Features of the pathology
Ectopia cordis is a developmental disorder of the fetus in which the normal position of the heart changes. Isolated ectopia is rare - in one baby per 100 thousand children. A combination of abnormal position of the organ and other disorders is 3-4 times more common, for example, irregular shape of the sternum or rib cage, congenital hernias.
Almost always, ectopia is combined with a violation of the anatomy and functions of the heart muscle itself, which can manifest itself:
- pathology of the valves - their incomplete closure or opening, which leads to improper blood flow,
- thickening of the walls of the heart or expansion of its cavities,
- development of arrhythmias,
- weakness of the heart muscle due to the replacement of muscle tissue with connective tissue fibers.
Abdominal ascites - treatment
Dropsy can accompany a number of diseases, but most often it affects patients with cirrhosis of the liver, oncology and heart failure.
Treatment of ascites in liver cirrhosis
Due to the fact that the affected liver loses its ability to “filter” the proper volume of blood, its liquid fraction is squeezed out through the walls of blood vessels, entering the abdominal cavity. The active release of fluid is facilitated, in particular, by the increased pressure in the portal vein, characteristic of cirrhosis.
According to the nature of fluid accumulation, dropsy is classified into:
- transient - disappears as cirrhosis is treated;
- stationary – despite treatment, fluid continues to accumulate;
- tense - treatment does not work, and the volume of fluid inevitably increases.
Based on the amount of liquid, dropsy is divided into small (up to 3 l), medium and large (20-30 l).
Abdominal ascites involves treatment with drugs aimed primarily at restoring liver function. For minor and moderate transient dropsy, the fluid is eliminated as liver function improves, and the patient is prescribed diuretics, as well as limited drinking and a salt-free diet.
If therapy for cirrhosis does not produce results, treatment of ascites consists of puncture: a puncture is made with a thick needle below the navel, due to which part of the fluid is removed, easing the patient’s condition.
In the most severe cases, only liver transplantation can relieve ascites caused by cirrhosis. In general, dropsy is an unfavorable sign and worsens the prognosis for cirrhosis.
Treatment of ascites in oncology
Dropsy, as a rule, makes itself felt in primary tumor foci formed in the stomach, mammary gland, pancreas, colon, ovaries or bronchi.
Practice shows that in 65% of patients, fluid is removed by taking diuretics. When treating ascites, abdominal paracentesis (puncture of the abdominal cavity) is often performed, which not only alleviates the patient’s condition, but also makes it possible to examine the fluid for total protein, leukocytes, and the presence of infection (Gram method, culture).
For cancer, treatment of abdominal ascites also involves chemotherapy. Thus, platinum drugs and paclitaxel are effective in testicular cancer, and 5-fluorouracil and leucovorin are used in colon cancer.
In some cases, intracavitary therapy is prescribed, which consists of removing fluid from the abdominal cavity and administering the drug bleomycin.
Treatment of ascites in heart failure
Dropsy is treated in combination with the underlying disease - heart failure, and the evacuation of accumulated fluid is carried out by two methods:
- Diuretics - the effect of taking them does not appear earlier than after a few weeks. The optimal diuresis is 3 liters, and it is impossible to force the process of fluid removal, because the body may interpret this as dehydration.
- Puncture - performed at the stage when taking diuretics does not produce results. After the puncture, the patient may be prescribed medications containing protein.
Treatment of ascites with folk remedies
Traditional medicine suggests fighting dropsy with the help of decoctions and infusions:
- Coltsfoot and sweet clover are taken equally; for 1 spoon of raw material you will need 500 ml of boiling water. The product is infused for half an hour, drinking 3 spoons 5 times a day.
- Dried angelica root (2 tablespoons), pour boiling water (1 cup), cook for 25 minutes. Drink 100 ml four times a day before meals, after cooling and straining the product.
If you have ascites, treatment with traditional methods should be agreed with your doctor and act as a complement to traditional methods of therapy.
Types of ectopia of the heart
The classification identifies the following variants of abnormal heart position:
- Abdominal (ectopia of the heart into the abdominal cavity) - the formation of the heart muscle below the normal level, in the area of the diaphragm or under it (in the abdominal cavity).
- Cervical ectopia of the heart - if the “migration” of the heart is disrupted during fetal development, it can remain at the level of 5-7 cervical vertebrae.
- Dextracardia - the organ is located in the chest cavity, at the level of 2-5 intercostal spaces, but not to the left of the midline, but to the right.
- Extrasternal - a violation of the relative position of the sternum and heart. Normally, the bone covers the organ, protecting it from external influences. With extrasternal ectopia, the heart lies on the surface of the sternum, directly under the skin (partial ectopia of the heart) or protrudes from the chest, uncovered by the integumentary tissues and serosa (complete ectopia of the heart). Which makes him vulnerable to any injury.
Gastric ectopia of the heart, at the moment, is not identified as a separate variant of the disease and is considered as one of the varieties of the abdominal form.
Diagnostics
Ascites can be diagnosed using physical, laboratory and instrumental studies. First of all, this is inspection, palpation and percussion.
Even at the examination stage, the doctor draws attention to an enlarged abdomen, dilation of the veins of the anterior abdominal wall, shiny skin of the abdomen, the presence of a flattened “frog” belly in the supine position, and protrusion of the navel.
When palpating the abdomen in a patient with ascites, a symptom of fluctuation is determined - fluctuations in intra-abdominal fluid when applying light jerking movements. This symptom can be determined if there is at least 1 liter of pathological fluid in the abdominal cavity, but it is impossible if there is excessive accumulation and tension in the abdominal wall.
This is interesting: Abdominal ascites: causes, types, symptoms and treatment
The percussion method reveals dullness of sound in the sloping parts of the abdomen. When the patient is positioned on his back, the dullness of the percussion sound is determined by the lateral surfaces where the liquid will flow; a tympanic sound will be heard above the remaining surfaces due to the airiness of the intestinal loops.
Laboratory tests include general clinical tests (general blood count, urine test) and biochemical studies (lipid profile, blood glucose and protein levels, blood bilirubin level, coagulogram). Research is aimed at detecting pathological changes that indicate an underlying disease, disturbances in the homeostasis system.
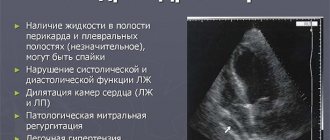
Instrumental research methods directly confirm the presence of ascites and help identify the causes of its occurrence. If ascites occurs in heart failure, electrocardiography, echocardiography, and, if necessary, myocardial scintigraphy are performed. These studies make it possible to establish the cause of heart pathology.
To confirm ascites, methods are used to detect pathological fluid in the abdominal cavity. These include:
- Ultrasound examination of the abdominal organs (ultrasound);
- Magnetic resonance imaging (MRI);
- Laparocentesis followed by analysis of ascitic fluid.
Ultrasound of the abdominal organs makes it possible to detect effusion of 100 ml, determine the condition of internal organs, and identify or exclude other possible pathologies.
In heart failure, dilatation of the inferior vena cava can be detected. This method is the simplest and most informative.
On ultrasound you can see ascites with a volume of 100 ml or more
Magnetic resonance imaging is the method with the best visualization of tissue. This method can detect small amounts of fluid in difficult to visualize areas. MRI is used for differential diagnosis of the causes of ascites.
This is interesting: How to treat dropsy of the abdominal cavity? Causes and symptoms of the disease in women and men
Laparocentesis is a study based on puncture of the anterior abdominal wall and aspiration of ascitic exudate. The method is both diagnostic and partially therapeutic. The resulting ascitic fluid is assessed by specific gravity, analyzed for protein content, leukocytes, erythrocytes, and the presence of atypical cells.
If the cause of ascites is heart failure, then the liquid will be transparent, have a specific gravity of 1.012-1.020, contain up to 2.5% protein, desquamated endothelial cells. During the first laparocentesis, leukocytes are not detected, but appear with subsequent punctures.
Causes
At the moment, there are 2 large groups of reasons that can lead to ectopia:
| Causes of the disease | Provoking factors |
| Damage to the genetic code of the fetus (chromosomal and gene mutations) | Damage to eggs due to toxic substances: alcohol, industrial hazards, tobacco, drugs. Even a single use of the above substances matters; the risk increases with the “experience” of using toxins |
| The child's father ingested toxins within 6 months before conception. | |
| Mother's age over 35 years/under 17 years | |
| Hereditary pathologies of the mother or father | |
| Use of a number of medications during pregnancy or immediately before it: chemotherapy with anthracyclines (“Doxorubicin”, “Bleomycin”), fluoroquinolones, cytostatic drugs | |
| Pathology of the placenta and metabolic disorders between mother and fetus | Increased risk of thrombosis in the mother: hereditary thrombophilias, previous pregnancy/abortion within 6 months before conception, antiphospholipid syndrome, improper use of diuretics, diabetes mellitus and obesity, etc. |
| Abnormal shape/position of the uterus | |
| Pregnancy with multiple fetuses (multiple) | |
| Chronic endometritis and fetal infections | |
| Diseases of the maternal cardiovascular system: high/low blood pressure, heart rhythm disturbances |
Important: Also, the etiology of ectopia may include any traumatic factors that were observed in the first trimester of pregnancy.
Features of the abdominal aorta and its diseases
First you need to understand what the abdominal aorta is and where it is located. This is a continuation of the thoracic aorta. Together they create the largest node in the large circle of the circulatory system. It serves to provide nutrients and the necessary amount of oxygen to all the organs of the abdominal cavity and the network of vessels that is connected to it.
Aortic diseases can be fatal.
Features and norms
Human anatomy is considered a complex but very interesting science. Knowing what each department and organ is responsible for, how our body works, it becomes easier to monitor our health and respond to any changes in a timely manner.
We can be affected by many diseases, which only qualified specialists can help us cope with. Often we are faced with diseases of organs and blood vessels directly related to them. One of them is the abdominal aorta (AA).
Normally, the cross-section of this artery is 2–3 centimeters in diameter. The length does not exceed 13 cm. The BA is located in the region of the 7th thoracic spine. From there it originates and nourishes the nearby abdominal organs.
It ends in the area of the 4th lumbar vertebra, after which it branches into 2 directions.
Each person may have their own characteristics and structure, which is why BA sometimes ends in the area of the 3rd or 5th lumbar vertebra.
The structure allows the aorta to be protected from all kinds of damage, since it is located on the inside of the human spine. You can find it a little to the left of the medial line.
The top is covered with fiber and lymphatic vessels, which guarantees protection from damage. The aorta, located in a straight line, gradually changes at an early age, acquiring a curved shape.
Next to BA, a person has:
- vein of the left kidney;
- inferior vena cava;
- pancreas;
- splenic vein;
- intermesenteric plexus;
- lumbar sections of the left sympathetic trunks;
- upper roots of the mesentery of the intestine (small).
This aorta is directly involved in the digestive process, since it provides nutrients to most of the organs that are responsible for digestion. In its normal state, it is characterized by a regular cylindrical shape, and when cut, the diameter is 2–3 centimeters.
Any expansion, change and deviation from the norm is an impetus for examination and comprehensive diagnosis. Violation of the correct form leads to the development of pathologies. The detection of an altered abdominal aorta indicates the development of potentially dangerous diseases of internal organs and systems.
It is necessary to consider the most common diseases caused by disturbances in the structure of the abdominal aorta.
Common diseases
An altered diameter of the abdominal aorta, increased or decreased its size can provoke the development of a number of pathological processes. Every nearby organ is under potential threat.
It is important to seek help in time for illness, undergo an ultrasound examination, that is, ultrasound of the abdominal cavity, and strictly follow the recommendations of the attending physician. Diseases are different, so each of them has its own symptoms.
It is important for people to monitor their health and promptly respond to uncharacteristic and unpleasant health conditions. An attack of abdominal pain (stomach ache) is not always a sign of banal indigestion or food poisoning.
The most common pathologies of the abdominal aorta include:
- aneurysms;
- atherosclerosis or thrombosis processes;
- nonspecific aortitis.
When performing an ultrasound of the abdominal aorta, you need to pay attention to its condition. Some atypical changes may be observed, indicating the development of potentially dangerous diseases.
- Bias. A displacement compared to the normal state of BA is possible with scoliosis, the formation of a retroperitoneal tumor, or with disease of the para-aortic lymph nodes. Sometimes this condition resembles the manifestation of an aneurysm, which misleads patients and treating doctors. A thorough scan will be required. To do this, the pulsation of the abdominal aorta is examined. Lymph nodes or other structures will be visually shown around or behind the BA. If an ultrasound of the abdominal aorta reveals that the cross-section has increased to 5 centimeters or more, urgent intervention will be required. There is a high probability of a rupture occurring.
- Narrowing. Any local narrowing requires increased attention. They need to be visualized using abdominal ultrasound in 2 different planes. This helps determine the level of prevalence of the pathological process. Narrowing can be observed along the entire length of the BA. This potentially leads to thrombosis.
Before making a final diagnosis to the patient, a comprehensive examination is carried out and the degree and nature of changes in the asthma along its entire length are identified. Only after this can treatment begin. Now let's go over the diseases characteristic of changes in the abdominal aorta.
Aneurysm
BA aneurysm is common in humans. This is an expansion of the aorta in the area that is located between the lower branches and the thoracic aorta.
The expanded area is characterized by thinner walls compared to other areas, and therefore becomes the most vulnerable spot. Initially, the aneurysm does not manifest itself in any way, which does not force people to seek help.
But if the situation is aggravated by external and internal factors, negative consequences begin to appear. They are expressed in the form of symptoms. With an aneurysm, a person faces:
- attacks of nausea without objective reasons;
- gagging:
- change in the usual color of urine;
- lack of blood supply to the arms and legs;
- manifestation of a neoplasm in the abdominal cavity, which pulsates intensely;
- pain in the lumbar area.
Each symptom manifests itself in varying degrees of intensity. This often indicates the development of a BA aneurysm. Therefore, it is necessary to promptly prepare for a visit to the clinic and an ultrasound scan of the abdominal aorta. Preparation and the ultrasound examination itself involve several nuances.
- You need to prepare for the study in advance. The procedure is done on an empty, empty stomach, so at least 6 to 7 hours should pass between the last meal and the ultrasound.
- A couple of days before the procedure, stop eating foods and drinks that can cause increased gas formation in the intestines. Also exclude everything that is fatty, harmful and takes a long time to digest.
- 24–48 hours before an ultrasound scan of the abdominal aorta, take medications as prescribed by your doctor that stimulate a reduction in the formation of gases. This is especially true for people who have flatulence.
- Pre-procedural preparation. Before the procedure, it is better not to drink or eat anything, chew gum or smoke. This will allow you to conduct the examination as efficiently as possible and make an accurate diagnosis.
The abdominal cavity must be properly prepared for examination procedures. If you do not follow the recommendations, then the doctor will not be able to get a clear picture. This will negatively affect the possible diagnosis and prescription of adequate treatment.
The enlarged area of BA may not withstand the excess blood pressure, losing its elasticity and bursting. The risk of rupture increases with physical, even minor, physical activity. When a rupture occurs, a large amount of blood enters the abdominal cavity.
It is not always possible to save a person even in the case of surgical intervention. Another potential complication of an aneurysm is the formation of blood clots in the area of swelling of the aorta.
If a blood clot breaks off and begins to move through the circulatory system, it can result in a heart attack and death for a person.
Not every person is predisposed to aneurysms. The risk group includes:
- those suffering from hypertension;
- people with connective tissue pathologies;
- alcoholics and smokers;
- suffered from infectious diseases that resulted in inflammation of the walls of the aorta.
Another risk factor for BA aneurysm is age. The older a person is, the higher the likelihood of such a pathology. But we can no longer do anything about this. You need to try to lead a healthy lifestyle, give up bad habits and engage in disease prevention.
Atherosclerosis
This is a process caused by the formation of lipid plaques on the surfaces of the internal walls of the asthma. An internal narrowing of the lumen occurs, and blood flow through this area is disrupted. Do not forget how important the role this aorta plays in providing blood:
- liver;
- gall;
- pancreas;
- stomach.
Developing thrombosis of the abdominal aorta, that is, its gradual clogging, manifests itself in the form of a disrupted digestion process. The main symptoms include:
- constipation (even with a proper and balanced diet it cannot be avoided);
- severe bloating followed by flatulence;
- paroxysmal pain in the abdominal area;
- diarrhea;
- regular burping;
- ingestion of incompletely digested food into the stool;
- attacks of abdominal pain.
If the disease has progressed to severe stages, then pain in the abdominal area will continue for several hours. This is a clear reason to immediately contact specialists.
By delaying the examination in the clinic, holding back the pain and trying to relieve it with painkillers, you can provoke the onset of irreversible processes.
Ignoring the symptoms of asthma atherosclerosis ends with chronic intestinal pathologies, from which there is almost no chance of getting rid of them. Atherosclerosis affecting the abdominal aorta can be effectively and successfully treated.
Much depends on how quickly you decide to go to the doctor, conduct an examination and begin comprehensive treatment of the problem. The longer you try to self-medicate or simply ignore obvious symptoms, the higher the likelihood of aggravating your condition and triggering fatal processes in the body.
Symptoms
Cervical ectopia is incompatible with life - in this position the heart cannot adequately perform its function and the child dies. Dextracardia often occurs without symptoms and is discovered accidentally during preventive examinations.
In other types of disorders, signs of cardiac dysfunction develop:
- moist “gurgling” rales, aggravated by frequent breathing and movements,
- bluish discoloration of the skin, most clearly visible on the arms and legs,
- swelling, dense to the touch, is often located on the extremities and in the abdominal cavity.
Pain may occur due to compression of surrounding organs by the heart.
Detection of the disease when the organ is located extrasternally is not difficult - heartbeats are visually detected directly under the skin and subcutaneous tissue of the chest, and the organ is palpated. If there is a blow to this area, compression or other trauma, not only tissue damage can occur, but also severe arrhythmias can rapidly develop, including cardiac arrest (asystole).
Ascites. Causes, treatment
Ascites is an accumulation of fluid in the abdominal cavity.
Pathogenesis
:
1. High portal pressure and liver congestion.
2. Hypoproteinemia due to impaired protein synthesis in the liver, resulting in a decrease in oncotic pressure of the blood and effusion of fluid into the abdominal cavity.
3. Violation of water-electrolyte metabolism. Na retention due to irritation of osmoreceptors by low oncotic pressure of the blood, resulting in the release of aldosterone, and even greater Na retention, which draws water with it and further increases effusion.
4. Impaired activation of renin, aldosterone, AT, resulting in vasospasm, Na retention and even greater accumulation of water in the bcc, and an increase in effusion.
5. Increased permeability of the vascular wall due to hypoxia and intoxication.
In newborns, ascites may be a manifestation of hemolytic disease of the fetus and newborn or occult fetal blood loss. In children of the first 3 years of life, ascites is most often associated with liver disease, but it can also be a consequence of chronic nutritional disorders, exudative enteropathy, and a manifestation of congenital nephrotic syndrome. The occurrence and growth of ascites is facilitated by disturbances in the regulation of water-salt metabolism.
The accumulation of fluid in the abdominal cavity (sometimes more than 20 liters) leads to increased intra-abdominal pressure and pushing of the diaphragm into the chest cavity. As a result, the respiratory movements of the lungs are significantly limited (up to the development of respiratory failure), the activity of the heart is disrupted, and the resistance to blood flow in the abdominal organs increases, the functions of which are also impaired. The concentration of protein in serous ascitic fluid is relatively small, but its overall loss in massive ascites can be significant, especially with frequent repeated removal of fluid by puncture of the abdominal cavity (the loss of protein is combined with the loss of salts), which leads to the development of protein deficiency.
Clinically, ascites can be detected when there is at least 1 liter of fluid in the abdominal cavity. During the examination, an enlarged abdomen is detected, which, when the patient is in an upright position, looks saggy; protrusion of the navel is often noted; in a patient who is in a horizontal position, the abdomen is flattened, its lateral sections bulge (the so-called frog belly). With severe portal hypertension, an expanded venous network is visible on the skin of the abdomen due to the development of anastomoses between the portal and vena cava systems. Dilated, swollen and tortuous venous collaterals are located around the navel and extend from it in the form of rays, forming a characteristic figure (“Medusa’s head”). When percussing the abdomen, a dull sound is detected over the sloping or lateral part of it; the border of dullness moves when the position of the body changes. With your palm placed on the side wall of the abdomen on one side, you can feel the tremors caused by tapping the fingers of the other hand on the wall of the opposite side of the abdomen (fluctuation symptom). Percussion and x-ray examination reveal the high position of the diaphragm and the limitation of its respiratory mobility. With ascites in patients with congestive heart failure, fluid in the pleural cavity is often detected - hydrothorax.
In the presence of ascites, an important diagnostic task is to determine the underlying disease (if it has not been recognized previously), which is helped by the analysis of signs accompanying ascites. With severe portal hypertension in patients with liver cirrhosis, ascites is often combined with bleeding from varicose veins of the esophagus and is usually accompanied by the development of collaterals under the skin of the abdomen. In case of heart failure, in addition to ascites, swelling of the legs and feet, acrocyanosis is observed, and in case of renal failure - widespread swelling of the skin and subcutaneous tissue. Diagnostic puncture of the abdominal cavity with laboratory examination of ascitic fluid is of great importance. In patients with liver cirrhosis and congestive heart failure, ascitic fluid is usually transparent, its specific gravity is not more than 1.015, and the protein concentration is not higher than 2.5%; the fluid contains mainly endothelial cells, but irritation of the peritoneum as a result of repeated punctures promotes the appearance of leukocytes. With cancer of the peritoneum, tumor cells can be found in the ascitic fluid. With tuberculous lesions of the peritoneum, the so-called ascites-peritonitis develops, in which the ascitic fluid can be hemorrhagic in nature, usually contains lymphocytes, and Mycobacterium tuberculosis can be found in it. In children of the first three years of life, ascites often has to be differentiated from pseudoascites (intestinal atony with bloating), observed in celiac disease and cystic fibrosis.
Treatment of ascites
Treatment is aimed at the underlying disease. To reduce ascites, diuretics and aldosterone antagonists are used, measures are taken to correct disorders of water-salt metabolism and reduce portal hypertension. If drug therapy is ineffective, the fluid can be removed by puncture of the abdominal cavity - laparocentesis (abdominal paracentesis), which is carried out after preliminary emptying of the bladder with the patient in a sitting position (seriously ill patients are placed on their side) in compliance with the rules of asepsis and antisepsis, which is best achieved when laparocentesis in the hospital. A puncture with a trocar after local anesthesia is carried out along the midline of the abdomen between the pubis and the navel or along the line connecting the navel to the iliac crest. The fluid must be released slowly (due to the risk of collapse) and usually no more than 5-6 liters per puncture. Repeated punctures can lead to inflammation of the peritoneum and fusion of the intestines or omentum with the anterior wall of the abdomen, which creates the threat of severe complications during subsequent punctures.
Surgical treatment of ascites is used mainly in cases of significant portal hypertension in order to reduce it (the application of various portocaval organ anastomoses) and create conditions for the absorption of ascitic fluid by adjacent tissues. One of the effective surgical operations, omentohepatophrenopexy, involves suturing the omentum to previously scarified areas of the surface of the liver and diaphragm.
The prognosis of the underlying disease with ascites worsens. It is especially unfavorable with a rapid increase in ascites after repeated punctures.
Popular answers
Similar answers
All information is provided for informational purposes only. Only a doctor can make the correct diagnosis and prescribe appropriate treatment!
Ascites
- accumulation of fluid in the abdominal cavity. Occurs most often as a result of portal hypertension with cirrhosis of the liver, congestive heart failure, thrombosis of the branches of the portal vein or compression of its trunk; less often due to damage to the peritoneum (cancer, tuberculosis, etc.), the thoracic lymphatic duct, and also as a manifestation of the general edematous syndrome in kidney diseases, nutritional dystrophy.
In newborns, ascites may be a manifestation of hemolytic disease of the fetus and newborn or occult fetal blood loss. In children of the first 3 years of life, ascites is most often associated with liver disease, but it can also be a consequence of chronic nutritional disorders, exudative enteropathy, and a manifestation of congenital nephrotic syndrome.
The occurrence and growth of ascites is facilitated by disturbances in the regulation of water-salt metabolism. The accumulation of fluid in the abdominal cavity (sometimes more than 20 liters) leads to increased intra-abdominal pressure and pushing of the diaphragm into the chest cavity. As a result, the respiratory movements of the lungs are significantly limited (up to the development of respiratory failure), the activity of the heart is disrupted, and the resistance to blood flow in the abdominal organs increases, the functions of which are also impaired.
The concentration of protein in serous ascitic fluid is relatively small, but its overall loss in massive ascites can be significant, especially with frequent repeated removal of fluid by puncture of the abdominal cavity (the loss of protein is combined with the loss of salts), which leads to the development of protein deficiency.
Clinically, ascites can be detected when there is at least 1 liter of fluid in the abdominal cavity. During the examination, an enlarged abdomen is detected, which, when the patient is in an upright position, looks saggy; protrusion of the navel is often noted; in a patient who is in a horizontal position, the abdomen is flattened, its lateral sections bulge (the so-called frog belly).
With severe portal hypertension, an expanded venous network is visible on the skin of the abdomen due to the development of anastomoses between the portal and vena cava systems. Dilated, swollen and tortuous venous collaterals are located around the navel and extend from it in the form of rays, forming a characteristic figure (“Medusa’s head”).
When percussing the abdomen, a dull sound is detected over the sloping or lateral part of it; the border of dullness moves when the position of the body changes. With your palm placed on the side wall of the abdomen on one side, you can feel the tremors caused by tapping the fingers of the other hand on the wall of the opposite side of the abdomen (fluctuation symptom).
Percussion and x-ray examination reveal the high position of the diaphragm and the limitation of its respiratory mobility. With ascites in patients with congestive heart failure, fluid in the pleural cavity is often detected - hydrothorax.
In the presence of ascites, an important diagnostic task is to determine the underlying disease (if it has not been recognized previously), which is helped by the analysis of signs accompanying ascites. With severe portal hypertension in patients with liver cirrhosis, ascites is often combined with bleeding from varicose veins of the esophagus and is usually accompanied by the development of collaterals under the skin of the abdomen.
In case of heart failure, in addition to ascites, swelling of the legs and feet, acrocyanosis is observed, and in case of renal failure - widespread swelling of the skin and subcutaneous tissue. Diagnostic puncture of the abdominal cavity with laboratory examination of ascitic fluid is of great importance.
In patients with liver cirrhosis and congestive heart failure, ascitic fluid is usually transparent, its specific gravity is not more than 1.015, and the protein concentration is not higher than 2.5%; the fluid contains mainly endothelial cells, but irritation of the peritoneum as a result of repeated punctures promotes the appearance of leukocytes. With cancer of the peritoneum, tumor cells can be found in the ascitic fluid.
With tuberculous lesions of the peritoneum, the so-called ascites-peritonitis develops, in which the ascitic fluid can be hemorrhagic in nature, usually contains lymphocytes, and Mycobacterium tuberculosis can be found in it.
In children of the first three years of life, ascites often has to be differentiated from pseudoascites (intestinal atony with bloating), observed in celiac disease and cystic fibrosis.
Diseases leading to ascites:
Peritoneal diseases
- tuberculosis of the peritoneum.
- mesothelioma (a malignant tumor originating from the peritoneum).
Damage to the peritoneum in other diseases
- metastatic lesion. Most common in stomach cancer, colon cancer, cancer. ovarian, breast cancer.
- pseudomyxoma.
Portal hypertension (increased pressure in the portal vein - the vein that collects blood from the abdominal organs)
- hepatic vein thrombosis. Occurs in liver cancer, hypernephroma, blood diseases, widespread thrombophlebitis and estrogen use.
- thrombosis (blockage by a blood clot) or stenosis (narrowing) of the inferior vena cava.
- obstruction or stenosis of the portal vein and its branches.
- cirrhosis of the liver.
- liver tumors.
Kidney diseases
- nephrotic syndrome (accompanied by loss of protein in the urine).
- chronic nephritis in the terminal stage.
Diseases of the heart and pericardium
- pericarditis.
- heart failure.
Diseases of the gastrointestinal tract
- Whipple's disease, Crohn's disease, etc. accompanied by diarrhea and protein loss.
- intestinal lymphangiectasia (dilation of the lymphatic vessels of the abdominal cavity).
Other diseases
- myxedema (swelling due to decreased thyroid function).
- Meigs syndrome (with ovarian tumors).
- pancreatitis.
Treatment of ascites
Treatment is aimed at the underlying disease. To reduce ascites, diuretics and aldosterone antagonists are used, measures are taken to correct disorders of water-salt metabolism and reduce portal hypertension.
If drug therapy is ineffective, the fluid can be removed by puncture of the abdominal cavity - laparocentesis (abdominal paracentesis), which is carried out after preliminary emptying of the bladder with the patient in a sitting position (seriously ill patients are placed on their side) in compliance with the rules of asepsis and antisepsis, which is best achieved when laparocentesis in the hospital.
A puncture with a trocar after local anesthesia is carried out along the midline of the abdomen between the pubis and the navel or along the line connecting the navel to the iliac crest. The fluid must be released slowly (due to the risk of collapse) and usually no more than 5-6 liters per puncture.
Repeated punctures can lead to inflammation of the peritoneum and fusion of the intestines or omentum with the anterior wall of the abdomen, which creates the threat of severe complications during subsequent punctures.
Surgical treatment of ascites is used mainly in cases of significant portal hypertension in order to reduce it (the application of various portocaval organ anastomoses) and create conditions for the absorption of ascitic fluid by adjacent tissues.
One of the effective surgical operations, omentohepatophrenopexy, involves suturing the omentum to previously scarified areas of the surface of the liver and diaphragm. The prognosis of the underlying disease with ascites worsens. It is especially unfavorable with a rapid increase in ascites after repeated punctures.
Internet resources:
- trimm.ru - Ascites: modern approaches to classification and treatment.
- volgograd.ru - Conservative treatment of ascites.
- medinfa.ru - Ascites, symptoms and treatment of ascites.
- humbio.ru - Liver cirrhosis and ascites, treatment.
- diagnos.ru - Ascites, causes, manifestations, diagnosis.
Treatment
If dextracardia is detected, there are no clinical symptoms, or disturbances in the functioning of the heart and surrounding organs, no treatment is required. In this case, observation at the place of residence by a local therapist and cardiologist is indicated with an examination frequency of once a year.
Other types of organ ectopia most often require surgical intervention. It is carried out only in large multidisciplinary children's hospitals, which should have a pediatric cardiac surgery department. In Russia, the number of such centers is small - 1-2 centers per region. It should be noted that all medical care, including surgery, is provided free of charge for all people with a compulsory medical insurance policy.
The extent of surgical intervention and the method of its implementation are determined individually by the treating cardiac surgeon. After the operation, a long period of rehabilitation and constant monitoring of the child by a pediatrician or cardiologist are required.
General principles of nutrition for ascites
It is vital for a patient with ascites to strictly follow a diet. There are general rules for fluid accumulation in the abdomen:
- Salt is completely prohibited;
- Eliminate fresh white bread and baked goods from your diet;
- You can't eat fried food;
- Fatty meats and fish, lard, and smoked products are prohibited;
- You will have to give up fatty sour cream (more than 10% fat content), cottage cheese (more than 3% fat content), kefir (more than 0% fat content), milk (more than 1.5% fat content);
- The following are strictly prohibited: cabbage, radishes, radishes, onions, garlic;
- Sweets: cakes, pastries, chocolate are not recommended for consumption;
- Also, coffee, cola, and other soda are not allowed.
Nutrition for ascites is controlled by the attending physician. If the patient follows the prescribed diet, the general condition will improve.
It is worth excluding everything spicy and those foods that make you thirsty from your diet. Liquids should be consumed in moderation to reduce the amount of fluid in the stomach.
A therapeutic diet for ascites can affect the development of complications. She may not allow them to develop. Peritonitis, bleeding and hernia will not be scary.
There is no point in developing a proper nutrition system on your own. It is advisable to listen to dietary recommendations and advice from a specialist, because he has a complete picture of the development of the disease and, if necessary, will refer you for additional examinations.
This is interesting: Prognosis and treatment of ascites in oncology. What are the chances of success?
Description of the disease
Contents
It is not very easy to determine atherosclerosis of the abdominal aorta, since this disease can hide under the guise of other ailments. However, it is very important to do this in view of all the consequences and complications. First, let's look at how this disease develops.
What's happening and why
Computed tomography of the aorta
Abdominal aortic aneurysm is a disease that affects the largest blood vessel in the human body. The aorta is directly connected to the heart, since a large amount of blood enters its cavity from it, which is subsequently transported through small vessels to individual organs.
An aneurysm is a pathological expansion of a certain section of the aorta in the abdominal region, which is accompanied by protrusion of the walls of the vessel or their thinning. In the chest cavity, such a violation occurs extremely rarely.
When damaged, the aortic wall becomes much thinner, leading to its rupture. Violation of the integrity of the vessel occurs due to the inability to withstand high blood pressure.
There are several types of pathology. The most common is the saccular form, in which the aneurysm is a formation that looks like a cavity.
In addition, there is a spindle-shaped variety, which is characterized by large sizes. The third form of the disease is dissecting aneurysm, in which dissection of the aortic wall occurs.
The likelihood of an aneurysm rupturing directly depends on its size and many other factors. If its diameter is more than 5 cm, the risk of complications is about 25%. Wall rupture usually occurs within several years (maximum 8-9) after the formation of the aneurysm.
With the disease, there is often a significant increase in the size of the aorta. As a rule, it increases by at least 50%. Because of this, the disease is often accompanied by cardiac arrhythmias and sudden surges in blood pressure. As a result of such disturbances, the aneurysm may become larger, increasing the likelihood of rupture.
A serious complication of an abdominal aneurysm is the active formation of blood clots that occurs within the affected area of the vessel. Blood clots are able to move along with normal blood into small arteries, disrupting their patency.
As a result, there is a negative effect on the body associated with oxygen starvation of tissues and nutrient deficiency. In severe cases, disruption of the patency of the blood vessel leads to the development of a necrotic process, which leads to complete dysfunction of the organ.
Also, the disease can lead to the formation of aortic valve defects. As a result, patients experience decompensation of cardiac activity.
Such a violation can lead to a significant deterioration in blood circulation and the development of coronary heart disease.
Abdominal aortic aneurysm is one of the most common cardiovascular disorders, which in most cases leads to the development of serious complications.
An abdominal aortic aneurysm is a diffuse dilation of the walls of the aorta in its abdominal cavity. Protrusion of the vessel wall occurs at the height of the 8-6th lumbar vertebra. In cardiological practice, abdominal aortic aneurysm occurs in 95% of all cases of aneurysmal diseases.
The disease occurs more frequently in older people, especially men over 60 years of age. The disease is diagnosed in 2.5% of elderly patients who seek medical help. Pathology tends to develop over a long period of time. The aneurysm increases in size by 10% per year. After 8 years of the disease, a rupture occurs.
| Localization | Protrusion form | Etiological factor | Clinical course variant |
|
|
|
The pathology is considered small if its size does not exceed 3-5 cm. The average is 5-7 cm, and the large one is over 7. A person is registered when a small aneurysm is detected. You should be examined every 6 months.