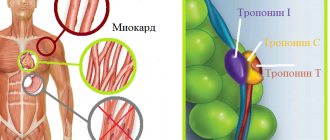
Differential diagnosis of myocardial infarction is used to exclude errors.
The fact is that there are diseases that have symptoms similar to a heart attack. So, for example, the gastralgic form of a heart attack can be perceived as food poisoning - and the necessary actions are completely different than for a heart attack. The clinical picture of a typical myocardial infarction (MI) is manifested by a number of fairly specific symptoms: severe pain in the chest, lasting more than 20 minutes and not relieved by nitrate drugs, shortness of breath, fear of death, etc. In this regard, the diagnosis of classic myocardial infarction is rarely difficult.
As a rule, with a typical course of an attack in the first half hour from the onset of the disease, only differential diagnosis of myocardial infarction and angina is performed.
For reference. However, with an atypical course of an attack, MI can be disguised as many different diseases, including gastrointestinal and pulmonary pathologies. Therefore, competent and quick differential diagnosis of a heart attack plays a vital role in timely diagnosis.
How can atypical myocardial infarctions manifest?
For reference. With an atypical course of an MI attack, there may be no severe pain symptoms (most often, such forms of MI are observed in people with diabetes). In this case, the main manifestation of myocardial infarction will be acute, severe shortness of breath symptoms.
In abdominal forms of myocardial infarction, patients are bothered by abdominal pain, tachycardia, nausea, shortness of breath, etc.
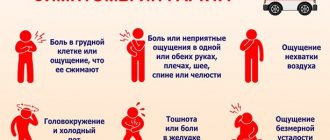
Also, a manifestation of atypical myocardial infarction may be:
- intense toothache, combined with shortness of breath and tachycardia;
- severe weakness;
- fear of death;
- fainting conditions;
- severe dizziness;
- changes in blood pressure, etc.
In this regard, in order to suspect an atypical myocardial infarction when examining a patient, it is important to assess the presence of cardiovascular risk factors (age, history of coronary artery disease, obesity, etc.).
What diseases are differentially treated? diagnosis of myocardial infarction
Diff. Diagnosis of a heart attack is carried out with:
- other cardiovascular pathologies (vasospastic forms of angina, aortic stenosis, inflammatory damage to the myocardium and pericardium, dissecting aortic aneurysms, Brugada syndrome, SVC syndrome, etc.);
- gastrointestinal pathologies (esophageal spasms, esophageal ulcers, exacerbation of gastritis, perforation of ulcers, acute forms of pancreatitis and cholecystitis, an attack of appendicitis);
- pulmonary pathologies (pulmonary embolism (PE), preumothorax, inflammatory lesions of the pleura, etc.);
- panic attacks;
- acute cerebrovascular accidents;
- subarachnoid hemorrhages;
- radicular syndrome, etc.
For reference. In clinical practice, differential diagnosis of myocardial infarction is most often carried out with attacks of angina pectoris, dissecting aortic aneurysms, pulmonary embolism, acute pericarditis and myocarditis, acute pancreatitis, gastric ulcers, and attacks of intercostal neuralgia.
Distinctive diagnosis of angina and other cardiovascular diseases
- The sensation of pain during a heart attack differs from a regular attack of angina in intensity and duration. The pain does not go away after taking cardiac and painkillers. The attack stops only after taking narcotic painkillers. During this period, a person experiences fear of death and emotional agitation.
Sometimes the resulting pain is too strong, and patients begin to rush and scream. During overexcitement, they may begin to work physically, not realizing the seriousness of the situation.
First of all, it is necessary to correctly diagnose angina and determine its form.
Atypical forms of angina pass painlessly or with mild discomfort. A heart attack in such situations is diagnosed after it has happened, during an ECG.
- Inflammatory pathologies of the heart muscle are associated with previous infection:
- during myocarditis, the pain is constant and stops after undergoing anti-inflammatory therapy;
- Diastolic heart murmur appears with endocarditis. An echocardiogram shows valvular damage, and patients are febrile.
- Defects of the heart muscle can be accompanied by various pain syndromes. They can be cutting, constant, aching even without physical activity. Defects are diagnosed by direct or indirect auscultation and echocardiogram.
- High blood pressure is often accompanied by pain in the heart. Mostly they are aching in nature and appear during high blood pressure. Hypertensive patients are at risk of developing angina.
- Pulmonary embolism (PE) is accompanied by:
- severe pain syndrome;
- hemoptysis;
- shortness of breath.
People with pulmonary embolism experience a decrease in blood pressure and an increase in temperature. Without emergency medical care, death is possible.
The main differential diagnostic criterion is direct signs of myocardial necrosis
- With cardiac tumors, regardless of their origin, pain appears during tumor growth into the pericardium. The pain becomes stronger when inhaling, and pericardial friction sounds may occur. Patients often present with congestive failure.
- Young people are more likely to suffer from vegetative-vascular dystonia. The pain is stabbing in nature. During the examination of patients with VSD, there were no symptoms of organic damage or ischemia on the ECG.
- People with alcohol dependence develop alcoholic cardiomyopathy. The pain is nagging, usually occurs on the second day after drinking alcohol, and is not related to physical activity.
Differential diagnosis of myocardial infarction and dissecting aortic aneurysm
Aortic dissection (dissecting aortic aneurysm) is a rupture of the aortic wall accompanied by leakage
blood between the layers of the aortic wall. In this case, blood accumulating between the layers of the aortic wall provokes its further dissection.
The main reasons for the development of dissecting aortic aneurysm are:
- severe atherosclerotic damage to the aorta;
- hypertension with frequent pressure surges and the development of hypertensive crises;
- focal necrotic lesions of the aorta with bacterial emboli caused by acute infectious pathologies;
- damage to the aorta due to spondylitis, malignant lesions of the esophagus, penetration of peptic ulcers, etc.;
- damage to the aorta by a foreign body;
- closed injuries to the chest or abdomen.
For reference. An attack during aortic aneurysm dissection always begins with the appearance of sharp, intense pain in the chest (which is very similar to a heart attack). The pain often radiates to the left shoulder blade and arm.
In isolated cases, pain during dissection of the aortic aneurysm can radiate to the jaw. Against the background of severe pain, motor agitation is often observed.
Krasnoyarsk medical portal Krasgmu.net
Angina pectoris (obsolete angina pectoris (lat. angina pectoris)) is a disease characterized by a painful sensation or a feeling of discomfort behind the sternum.
Differential diagnosis of angina pectoris. Diagnosis of angina pectoris includes a set of measures consisting of a clinical examination, laboratory and cardiological studies. But differential diagnosis of angina occurs using an electrocardiogram.
Pain from angina pectoris can radiate to the epigastric region (stomach area) and be accompanied by nausea and heartburn. This pain is often confused with an attack of pancreatitis, which makes diagnosis and timely initiation of treatment difficult.
Differential diagnosis of myocardial infarction and pulmonary embolism
PE is a pathology that is a blockage of the branches or main trunk of the pulmonary artery (pulmonary artery) with blood clots (emboli). The source of blood clots in pulmonary embolism is most often the large veins of the legs or pelvis.
In some cases, PE may be associated with fatty, airborne, tumor, etc. emboli.
At a young age, pulmonary embolism is more often recorded in women, however, after fifty-five years, symptoms of pulmonary embolism more often occur in men.
The cause of the development of symptoms of pulmonary embolism is increased thrombus formation in the vessels, caused by:
- impaired blood flow;
- inflammatory or traumatic damage to the vascular wall;
- hypercoagulation and inhibition of fibrinolysis.
For reference. Most often, PE occurs in patients with deep vein thrombosis of the lower extremities, therefore, when making a differential diagnosis of PE and myocardial infarction, the doctor pays attention to the condition of the patient’s veins.
PE can also occur against the background of acute infectious pathologies, hip fractures, malignant neoplasms, polycythemia, erythrocytosis, etc.
The pain syndrome during pulmonary embolism is similar to an attack during myocardial infarction. The pain is sharp, burning, can radiate to the arm, shoulder blade, etc., and is combined with intense shortness of breath symptoms.
Differential diagnosis of angina pectoris
Angina pectoris (“angina pectoris” or Heberden’s disease) is a pathology, the main symptom of which is pressing pain in the chest area.
Pain in the heart area is a very common symptom, but the cause of its occurrence may not be angina pectoris. They can be caused by vegetative-vascular dystonia, thoracic osteochondrosis and other diseases.
The doctor knows the exact symptoms of the pathologies and is sure to carry out a differential diagnosis of angina pectoris before prescribing treatment.
What can cause angina?
The causes that cause pathology are divided into several groups:
- Diseases of the cardiovascular system:
- IHD;
- inflammatory pathologies (myo-, endocarditis, aortitis);
- abnormal development of the heart muscle, coronary vessels;
- TELA;
- neoplasms of the heart muscle;
- VSD;
- alcoholic cardiomyopathy;
- primary cardiomyopathy.
Failure to recognize angina pectoris can cause irreparable harm to the patient
- Systemic connective tissue lesions.
- Diseases of the upper and lower respiratory tract (bronchitis, pneumonia, tonsillitis).
- Pathologies of the abdominal organs and diaphragm. These can be either congenital or acquired defects.
- Diseases of the spinal column and shoulder girdle.
- Climacteric cardiopathy NRC.
There are many reasons for chest pain. Although the symptoms are somewhat identical, they have clinical and diagnostic differences.
Distinctive diagnosis of angina and other cardiovascular diseases
- The sensation of pain during a heart attack differs from a regular attack of angina in intensity and duration.
The pain does not go away after taking cardiac and painkillers. The attack stops only after taking narcotic painkillers. During this period, a person experiences fear of death and emotional agitation.
Sometimes the resulting pain is too strong, and patients begin to rush and scream. During overexcitement, they may begin to work physically, not realizing the seriousness of the situation.
First of all, it is necessary to correctly diagnose angina and determine its form.
Atypical forms of angina pass painlessly or with mild discomfort. A heart attack in such situations is diagnosed after it has happened, during an ECG.
- Inflammatory pathologies of the heart muscle are associated with previous infection:
- during myocarditis, the pain is constant and stops after undergoing anti-inflammatory therapy;
- Diastolic heart murmur appears with endocarditis. An echocardiogram shows valvular damage, and patients are febrile.
- Defects of the heart muscle can be accompanied by various pain syndromes. They can be cutting, constant, aching even without physical activity. Defects are diagnosed by direct or indirect auscultation and echocardiogram.
- High blood pressure is often accompanied by pain in the heart. Mostly they are aching in nature and appear during high blood pressure. Hypertensive patients are at risk of developing angina.
- Pulmonary embolism (PE) is accompanied by:
- severe pain syndrome;
- hemoptysis;
- shortness of breath.
People with pulmonary embolism experience a decrease in blood pressure and an increase in temperature. Without emergency medical care, death is possible.
The main differential diagnostic criterion is direct signs of myocardial necrosis
- With cardiac tumors, regardless of their origin, pain appears during tumor growth into the pericardium. The pain becomes stronger when inhaling, and pericardial friction sounds may occur. Patients often present with congestive failure.
- Young people are more likely to suffer from vegetative-vascular dystonia. The pain is stabbing in nature. During the examination of patients with VSD, there were no symptoms of organic damage or ischemia on the ECG.
- People with alcohol dependence develop alcoholic cardiomyopathy. The pain is nagging, usually occurs on the second day after drinking alcohol, and is not related to physical activity.
Differential diagnosis of myocardial infarction and angina (table)
There are several types of diagnostics and symptoms, all of them can be presented in table form:
| Disease | Symptoms and their characteristics |
| Angina pectoris |
|
| Pulmonary artery embolism |
|
| Pericarditis |
|
| Acute coronary insufficiency |
|
| Unexpected entry of air or gas into the pleural cavity |
|
| Acute radicular pain (cancer, radiculitis, spinal tuberculosis) |
|
| Acute pleurisy |
|
Distinctive characteristics of gastrointestinal diseases
Pathologies of the abdominal organs are often accompanied by involuntary pain in the area of the heart muscle:
- Ulcers of the stomach and duodenum sometimes manifest as chest pain. Therefore, the doctor should pay attention to the medical history and find out if the patient has a digestive disorder from the gastrointestinal tract. If the patient’s pain is associated with eating, and also has eating disorders, then after an ECG and exclusion of cardiac pathology, he is prescribed an endoscopic examination of the gastrointestinal tract and an x-ray of the stomach.
- Displacement of the abdominal organs into the thoracic cavity through a natural or pathological opening can manifest itself as cardialgia. Pain occurs during coughing, after eating, due to intestinal bloating. The patient feels better after removing gases through the mouth, vomiting, and drinking plenty of fluids. Diaphragmatic hernia is diagnosed by fluoroscopy and fibrogastroduodenoscopy.
An experienced doctor knows well the “masks” of angina and knows how the differential diagnosis of angina is carried out
Diff. diagnosis of angina pectoris in pathological changes in the musculoskeletal system
If there are degenerative disorders in the intervertebral discs, the pain becomes stronger in certain body positions or when moving, for example, if you move your arm back. Pain can be relieved only with the help of NSAIDs; Nitroglycerin does not block it.
An attack of osteochondrosis intensifies with palpation of the pectoralis major muscle at certain points located at the points of attachment of the muscles to the sternum.
With intercostal neuralgia, pain can be localized on the left side. Therefore, it can easily be mistaken for “toad angina.” During diagnosis, upon palpation, the pain will intensify in several points - in the center of the axillary line, in front at the edge of the sternum, in the intercostal spaces.
Intercostal neuralgia. If neuralgia is localized on the left, then the pain can be confused with angina pectoris
Detection of unstable angina
The unstable form of “angina pectoris” (rest angina) is often manifested by pain. Small focal infarction is the main condition that should be considered when distinguishing unstable angina from other pathologies.
Diff. Diagnosis of unstable angina is carried out using an electrocardiogram, which shows changes in the final part of the ventricular complex. But a normal ECG does not confirm the absence of pathology. A resting ECG helps identify large focal myocardial infarction.
Holter ECG monitoring makes it possible to learn about the changes that are characteristic of resting angina, especially episodes of painless decrease in blood supply to the myocardium.
Echocardiography in many cases provides insufficient information to determine Heberden's disease, since pathological changes in the walls of the left ventricle can only be detected during pain.
If surgery is prescribed, the doctor will recommend coronary angiography. But only if the patient has signs of a severe course of the disease. Using this study, you can find out about the location of blood clots and stenoses in the coronary arteries.
Conclusion
Thus, it is impossible to correctly differentiate the diagnosis of angina pectoris at home and without certain knowledge. Only an experienced specialist can determine the source of pain during the disease.
He will order an examination of the patient, and based on the results obtained, he will make the correct diagnosis and prescribe treatment.
To make a correct diagnosis, the patient should visit not only a cardiologist, but also a neurologist, surgeon, and therapist.
Source: https://meningreen.ru/stenokardiya/differencialnaya-diagnostika-stenokardii.html
Differential diagnosis of MI and angina attack
Angina pectoris is a clinical variant of coronary heart disease, manifested by intense pressing or burning pain in the chest. Pain syndrome is often associated with stress, physical fatigue, fear, etc.
The pain is usually less intense than during myocardial infarction and always lasts less than fifteen (maximum twenty minutes).
Attention. It should be noted that the pain syndrome of angina pectoris is effectively relieved by taking nitrate drugs (Nitroglycerin).
ACQUIRED HEART DEFECTS.
AORTIC STENOSIS
Pain in the heart area is a characteristic symptom of aortic heart defects. The ischemic variant of aortic stenosis was described by Vasilenko in 1963. The cause of ischemia is that with stenosis, pronounced hypertrophy of the left ventricular myocardium occurs, a significant increase in its mass, vascular collaterals do not have time to develop and this leads to relative insufficiency of coronary circulation.
In the stage of compensation for aortic stenosis, the pain has the character of cardialgia, but as the defect progresses, it becomes true angina. Although there are some peculiarities: angina pectoris with aortic stenosis is not always clearly related to physical activity, nitrates do not always help, attacks last longer, and the intensity of pain is less pronounced.
MITRAL VALVE PROLAPSE can cause pain very similar to angina. They are of a pressing or burning nature, localized in the III-IV intercostal space to the left of the sternum, can last for hours, intensify with physical and emotional stress, are often accompanied by extrasystole and occur, as a rule, at a young age.
1. Unpleasant sensations or pain in the heart area.
2. Feeling of lack of air and feeling of dissatisfaction with inhalation
3. Palpitation or sensation of pulsation in the precordial area.
4. Feeling lethargic, weak in the morning and increased fatigue.
5. Neurotic symptoms, irritability, anxiety, insomnia
.6. Headache, dizziness, cold and wet extremities.
1. Instability, lability of heart rate, tendency to tachycardia.
2. Lability of blood pressure with a tendency to hypertension.
3. Respiratory disorders - dyspnea, tachypnea.
4. Signs of peripheral vascular disorders - hyperemia, marbling of the skin.
5. Zones of hyperalgesia in the heart area. 6. Signs of autonomic dysfunction: local sweating, persistent dermographism.
Tags: diagnosis, tension, angina
About the author: admin4ik
« Previous entry
Acute pericarditis
Acute pericarditis is an inflammatory lesion of the serous heart membrane. As a rule, the disease develops as a complication of infectious pathologies, autoimmune diseases, etc. In isolated cases, idiopathic pericarditis develops.
The development of pericarditis is accompanied by the appearance of excess fluid in the pericardial cavity or the formation of fibrous adhesions.
Unlike myocardial infarction, symptoms of pericarditis are often preceded by bacterial or viral infections.
For reference. Pain with pericarditis is less intense, intensifying with inspiration. It should also be emphasized that pain depends on body position, which is not typical for MI.
During auscultation, the appearance of a pericardial friction noise is noted.
The electrocardiogram with pericarditis shows concordant ST elevation. Pathological QS and Q are absent.
For reference. In a biochemical blood test, an increase in markers of myocardial necrosis may be noted due to inflammatory damage to the subepicardial zone.
Emergency medicine
In some patients with a typical clinical picture of angina pectoris and positive stress tests (according to objective criteria), coronary angiography does not find any changes in the coronary arteries; Such patients have no signs of spontaneous angina. In these cases, we can talk about coronary artery disease with unchanged coronary arteries. In the English-language literature, this type of pathology is called “syndrome X.”
Special studies show that in these patients the ability of the coronary arteries to dilate is significantly reduced, which is detected when assessing coronary blood flow using argon or rubidium radionuclides under the conditions of a dipyridamole test. When performing a myocardial biopsy in these patients, electron microscopy reveals degenerative changes in cardiomyocytes.
Thus, both the decrease in coronary reserve and biopsy data allow us to think of “syndrome X” as the initial manifestations of dilated cardiomyopathy. This diagnosis becomes even more reliable if patients have persistent or transient (appearing under load) blockade of the left branch of the His bundle.
Patients with hypertrophic cardiomyopathy, both obstructive and non-obstructive, have angina that is not caused by damage to the coronary arteries. Angina syndrome in these patients occurs due to an increase in myocardial oxygen demand. In these patients, the movement of the left ventricular wall in diastole is impaired.
Patients with hypertrophic cardiomyopathy often consult a doctor, complaining of discomfort in the heart area. Pain is not as clearly related to physical activity as with ischemic heart disease. They usually last longer and in cold weather go away rather than get worse. At the same time, many patients with hypertrophic cardiomyopathy may have typical attacks of angina.
The ECG often shows deep pathological Q waves in leads II, HI AVF, V3-V6, which are taken for traces of myocardial infarction, as well as signs of left ventricular hypertrophy, which are often interpreted erroneously. The bicycle ergometer test is often positive. On FCG, in contrast to valve stenosis, the systolic murmur is late.
X-rays do not detect post-stenotic dilatation of the aorta and calcification of the aortic valve. The ability to detect this disease has increased significantly thanks to echocardiography, which makes it possible to establish a thickening of the upper part of the interventricular septum of more than 1.5 cm. Unlike valvular stenosis, the degree of thickening of the interventricular septum exceeds the degree of thickening of the wall of the left ventricle.
With mitral valve prolapse syndrome, there is a pressing or burning pain in the third or fourth intercostal space to the left of the sternum. Much less often the pain is localized behind the sternum or xiphoid process. Mild pain can last for hours, intensifying after physical and emotional stress.
Mitral valve prolapse is thought to predispose to coronary artery spasm. This syndrome is more common in patients with an asthenic build with a flat chest - with a reduced anteroposterior size. In patients with mitral valve prolapse, abnormalities of the ST segment and T wave are often detected, especially when performing an exercise test.
On FCG and during auxultation, patients exhibit a mesosystolic murmur at the apex, which is often preceded by a mesosystolic click. The diagnosis of mitral valve prolapse has improved significantly due to the widespread use of ultrasound methods of cardiac examination in the clinic. It allows you to detect prolapse of one or both mitral valve leaflets into the atrium.
We suggest you read: Extrasystole in children: ventricular, causes, treatment, symptoms
Nonspecific aortoarteritis. This disease, manifested by high arterial hypertension, is characterized by widespread inflammatory damage to the aortic arch, thoracic and abdominal sections of the aorta and its branches. In some patients, the inflammatory process may spread to the coronary vessels, which leads to angina syndrome. In the pathogenesis of angina in these patients, the occurrence of left ventricular hypertrophy is important.
If angina is suspected, a stress test and selective coronary angiography are necessary. For nonspecific aortoarteritis, the most typical lesion is the ostia of the coronary arteries, but proximal and even distal sections may be involved.
Valvular stenosis of the aortic mouth, like arterial hypertension, leads to overload and hypertrophy of the left ventricle, increasing the myocardial oxygen demand. The shortening of the period of diastolic filling of the left ventricle observed with a defect of this type contributes to a decrease in coronary blood flow. These patients often complain of pain in the heart area. In the early stages of the disease, they have the character of cardialgia, and with severe aortic stenosis, typical attacks of angina occur.
If a systolic murmur is heard in the aorta in patients with angina pectoris, then it is necessary to conduct all available diagnostic studies aimed at identifying aortic stenosis. The diagnosis of aortic stenosis is made on the basis of the characteristic systolic murmur (diamond-shaped murmur on a phonocardiogram), physical, radiological and electrocardiographic signs of left ventricular hypertrophy. X-rays often reveal calcification of the aortic valve.
Echocardiographic data are of great differential diagnostic importance. Detection of aortic stenosis does not exclude the simultaneous presence of atherosclerosis of the coronary arteries. Aortic stenosis in a patient with angina pectoris, combined with attacks of cardiac asthma, has a dire prognosis.
With mitral heart disease, patients often complain of pain in the heart area, in some cases indistinguishable from angina. The cause of this pain may be pulmonary hypertension, characteristic of mitral stenosis, pathogenetically associated with insufficient blood supply to the hypertrophied right ventricle.
When carrying out a differential diagnosis of angina, it is necessary to exclude aortalgia - pain that accompanies inflammatory and degenerative diseases of the aorta. With syphilitic aortitis, which is rare in our time, aortic insufficiency occurs; the pathological process also affects the mouths of the coronary arteries of the heart, which can be accompanied by typical attacks of angina. With nonspecific aortoarteritis, typical angina is rarely observed; prolonged pain in the heart area without irradiation is characteristic.
With an aortic arch aneurysm, numerous accompanying symptoms caused by compression of neighboring organs (cough, dysphagia, hoarseness, visual disturbances, fainting, asymmetrical pulse, compression of the superior vena cava) help to make a correct diagnosis.
With aortic dissection, the pain is at its maximum intensity from the very beginning. The widest irradiation is characteristic: pain, starting behind the sternum, then radiates to the neck, back, abdominal area, along the spine and even to the legs. Spider fingers and other signs of Marfan syndrome may lead the doctor to believe that chest pain is related to aortic dissection, to which these patients are predisposed.
Pain in the heart area is the most common and one of the early symptoms of myocarditis. They are varied, unlike angina pectoris, they last for hours and days. In the acute period of the disease, the intensity of pain may vary, but the pain is almost constant. When diagnosing, it is necessary to take into account the connection with a recent infection, fever, leukocytosis, and enlargement of both ventricles of the heart.
With a more or less prolonged course, cardiomegaly and heart failure become obligatory symptoms of myocarditis. Differential diagnostic difficulties more often arise with mild heart damage, when after a sore throat, flu or other infection, unpleasant sensations appear in the heart area, accompanied by changes in the final part of the ventricular ECG complex.
It should also be said about the differential diagnosis of angina and pericarditis. According to the retrosternal localization, pain with pericarditis resembles pain with angina pectoris, but unlike angina pectoris, it lasts a day or longer. In acute pericarditis, pain behind the sternum or in the area of the heart can be unbearable, and it intensifies with breathing.
With pericarditis, the irradiation of the pain may resemble angina pectoris, spreading to the clavicle and shoulder, but its connection with breathing allows for differential diagnosis. Clinical symptoms in acute pericarditis are determined by the most important pathogenetic links - inflammation of the pericarditis, accumulation of exudate and compression of the heart.
The intensity of chest pain decreases when the patient is sitting and intensifies when lying on his back. A pericardial friction rub is heard over the heart area, which persists for 1-2 weeks. The ECG reveals ST segment elevation in all leads. Unlike myocardial infarction, R waves are preserved and there are no pathological Q waves.
Differential diagnosis of myocardial infarction with myocarditis
Myocarditis is called damage to the myocardium, mainly of an inflammatory nature. Most often, the development of myocarditis is preceded by an infectious disease.
Symptoms of myocarditis, in contrast to signs of MI, are often recorded at a young age. The pain syndrome is less intense than with MI. When performing coronary angiography in patients with myocarditis, there are no signs of atherosclerotic vascular lesions.
For reference. When conducting electrocardiography in patients with myocarditis, a decrease in the amplitude of R is recorded. The dynamics of ECG symptoms typical for MI are absent in myocarditis.
Differential diagnosis of angina pectoris
Angina pectoris is a disease whose main symptom is pressing chest pain. But heart pain is an extremely common symptom, and the patient who complains of pain does not always have heart problems.
Angina pain can be confused with pain in the thoracic spine, other cardiac pathology, or vegetative-vascular dystonia. An experienced doctor knows well the “masks” of angina pectoris and knows how the differential diagnosis of angina pectoris is carried out.
It will also be useful for the patient to know what diseases can be confused with “angina pectoris” - angina pectoris, and how to distinguish them from each other.
Diseases of the heart and blood vessels (heart attack)
All causes of pain in the heart area can be divided into the following groups:
- Diseases of the heart and blood vessels:
- IHD (angina pectoris, heart attack),
- inflammatory diseases (myo-, peri-, endocarditis, aortitis),
- heart and valve defects, vascular anomalies,
- AG,
- TELA,
- heart tumors,
- vegetative-vascular dystonia,
- alcoholic cardiomyopathy,
- idiopathic cardiomyopathy;
- Systemic connective tissue lesions;
- Diseases of the lungs and bronchi, pleura and mediastinum;
- Diseases of the abdominal cavity and diaphragm;
- Menopausal cardiomyopathy;
- Pathologies of the spinal column, shoulder girdle.
These are the many reasons for the possible occurrence of pain in the chest and heart. Although these pains are characterized by a somewhat similar picture, they have their own characteristics, both clinical and diagnostic. Let's look at these features in more detail.