Atherosclerosis is rightly considered one of the main causes of mortality from cardiovascular diseases. Such vascular damage is fraught with very serious complications - heart attacks, strokes, aneurysms - the progression of which can cause disability or death.
Many specialists, groups of scientists and pharmaceutical companies are developing new drugs and active ingredients to combat various forms of this disease. Next, the modern classification of atherosclerosis is considered depending on its location and etiology.
Features of the disease
Atherosclerosis affects mainly large arteries - the heart, brain, lower extremities; less often, the pathology affects the vessels of the kidneys and intestines. The main mechanism for the development of the disease is a violation of lipid metabolism.
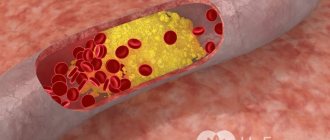
In blood plasma, fats are combined with proteins and form lipoproteins. They settle on the endothelium of the arteries and form a fatty spot, which grows over time, then ulcerates and calcifies.
This pathological process develops slowly, over several decades. The clinical picture of atherosclerosis occurs only when a cholesterol plaque blocks the lumen of the vessel by more than 50%. Therefore, the disease is diagnosed only at 50-60 years of age.
Complications of atherosclerosis
If left untreated, atherosclerosis can cause the development of:
- coronary heart disease;
- myocardial infarction;
- cerebral ischemia;
- stroke;
- inflammatory processes in the gastrointestinal tract;
- necrosis of intestinal areas;
- aortic aneurysm;
- senile dementia (dementia);
- renal failure.
Obliterating atherosclerosis of the lower extremities may cause the need for leg amputation (if gangrene occurs).
Risk factors for the disease
Atherosclerosis is a polyetiological disease that has many risk factors.
Among them are:
- Hereditary predisposition - atherosclerosis, like many somatic diseases, can be transmitted at the genetic level.
- Age – the disease is diagnosed only after 50 years; this is due to the slow growth of lipid plaque, deterioration of metabolism in cells, and a decrease in the ability to restore vascular tissue.
- Excess body weight and obesity - excess weight contributes to an increased content of lipid substances in the blood, increasing the risk of developing metabolic pathologies.
- Smoking – substances contained in cigarettes lead to dysfunction of the inner wall of blood vessels; In addition, smoking increases blood clotting - the risk of thrombosis increases, which significantly worsens the course of the disease.
- Physical inactivity – a passive lifestyle reduces cardiac output and reduces the volume of circulating blood; This condition impairs the elasticity of blood vessels and thickens their walls.
- Poor nutrition - excessive consumption of food containing large amounts of fat and salt accelerates the growth of lipid plaques - the disease begins to progress faster.
- Metabolic diseases - for example, in diabetes mellitus, excess glucose in the blood gradually damages the vascular endothelium, facilitating the formation and growth of cholesterol plaques.
- Arterial hypertension - increased pressure gradually causes dysfunction of the vascular endothelium and narrows their lumen.
Over time, such risk factors inevitably lead to arterial stenosis, provoking the development of an obliterating form of atherosclerosis.
In this condition, occlusion (complete blocking of the lumen) of the vessel often occurs with the development of a heart attack, stroke, rupture of an aneurysm, the occurrence of trophic ulcers and gangrene.
Prevention of atherosclerosis
The main preventive measure is a healthy lifestyle. A varied diet is recommended that can satisfy all the body's needs for vitamins, minerals and other important substances. It is best to consult a doctor to plan your diet. Giving up bad habits (smoking, drinking alcohol) will have a positive effect on the condition of blood vessels. It is also necessary to devote time to daily physical activity: moderate exercise helps normalize lipid balance in the body.
Since infectious and endocrinological diseases increase the risk of developing atherosclerosis, it is important to undergo a general medical examination annually for timely diagnosis and treatment. People over 40 are also recommended to take a blood test for cholesterol once a year: this will help identify disorders in the early stages.
Pathological anatomy of the disease
The main mechanism for the development of atherosclerosis is atherogenesis. The emergence of atherosclerotic plaques is facilitated by a host of pathological processes in the endothelium of the arteries: the release of leukocytes from it, cell necrosis, degeneration of elastin, as well as thinning and decreased elasticity of the vessels themselves.
Atherogenesis has several stages:
- The initial stage is the appearance of lipid stripes and spots, which are areas of light gray or yellow color and have a flat shape.
- The formation of lipid clots rising above the surface of the vascular endothelium, having a heterogeneous structure and a tendency to merge.
- The formation of atheroma, when the plaque ulcerates and ruptures, causes the formation of blood clots, which threatens the occlusion of large vessels.
- Plaque calcification is the deposition of calcium salts in it, leading to its hardening and deformation of the affected area of the artery.
Most often, atherosclerosis is diagnosed at the stage of atheroma formation or plaque calcification, since at earlier stages the disease rarely manifests itself clinically.
Classification of atherosclerosis by localization
Atherosclerosis can affect various arteries of the human body - vessels of the heart, brain, kidneys, and limbs. Let us consider in more detail the stages of development and clinical manifestations of the disease in these vessels.
Aorta
Damage to the aorta occurs in several stages:
- The stage of formation of a lipid stain, the duration of which varies and depends on the number of risk factors affecting the body.
- Fibrous stage - the lipid plaque increases due to the proliferation of connective tissue.
- Stage of atherocalcinosis - the plaque accumulates microthrombi, ruptures, ulcerates and succumbs to calcification, narrowing a significant part of the lumen of the artery.
Due to the large caliber of the aorta, symptoms of its damage appear very late, since in order to block the lumen the lipid plaque must gain significant size.
The aorta has several sections: the arch and brachiocephalic trunk, the thoracic and abdominal parts.
Brachiocephalic vessels supply blood to the brain and spinal cord, so when they are damaged, complaints of pain in the head, dizziness, noise in the head and ears, and orthostatic fainting occur.
With atherosclerosis of the thoracic aorta, the clinical picture is quite poor - only periodic chest pain and paresthesia of the upper extremities occur.
Symptoms increase with the development of a complication - an aneurysm. There is a burning pain behind the sternum; when compressed by protrusion of the trachea, shortness of breath and cough occur, the esophagus - dysphagia and belching.
Symptoms of damage to the abdominal aorta are associated with chronic ischemia and hypoxia of the internal organs of the abdominal cavity. They manifest themselves as abdominal pain, peristaltic disorders, and weight loss.
Arteries of the brain
When the vessels supplying the brain are damaged, discirculatory encephalopathy occurs - this is a slowly progressive disease of the blood vessels of the brain.
It has three stages of development:
- Initial stage. Characterized by decreased memory, fatigue, dizziness, and sleep disturbances.
- Compensatory stage. Cognitive disorders occur: memory loss, impaired thinking and attention, emotional lability, decreased resistance to stress.
- Decompensatory stage. Signs of dementia develop: decreased self-criticism, lethargy, gait disturbance, urinary and fecal incontinence.
In addition to chronic processes, with ischemia of cerebral vessels, ischemic stroke can occur - this is an emergency condition requiring emergency care . Its symptoms include facial asymmetry, limb paresis, aphasia and dysphagia (impaired speech and swallowing).
Arteries of the lower extremities
The stages of atherosclerosis of the vessels of the lower extremities are divided depending on the degree of tolerance to physical activity, the intensity of pain in the legs, as well as the severity of clinical signs.
The following classification is proposed:
- Compensatory stage. The disease practically does not manifest itself in any way; the person is only bothered by chilly feet and increased sensitivity to cold. Pain in the legs occurs when walking more than 1000 m.
- Subcompensatory stage. There is a decrease in the sensitivity of the fingers, and paresthesia periodically occurs. With the development of intermittent claudication over 900 m, atherosclerosis of the 2nd degree with the letter A is recognized, within 200-900 m – 2nd degree B.
- Decompensatory stage. There is a decreased temperature of the extremities, pallor and dry skin. The phenomena of paresthesia occur at rest, intermittent claudication torments when walking 100 m.
- Stage of complications. There is a complete disruption of blood flow - the limbs acquire a bluish tint. Trophic ulcers and necrotic areas appear. Gangrene often develops.
Arteries of the heart
Atherosclerotic damage to the blood vessels of the heart leads to insufficient nutrition of the heart muscle, triggering anaerobic processes in it.
Acute lack of oxygen and other substances provokes the development of pain syndrome (angina attack) up to tissue necrosis (infarction), chronic - to the degeneration of muscle into connective tissue (cardiosclerosis).
The following stages of development of cardiac atherosclerosis are distinguished:
- The first or initial stage of cardiac atherosclerosis has no clinical manifestations. Heart damage is diagnosed only on a cardiogram - a shift in the ST interval occurs, which is related to physical activity. At this stage, dystrophic changes in the heart muscle begin to occur.
- The second stage is characterized by ischemia of tissue areas to the point of necrosis. Clinically it manifests itself in the form of attacks of angina pectoris, heart attack: burning, pressing pain behind the sternum with irradiation to the left arm and shoulder blade, and difficulty breathing often occurs. The ECG shows changes in the ST interval, Q and T waves.
- The third stage is characterized by the appearance of connective tissue scars (cardiosclerosis). Such areas, depending on their extent, lead to the development of complications - arrhythmias, atrioventricular block, chronic heart failure. The cardiogram shows a shift of the electrical axis of the heart (EOS) to the left, signs of rhythm disturbances, and previous myocardial infarction.
Kidney arteries
The vessels of the kidneys are most often exposed to atherosclerotic lesions in the area of the mouth and adjacent areas. In this case, the disease also has three stages of development:
- The first stage is when ischemic changes occur, which lead to nephrogenic arterial hypertension. A person is concerned about periodic increases in peripheral blood pressure, which do not immediately respond to antihypertensive therapy.
- The second stage is characterized by incomplete vascular occlusion and thrombus formation. Dystrophic changes occur in the parenchyma of organs, and symptoms of impaired blood flow begin to appear.
- At the third stage of renal atherosclerosis, necrotic changes occur in organ tissues and chronic renal failure develops. Swelling of the limbs and face, dryness and itching of the skin appear. This pathology increases the load on the cardiovascular system.
The last stage is dangerous due to the development of acute renal failure - the kidneys stop functioning and signs of intoxication appear. This pathology can result in the development of coma followed by death.
Diagnostics
A cardiologist diagnoses atherosclerosis. The doctor collects an anamnesis, then a general examination is carried out, during which the doctor palpates (feels) large arteries, measures the patient’s height and weight, listens to the heart and aorta, and measures pressure. Based on the results of the examination, the following signs of atherosclerosis can be identified: edema, trophic disorders (local disorders of blood and lymph circulation), deformation of nails, increased function of the sebaceous and sweat glands, lack of hair on the extremities. Also an alarming symptom is sudden weight loss.
If there is suspicion of atherosclerosis, functional tests are performed. These are tests using disturbing actions (small physical activity, changes in body position, pressing on parts of the body, etc.).
The following research methods are used:
- blood test for cholesterol and sugar;
- X-ray examination (to study the condition of the aorta);
- angiography (radiography using a contrast agent allows to detect obliteration - narrowing or closure of the lumen of the artery);
- magnetic resonance imaging (to study the walls of the arteries and the plaques that have formed on them)
- Doppler ultrasound (to assess blood flow);
- Ultrasound of the aorta;
- echocardiography (ultrasound examination of the heart and valve apparatus).
Additionally the following can be carried out:
- cardiac stress tests (a test performed to determine the critical load on the heart);
- coronary angiography (x-ray method to detect coronary heart disease);
- Ultrasound of the abdominal organs;
- lipid profile (a comprehensive blood test that makes it possible to assess the lipid balance in the body).
If there are concomitant diseases, treatment and diagnosis may require the help of an endocrinologist, nephrologist, urologist, phlebologist, neurologist, or therapist.
Classification of atherosclerosis by morphogenesis
The emergence and development of cholesterol plaque is a long process. In the morphogenesis of atherosclerosis, six stages of its formation are distinguished. Let's take a closer look at each of them.
First stage
The first stage is prelipid. At this stage, favorable conditions occur for the formation of atherosclerotic plaques:
- In the blood plasma there is an increased content of low and very low density lipoproteins (LDL and VLDL), large protein molecules;
- There is an increase in the permeability of the membrane of the vascular wall, it swells, accumulating protein-fatty compounds, fibrin, microthrombi;
- The level of polysaccharides in the blood increases, which simplifies the attachment of LDL, total cholesterol and protein compounds to the endothelium of the affected vessel;
- Microdamages of the intima of the artery are formed, and connective tissue grows.
The rate of transition from the first stage to the second depends on how quickly the enzymes are able to break down lipid substances that attach to the damaged area of the vessel.
Second stage
This stage is called lipoidosis. When enzymes no longer cope with lipid deposits, metabolic processes increase and the formation of an atherosclerotic plaque occurs.
The upper layers of the endothelium are saturated with “bad” lipoproteins - fatty spots and stripes appear that have a yellowish or light gray color. At this stage, lipid plaques are very small in size and do not interfere with blood circulation.
The disease does not manifest itself clinically.
Third stage
The third stage is called liposclerosis. As the pathology develops, inflammatory processes occur at the site of formation of the primary plaque.
Connective tissue fibers rapidly grow into the affected area of the blood vessel - a fibroid plaque develops, along the edges of which capillaries are formed, supplying it with lipids and proteins.
At this stage, the lipid plaque begins to block the lumen of the artery, but this is not enough for the development of the clinical picture of the disease.
Fourth stage
This stage is called atheromatous. At this time, the atherosclerotic plaque accumulates a sufficient amount of elastic, collagen and lipid fibers and prepares for decay. Inside, a heterogeneous mass of particles of cholesterol and triglycerides is formed, which is still covered with a capsule. Often it also contains a hematoma.
Pathological processes occurring in the plaque deepen it into the muscle layer of the vessel. The mass enlarges, causing incomplete occlusion of the artery. At this stage, symptoms of the disease begin to appear.
Fifth stage
At this time, ulceration of the atherosclerotic plaque occurs - it ruptures, its particles are carried through the bloodstream. On the smooth, even intima of the artery, an erosive area is formed - a favorable place for platelets to settle.
As a result of such processes, blood clots form on the walls of blood vessels, and complications of atherosclerosis arise - myocardial and cerebral infarctions.
Sixth stage
The next stage is called atherocalcinosis and is the final stage in the development of atherosclerotic plaque. After its rupture, calcium salts precipitate at the site of the formed blood clot. Gradually it calcifies, grows and thickens the affected area of the vessel.
Such processes lead to permanent stenosis and impaired circulation of tissues and organs, causing chronic ischemia.
Treatment
Treatment of atherosclerosis is carried out comprehensively. The patient is prescribed a diet aimed at reducing blood cholesterol levels and normalizing lipid balance: animal fats, simple carbohydrates, and salt are limited. The diet is developed by a doctor; it is not recommended to create a diet on your own. The patient also needs to give up bad habits, especially smoking. Gentle exercise will also help normalize lipid levels. You should consult your doctor about exercises, duration and frequency of exercises.
Drug therapy is aimed at achieving the following goals:
- removal of excess cholesterol from the body;
- reducing the body's production of cholesterol;
- fight against infections.
Patients may be prescribed:
- statins (drugs that reduce cholesterol production in the body);
- medications with nicotinic acid (normalize lipid levels);
- fibrates (reduce the production of fats in the body);
- sequestrants (remove bile acids from the intestines that are formed when cholesterol levels are reduced);
- estrogens (hormone replacement therapy for women during menopause).
If conservative treatment does not give the desired result or an artery is blocked (or there is a high risk of such an outcome), surgery is performed. The following surgical methods are used today:
- Endarterectomy. In the problem area, the artery is cut and the atherosclerotic plaque is removed from its wall. As a result of the operation, the lumen of the artery expands, and blood flow in it is normalized. This method is not used if the patient has diabetes mellitus, malignant tumors, congestive heart failure, hypertension, angina pectoris, or within six months after a heart attack.
- Angioplasty. This is a minimally invasive (low-traumatic operation) that uses a special device with a catheter on one side and a small balloon on the other. The balloon is inserted into the lumen of the vessel through a small puncture in the skin and inflated using compressed air. Under this influence, the artery expands, and the plaque is evenly distributed along its wall. After this, the balloon is “deflated” and removed from the vessel.
- Stenting . The operation is performed using a stent - a metal frame. First, the artery is widened (usually angioplasty is used for this purpose), and then a stent is installed into it. The frame expands the lumen of the vessel, thereby restoring blood flow.
- Shunting. During the operation, an artificial connection (shunt) is created between two points, bypassing the severely narrowed section of the artery. As a result of surgical intervention, normal blood supply to tissues is restored. This method is often used for atherosclerosis of the lower extremities.
- Vascular prosthetics. The affected artery is completely replaced with an artificial one.
In some cases, several surgical methods may be combined.
Features of the course of the disease
Atherosclerosis is a chronic disease that has a wavy course. This means that cholesterol plaques go through all stages many times, appearing in the same or another place.
There are three phases of the course of atherosclerosis:
- Active phase (progression);
- Passive phase (stabilization);
- Regression phase.
The first (active) phase is characterized by the deposition of lipid and protein substances on previously damaged areas - the lipoid stage occurs. Then the plaque goes through all stages of its development, calcifies and the process stabilizes - the second phase begins.
During the regression phase, enzymes gradually break down the lipid plaque, and the site of its formation is overgrown with connective tissue.