Causes of angina
All the causes that cause heart pain can be divided into several groups:
- Cardiovascular diseases.
- Connective tissue damage.
- Diseases of the lungs and bronchi.
- Diseases of the abdominal region or diaphragm.
- Climatic cardiomyopathy.
- Spinal column problems.
As you can see, there are quite a few reasons that cause pain in the heart and chest. Although such sensations have a similar picture, there are some differences between them at the clinical and diagnostic levels. Therefore, we need to understand each of them in more detail.
What is angina
Angina pectoris is a specific pain syndrome characteristic of myocardial ischemia. There are stable and unstable angina, as well as exertional and resting angina.
Stable angina is one that occurs in an unchanged form. We can say that this is a “habitual” symptomatology for a person. However, this situation cannot be considered the norm: serious treatment is required, often surgical.
Unstable angina is either angina that has arisen for the first time, or one where the nature of the pain syndrome and sensations differs significantly from the usual state. This is an extremely dangerous condition, fraught with a high risk of developing a heart attack, and requiring an immediate call to the ambulance.
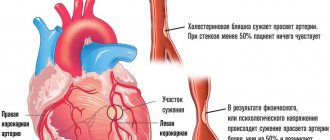
Angina pectoris is one of the manifestations of atherosclerosis and coronary heart disease, which is manifested by severe chest pain during physical activity and stress. However, chest pain is not always a manifestation of angina.
It is important to note symptoms such as:
- squeezing, pressing or burning nature of the attack;
- impact under the left shoulder blade or in the arm, neck, lower jaw;
- lack of oxygen and dizziness;
- obvious interruptions in the functioning of the heart: fluctuations in heart rate and blood pressure.
Most often, pain with angina pectoris manifests itself during walking, climbing stairs, physical effort, and stress. The attack lasts from 1 to 15-20 minutes and is facilitated by taking nitroglycerin. Symptoms may appear all at once or separately.
Angina at rest, unlike the previous type, is characterized by a sudden and prolonged attack, which is activated without external provoking factors, sometimes during sleep. In this case, we can add to the main symptoms: an uncontrollable panic attack, a pronounced feeling of suffocation, a violation of the autonomic functions of the body. We will write more about this type of angina in the following articles.
In addition to extremely unpleasant symptoms, such manifestations indicate a high risk of myocardial infarction, as well as the development of heart failure.
Cardiovascular diseases claim half of human lives - exactly the same as all other causes combined.
Forms of unstable angina
Unstable angina has several forms of development:
- Angina pectoris, which appeared for the first time. The disease manifests itself in the form of discomfort, as well as chest pain of a compressive nature. The pain can radiate not only to the chest, but also to the shoulder blade or arm. The time of appearance is approximately 1 month from the onset of the first syndrome.
- Progressive angina lasts approximately 4 weeks. The pain appears more often, it becomes much stronger, work efficiency decreases and the antihistamines used do not help. A person's need for a dosage of nitroglycerin increases.
- Post-infarction angina. Appears between 24 hours and 8 weeks after a heart attack. In other words, particles of the heart muscle begin to die, as a result of which blood flow in that area stops.
- Spontaneous angina. Manifests itself in the form of severe pain in a calm state. Such manifestations last no longer than 15-20 minutes, the patient sweats heavily, may lack air, and the rhythm of the heartbeat and breathing is disturbed.
If angina pectoris appears for the first time, then additional diagnostic measures will not be required to determine it. With progressive angina, the patient's condition sharply deteriorates, and pain appears with light exertion. To accurately determine the disease, a differential diagnosis must be made.
Unstable angina: Unstable angina
The diagnosed pathology requires prompt hospitalization for observation and treatment. Strict bed rest, a salt-free diet are prescribed, and the full range of necessary clinical studies is carried out. Dynamic ECG recording is mandatory. Primary goals include preventing the development of infarction, reducing symptoms, and improving the patient's quality of life and prognosis. With adequate therapy and a favorable course of the disease, stabilization occurs in one to two weeks. The main method remains medication, which involves the use of drugs from several main pharmacological groups:
- Antianginal drugs
. Necessary for immediate relief of angina pectoris. Nitrates are prescribed to help expand the lumen of blood vessels and improve blood supply to the heart muscle, reducing preload. Cardioselective beta blockers and calcium channel antagonists, which reduce heart rate and myocardial oxygen demand, are also used. In emergency cases, neuroleptanalgesia can be used by intravenous administration of strong painkillers. - Thrombolytic drugs
. Mandatory components of the treatment program are antiplatelet agents (aspirin, clopidogrel, ticlopidine) and direct anticoagulants (heparin), which prevent thrombus formation. In the absence of obvious contraindications, long-term use of drugs from these groups is required. - Lipid-lowering drugs.
In the long term, statins are used to help normalize cholesterol levels and are prescribed regardless of its initial level. Regular use significantly reduces overall mortality, the likelihood of recurrent attacks and complications. Atorvastatin or simvastatin is commonly used. A combination with nicotinic acid is possible.
The persistence of cardialgia, despite the therapy, the presence of a large area of ischemia with a progressive nature of the process and damage to the large coronary arteries are indications for prescribing invasive methods. The choice of revascularization method depends on coronary angiography data. Transluminar coronary angioplasty and coronary bypass surgery are performed. These surgical interventions only slightly improve the patient's long-term prognosis, but significantly increase his quality of life and almost completely eliminate symptoms.
Main characteristics of differential. diagnostics
Differential diagnosis is very important to distinguish between two diseases: heart attack and angina. The importance lies in the fact that all angina syndromes often serve as the initial stages of a heart attack. Therefore, if pain persists for 20 minutes and nitroglycerin is ineffective to relieve it, doctors should think about the likelihood of a heart attack. The main differences of this syndrome:
- Pain accompanies the patient for several hours and even days.
- Pain appears over a large area of the chest and heart.
- The sensations can be so unbearable that there is no strength to endure, the nature of the manifestations is compressive and oppressive.
- During an attack of angina, a person freezes and does not move, and during a heart attack, he moves restlessly. Often, with such sensations, people try to find a comfortable position so that the syndrome becomes weaker.
- Narcotic analgesics are used for relief.
Important! Pressing and tingling pain near the heart and in its area can appear in athletes under heavy loads. It is possible to develop coronary heart disease as a result of coronary atherosclerosis.
Angina pectoris
Angina pectoris (myocardial ischemia, “angina pectoris”) is a chronic disease of the cardiovascular system, characterized by attacks of chest pain, usually of a squeezing, pressing nature, lasting up to 15 minutes.
The pain often radiates to the left arm, to the interscapular region, and neck.
If the pain lasts more than 15 minutes, myocardial infarction must be excluded.
How does angina pectoris manifest? Complaints with angina pectoris:
- the first symptom, often the only one, is pressing pain behind the sternum, radiating to the arm, neck, lower jaw, back, often accompanied by shortness of breath;
- pain occurs during physical or emotional stress, in the cold or after eating and disappears with rest (within a few minutes) or after taking nitroglycerin;
— there are no complaints between attacks (but the disease persists!);
— chest pain can be caused by other diseases and conditions (esophagospasm, mitral valve prolapse, trauma, thyroid disease, heart rhythm disturbances).
Types of angina.
1. Angina pectoris.
Attacks of angina pain occur during physical activity of the same intensity.
The ECG shows changes during an attack (the ST segment drops), while in the interictal period the electrocardiogram remains unchanged.
2. Unstable angina.
If attacks of angina pectoris lengthen, become more severe, exercise tolerance sharply decreases, chest pain appears at rest, they speak of unstable angina. In this condition, the risk of myocardial infarction is high.
3. Angina at rest.
This is a type of unstable angina. Attacks occur at rest and at night. They interfere with sleep.
4. Angina pectoris in heart failure (“angina pectoris”).
The attacks appear in the supine position and disappear when the patient sits up.
5. Vasospastic angina.
The pain occurs at rest, for no apparent reason, and is caused by spasm of the coronary arteries (the arteries that supply the heart).
The ECG during an attack is characterized by ST segment elevation.
During an attack, ventricular arrhythmias are common, which can cause myocardial infarction.
Examination for angina pectoris.
Instrumental examination methods include ECG. This method is more informative during an attack, during interictal periods - changes may be minimal, not always characteristic of angina.
Stress ECG tests can detect angina in 75% of patients. However, a negative test cannot be regarded as absolutely reliable evidence that there is no coronary atherosclerosis.
The most reliable way to judge the presence of coronary atherosclerosis, the severity and stenosis of the coronary arteries is coronary angiography. The severity of angina does not always correspond to the degree of damage to the coronary arteries.
Laboratory diagnosis of angina pectoris.
Blood parameters in diagnosing angina pectoris are of no small importance:
- first of all, this is a clinical blood test with a leukocyte formula, with the determination of ESR.
— coagulogram (to exclude the risk of thrombosis);
— indicators of cholesterol metabolism (total cholesterol, HDL, LDL, triglycerides, atherogenicity index), markers of vascular atherosclerosis;
- biochemical blood test, study of enzyme activity (CPK, in particular its MB fraction; AST; LDH).
Treatment of angina pectoris.
To date, effective treatment for coronary heart disease has been developed.
Several groups of drugs are used to treat angina, depending on the severity of the disease, concomitant diagnoses, and tolerability of certain medications:
- nitrates;
- calcium antagonists;
- beta blockers;
- antiarrhythmic drugs;
- aspirin.
The selection of drugs and their dosage is strictly individual. In many ways, the prescription of a particular drug depends on the factors that provoke an attack of angina.
Only a doctor prescribes medication!
The medical appointment is conducted by an experienced cardiologist with more than 20 years of experience.
At the appointment, the doctor will review the complaints, collect an anamnesis of the disease, and make a diagnosis.
He will tell you how to avoid angina attacks in everyday life. He will select the necessary medication treatment, give recommendations on nutrition, physical activity, and teach you how to use medications during an attack. Prescribe an examination to identify risk factors for the disease. If necessary, he will recommend additional examination.
Make an appointment at a time convenient for you by phone:
+7(499)612-77-07
Prevention of angina pectoris.
All heart diseases have a hereditary predisposition; prevention is especially important in this case.
The goal of preventive measures is to eliminate risk factors for coronary artery disease:
- to give up smoking,
- loss of body weight,
- a diet low in animal fats,
- treatment of arterial hypertension and diabetes mellitus.
Attention! Pain in the heart area is a serious reason to consult a doctor, especially if there is a hereditary predisposition to coronary heart disease.
Regularly (at least once every 6 months) monitor the level of cholesterol in the blood (it is a marker of the development of atherosclerosis).
Angina pectoris affects 2-3% of people aged 25-64 years.
At a young age, the disease is more common in men; after 45 years, it rapidly progresses in women.
Make an appointment at a time convenient for you by phone:
+7(499) 612-77-07
Correct diagnosis
In case of angina pectoris, differential diagnosis consists of eliminating problems with the lungs. To check the pathology, an anamnesis should be analyzed so that there is a detailed description of pain dysphoria. Next, drug tests and electrocardiography are performed.
Pain in the thoracic region can occur due to diseases of the abdominal cavity and for other reasons. Electrocardiography is necessary but is often normal. Cardiography is used during an attack of angina with little physical exertion.
A well-conducted diagnosis will not only allow you to identify the correct diagnosis, but also find out the level of coronary insufficiency. During differential diagnosis, the symptoms of a previous heart attack, identified using an ECG, are used.
Diagnosis of IHD
Diagnosis of coronary heart disease (CHD) is a set of measures that consist of examining the patient and a number of studies. The examination plan includes the following steps:
- Collection of complaints and medical history. At this stage, the doctor must carefully determine all the patient’s symptoms, determine the expected duration of the disease, and also find out the presence of other pathologies.
- Examination of the patient. During the examination, the doctor assesses the person’s condition (the presence or absence of heart failure, edema, examines the pulse and listens to heart sounds). In addition, during the examination, the doctor can understand whether the patient has other somatic diseases in order to further conduct laboratory and instrumental diagnostics of these diseases.
- ECG. One of the oldest instrumental research methods. In many situations, after the study, an accurate diagnosis can already be made.
- Holter monitoring ECG. This method of studying coronary heart disease allows you to accurately determine the nature and magnitude of physical activity that provokes an attack of angina pectoris. In addition, this method is used to evaluate the treatment of coronary artery disease.
- Functional load tests. They represent a large group of tests that are based on recording and recording a cardiogram during dosed physical activity. This diagnostic method allows you to identify hidden coronary heart disease when there are no obvious signs of the disease.
- Echocardiography. It is an everyday method that allows you to obtain important data on the morphological and functional state of the heart muscle. Echocardiography can also be performed during exercise, which allows one to assess the degree of ischemia of the muscular wall of the heart. This type of study is called stress echocardiography (stress test).
- Functional tests in the diagnosis of ischemic heart disease. This type of study involves simulating coronary artery spasm in a patient. Daily blood pressure monitoring is carried out according to indications, especially in cases where there is a combination of coronary artery disease with hypertension or other causes of increased blood pressure.
- Laboratory blood tests. By studying the composition of certain indicators of fat metabolism, one can judge the risk of developing atherosclerosis; by the level of markers of myocardial infarction, one can talk about its presence and characteristics. In addition, general clinical examinations of urine and blood, as well as basic biochemical blood parameters, are mandatory.
- Angiography of the coronary arteries. Indicated for patients planning surgical treatment of coronary artery disease. In this case, a radiopaque substance is injected into the arterial bloodstream, which fills the vessels, and then a series of images is taken, on the basis of which the nature and location of lesions in the vascular bed of the heart is determined.
Thus, methods for diagnosing IHD are complex. Most of them are performed on an outpatient basis and do not require significant investment of time or money. Accurate diagnosis of coronary artery disease allows the cardiologist to select adequate treatment and, if necessary, refer the patient for surgical treatment. Also, studies conducted over time make it possible to evaluate the effectiveness of treatment of coronary heart disease.
Read more:
- sudden death due to ischemic heart disease.
Differential diagnosis of cardiovascular diseases
Pain during myocardial infarction differs from angina pectoris in greater intensity and duration. The sensations do not become weaker after using nitroglycerin, and standard analgesics do not help either. Pain can only be reduced by taking narcotic analgesics, namely morphine administered intravenously. The patient experiences severe agitation and fear of death.
Sometimes the pain is so severe that people can rush around, scream, and if a phase of excitement sets in, they can begin physical activity without realizing the severity of their condition. It must be remembered that there is an atypical form of heart attack in which the patient does not feel pain. If the pain is mild or completely absent, a heart attack is diagnosed after the fact using an ECG.
The patient may have inflammatory heart disease. Myocarditis is characterized by a connection with a recent infection. The pain syndrome is constant, and the use of anti-inflammatory drugs can reduce it. With pericarditis, there may be stabbing, squeezing pain with an increasing effect when inhaling, and shortness of breath appears. During auscultation, the doctor listens to the friction of the pericardium. If a patient has endocarditis, a heart murmur appears. Through echocardiography, the affected valves will be visible, and the patient's condition is usually accompanied by fever.
In the case of heart disease, the patient may have different pain syndromes - from aching and temporary to stabbing, permanent. In this case, there is no connection with the load. You can find out about heart defects only by using auscultation and echocardiography.
Diff. diagnosis of other cardiovascular diseases
Heart pain syndromes with hypertension are not uncommon. As a rule, they manifest themselves in the form of aching pain, which is accompanied by an increase in pressure. Often the diagnosis of “angina pectoris” can be accompanied by hypertension, because hypertension causes “angina pectoris.”
When pulmonary embolism appears, the patient begins to experience intense pain, which is combined with shortness of breath, hemorrhage appears, and body temperature rises sharply.
Heart tumors can be benign or malignant. In this case, the patient begins to experience heart pain, which often appears when the tumor grows into the pericardium. The sensation becomes stronger if the patient begins to inhale, and a pericardial friction rub may even be heard.
A disease called VSD usually appears in young people. A stabbing sensation appears in the upper part of the heart. If you ask a patient where it hurts, he will point with only one finger; with angina, the patient will point with his whole palm. When examining the patient using an ECG, no signs of ischemia will be detected.
Important! Treatment and diagnosis should only be carried out by a highly qualified doctor. If you experience pain, there is no need to let the situation take its course; this can lead to death.
People prone to alcoholism suffer from alcoholic cardiomyopathy. Unpleasant sensations of aching and pulling nature occur on the second day after intoxication, extrasystole is possible.
Diagnosis of angina pectoris and systemic diseases
Persistent vasculitis can damage the coronary arteries, causing the person to experience angina-like pain. Differences can be differentiated by acceleration of ESR, shifts of protein particles. Signs include: inflammation, kidney disease, fever, pain in joints and muscles. All these signs are characteristic only of systemic diseases.
Diagnosis of angina pectoris and diseases of the lungs and pleura
With pneumonia, the patient's temperature rises, chest pain may intensify when inhaling, and wheezing occurs on auscultation. X-rays are used to confirm the diagnosis.
In the case of chronic cor pulmonale, a person will have constant chest pain that is not transmitted to the arms and shoulder blades. Even taking nitroglycerin cannot reduce the syndrome. The use of bronchodilator therapy is excellent for relieving tension.
With diseases of the esophagus, the patient experiences discomfort in the chest, with a characteristic burning sensation. They appear after eating, as well as during fasting. The ECG will not show ischemic disease.
With a tumor of the mediastinum, chest pain may appear, and when the disease develops, there will already be obvious signs:
- Impaired swallowing reflex due to compression of the esophagus.
- Swelling of the neck veins.
- Difficulty breathing.
- The neck becomes thicker.
Important! During lobar pneumonia, pain is accompanied by pleurisy. Symptoms include fever, cough, and possible heart failure.
Types of angina and symptoms
The etiology of angina is determined by two states: rest and stress. Each of them is diagnosed by determining the circumstances of the occurrence of the attacks - at what time of day and during what activity they occurred, or their approach was noticed. In turn, this system is divided into classes according to the level of severity of symptoms and endurance of the body.
- Angina pectoris. Attacks in the area behind the sternum appear during the application of physical effort, or during psycho-emotional stress, during which an increase in heart rate is observed. Symptoms are relieved with the help of a nitroglycerin drug, or when the person calms down.
Angina pectoris can be:
- First-time occurrence - lasting no more than a month from the moment when it was first noticed;
- Stable - lasting more than a month from the first manifestation. Stable angina is divided into 4 classes of severity, limited by a person’s physical capabilities;
- Progressive - increased frequency of attacks accompanied by pain symptoms. With this type of angina, changes in ECG values are already noticeable.
- Angina at rest (spontaneous) is an unprovoked vascular spasm that occurs in a state of sleep or complete relaxation.
Most often, complaints from patients sound like: pressing, sharp, burning or lingering pain behind the sternum, sometimes in the myocardium. Painful manifestations can be subtle, tolerable or painful. The pain can shoot in the lower jaw, on the left side - in the shoulders, arms, and shoulder blades. They occur during minor physical stress, such as walking. Sometimes they are a consequence of emotional turmoil.
Painful attacks of varying strength last from one minute to twenty and are stopped, depending on the strength of manifestation and experience of previous situations. The standard remedy for relieving symptoms is nitroglycerin tablets. In some mild cases, it is enough for a sick person to lie down, relax, or simply stand quietly, leaning against some support.
The attack itself is characterized by sudden suffocation, in which the patient stops all activity and freezes in the position in which the pain found him. Strangers notice the paleness of the patient's skin, and when measuring blood pressure, increased values are recorded.
Diagnosis of angina and abdominal organs and diaphragm
As a rule, diseases are accompanied by reflex pain syndrome of the heart. Any stomach disease, especially ulcers, can cause heart problems. It will be possible to establish an accurate diagnosis using FGDS, X-ray of the stomach and ultrasound, if there is no suspicion of a heart attack or unstable angina. In the case of reflex angina, which is caused by diseases of the abdominal region, the ischemic type of ECG changes is less common than with ischemic heart disease.
An important problem will be the differential diagnosis of angina pectoris, when in 20% of patients pain syndromes manifest themselves in the heart. Unpleasant sensations often appear after a meal, especially if a lot has been eaten; the problem can also arise after stress on the body, during coughing. The sensation disappears after vomiting, belching, or when the person lies down.
In acute esophagitis, a burning sensation appears in the retrosternal region, the nature of the pain stretches throughout the esophagus, and intensifies during swallowing. The sensations intensify if you eat hot or cold foods.
DIFFERENTIAL DIAGNOSIS OF ANGINA AND SOME NON-CARDIAC DISEASES
I. PLEURITIS
Damage to the pleura is almost always accompanied by pain. The localization of pain in the chest depends on which part of the visceral pleura is affected. Damage to the pleura of the upper lungs causes pain in the scapular and shoulder areas; with apical pleurisy, irradiation into the arm is possible due to irritation of the brachial plexus; with diaphragmatic pleurisy, pain in the abdomen and costal arch. The diagnosis of pleurisy is based on the following signs: • Characteristic pain syndrome: pain of a stabbing nature, clearly associated with respiratory movements, intensifies at the height of inspiration and when coughing, when bending to the healthy side, disappears when holding the breath, decreases with shallow breathing. • Pleural friction noise during auscultation, auscultatory and percussion signs of pleural effusion. • To clarify the etiology of pleurisy, it is necessary to perform a pleural puncture with bacteriological and cytological examination. Pain in diseases of the lungs and pleura, as a rule, is not a leading clinical symptom and is accompanied by cough, sputum production, cyanosis, fever, and intoxication.
II. LOUPIC PNEUMONIA.
The pain syndrome is caused mainly by concomitant pleurisy. Symptoms such as sudden onset, high fever, cough, “rusty sputum”, in severe cases, signs of respiratory and heart failure, and inflammatory changes in the blood help to clarify the diagnosis. Decisive is the detection of crepitating or fine bubbling rales, dullness of pulmonary sound during percussion, and radiological signs of infiltration of pulmonary tissue.
III. ACUTE ESOPHAGITIS.
With this condition, patients note a constant burning sensation behind the sternum, nagging pain along the esophagus, sharply intensifying when swallowing, the intensity of the pain increases when eating cold or hot food, regurgitation and hypersalivation, and heartburn are characteristic. Diagnosis is based on a typical pain syndrome, dysphagia. X-ray examination reveals impaired motor function, uneven contours, and the appearance of barium depots during erosions.
IV. OSTEOCHONDROSIS OF THE THORACIC SPINE.
At first, the pain is localized only in the affected vertebra, and only over time do symptoms of thoracic radiculitis develop, in which pain along the intercostal nerves spreads to the anterior surface of the chest. The pain is associated with movements, occurs when staying in one position for a long time, is provoked by turning the body, intensifies when moving the left hand, or coughing. Sometimes it may appear in bed at night. which can create a misconception about resting angina. The pain can be sharp, cutting, shooting, accompanied by a sensation of electric current passing. Thus, when carrying out a differential diagnosis of angina pectoris and osteochondrosis of the thoracic spine, it is necessary to take into account that with the latter there is a longer duration of pain, significant pain on palpation of the vertebrae and intercostal spaces, a decrease in pain when prescribing non-steroidal anti-inflammatory drugs and massage, and no effect from nitrates. Osteochondrosis is characterized by X-ray examination of decreased disc height, subchondral sclerosis, marginal osteophytes, and Schmorl's hernia.