How many years can a person who has an artificial heart valve installed live? This is the question that interests many patients and their relatives when it comes to such an operation. The average life expectancy for patients with an artificial heart valve is 20 years. True, doctors say that the service life of the valve itself is about 300 years, and the valve itself does not lengthen or shorten life. Often, people who live 20 years with an artificial heart valve do not die due to cardiovascular problems.
When to place an artificial valve
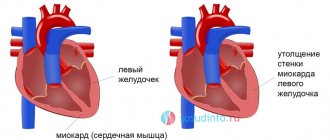
Doctors compare a heart valve to an ordinary door. When a door swells or becomes askew, it has to be repaired. It's the same with the heart valve. There are three types of damage to the heart valve, when serious treatment is required: narrowing or sticking (blood flow slows down, heart nutrition deteriorates and oxygen starvation occurs), expansion or overstretching (the tightness is broken and the load on the organ increases), a combination of these two problems.
There is no need to panic when diagnosed with heart failure. The valve cannot always be replaced. Sometimes it is simply reconstructed.
Heart valve replacement is used when its function becomes limited. The reason for this may be atherosclerosis, infection, impaired tissue development, etc.
A device that makes your heart beat like a clock
It’s hard to believe that the first pacemakers weighed up to 7 kilograms! Photo by Reuters
The heart rate depends on the beats produced by electrical impulses that cause the muscle to contract and thus achieve pumping of blood throughout the body. But what to do if this mechanism is unbalanced and the heart no longer works so well? A pacemaker, a small electronic device that can detect and correct errors in heart rhythm, can solve the problem.
The first pacemaker implantation in history was performed on October 8, 1958 at the Royal Hospital in Stockholm. It was a very dangerous operation with an unknown outcome. Swedish surgeon Åke Senning performed it on the heart of 43-year-old Arne Larsson, who suffered from severe heart rhythm disturbances. The rhythm disturbance was so severe that the patient lost consciousness almost every hour. His desperate wife persuaded him to agree to urgent implantation - the only chance to survive. The outcome of this operation was not obvious: Åke Senning and the engineer Rune Elmqvist, with whom the surgeon designed this pacemaker, had not yet managed to bring it to perfection.
It was the size of a hockey puck and ran on two transistors. The patient's chest was opened and pacemaker electrodes were sewn to the heart. Three hours later I had to do a second operation and change the device. The second pacemaker lasted a week. And again the operation. In total, Larsson's device was changed more than 20 times. Only in 1961, when the patient was given a pacemaker of a new design, was he able to live a full life. Arne Larsson lived to the age of 86, and died not due to cardiac problems, but from a completely different disease.
Before Senning and Elmqvist made a real revolution in medicine, there were many attempts to stimulate the heart using electrical impulses. But even if the patient managed to prolong his life, it was only for a very short time. In addition, he remained disabled and bedridden. Old pacemakers were bulky, complex machines that were located externally. Open wounds that formed when electrodes going to the heart were implanted were a constant source of dangerous infections.
The world's first pacemaker was invented by the American Wilson Greatbatch. While developing a device at the University at Buffalo for a local medical center that recorded heart rhythms, he mistakenly inserted the wrong resistance into the electrical circuit and noticed that the device began to generate electrical signals similar to heart rhythms, and wondered how to compensate for failures using electrical stimulation. human heartbeat.
An important step towards ensuring a normal life for a person with a pacemaker was made in 1957: pacemakers began to be powered by batteries. But at first they often had to be changed. The design of the devices gradually improved, but performance continued to depend on batteries. In 1971, Wilson Greatbatch invented the lithium cell and thereby solved the problem.
Currently, the lifespan of a pacemaker ranges between 5 and 10 years, depending on the patient's level of use. The technique of implanting the device has also been significantly improved to reduce harm to the body during installation and securing. Now it is possible not to place it under the collarbone, but to implant it using a catheter through the femoral vein. In addition, wireless pacemakers are beginning to be used. The first implantation of a wireless pacemaker took place in January 2014 in Spain at the Infanta Hospital in Badajoz.
Now, 60 years after the pacemaker was first implanted, this operation is considered routine. It is usually done under local anesthesia. It has become possible to program pacemakers and check their condition without surgery.
In the mid-1990s, dual-chamber pacemakers began to be implanted, which can simultaneously stimulate both the atrium and ventricle of the heart. The latest devices provide a physiologically natural contraction of the heart chambers.
Over time, pacemakers become not only more advanced and reliable, but also smaller and lighter. The first portable (or so they thought then) external pacemaker, invented in the late 1920s by Albert Hyman from New York, weighed more than 7 kg. Its modern counterpart weighs only 20–30 g and is the size of a small wristwatch. Pacemakers are implanted in more than half a million people each year, according to the American Heart Association.
Types of heart valves
Today, doctors operate with two types of artificial valves: mechanical and biological. Each of them has its own advantages and disadvantages.
Mechanical valves are a kind of prosthesis that is designed to replace the function of the natural human heart valve. The main job of the valves is to carry blood through the heart and release it back out. Mechanical valves are installed when the function of the native heart valve is no longer restored.
Tests of modern man-made valves estimate a service life of 50,000 years when placed under accelerated wear conditions. This means that if it takes root in a person, it will work until the moment the person is measured out.
The only thing worth remembering is that all artificial valves require additional support and the use of anticoagulants that thin the blood so that blood clots do not form in the heart. You will also have to undergo regular tests.
Biological valves are prosthetic valves made from animal tissue. Very often they use a pig heart valve. Naturally, it is pre-processed to make it suitable for implantation into the human body. Biological valves, in comparison with mechanical valves, are noticeably inferior in durability.
Heart surgery. Which valve to choose: biological or mechanical?
Patients often ask the following question: which valve will be implanted in me - mechanical or biological? What really is the difference and what does it all depend on? Much depends on age. And in general, I will try to write here about adult patients, i.e. who are 14 years old and older.
It also depends on what position you require valve implantation in: aortic, mitral or tricuspid?
If you have a damaged tricuspid valve at any age, then in 95% of cases you will have a biological valve implanted.
Why? It is known that valves are prepared from bovine or porcine pericardium or using cadaveric human tissue (i.e. allografts). In any case, a biological valve is a piece of dead tissue that has been specially treated, and such tissue does not naturally regenerate, i.e. cannot be restored if damaged.
Therefore, biological valves are not durable. As you know, the heart works 24 hours a day, and a certain pressure is created in each chamber of the heart, which in turn leads to a load on the valve. The minimum pressure is in the right ventricle, up to 25 mm Hg.
and therefore implantation of a biological valve in this position is the most preferred option. Implantation of a mechanical valve in this position is carried out in certain exceptional cases, but it is not advisable, due to the fact that taking anticoagulants (blood thinners) does not lead to the desired effect, i.e.
preventing thrombus formation. Since blood passes through the entire vein system, incl. hepatic, where part of the drug is simply disposed of, and renal vessels. Thus, the concentration of the drug in venous blood, which enters the right sections and tricuspid valve, is several times less than the drug content in arterial blood.
When the mitral and aortic valves are damaged, mechanical valves are often implanted. However, young girls implanted with biological ones , although it is known that biological ones will last up to 25 years.
Why? Yes, because when implanting a biological valve, long-term use of anticoagulants is not required, and every girl is preparing to soon be a mother and taking anticoagulants during pregnancy is not advisable.
When implanting a biological valve, they are usually taken for six months .
An exception is the category of patients with rhythm disturbances such as atrial fibrillation (atrial fibrillation), for whom anticoagulants are indicated for a long time to avoid thrombus formation in the left atrium and on the valve itself.
Patients over 60 years old
biological valves are also implanted .
For everyone else, implantation of a mechanical valve is desirable. The only inconvenience for patients with mechanical valves is the lifelong use of anticoagulants under the control of INR or IPT. But you should know that a modern mechanical valve, with proper selection and constant use of anticoagulants, will serve you for a long life.
Some people wonder - are all biological or mechanical valves quality? – Let me tell you – YES! I am often asked which valves are better – foreign or domestic? The fact is that Russian valve developers make them well, but foreign ones are better. This is unfortunately the case with everything.
What will you take – the new Lada Kalina or the new Mercedes? Many will choose the second option, although the first option is also not bad - you can drive it, it’s also new, but... That’s the same with valves.
Therefore, if you do not need to sell the latter and you have a reserve of money, it is better, of course, to implant an imported prosthesis, but if there is no money, then you should not grieve, the main thing is to follow all the instructions given by the attending physician. Compliance with all instructions is no less important than implantation of a particular valve.
I won’t write which foreign valves are better and which domestic ones are better - they all have their own pros and cons. Of the Russian biological ones , I would choose Kemerovo and Bakulevskie , I would never buy others.
Of the mechanical ones - bicuspid valves - Meding , and nothing else. Typically, domestic valves are implanted according to a quota. As for imported ones, it’s hard to choose from biological ones, all are good, but from mechanical ones I would prefer ATC and On-X . The former are distinguished by their noiselessness, i.e.
their ticking is practically inaudible, and the latter are more resistant to thick blood and it is impossible to quickly select anticoagulants. But medications must ALWAYS be taken! And no matter what mechanical valve you implant, all the surgeon’s work will be wasted if you do not follow the correct intake of anticoagulants.
You should know that implantation of an imported valve comes at an additional cost. You discuss your wishes with the surgeon, and pay to the hospital cash desk, and rest assured, an imported valve will be implanted during the operation. This happens both in Russia and abroad. But! You are not always implanted with one or another imported valve you want in Russia.
The choice is up to the surgeon! Firstly, it depends on the size of the fibrous ring in the heart, the configuration of your heart and... And it depends on which foreign company the surgeon (less often the clinic) has an agreement with. Yes, and also, you should discuss what the suture material will be, if it is not included in the cost of the imported valve, it is better to pay for it.
Abroad, the cost of treatment includes EVERYTHING! But the prices are an order of magnitude higher, not for the valve and suture material, but for the operation itself. Although the prosthesis itself and suture material cost two times, or even three times less. Abroad, doctors' services are more expensive than medicines and prostheses. That's all the difference from Russian medicine.
If you are traveling abroad, then it is better to undergo all diagnostic tests here, since they are more expensive abroad. And the operation can be performed abroad if the necessary research results are available. And if you have any questions about heart surgery in one of the best clinics for the quality of treatment in Europe (Denmark) - write, I will answer everyone - [email protected]
comphones in Moscow: 8(926)8856545
Take care of your health, treat your heart in the best clinics in Europe with reasonable savings...!
Source: https://denmark-surgery.livejournal.com/1159.html