Angina pectoris (chest pain caused by a lack of oxygen to heart cells) is not always accompanied by typical symptoms. Back in 1959, M. Prinzmetal described patients in whom pain occurred not during exercise, but at rest, and was accompanied not by depression of the ST segment on the ECG, but by its elevation (rise above the isoline).
Such angina was recognized as atypical and was called “variant”. In medicine, other terms are used to refer to this condition: vasospastic, angiospastic, spontaneous, Prinzmetal's angina.
Development mechanism
Angiospastic angina (another name for the process) is the result of narrowing of the coronary arteries. At the first stage, the body is affected by one or another pathogenic factor.
Which one you need to look at: harmful substances contained in cigarettes, increased levels of angiotensin-II, renin, aldosterone, cortisol, alcohol consumption and others.
Then there is stenosis or spasm of the vessels that supply the structures of the heart. Insufficient hemodynamics (blood movement through the vessels) at the local level leads to a decrease in the contractility of the muscular layer of the heart.
Hence the small release of blood into the systemic circle, poor supply of organs and systems. Both distant structures and the heart itself suffer.
In the case of Prinzmetal's angina (another name for the vasospastic form of angina), it is not clear what factor plays a role; clarification of the results does not provide any information, which affects the overall prognosis.
Distinctive features:
- Occurs in a state of complete rest, when a person is resting. Usually at night.
- Development at approximately the same time.
Stenosis of the coronary arteries occurs by 70% or more. First aid actions give a partial effect; the probability of death during an acute attack is maximum. Recovery is carried out in a hospital, then diagnostic measures are prescribed.
Causes of vasospastic angina
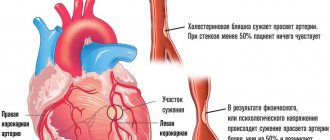
The largest arteries supplying the heart are located under its outer layer, the epicardium. With vasospastic angina, one of these arteries suddenly narrows by 30–75% of its original diameter, that is, it spasms. However, the patient has no signs of atherosclerosis.
The causes of vasospasm are not completely clear. The narrowing can be slight or extremely pronounced, occurring during stress or at rest. Known triggers for pain attacks are shortness of breath, cocaine use, and smoking. Of the biochemical substances, vasospasm is caused by acetylcholine, ergonovine, histamine and serotonin.
Acetylcholine normally dilates arteries by releasing nitric oxide from their walls. With a deficiency of this substance, the arteries, on the contrary, spasm. In addition, a lack of nitric oxide leads to increased activity of powerful vasoconstrictor substances and stimulators of thickening of smooth muscles located in the walls of blood vessels. These are angiotensin II and endothelin. Under their influence, the walls of the arteries thicken, and the lumen of the vessels decreases.
However, the role of nitric oxide in the development of vasospasm has not been definitively proven. In places where blood vessels narrow, its production is also normal. Associated mechanisms include increased phospholipase C activity, increased indicators of oxidative stress and inflammation. Personality characteristics – anxiety and constant stress – play a certain role in the development of variant angina.
Thus, the true causes of the pathology have not yet been clarified. Perhaps there are quite a lot of them, and some of them are caused by the genetic characteristics of the body.
We recommend reading the article about exertional angina. From it you will learn about the diagnosis of the condition and medications for treatment, the duration of therapy and the rehabilitation period.
And here is more information about how to relieve an attack of angina.
How dangerous is the condition?
The main threat from vasospastic angina is sudden death from one or another consequence. Among the possible complications of the pathological process:
- Heart attack. Acute death of cardiac structures. The myocardium dies rapidly, the cells destructure within a matter of hours, sometimes even faster. Necrosis is extensive, which leads to the rapid death of a person. An attack of Prinzmetal's angina ends with a similar outcome in 25% of cases. Recovery requires urgent hospitalization, assistance under the supervision of a group of specialists.
- Heart failure. Occurs in another 25-30% of cases. It is preceded by severe symptoms of an emergency condition. Emergency measures and resuscitation are a chance to save a person’s life. It requires special knowledge that almost no one has.
- Ischemic stroke. In the long term. The result of insufficient cerebral circulation. The essence is the death of neurons, without the possibility of their restoration. The process ends with a neurological focal deficit. Speech, vision, touch, muscle activity and other functions suffer.
- Severe forms of arrhythmias: ventricular or atrial fibrillation, group extrasystole.
Dangerous complications can be prevented through timely treatment and following the doctor’s recommendations. But even this is not a guarantee.
Clinical option I
In half of patients with diagnosed coronary artery stenosis, nocturnal attacks of spontaneous angina are combined with typical stable angina pectoris. In this case, attacks of angina pectoris occur during the daytime and are usually provoked by physical activity, psycho-emotional stress, and a rise in blood pressure; attacks of variant angina caused by spasm of the coronary arteries develop spontaneously at night or in the morning. Exercise tolerance in such patients may be significantly reduced due to the presence of coronary artery stenosis.
Particular attention is required in the situation when a patient suffering from exertional angina first experiences attacks of spontaneous angina, which usually indicates an exacerbation of coronary artery disease caused by destabilization of the atheroma.
Causes
Development factors are not always cardiac. Some can be corrected by the patient himself, while others are objective.
Despite the rich empirical material, doctors still cannot say exactly why such a dangerous form of angina occurs.
The only thing that can be pointed out with one hundred percent certainty is that the main reason is the narrowing of the coronary arteries.
In 90% of cases, an attack of vasospastic angina occurs against the background of complete rest. Moreover, at night, when all processes are slowed down, blood pressure is lowered, as is the heart rate.
What else can trigger an episode of violation:
- Intense physical activity inadequate to the level of training. Running, climbing stairs, carrying heavy objects, especially heavy ones. This is a relatively rare factor. This is how exertional angina develops, but not the Prinzmetal form. Although a similar scenario is possible. At the very least, it increases the likelihood of another night attack.
- Increased activity of the autonomic nervous system. Why does pathological work develop? Mainly against the background of damage to cerebral structures. The brain gives chaotic signals. There are already a lot of options here: consumption of alcohol, caffeine, drugs, especially amphetamine, stress, tumors in the skull and others. You need to find out from a neurologist or a specialized surgeon.
- Excessive ventilation of the lungs. With strong breathing against the background of an attack of bronchial asthma, panic attack, neurosis, the notorious vegetative-vascular dystonia.
- Stress, especially severe. Against the background of increased mental activity, there is a release of cortisol, adrenaline, dopamine and other substances.
The process is accompanied by a sharp narrowing of the coronary arteries, causing acute circulatory failure at the local level. In healthy people, this phenomenon almost never occurs.
The main patient population is smokers, drinkers, older men, heart patients and others. That is, those whose vessels are by default susceptible to spontaneous fluctuations in tone from the slightest deviations. An individual reaction of the body is possible.
- Low body temperature. As a result of exposure to cold water, prolonged exposure to frost, and other similar situations.
This factor is not always obvious. It is enough to sit by an open window for some time in the autumn months to become a victim of another attack. Others are more resilient. It all depends on the body’s resistance.
For what reasons does it occur?
The pathological process progresses due to:
- Violation of the functions of the inner wall of the arteries of the heart. When it is damaged, potent vasoconstrictors are intensively produced, provoking vascular spasm. The production of vasodilators, which are responsible for vessel dilation, also decreases.
- Severe spasm of the arteries supplying the heart. During this period, the passage is temporarily blocked, but its structure is not disturbed.
The coronary arteries can spasm as a result of:
- smoking;
- imbalance of potassium and magnesium in the body;
- hypothermia;
- diseases in which the immune system acts against the body's cells.
As a result of the cessation or reduction of blood flow to the myocardium, contractility and the process of conducting electrical impulses are disrupted.
This is accompanied by heart rhythm disturbances. The development of the disease is primarily promoted by atherosclerotic damage to the coronary arteries. In this case, their lumen decreases and blood flow to the organ decreases. In this case, a combination with exertional angina may occur.
Vasospastic angina is classified as spontaneous exertional angina. The development of this type of disease is accompanied by attacks of chest pain that occur regardless of exposure to stress or physical activity.
Predisposing factors
There are factors that do not directly trigger an attack, but create conditions for the formation of vasospastic angina. They are fundamental, and such moments must be fought vigorously.
- The main patient population is smokers. Up to 90% of all patients are people with a decent history of consuming tobacco products. Hence the disruption of the normal functioning of the heart and blood vessels.
Having given up the addiction, a heavy smoker can no longer count on spontaneous improvement. Long-term treatment is needed.
Duration - from a couple of years to a whole life, depends on the degree of restructuring of the body in a pathological way.
- Vegetovascular dystonia. In general, there is no such diagnosis in medical practice. It is not included in the international classifier, ICD-10. Not all doctors recognize its reality even within the framework of symptomatic complexes.
Typically, VSD is understood as a type of anxiety neurosis, a panic attack. Without going into terminological confusion, you need to measure: manifestations are represented by an increase in blood pressure, heart rate, weakness, dizziness and other moments.
The reason for this phenomenon is an increase in the activity of the autonomic nervous system. As already noted, this is a factor that provokes attacks. The correction is carried out under the supervision of a neurologist.
- Excess body weight. In this case, the role is played not so much by the weight itself, although it also determines a stable increase in the load on the heart, but by the process behind the change.
Its essence is the deviation of the movement of lipids. Fatty substances settle on the walls of blood vessels, leading to a narrowing of the lumen due to blockage.
The result is a gradual disruption of normal blood flow. Critical conditions lead to spontaneous spasm of the coronary arteries. Hence the acute, severe attacks with high mortality.
Attention:
Not all obesity leads to a similar outcome; you need to be examined by an endocrinologist.
- Atherosclerosis. Closely related to the previous option. The basis of the process is the narrowing or blockage of a blood vessel by a cholesterol plaque. The second point develops against the background of deviations in lipid metabolism.
What causes the first? Usually smoking. Alcohol intake, characteristics of individual metabolism, sensitivity to hormones and excessive spastic reaction.
Eliminating such a cause is not easy, since there are great difficulties in diagnosis.
- Severe stress on a constant basis. They end with the formation of a stereotypical reaction of the body, in particular the coronary arteries, to the influence of a hormonal factor.
- Autoimmune diseases, especially affecting blood vessels. The main process is vasculitis or inflammation of the endothelium (the internal lining of the blood supplying structures). Leads to gradual narrowing, scarring and even partial fusion of the lumen of the vessel.
Treatment tactics are strictly surgical in advanced stages. It involves prosthetics of the affected structure.
Attention:
The likelihood of death increases due to the stability of the anatomical defect.
If the first signs of deviation from the norm occur (palpitations, chest pain, etc.), you should immediately consult a cardiologist.
- Insufficient physical activity. Stagnant processes begin, including atherosclerotic ones. The connection is indirect.
- Arterial hypertension. Constant or periodic increase in pressure. Accompanied by defects, including those of the heart itself. Prinzmetal's angina against the background of hypertension has an even more unfavorable prognosis, especially without treatment.
- Pathologies of the digestive tract. Mainly intestines, gall bladder, liver. There are two reasons. On the one hand, the occurrence of persistent, but insignificant bleeding. Leads to anemia or decreased hemoglobin concentration and ischemia of all tissues. On the other hand, the production of prehormones decreases. For example, angiotensinogen. The reaction may be paradoxical.
- Alcohol consumption. The body's response to long-term use of an ethyl compound is determined by individual characteristics. Contrary to what you might think, alcohol does not have a beneficial effect on the body.
The causes are established as part of the diagnosis. By correcting possible triggers, there is a chance to prevent relapses and transfer angina into a state of stable remission for many years.
Clinical features
The hallmark symptoms of vasospastic angina most often include:
- Periodic episodes of angina at rest, often occurring in the early morning hours.
- Increased ST segment on the electrocardiogram.
- Fast acting short acting nitrates.
Vasospastic angina is characterized by the occurrence of “hot phases” with frequent repetition of attacks, which alternate with “cold phases”, with remission of symptoms over weeks or months.
Angina attacks are usually short in duration (2-5 minutes, sometimes no more than 30 seconds) and can be repeated during a single attack, which can last 20-30 minutes.
A high degree of suspicion for this disease is repeated short-term episodes of nocturnal angina, which are quickly relieved by sublingual nitrates. A similar diagnosis may also be made in cases of recurrent angina associated with syncope or even cardiac arrest, since patients with variant angina may experience malignant arrhythmias during ischemic attacks.
With the exception of tobacco smoking, the usual risk factors in the form of atherosclerosis most often do not contribute to the development of variant angina. Also, physical exercise usually does not provoke an attack of angina pectoris, while hyperventilation and exposure to cold can cause characteristic symptoms.
Variant angina may not appear for a long time, and then bother the patient with several severe attacks. During these “hot phases,” stimulating factors that would not normally trigger an episode of variant angina may contribute to the disease.
The circadian nature of this disorder is also well known and illustrated by Yasue H. et al. [1 — Circadian variation of exercise capacity in patients with Prinzmetal's variant angina: role of exercise-induced coronary arterial spasm. Yasue H, Omote S, Takizawa A, Nagao M, Miwa K, Tanaka S: Circulation 1979, 59:938-948]. According to the data, ST elevation in patients with vasospastic angina most often occurs in the early morning (5-8 hours), but in rare cases the recurrence in these patients occurs in the afternoon (3-4 pm).
Symptoms
Manifestations are generally standard for coronary insufficiency. However, the vasospastic form is determined by a more severe course, and its duration is also longer. If a standard episode lasts from 5 to 30 minutes, even an hour is not enough.
- Severe pain behind the sternum. Burning, pressing. It radiates to the arm, forearm, neck, shoulder blade. The intensity does not change when standing up or breathing. At the same time, it is impossible to distinguish the condition from a heart attack. The course of the attack is atypical. It is recommended to call an ambulance for hospitalization and urgent diagnosis.
- Dyspnea. In a state of complete rest. The episode develops spontaneously, usually at night or early in the morning while the patient is still sleeping.
- Sweating. Hyperhidrosis. The patient, relatively speaking, can be squeezed out.
- Darkening in the eyes, dizziness, vertigo. Signs of malnutrition of cerebral structures. They pose a great danger and can cause a stroke.
- Fainting state. It happens more than once, during the same attack. This is a poor prognostic sign and worsens overall outcome.
- Tachycardia. Increased heart rate. Dangerous forms of arrhythmias, such as fibrillation or extrasystoles, are not presented unless there are concomitant cardiac problems.
- Paleness of the skin.
- Cyanosis or blue discoloration of the nasolabial triangle.
- Panic attack. The patient experiences severe fear for no apparent reason. Possible sudden psychomotor agitation. A person at such a moment is inadequate and can pose a danger to himself.
- Nausea, extremely rarely - vomiting.
- Instability of blood pressure: sometimes high, sometimes low and vice versa.
Symptoms of vasospastic angina are not only cardiac, but also neurological, since the brain is affected. This increases the overall danger of the condition. Without medical care, organ failure, stroke, or heart attack are possible.
Diagnostics
It takes place in a hospital. If the patient is in serious condition, there is no point in thinking for a long time. Sometimes instrumental examination is not even carried out. There is no time for research.
The situation needs to be stabilized. The minimum that allows us to talk about angina is auscultation, measurement of blood pressure, heart rate, and assessment of respiration.
After removing a person from a critical condition, a thorough diagnosis is required:
- Oral survey. What are the complaints, how long ago have they arisen?
- Anamnesis collection. Previous and current illnesses, family history, medications taken, lifestyle, addictions.
- Measuring blood pressure and heart rate using routine methods.
- 24-hour Holter monitoring. The same indicators are subject to registration within 24 hours.
- Electrocardiography. Shows typical functional abnormalities.
- Echocardiography. Visual technique for determining the anatomical features of the heart and blood vessels.
- MRI as needed.
- Assessment of neurological status.
- MR angiography. Tomographic diagnostics of the condition of large arteries.
- General blood test, biochemical and for hormones of the thyroid gland, adrenal glands, pituitary gland.
This is sufficient in most cases. It makes sense to repeat some activities. Because the most informative data is recorded during the attack itself.
There is no provocation of an episode; it is extremely dangerous. Therefore, stress tests are contraindicated. But you don't have to wait long. The attacks recur at approximately the same time.
Treatment
In a hospital setting at an early, acute stage. Then outpatient with regularly scheduled hospitalizations. The most commonly used medicinal tactics are:
- Nitroglycerin for urgent relief of pain. These are the only approved drugs for self-help at home (1 tablet under the tongue, if there is no effect after 20 minutes, then another one). Against the background of a severe episode, the drug helps partially. No complete correction is observed.
- Cardio- and cytoprotectors to improve metabolism, protect against oxidation, and negative external influences. Mildronate, Trimetazidine in combination.
- Beta blockers. Metoprolol. It affects both blood pressure and heart rate.
- Calcium antagonists. Verapamil or Diltiazem.
- Antiplatelet agents to improve the rheological properties of blood and increase its fluidity. Aspirin-Cardio, Heparin and others. In strictly controlled dosages.
- Anti-arrhythmia medications are prescribed as needed. Amiodarone as the main one.
Attention:
The regimen should only be determined by a doctor. Many drug combinations lead to rapid development of heart or kidney failure. It is not recommended to take risks.
If organic defects are present, surgical treatment is performed. Stenting, ballooning of the coronary artery (mechanical expansion of the lumen), prosthetics of the affected area of the vessel. Bypass surgery, the creation of an artificial source of blood supply bypassing the natural one, is also possible.
Treatment of vasospastic angina has three objectives: eliminating the root cause, relieving symptoms, and preventing attacks (relapses).
As part of additional feasible measures, mandatory cessation of smoking, alcohol (alcohol), and fatty foods is indicated. It is recommended to adjust the diet in accordance with table No. 10; if possible, consultation with a nutritionist is indicated.
Coronary angiography
Unfortunately, it is quite difficult to detect coronary spasm in spontaneous variant angina. As a result, it is advisable to use functional tests to provoke spasm of the coronary arteries.
Hyperventilation and cold testing are characterized by low sensitivity, since ischemic changes in the ST segment are detected in approximately 15-20% of patients with vasospastic angina.
Many coronary angiographic centers use acetylcholine injection into the coronary arteries and an intracoronary test with ergometrine. These methods are considered the gold standard in the diagnosis of variant angina.
It should be noted that the intravenous ergometrine test, which is recorded using ECG or scintigraphy, is considered the most adequate in terms of sensitivity and specificity for identifying vasospastic reactions in patients with coronary artery disease. Acetylcholine and ergometrine tests are safe provided that the drug is selectively injected into each of the three large coronary arteries. Provocative tests without coronary angiography or in patients with high-grade coronary artery occlusion are not recommended.
After administration of ergometrine, a pronounced spasm of the proximal part of the anterior interventricular branch (LAD) of the left coronary artery is observed - dynamic occlusion ().
Forecast
Vasospastic angina is a rare form of the disease. It is diagnosed in only 1.3-2.2% of situations.
The outcome depends on the severity of the pathological process. In general, the case fatality rate is 25%. In terms of what time it is not known: it could be a day, a week, a year or more. Therefore, delaying treatment is not recommended.
Death from heart attack, stroke, or cardiac arrest is likely. At a minimum, a dangerous arrhythmia develops. With comprehensive treatment, it is possible to bring the disease under control.
Prevention
The following activities are shown:
- Quit smoking, alcohol, drugs, and self-administration of any medications, including non-steroidal anti-inflammatory drugs.
- Diet correction.
- Moderate physical activity to eliminate physical inactivity.
- Avoid stress whenever possible.
- Timely treatment of diseases that can provoke a dangerous form of coronary insufficiency.
This is not a guarantee, but the risks are significantly lower. Once a condition is detected, recommendations remain relevant.
Diagnostics and ECG signs
Making a diagnosis of Prinzmetal's angina is quite difficult, although it is crucial in treatment tactics.
On a regular ECG there are no signs of disease outside of an attack. When performing standard tests with physical activity (bicycle ergometry or treadmill test), signs of myocardial ischemia will most likely not be detected. EchoCG does not reveal any pathology directly indicating this disease.
Daily ECG monitoring is more informative. It makes it possible to record the patient’s heart readings, including at night and early in the morning. At this time, the patient experiences an attack of pain, which is accompanied by ECG changes.
A typical ECG sign of vasospastic angina is ST segment elevation in several leads. However, according to modern data, it appears in only half of patients. The remaining patients have ST depression. It can be caused not only by variant angina, but also by ordinary exertional angina, as well as by a combination of these two forms of coronary artery disease. Therefore, even daily ECG monitoring does not always clarify the diagnosis.
In practice, during daily observation, the patient is often asked early in the morning to do a hyperventilation test (breathe frequently and deeply for 15-20 seconds), perform an exercise (for example, climb the stairs) or wash with cold water. These actions can cause arterial spasm and provoke ECG changes.
Therefore, the method of choice for diagnosing Prinzmetal's angina is coronary angiography, if necessary in combination with the injection of substances into the arteries that cause their spasm.
The safest and most sensitive test is acetylcholine. It allows you to diagnose the disease in 70% of cases. If the test is positive, the probability of variant angina in the patient reaches 99%.
Acetylcholine is administered during cardiac catheterization during coronary angiography and the response is monitored. In case of angiospastic angina, this substance will cause their spasm. In this case, an important condition is the absence of atherosclerotic plaques in the arteries, otherwise it can be difficult to accurately distinguish variant angina from regular angina.
A patient with suspected vasospasm is prescribed the following laboratory tests:
- complete blood count to rule out anemia;
- biochemical analysis with lipid profile to exclude atherosclerosis;
- MV-CK and troponins to exclude myocardial necrosis, which is also manifested by ST elevation on the ECG;
- magnesium level (its deficiency can provoke attacks).
Watch the video about vasospastic angina: