Mechanism of pathology
The blood supply to the heart muscle requires a constant supply of sufficient blood through the coronary arteries. The heart's need for oxygen changes depending on the conditions: physical activity, complete immobility, excitement, intoxication of the body due to infectious diseases.
In contrast to the calm state, tachycardia occurs (increased heart rate). It requires more energy, which means oxygen consumption increases, since the heart muscle cells “extract” calories for themselves only in its presence.
If the patency of the coronary arteries is good, blood flows in sufficient quantities to compensate for the necessary costs. What happens if one or all arteries are narrowed? The working heart will experience a state of “hunger”, tissue hypoxia. Clinical symptoms can be called a “cry for help.”
Description of the disease
My patients at their initial appointment often ask the question: “What is unstable angina: a syndrome, a separate disease or a stage of exacerbation of chronic ischemic heart disease?”
The most accurate definition will be the following: this is acute myocardial ischemia, which does not lead to necrosis, that is, death, of heart cells. The sudden development of symptoms is similar to the clinical picture of a heart attack, therefore, in modern cardiology, unstable angina is included in the concept of acute coronary syndrome (ICD-10 code - I20.0). This diagnosis is “working”, emergency and must be clarified within the next few hours after the patient’s admission to the hospital. The final word here lies with laboratory tests: if the markers of myocardial necrosis are elevated, it is a heart attack; if not, it is unstable angina.
Etiology
The basis of unstable angina, like any other form of coronary artery disease, is atherosclerosis - the deposition of cholesterol in the vessel wall, leading to the formation of plaques. They can grow and penetrate inside it, which will ultimately lead to narrowing of the arteries and, as a result, hypoxia (oxygen starvation of cells). The clinic is especially clearly manifested when the heart rate increases, for example, when walking quickly or climbing stairs.
A vulnerable atherosclerotic plaque leads to unstable angina: the membrane covering its lipid core becomes thinner under the influence of various factors. This triggers a chain of reactions - inflammation, thrombus formation. A characteristic clinical symptom is pain, which is accompanied by low exercise tolerance and shortness of breath.
Why is angina called “unstable”?
In medical practice, “convenient” cases are cases of diseases with clear and understandable symptoms. Angina is divided into two groups: stable and unstable.
In the case of a stable form, symptoms always arise depending on physical activity or anxiety, have a typical duration of pain, recurrence of attacks, and can be easily relieved with Nitroglycerin.
With unstable angina, there is no such clear dependence on the physical condition of the patient, the pain is long-lasting, it is impossible to predict the recurrence of attacks, or to select the necessary load limitation in treatment. Each attack can turn into an acute myocardial infarction, characterized by doctors as a “pre-infarction state.”
Features of the classification of the stable form of the disease
Stable angina pain is a type of disease when pain in the chest occurs during the period of exposure to physical loads on the body and tends to fade after they are removed. The classification of stable angina is based on the principle of identifying functional classes of the disease, depending on the nature of the physical activity provided.
The following functional classes of angina are distinguished:
- FC I – attacks rarely develop under significant physical stress;
- FC II - chest pain occurs when moving quickly over a distance exceeding 300 meters, or after climbing stairs to the height of the second and subsequent floors (the second functional class of angina is assigned to patients in whom attacks develop against the background of stress, smoking or have meteorological dependence );
- FC III - attacks appear if the patient climbed to the first floor or walked a distance of 100-300 meters at a fast pace;
- FC IV - angina pain occurs with minimal physical activity or in a calm state.
To assess the condition of patients with this type of disease, four degrees of angina are distinguished:
- Latent or angina manifestations of the first degree - a person’s habitual activity and lifestyle do not provoke the development of an attack;
- Grade 2 or mild angina – there is minimal limitation of usual physical activity;
- Moderate severity (grade 3 angina) – characterized by a noticeable limitation of motor activity due to the risk of developing cardialgia syndrome;
- Severe or stage 4 angina pectoris - attacks of angina pain occur with any physical activity.
Causes
Unstable angina has the same causes as all manifestations of myocardial ischemia:
- Damage to the coronary vessels by the atherosclerotic process when the diameter is narrowed by ½. Risk factors should be taken into account here (age after 45 years, predominantly male gender, presence of hypertension, diabetes mellitus, cigarette smoking, alcohol dependence).
- Thrombosis of cardiac vessels with increased blood clotting, decreased blood flow speed (heart failure), thromboembolism from various sources.
According to cardiologists, it is the addition of thrombosis that plays a major role in the instability of vasoconstriction. This possibility increases in patients with thyrotoxicosis and anemia.
Morning jogging can cause pain
Mechanism of symptom development
The essence of the development of a pathogenic phenomenon lies in the disruption of the supply of cardiac structures, in particular the myocardium, with blood, and therefore with oxygen and nutrients.
The duration of the development of the problem is from several months to a couple of years, then angina pectoris goes on a constantly progressive straight line with a delayed prospect of a heart attack. The possibility remains even during therapy.
One or two factors cause the onset of unstable angina:
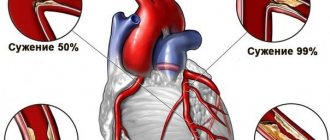
- The coronary artery narrows (stenoses).
- Less commonly, blockage of the lumen of the vessel occurs with a cholesterol plaque or thrombus.
In the first case, an increasing clinical picture is more likely, with a chronic or latent course. In the second there is an acute variety.
As soon as the blood supply structure is narrowed to 70%, typical symptoms occur. Among which are chest pains and others.
In the absence of urgent help, acute myocardial ischemia, heart attack and death from failure of the muscular organ are possible.
The prospect of recovery directly depends on the speed of first aid, its nature and literacy, and the adequacy of basic therapy in the hospital.
Clinical manifestations
There are slight differences in the symptoms of unstable angina regarding clinical forms.
General signs:
- Pain in the heart area (behind the sternum, to the left of it) manifests itself as pressing, squeezing, radiating to the left arm, shoulder blade, jaw, throat. The intensity is quite high.
- Patients are tossing about, worried about the fear of death.
- Increased sweating.
- Dizziness occurs.
- Choking as a subjective symptom.
- There is no increase in respiratory movements.
Much less often, pain is localized in the chest between the shoulder blades or in the abdomen and takes on a girdling character.
Differences from stable angina:
- attacks are repeated more often;
- the duration of attacks is more than 15 minutes;
- the pain is much stronger;
- physical activity does not provoke pain, they occur equally often at rest and during exercise;
- Nitroglycerin briefly alleviates the patient’s condition or does not help at all; some require a larger dosage of the drug.
Symptoms and clinic
Pain behind the sternum of a compressive nature
Unstable angina is characterized by intensification and aggravation of all signs and symptoms of “angina pectoris”. These signs include:
Do you trust doctors and their prescriptions?
Yes
20.4%
No
11.94%
I trust, but I check all medications for reviews on the Internet from people who have already tried them and only then do I start taking them.
50.25%
Yes, but only to appointments and doctors from paid clinics.
17.41%
Voted: 201
- Pain - pain behind the sternum of a compressive nature intensifies, places of irradiation may appear that were not observed before: shoulder, lower jaw, stomach;
- Connection with load - an attack occurs under such a load, which was previously calmly tolerated by the patient without pain, sometimes an attack may occur at rest (a sign of a spontaneous form);
- Taking nitroglycerin - to reduce the severity of pain, the patient is forced to take more nitroglycerin tablets.
It should be remembered that unstable angina sometimes develops atypically: pain in the stomach, digestive disorders, pain in the area of the heart of a stabbing, rather than squeezing nature may be observed. Sometimes only shortness of breath may be present. Therefore, to confirm the diagnosis as the disease progresses, the doctor will always prescribe a set of examinations.
Types of unstable angina
Four types of unstable angina have been identified and studied:
- new onset of the disease - the patient’s complaints have been bothering him for only one month;
- post-infarction - attacks begin in the first two days after an acute heart attack or during the acute period (8 weeks from onset);
- progressive - deterioration of health and more frequent attacks in the last 30 days;
- Prinzmetal's angina is the only type whose pathogenesis clearly demonstrates narrowing of the coronary vessels in the form of spasm rather than atherosclerosis.
If you have pain, you need to take medication
Causes of the disease
The cause of unstable angina in coronary artery disease is the rupture of a fibrous plaque previously formed in the lumen of the coronary artery. This leads to the formation of a blood clot, which prevents a complete supply of blood to the myocardium of the heart. The result is hypoxia of the heart muscle. Damage to plaque integrity can be caused by:
- excess fat deposits directly inside the plaque itself;
- inflammation;
- lack of collagen;
- deviations related to hemodynamics.
The development of unstable angina can be caused by:
- strengthening the adhesive abilities of platelets;
- hemorrhage inside the plaque;
- local narrowing of the lumen of the coronary vessels of the heart due to the release of the hormone serotonin or thromboxane;
- reduction by the endothelium of its antithrombotic properties.
Unstable angina can be caused by the following diseases and conditions of the body:
- diabetes;
- genetic predisposition if relatives have been diagnosed with IHD;
- stable increase in blood pressure;
- changes in blood quality and thickening;
- being overweight;
- high/low blood cholesterol;
- sedentary lifestyle;
- the presence of male gender characteristics in women;
- nicotine addiction;
- old age.
Advice! Treatment of this heart pathology is always carried out inpatiently.
Typical signs of Prinzmetal's angina
New York cardiologist M. Prinzmetal described a type of angina pectoris in 1959, which is included in the modern classification of unstable forms of angina pectoris. In pathogenesis, great importance is attached to the increased tone of the vagus nerve.
Features of the clinic:
- occurs more often in young men;
- attacks of pain occur at rest, there are characteristic ECG changes;
- patients do not complain of pain during physical activity and tolerate it well;
- attacks often occur in the morning rather than during the day or at night;
- good effectiveness in treatment with drugs from the group of nitrates and calcium antagonists.
The prognosis of this form is unfavorable due to the high probability of transition to acute myocardial infarction.
Classification
The classification of unstable angina is associated with the determination of the likely development of an acute infarction, the dependence and frequency of painful attacks, and physical and emotional stress.
According to severity and duration, they are distinguished:
- first degree - the onset of the disease less than two months ago, develops at rest, the course is severe and progressive;
- second degree (subacute course) - the disease lasts more than two days, before this time no attacks were observed;
- the third (acute form) - developed only in the last two days.
The Braunwald classification of unstable angina suggests assessing the risk of myocardial infarction based on the clinical picture and causes of the pain attack. Three classes of disease and a division of the circumstances of the disease into groups A, B, C are proposed.
- The first class includes ordinary angina pectoris, the occurrence of pain against the background of a lower load than before, cases of increased frequency of attacks, cases registered for the first time in the last 2 months. At rest there are no attacks for 2 months.
- The second class is constant angina at rest or that occurs from two days to two months.
- The third class is acute angina at rest, occurring in the last 48 hours.
Groups by circumstances of manifestation:
- A (secondary) - attacks are provoked by non-cardiac diseases (anemia, thyrotoxicosis, acute infection, hypoxic conditions);
- B (primary) - associated with heart disease;
- C - occurs in the first two weeks after a heart attack.
The diagnosis of unstable angina according to Braunwald looks like “unstable angina, class 2 A.” This means that the attacks occur at rest, have been bothering them for about two months, and the patient has a concomitant pathology that causes spasm of the coronary arteries.
According to Rizik's classification, an anginal attack is associated with characteristic changes on the ECG:
- class 1a - increased attacks, but no signs on the ECG;
- class 1b - ECG symptoms appear in signs 1a;
- class 2 - exertional angina that occurs for the first time;
- class 3 - angina at rest, first appeared;
- class 4 - attacks at rest with ECG symptoms last a long time.
The conducted studies revealed that in patients classified as fourth class, acute infarction occurred in 42.8% of cases.
Diagnostics
Management of patients with coronary insufficiency (a particular type is unstable angina) is the task of a specialized doctor.
If there is suspicion, it makes sense to hospitalize the person for a short time; this is the most correct decision, because the patient’s life is at stake. The next episode could be the last.
Scheme of events:
- Oral interview with the patient. The complaints are typical, which allows us to draw conclusions almost immediately.
- Anamnesis collection. Data for organic pathologies is also on the surface. This is the path to identifying the origin of a process.
- Measurement of blood pressure, heart rate.
- Listening to heart sounds. The tones are dull and irregular. Violations worsen the prognosis.
- Daily monitoring using an automatic Holter device.
- Electrocardiography. Specific functional signs on the ECG include widening of the QRS complex, premature appearance of the P wave, doming of the ST segment, and many others. The interpretation is carried out by a cardiologist and diagnostic specialist. Errors may occur.
- Echocardiography. To determine organic changes and defects.
- MRI or CT.
- Angiography of the coronary arteries.
This is enough for the system. It is possible to involve third-party specialists as part of advanced diagnostics if there is no evidence of cardiac sources of the problem.
Diagnostic detection methods
The presented data convinces of the need for a detailed interview with the patient, clarifying the connection between a painful attack and other symptoms, time frames, and causes.
The main diagnostic method - ECG studies - is available in clinics and ambulances. Typical diagnostic manifestations are familiar to doctors of all specialties. It is necessary to take into account the course of the disease, symptoms and the possibility of delayed ECG manifestations or even their absence.
Holter monitoring during the day is especially indicated in stationary conditions.
ECG can be taken even at home
Laboratory methods reveal:
- leukocytosis in a general blood test;
- high levels of low-density lipoproteins, enzymes AST (aspartic aminotransferase) and LDH (lactate dehydrogenase), CPK (creatine phosphokinase) in biochemical analysis.
An ultrasound can show areas of decreased myocardial contractility and establish a decrease in cardiac output.
To check the patency of the coronary vessels, an angiogram is performed with the introduction of a contrast agent.
Treatment
Treatment of unstable angina is carried out in an inpatient setting in a therapeutic or cardiology department.
Treatment goals:
- restore the patency of the coronary vessels as early as possible;
- stabilize clinical manifestations, relieve pain;
- prevent acute heart attack and sudden death;
- provide the opportunity for rehabilitation and adaptation to living conditions.
As first aid, the patient can take up to two Nitrogrycerin tablets. Some people prefer a spray under the tongue. It is recommended to take two Aspirin tablets to prevent thrombosis.
"Old Man" Aspirin is still in demand
In the hospital, the patient is prescribed bed rest, gradually increasing as his condition improves.
The diet comes down to frequent meals in small portions, limiting spicy and fatty foods, foods that contribute to bloating and elevation of the diaphragm.
Recommended are porridge, stewed vegetables, kefir, cottage cheese, low-fat soups, beef meat dishes, boiled chicken, and unsalted fish.
Treatment with medications
We also recommend reading: Symptoms and first aid for angina pectoris
In an acute condition, nitro-containing drugs (isosorbide dinitrate, Nitroglycerin) are administered intravenously, then the dose for internal use is selected.
Anticoagulants (Heparin subcutaneously, Aspirin orally) to reduce coagulation and prevent the development of thrombosis. Modern aspirin-containing drugs can protect the stomach from harmful effects (Aspirin Cardio, Thrombo Ass, Cardiomagnyl).
A group of adrenergic blockers is prescribed in all cases except Prinzmetal's angina. These drugs are contraindicated for bronchial asthma, chronic bronchitis with respiratory failure.
Calcium channel antagonists are indicated in the absence of severe vascular damage (Cordafen, Nifidipine, Verapamil).
Symptomatic medications (painkillers, diuretics) are prescribed by the doctor on an inconsistent basis.
Possible complications
Untreated angina can cause:
- sudden ventricular fibrillation with fatal outcome;
- acute myocardial infarction;
- acute failure of the heart muscle with pulmonary edema;
- thromboembolism of the pulmonary arteries.
Therefore, an increase in attacks and the appearance of unusual symptoms are important reasons for urgent medical attention.
When referred for inpatient treatment, refusal is considered as the patient’s responsibility for his own life.
Prevention of angina
A healthy lifestyle is the most effective way to reduce the risk of angina.
If you have angina, maintaining a healthy lifestyle will also help prevent worsening symptoms and reduce your risk of heart attack or stroke.
This can most easily be achieved by eating a balanced, healthy diet, maintaining normal blood pressure levels and quitting smoking. This will lower your blood pressure, lower your cholesterol and strengthen your heart.
Apart from this, you also need to reduce your salt intake as it increases your blood pressure. You should consume less than 6 g of salt per day (about a teaspoon).
Let's work together to make the unique material even better, and after reading it, we ask you to repost it on a social network convenient for you. net.