturbances are quite common among patients with cardiac pathology; they often accompany the above forms of coronary artery disease. Arrhythmias can either not significantly affect the course and prognosis of the disease, or significantly worsen the patient’s condition and even pose a threat to life. Among arrhythmias, the most common are sinus tachycardia and bradycardia (increased and decreased heart rate), extrasystoles (the appearance of extraordinary contractions), and disturbances in the conduction of impulses through the myocardium - so-called blockades.
Main causes of cerebral ischemia in newborns
Intrauterine hypoxia or asphyxia during childbirth (complete stop of oxygen supply)
- acute placental insufficiency (see fetal hypoxia), placental abruption
- long labor
- umbilical cord compression during contractions and pushing
Respiratory failure after birth
- congenital heart defects
- disturbance of the blood supply to the heart
- patent ductus arteriosus
- respiratory failure in premature infants
Decreased blood pressure after birth
- sepsis
- excessive bleeding (blood clotting disorders, liver injuries and other causes)
Methods for diagnosing coronary heart disease
Currently, there are many modern and diverse methods for detecting coronary blood flow disorders and cardiac ischemia. However, one should not neglect the simplest and most accessible ones, such as:
- Careful and detailed questioning of the patient, collection and analysis of complaints, their systematization, clarification of family history;
- Examination (detecting the presence of edema, changes in skin color);
- Auscultation (listening to the heart with a stethoscope);
- Carrying out various tests with physical activity, during which the activity of the heart is constantly monitored (bicycle ergometry).
These simple methods in most cases make it possible to fairly accurately determine the nature of the disease and determine a further plan for examination and treatment of the patient.
Instrumental research methods help to more accurately determine the form of coronary artery disease, severity and prognosis. Most often used:
- electrocardiography is a very informative way to diagnose various types of myocardial ischemia, since ECG changes under various conditions have been studied and described quite well. ECG can also be combined with dosed physical activity.
- biochemical blood test (detection of lipid metabolism disorders, the appearance of signs of inflammation, as well as specific enzymes characterizing the presence of a necrotic process in the myocardium).
- coronary angiography, which allows, by introducing a contrast agent, to determine the localization and extent of damage to the coronary arteries, the degree of their narrowing by cholesterol plaque. This method also allows you to distinguish IHD from other diseases when diagnosis using other methods is difficult or impossible;
- echocardiography (detection of disturbances in the movement of individual sections of the myocardium);
- radioisotope diagnostic methods.
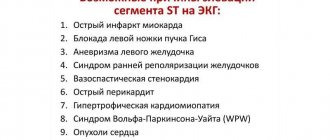
Today, electrocardiography seems to be a fairly accessible, fast and, at the same time, very informative research method. Thus, with the help of an ECG, a large-focal myocardial infarction can be detected quite reliably (decrease in the R wave, appearance and deepening of the Q wave, elevation of the ST segment, taking on a characteristic arc shape). Depression of the ST segment, the appearance of a negative T wave, or the absence of any changes on the cardiogram will indicate subendocardial ischemia in angina. It should be noted that now even linear ambulance teams are equipped with ECG machines, not to mention specialized ones.
Diagnostics
Typically, cerebral ischemia manifests itself in the first days after birth. Mild encephalopathy resolves fairly quickly, but severe encephalopathy may have a false “bright spot,” a few hours or days of improvement followed by a sharp deterioration. Therefore, a complete examination is necessary to make a diagnosis.
Examination of the baby
The examination includes an assessment on the Apgar scale, testing of all important reflexes (sucking, swallowing, grasping), measurement of body weight and height.
Analyzes
- general blood analysis
- blood electrolyte level
- blood clotting assessment
- amount of blood gases (oxygen, carbon dioxide)
MRI of the brain
For moderate and severe cerebral ischemia, magnetic resonance imaging of its structures is often used. With mild ischemia that resolves within 24 hours, there is rarely a need for MRI.
Ultrasound of the brain
Despite popular belief, ultrasound is not an accurate way to detect hypoxic encephalopathy. With its help, you can sometimes notice signs of cerebral edema and hemorrhage. But more often this research method gives a false positive result. Therefore, ultrasound is used for the initial diagnosis, with the need for additional examination.
EEG (electroencephalography)
This study is indispensable in children with severe cerebral ischemia. With its help, you can identify hidden seizures, assess the degree of brain damage and the integrity of its activity, and select the correct anticonvulsant therapy.
Treatment methods for various forms of myocardial ischemia
Currently, there are many different methods of treating coronary heart disease, which can not only prolong the patient’s life, but also significantly improve its quality. These can be conservative (use of medications, physical therapy) and surgical methods (operations that restore the patency of the coronary vessels).
Proper nutrition
An important role in the treatment of coronary artery disease and rehabilitation of the patient is played by the normalization of the regimen and the elimination of existing risk factors. It is imperative to explain to the patient that, for example, smoking can minimize all the efforts of doctors. So, it is important to normalize nutrition: exclude alcohol, fried and fatty foods, foods rich in carbohydrates; in addition, if you are obese, it is necessary to balance the amount and calorie content of food consumed .
The diet for coronary artery disease should be aimed at reducing the consumption of animal fats, increasing the proportion of fiber and vegetable oils in food (vegetables, fruits, fish, seafood). Despite the fact that significant physical activity is contraindicated for such patients, proper and moderate physical therapy helps adapt the affected myocardium to the functional capabilities of the vessels supplying it. Walking and dosed physical exercise under the supervision of a specialist are very useful.
Drug therapy
Drug therapy for various forms of coronary artery disease is reduced to the prescription of so-called antianginal drugs that can eliminate or prevent attacks of angina pectoris. Such drugs include:
- Nitrates (for example, nitroglycerin) - it has the property of dilating the coronary arteries and quickly improving blood delivery to the myocardium. It is used for an attack of angina pectoris, acute pain during myocardial infarction, and the development of pulmonary edema;
- Drugs from the group of beta-blockers (metoprolol, atenolol) - reduce the heart rate during tachycardia, reduce the oxygen demand of the heart muscle, and exhibit an antiplatelet effect. Used for angina pectoris, chronic heart failure;
- Drugs from the group of calcium antagonists (verapamil, nifedipine) - in addition to antianginal, have a hypotensive effect, improve exercise tolerance;
- Thrombolytic and antiplatelet therapy is especially important in case of myocardial infarction for the rapid dissolution of a blood clot and restoration of patency of the affected vessel, as well as for the prevention of thrombosis in chronic forms of coronary artery disease. Heparin, streptokinase, acetylsalicylic acid preparations (aspirin cardio, cardiomagnyl) are used.
In all acute forms of coronary artery disease, prompt and qualified assistance is required with the use of effective painkillers, thrombolytics, and the administration of plasma replacement drugs (if cardiogenic shock develops) or defibrillation may be required.
Operation
Surgical treatment of cardiac ischemia is reduced to:
- restoration of the patency of the coronary arteries (stenting, when a tube is inserted at the site of damage to the vessel by atherosclerosis, preventing further narrowing of its lumen);
- or to create a bypass blood supply (coronary artery bypass grafting, mammary coronary artery bypass grafting).
When clinical death occurs, it is very important to begin resuscitation measures in a timely manner. If the patient’s condition worsens, severe shortness of breath appears, or heart rhythm disturbances occur, it is too late to run to the clinic! Such cases require calling an ambulance, since the patient may need to be hospitalized as quickly as possible.
Video: lecture by a specialist on the treatment of ischemia
Hypertrophic cardiomyopathy
This is exclusively a congenital cardiomyopathy. Due to gene mutations, a morphological restructuring of the left parts of the heart occurs, especially the left ventricle. Its hypertrophy occurs, which increases the heart's need for oxygen. Even with normal patency of the coronary arteries, the heart suffers from ischemia. As a result, decompensation of the body’s capabilities occurs, resulting in circulatory failure.
This is exclusively a congenital cardiomyopathy. Due to gene mutations, a morphological restructuring of the left parts of the heart, especially the left ventricle, occurs. Its hypertrophy occurs, which increases the heart's need for oxygen.
Even with normal patency of the coronary arteries, the heart suffers from ischemia. As a result, decompensation of the body’s capabilities occurs, resulting in circulatory failure.
After discharge from hospital
Treatment with folk remedies can only be effective in combination with traditional methods. The most common use of various herbs and infusions, such as chamomile flowers, motherwort herb, tincture of birch leaves, etc. Such infusions and herbal teas can have a diuretic, calming effect, and improve blood circulation in various organs. Considering the severity of the manifestations, the high risk of death , the use of purely unconventional means of influence is unacceptable, therefore, it is extremely undesirable to look for any means that can be recommended by ignorant people. Any use of a new medicine or folk remedy should be discussed with the attending physician.
In addition, when the worst is over, in order to prevent recurrence, the patient should take for granted the prescription of drugs to correct the lipid composition of the blood plasma. It would be great to dilute the drug treatment with physiotherapeutic procedures, visiting a psychotherapist and receiving sanatorium treatment.
Signs of cerebral ischemia at the third stage
Over time, the disease turns a person into a disabled person:
- Intellectual functions are impaired: abstract thinking, reading, counting, memorizing and reproducing information, etc.
- Facial expressions become sluggish.
- Walking slows down.
- The gait becomes uncertain, coordination of movements is significantly impaired.
- Falls and fainting are observed.
Many patients suffering from cerebral ischemia at the third stage have already suffered a stroke or an attack of transient ischemic attack (sometimes more than once).
Features of cardiopathy
In infants, cardiopathy is observed after intrauterine or perinatal hypoxia and is called posthypoxic cardiopathy. When it occurs, the metabolism of the heart and its autonomic regulation are disrupted, which impairs its function. This condition is not included in the diagnosis and medical statistics, but it occurs in more than 50% of newborns. It is worth saying that the consequences of intrauterine hypoxia most often disappear within 3 years.
Newborns may also suffer from cardiopathy. The disease often develops against the background of a lack of oxygen. Moreover, it does not matter when hypoxia occurred, during childbirth or during pregnancy. Due to oxygen deficiency, the regulation of heart function is disrupted with changes in the autonomic nervous system.
Myocardial dysfunction occurs due to disruption of energy metabolism processes. On average, 50-70% of newborns who have suffered hypoxia suffer from cardiopathy. The severity of the pathology largely depends on the duration of hypoxia. If a lack of oxygen was observed after birth, then heart pathology is more likely to develop, which then needs to be specifically treated. Typically, such cardiopathy persists from a month to three years of age in about a third of affected children.
In Greek, the word “cardiopathy” means “disorder of the heart.” ICD (International Classification of Diseases) code 10th revision for pathology I42. In this regulatory document it is described as “cardiomyopathy”. In fact, there is no difference between these two concepts (cardiopathy and cardiomyopathy), therefore both options are used when describing structural changes in the myocardium in a child.
They are often detected by ultrasound examination of the heart. There are many types of cardiopathy, each of them is provoked by certain factors. The less dangerous and most common form of the disease is considered functional. It often develops in school-age children due to stress and overload and does not actually manifest itself.
Other types of pathology have more significant causes and often leave irreversible consequences. In an infant, the problem can be identified by focusing on symptoms, or using instrumental research methods. In older children, cardiopathy is often detected by their behavior during physically active play.
- coronary vessel anomalies;
- growth of the septum between the ventricles;
- irregular heartbeat;
- disturbances in the signal conduction system;
- ventricular malformations;
- prolapse (incomplete closure) of valves.
These are characteristic cardiopathy changes in the structure and functioning of the heart. Most factors indicate the presence of heart defects. In other cases, the disease manifests itself against the background of the development of other diseases and metabolic failures. To make an accurate diagnosis, you will have to undergo a complete instrumental examination.
Many parents had to learn from their own experience what cardiopathy is in children because of its prevalence. In infants, the disease has a congenital form, while in more mature children it is more often diagnosed as acquired. The pathological process is based on metabolic disruptions. Because of them, muscle tissue dystrophy develops.
They are gradually being replaced by connecting ones that do not conduct electrical impulses. The child experiences various arrhythmias, heart failure manifests itself and the myocardium grows (hypertrophies). The highest probability of cardiopathy appears at school age. The baby is constantly tired (physically and mentally) and experiences hormonal surges associated with puberty, which leads to disruptions in metabolic processes and development of heart failure. The process is accompanied by the appearance of excess weight and shortness of breath during any physical activity.
The famous pediatrician, Evgeniy Olegovich Komarovsky, is often asked about cardiopathy in newborns, since many doctors cannot answer exactly what it is. According to the specialist, the disease is attributed to all people who have a healthy heart, but there are some pathological changes. Translated from Greek, “pathos” means “disease”.
In infants, cardiopathy is observed after intrauterine or perinatal hypoxia and is called posthypoxic cardiopathy. When it occurs, the metabolism of the heart and its autonomic regulation are disrupted, which impairs its function.
This condition is not included in the diagnosis or medical statistics, but it occurs in more than 50% of newborns. It is worth saying that the consequences of intrauterine hypoxia most often disappear within 3 years.
Newborns may also suffer from cardiopathy. The disease often develops against the background of a lack of oxygen. Moreover, it does not matter when hypoxia occurred, during childbirth or during pregnancy. Due to oxygen deficiency, the regulation of heart function is disrupted with changes in the autonomic nervous system. Myocardial dysfunction occurs due to disruption of energy metabolism processes.
On average, 50-70% of newborns who have suffered hypoxia suffer from cardiopathy. The severity of the pathology largely depends on the duration of hypoxia. If a lack of oxygen was observed after birth, then heart pathology is more likely to develop, which then needs to be specifically treated. Typically, such cardiopathy persists from a month to three years of age in about a third of affected children.
Causes and symptoms of secondary cardiomyopathy
The prevalence of heart disease is growing rapidly these days.
More and more people are turning to doctors with complaints of pain in the heart area. It is not uncommon during the examination to diagnose diseases that are a consequence of other diseases. Changes in the structure and function of the heart muscle, which are a consequence of major primary diseases, are called secondary cardiomyopathy (hereinafter referred to as VCMP). This disease is not limited to older people. It is often diagnosed in children, young people and middle-aged people. Although, it should be noted that secondary cardiomyopathy does not occur very often, and is a consequence of the effects of other heart diseases on the heart and blood vessels.
Clinical picture
When examined by a doctor, you can suspect a pathology in a child based on the following symptoms:
The symptoms of cardiopathy depend on its form and cause. Some types of the disease do not actually appear for a long time. Signs become more pronounced as heart failure and other complications develop. The most common clinical picture below is:
- general weakness;
- chest pain;
- low performance;
- rapid heartbeat, extrasystoles (extraordinary contractions);
- hypoxic syndrome (dizziness, pale skin).
With serious damage to the right ventricle and atrium, symptoms of pulmonary failure occur:
- increased sweating;
- shortness of breath at the slightest physical exertion;
- swelling of the lower extremities;
- cough;
- heaviness in the chest.
Cardiopathy in childhood can be congenital or acquired. You can familiarize yourself with the features of these forms below:
- A baby can get congenital cardiopathy due to heart defects and autoimmune disorders. If the causative factors do not have a significant impact, then the disease is detected only over time, and not in the first months of life.
- The acquired form is diagnosed around 8-12 years of age. It is associated with the active growth of the child. If we are talking about a 15-16 year old teenager, then changes often occur due to hormonal surges caused by puberty.
In children, cardiopathy is divided according to its development mechanism into the following main types:
- The dilated form can be congenital or acquired over time. The baby's parts of the heart hypertrophy, the intensity of contractions decreases and the passage of the impulse is disrupted. Heart failure gradually develops.
- Hypertrophic cardiopathy is congenital. Due to developmental defects, the myocardium grows and its need for oxygen increases. Ischemic disease and severe disruptions in hemodynamics gradually develop.
- The restrictive variety is exclusively congenital and is the least common. Its etiology (conditions of origin) is not known for certain. As the pathology develops in the child, the volume of the heart chambers decreases (without wall growth), which leads to impaired filling of the left ventricle with blood. Against the background of the occurrence of structural changes in the myocardium, hypoxia of all organs and tissues appears.
According to the causative factor, cardiopathy is divided into many types, but only some of them are typical for children:
- dismetabolic (metabolic);
- posthypoxic;
- functional;
- secondary;
- dysplastic.
Functional
It is advisable for parents who want to take their child to many different sports sections at once to understand what “functional cardiopathy in children” is. Pathology manifests itself due to excessive physical and psycho-emotional overload. The heart tries to adapt to this regime, which is why pathological changes occur.
Sometimes the disease develops due to unprofessional physical education teachers and coaches who do not know about acceptable age standards. They force children to exercise more than expected, as a result of which cardiopathy occurs. Sometimes its appearance is associated with raising a child in a dysfunctional family. No one is watching him, and against the backdrop of frequent stress and overwork at school, heart problems may begin.
Dysplastic
The dysplastic type of the disease develops as an independent pathological process. In most cases, it is not affected by malfunctions and other ailments. Some experts believe that with this form of cardiopathy there is a section of connective tissue in the heart, due to which failures occur during the conduction of the impulse.
Other doctors equate it to a functional form of failure. In some countries, dysplastic cardiopathy means mitral valve prolapse. In Russia, a similar diagnosis is more often made if changes are detected in the heart, but there is no explanation for them. Usually no course of therapy is prescribed and it is enough to follow the rules of prevention.
If other factors influence the development of the disease, then they must be stopped. Secondary cardiopathy in a child is a consequence of various pathologies. The disease is often diagnosed in school-age children. The list of the most common diseases that affect it is as follows:
- inflammatory diseases (myocarditis, endocarditis, pericarditis);
- respiratory diseases;
- severe metabolic disturbances;
- chronic inflammatory processes.
It is easiest to detect secondary cardiopathy in children in the latter case. The child has been under the supervision of a doctor for a long time, so structural changes in the myocardium rarely go unnoticed.
Metabolic
Metabolic cardiopathy is a consequence of metabolic failures. It is most often found in adolescents and is associated with a poorly designed diet, frequent colds and hormonal surges. Among the diseases that influence the development of this pathology are diabetes mellitus and thyroid dysfunction.
Posthypoxic
The posthypoxic form is characteristic of infants who have experienced intrauterine hypoxia (oxygen starvation). Because of it, metabolic processes in the heart muscle are disrupted and disruptions in nervous regulation occur. Data about this problem is not recorded in the outpatient card, but it occurs in every second newborn. Posthypoxic cardiopathy goes away on its own within 2-3 years.
Course of therapy
The treatment regimen for cardiopathy depends on its form. It may include medications, traditional medicine recipes, lifestyle changes and surgery. The basis of treatment is the fight against the causative factor. If it cannot be eliminated, then supportive medications are prescribed to eliminate unpleasant symptoms.
For dilated cardiopathy, the doctor will recommend the following medications:
- ACE inhibitors (Spirapril, Ramipril) must be taken to stabilize blood pressure and stop the growth of the heart muscle.
- Beta-blockers (Nipradilol, Alprenolol) reduce myocardial oxygen demand and stop arrhythmia.
- Diuretics (Indapamide, Furosemide) are used to remove excess moisture from the body, especially if there is stagnation in the pulmonary or systemic circulation.
- Blood thinners (Curantil, Phenilin) prevent the development of blood clots.
To eliminate the hypertrophic form of cardiopathy, medications are used to reduce the myocardial oxygen demand and improve its contractility. The treatment regimen includes beta-blockers and blood thinners. Only calcium antagonists (Verapamil, Diltiazem) can be added to it. They stabilize the heart rhythm and reduce the automaticity of the sinus node. In severe cases, it is necessary to perform surgical intervention, the purpose of which is to install a pacemaker or remove a hypertrophied section of the septum.
The restrictive type of the disease is the most difficult to treat, especially its primary form. The course of therapy is aimed at eliminating symptoms and underlying pathologies, for example, hemochromatosis is treated with bleeding, and sarcoidosis is treated with corticosteroids. To slow the development of heart failure, beta-blockers, ACE inhibitors and diuretics are prescribed. Heart transplantation was previously popular, but its effect was only temporary. Gradually, pathology developed in the new organ.
Ischemic cardiopathy is treated by slowing the development of the underlying pathological process. In severe cases, surgery is prescribed to improve coronary blood flow or a heart transplant.
Among the general drugs suitable for any form of the disease are the following:
- "Riboxin" activates metabolic processes in the heart muscle, reduces platelet aggregation and eliminates areas of ischemia.
- "Metonate" improves oxygen transport, normalizes nerve conduction and eliminates areas of ischemia.
- "Carnivit" is used to enrich heart tissue with levocarnitine. The substance will improve myocardial metabolism and slow down the development of structural changes.
ethnoscience
As a complement to the treatment regimen for cardiopathy, the use of folk remedies is allowed. They virtually have no contraindications or side effects, which is a clear advantage, especially with long-term use. The following recipes are most relevant:
- Flax seed contains a high concentration of organic acids, which can stabilize metabolic processes in cardiomyocytes. To prepare the decoction, you need to pour 40 g of the main ingredient into 1 liter of boiling water. Next, the container is placed in a water bath. After 50 minutes, you need to remove it from the stove and remove the raw materials. Drink the prepared medicine during the day, half a glass at a time.
- Viburnum is rich in essential oils, vitamins and microelements that are vital for normal heart function. Every day it is enough to take 100 g of its fruits. Making a decoction is not recommended, as the beneficial substances are partially destroyed during heat treatment. Berries are contraindicated for angina pectoris and varicose veins.
- An infusion of hare cabbage is especially useful for the dilated form of cardiopathy. It tones the body, improves tissue regeneration, relieves inflammation and strengthens the immune system. To prepare, you will need to pour 50 g of cabbage leaves into 250 ml of boiling water. Then close for 4 hours. Before use, remove the raw materials. Drink 50 ml 4 times a day.
Treatment
The pathology must be treated immediately after symptoms are identified. The main thing in treatment is to prevent the latter degree of severity, since in this case even modern medicine will not be able to do anything.
Treatment of heart failure in children can be done conservatively or through surgery. If signs of pathology are noticed, emergency assistance will be required, which consists of the following:
- The child must be kept in a semi-sitting position.
- Next, a tourniquet is applied to the legs so that arterial blood flow is not impaired.
- Feet should be placed in warm water.
If the child is already in the hospital, he will be injected with a drug. Typically, morphine is used. After this, an oxygen mask is installed through which breathing occurs. If the patient has acute deficiency, treatment is carried out with the administration of heparin.
Stenosis of the coronary vessels of the heart
Surgeries are performed when other treatments fail. Treatment in this case is radically different:
- In the first case, a complete heart transplant occurs. The damaged organ is removed, after which the donor organ is sutured.
- In the second case, treatment is carried out with cardiomyoplasty. In other words, the surgeon takes a piece of the patient's latissimus dorsi muscle, after which it covers the patient's heart. Due to this, improved contraction of the heart muscles is achieved.
- In the latter case, treatment involves replacing the heart with an artificial one. In this case, prostheses are used that improve contractility.
After the child recovers, certain care will be required.
Important! After surgery and in case of complications, it is necessary to observe bed rest, while maintaining a semi-sitting position. It is better to coordinate the loads with the treating doctor.
Restrictive cardiomyopathy
This type of congenital cardiomyopathy is poorly understood, which affects the life expectancy of children with this pathology. Etiology unknown. With this type of disease, the volume of the heart chambers decreases without changing the wall thickness. The filling of the heart is disrupted, and hypoxia of tissues and organs develops.
The disease quickly leads to death.
This type of congenital cardiomyopathy is poorly understood, which affects the life expectancy of children with this pathology. Etiology unknown. With this type of disease, the volume of the heart chambers decreases without changing the wall thickness. The filling of the heart is disrupted, hypoxia of tissues and organs develops. The disease quite quickly leads to death.