Features of the disease
One of the main features of progressive angina is the rapid deterioration of the patient’s well-being and an increase in the frequency of attacks of chest pain. The general ICD code – I20.0 – unites this disease under the general formulation of unstable angina.
Depending on the moment of manifestation, this clinical symptom is divided into two groups. If squeezing and pressing pain in the chest appears during physical activity or stress (emotional stress), the disease is called angina pectoris; in their absence, angina pectoris at rest.
Important! Pain and discomfort in the absence of exercise are most dangerous.
Attacks that manifest themselves in a state of physical and emotional calm are characterized by pain intensity, duration, the presence of autonomic reactions (tachycardia, sweating, skin discoloration, nausea), severe suffocation and fear of death.
As the patient's condition worsens, progressive angina pectoris leads to the appearance of chest pain even in the absence of provoking factors. The danger of this is the high risk of heart attack: with an increase in the frequency of attacks or their duration (more than 20 minutes), the patient requires immediate diagnosis and observation in a hospital setting.
Clinical case
A 53-year-old woman, whom I had previously observed, came to see me. Her diagnosis was: “Ischemic heart disease, exertional angina pectoris II FC NK I stage CH 1 FC (NYHA). Arterial hypertension stage II, risk 4. Diabetes mellitus type 2, moderate severity, regulated .
Her main complaints were: increased frequency of attacks of anginal pain with the appearance of pain in the left half of the body (scapula, shoulder), increased shortness of breath during normal physical activity, lack of effect from 1 tablet of Sidnopharm. Objectively: auscultation heard an accent of the second tone over the aorta, 3 extrasystoles per minute. There was an increase in blood pressure to 150/95 mm Hg. Art. Clinical tests are unchanged, blood sugar is 5.9 mmol/l. In the lipidogram, cholesterol increased to 6.1 mmol/l, VLDL to 1.9 mmol/l, LDL - 3.94 mmol/l. Troponin test is negative. During 3 days of Holter ECG monitoring, the following were revealed: single extrasystoles, ST segment elevation in the lateral leads after ascending to the second floor. The results of coronary angiography showed the presence of atherosclerotic plaques in the anterior descending and circumflex branches of the left coronary artery.
The pain syndrome was successfully relieved with Nitroglycerin, and treatment was also carried out, including anticoagulants (Cibor) and metabolic therapy (potassium-magnesium mixture). Statins (Mertenil), beta-blockers (Carvedilol), antiplatelet agents (Lopigrol), nitrates to resolve the attack (Nitrosprey) were prescribed, and stenting of the affected vessels was recommended. The patient refused surgical treatment, but noted a decrease in the number of anginal attacks.
Progressive angina is a common pathology that requires immediate hospitalization when detected. Based on my personal experience, I would like to note that surgical techniques show the best results in the treatment of this disease. In most cases, my patients who underwent stenting and coronary artery bypass grafting of coronary vessels damaged by atherosclerosis noted a complete regression of clinical manifestations.
Do you have any friends or relatives who have undergone surgery for progressive exertional angina?
Classification of the severity of the patient's condition
To determine the severity and characteristics of the patient’s condition, cardiologists use the Braunwald classification.
| Severity and specificity of the condition | A – secondary unstable angina | B – absence of external cause for attacks | C – post-infarction manifestations |
| I – the appearance of attacks for the first time, only in a state of tension | IA | IB | IС |
| II – presence of angina attacks at rest during the last month, not in the next 2 days | IIA | IIВ | IIС |
| III – manifestation of pain in a calm state in the next 2 days | IIIA | IIIB | IIIС |
Class A combines cases of unstable angina, which are aggravated by additional factors - tachyarrhythmia, low hemoglobin levels, hyperthermia, the presence of infection in the patient's body, respiratory failure, intoxication with thyroid hormones, hypotension and uncontrolled hypertension.
Class B includes all clinical cases of the disease in which cardiac ischemia is not combined with the above conditions.
Class C defines early post-infarction attacks: this diagnosis is made to patients with characteristic chest pain that appeared within 2 weeks after an acute myocardial infarction.
The disease can progress and occur in various forms depending on the signs associated with changes in the intensity or frequency of its attacks. The following options are possible:
- The attacks become more frequent, but no change in the nature of the pain is observed.
- The intensity of pain and the duration of attacks increases, but their frequency remains unchanged.
- Pain manifests itself both during exercise and at rest alternately (subacute angina of exertion and rest, which is defined as class II).
- The frequency, duration and intensity of attacks of pain behind the sternum simultaneously increases.
The above-described symptom of coronary heart disease can occur both with complete absence of treatment or minimal use of drugs, and with adequate and even intensive therapy, including intravenous administration of antianginal medications. Classification depending on the presence or absence of therapeutic measures against the background of attacks of the disease makes it possible to more accurately determine the severity of the patient’s condition and the prospects for outpatient treatment.
Symptoms
Progressive angina is distinguished by a number of features that are characteristic specifically for this type of cardiac pathology. Myocardial dysfunction manifests itself in completely different forms. Sometimes symptoms can generally be confused with signs of other diseases. People need to become more health conscious. This will make it possible to notice problems in the body in time and contact a competent specialist. Only a cardiologist can help cope with the manifestations of angina pectoris. It is not recommended to resort to dubious folk methods and visit healers. As medical practice shows, this only aggravates the situation, and the patient himself loses precious time.
Progressive angina, like any other disorder of the body, manifests itself in its own way. It is extremely important to know the main signs of this pathology in order to consult a doctor in time. Diagnosis of the disease in the early stages greatly facilitates treatment and increases its effectiveness. The following signs may indicate the presence of a progressive form of angina:
- an increase in the number of attacks over a certain period of time;
- worsening of attacks;
- the patient’s inability to withstand basic physical activity;
- a feeling of tightness in the throat;
- the appearance of cold sweat;
- nausea for no particular reason;
- heartache;
- lethargy;
- shortness of breath at the slightest physical exertion;
- fast fatiguability.
The above symptoms are the main ones. They are often accompanied by irritability, apathy, sudden weight gain, increased appetite, and problems with emptying the rectum. Manifestations of the disease, as a rule, depend on individual factors, such as the level of physical fitness, genetic characteristics, lifestyle, nutrition, type of professional activity, exposure to stress, and the degree of moral and psychological stability.
The patient's medical history should be thoroughly studied by the attending physician. Only on the basis of a thorough analysis of previous diseases and chronic pathologies will the doctor be able to make a true diagnosis and prescribe adequate treatment. The main task of the patient is to seek help in time and not to self-medicate. Today, medicine is so developed that you can live with IHD for many years and even decades.
Causes of development of progressive angina
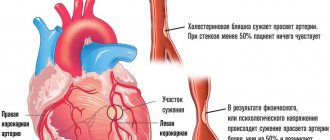
The most common cause of progressive angina is coronary heart disease complicated by atherosclerosis. The vessels through which blood is delivered to the heart muscle narrow due to the deposition of cholesterol plaques on their walls. Due to the narrowing of the lumen of the arteries, the myocardium is not sufficiently supplied with oxygen and metabolic disorders occur in muscle tissue.
At the initial stage of development of the disease, angina attacks occur only during intense physical or emotional stress, during which the blood supply to the myocardium normally increases. The transition of the disease to a progressive form, changes in the intensity and duration of attacks are usually associated with damage to atherosclerotic plaques due to internal or external causes, and active thrombus formation.
Blood clots formed in the area of damage further narrow the lumen of the vessel, provoking the development of angina at rest. In addition, when clots break off, complete blockage of small vessels and microinfarction often occur. The most difficult clinical case is the fusion of a blood clot with connective tissue and the subsequent ingrowth of the resulting neoplasia into the wall of the coronary artery.
The medical history of a patient with angina pectoris may include other cardiac pathologies: coronary spasm, cardiomyopathy, aortic insufficiency, aortic stenosis.
For patients with atherosclerosis and coronary heart disease, living conditions, bad habits and diet are of great importance. Risk factors that increase the likelihood of angina going into an unstable stage are long-term smoking, physical inactivity, a high percentage of fatty foods on the menu and poor diet, as well as systemic diseases associated with metabolism (obesity, diabetes).
Causes
Often, progressive angina is observed with the development of atherosclerosis, which affects the coronary vessels of the human heart.
The lumen in the arteries actively narrows as atherosclerotic plaques spread and mature there.
There are a number of provoking factors that can aggravate the course of the disease. These include:
- tachycardia;
- increased blood pressure;
- psychological and emotional overload;
- excessive physical activity;
- abuse of alcohol and tobacco products;
- uncontrolled use of medications;
- a diet that includes a large number of foods high in cholesterol, etc.
Therefore, for patients with coronary artery disease, it is extremely important to adhere to the rules of a healthy lifestyle, eat healthy, and eliminate all kinds of provoking factors.
Symptoms and diagnosis
Depending on the stage of the disease, progressive angina is manifested by a number of characteristic symptoms:
- At the first stage, attacks of pressing chest pain occur only under severe stress and physical strain.
- At the subacute stage of the disease, pressing pain turns into burning pain and radiates to the left arm and back. Shortness of breath, arrhythmia, dizziness, sweating and general weakness appear. A common complaint at the second stage is nausea and vomiting. Seizures occur even at rest.
- The third stage is manifested by prolonged attacks at rest, which are not controlled by standard doses of medications. The pain becomes more intense and can radiate to the peritoneum and lower extremities.
The third stage is the most unstable and requires immediate hospitalization - there is a high risk of heart attack.
A modern algorithm for determining the causes of angina pectoris necessarily includes instrumental and laboratory tests. Required research includes:
- General blood analysis;
- Glycated hemoglobin test;
- Analysis of the level of thyroid hormones (if there are signs of thyroid dysfunction);
- Analysis of blood biochemistry to assess the function of the cardiovascular system and kidneys, as well as samples of markers of myocardial damage (troponin and creatine phosphokinase fraction).
Laboratory tests help to quickly identify each clinical case complicated by other systemic pathologies (thyrotoxicosis, diabetes, anemia).
The most informative and simple instrumental method of research for angina pectoris is an ECG. The cardiogram is taken at rest, during exercise (stress studies, treadmill test and bicycle ergometry), as well as during daily activities (daily monitoring or Holter method).
Echocardiography and ultrasound in a calm state make it possible to assess the function and size of the ventricles of the heart and exclude concomitant disorders.
If patients cannot perform physical activity according to the standard of the studies described above, then they are administered drugs that stimulate cardiac activity and undergo scintigraphy or echocardiography.
Diagnostics
None of the patients like to take tests or go for an ECG. At least, I have not yet met anyone who is eager to go through the entire necessary set of studies. However, comprehensive diagnosis is a very important point that cannot be neglected. What is important here is a thorough collection of characteristic complaints (onset, duration of attacks, collection of risk factors and treatment used), measurement of blood pressure, pulse and auscultation of the heart. Using the latter, it is possible to identify an accent of the II tone over the aorta, a pathological III tone, and a systolic murmur at the II point.
I also prescribe the following minimum laboratory and instrumental types of research to my patients:
- ECG (read about characteristic changes on the film here)
- general blood and urine analysis;
- Holter monitoring of the electrocardiogram for 3 days;
- ultrasound examination of the heart (EchoCG);
- lipid profile - determination of the level of fats of various fractions;
- coronary angiography - X-ray contrast examination of the blood vessels of the heart;
- troponin test - identification of specific cardiac markers.
Treatment and prevention of progressive angina
With progressive angina, treatment largely depends on the patient's daily routine and diet. The patient’s independent actions during therapy should include:
- giving up bad habits (drinking alcohol, smoking);
- daily but moderate exercise (cardio exercise);
- taking multivitamin and mineral courses with potassium, magnesium, calcium;
- reducing the consumption of animals and other fats (up to 30% of the calorie content of the daily menu).
These same measures are effective in preventing the development of angina pectoris. Diseases are easier to prevent than to treat, so people over 45 years old should reconsider their diet, work and rest.
The drug treatment course includes drugs such as:
- β-blockers, which reduce the oxygen demand of the heart muscle;
- calcium channel blockers, which prevent narrowing of the coronary arteries;
- antiplatelet agents, blood thinners;
- fibrates, which reduce the risk of trauma to atherosclerotic plaques;
- statins, which reduce the concentration of cholesterol in the blood;
- nitrates that relieve angina attacks (nitroglycerin, isosorbide mono- and dinitrates);
- ACE inhibitors, which lower blood pressure;
- diuretics, which remove fluid from the body;
- other drugs if the standard treatment protocol is ineffective (Ranolazine, Nicorandil, Trimetazidine, Ivabradine).
If the progression of the disease does not allow us to limit ourselves to drug therapy, cardiologists may resort to surgery. There are two generally accepted methods of surgical treatment of progressive angina:
- Angioplasty or stenting of the coronary arteries, in which the lumen of the vessel is expanded using a special metal frame.
- Coronary artery bypass surgery, which creates a shunt, a “bypass”, between the aorta and the coronary artery. The material for the shunt is the patient’s own vessels (internal thoracic or radial artery, great saphenous vein of the leg).
Traditional medicine offers aloe, garlic, lemon, hawthorn and various soothing herbal preparations for the treatment of angina.
It should be noted that not a single traditional method is able to reduce the risk of heart attack in case of progressive disease and the absence of drug therapy.
How is IHD diagnosed?
The main task of a cardiologist is to make an accurate diagnosis and give a clinical opinion. Only after this can you begin to prescribe medications or recommend more radical methods of stabilizing the patient’s condition. Diagnostics is carried out in several stages. It includes the following procedures:
- electrocardiogram;
- studies of the carotid artery using Doppler;
- ultrasound diagnostics of the heart;
- laboratory examination of a general blood test.
If necessary, the doctor may prescribe additional procedures. The choice of diagnostic methods varies depending on the reasons that caused the disease. The main signs of angina pectoris are clearly visible on the ECG results. Examination of the carotid artery shows how well the heart is supplied with blood.
If angina is not detected in time, coronary artery disease can provoke myocardial infarction. A sudden attack most often leads to death. However, a heart attack can be prevented by going to the hospital in time. The following symptoms indicate an approaching attack:
- constant anxiety;
- feeling of intense fear for no apparent reason;
- an attack of angina that lasts more than 20 minutes;
- heart pain during sleep;
- the appearance of severe attacks in complete rest;
- negative ECG result.
As a rule, it is the electrocardiogram that shows that myocardial infarction is approaching. At the same time, the heart rhythm is completely disordered. During ultrasound diagnostics, coronary arteries are visible on the computer screen, the lumen of which is almost completely blocked by a thrombus or plaque.
Possible complications and prognosis
The prognosis for patients diagnosed with coronary heart disease, angina pectoris with timely treatment is quite optimistic. Less than 40% of patients suffer a heart attack or die.
However, the prognosis in each case depends on the presence of concomitant diseases and the stage of the disease. Subacute angina pectoris at rest and acute angina at rest require hospitalization of the patient. In the earlier stages, regular monitoring and following all the cardiologist’s recommendations are sufficient.
If treated incorrectly or untimely, progressive angina can result in dangerous complications, including chronic heart failure (CHF), arrhythmia, ischemic stroke, cardiac asthma, coronary thrombosis and pulmonary edema.
It is necessary to prevent attacks and give up bad habits not only for those who have learned from their own experience what progressive angina is, but also for healthy people who are at risk due to age or concomitant diseases. If you have pain in the sternum, it is necessary to undergo a comprehensive diagnosis and receive medications that will reduce the risk of heart attack and dangerous complications of ischemia. Timely treatment is the key to a positive treatment prognosis.
Symptoms: how to understand that you are developing a pathology?
Traditionally, angina is characterized by pronounced symptoms, so it is simply impossible not to notice the onset of attacks. Another thing is that many patients do not resort to therapy, attributing pain to already identified diseases, for example, coronary artery disease. How does progressive angina manifest itself? There are several symptoms:
- Increased frequency of attacks and their duration compared to previous periods;
- Minor physical or emotional stress is enough for pain to occur;
- Choking, vomiting, dizziness are infrequent symptoms that indicate a deterioration in the patient’s general condition;
- The pain changes location - it is felt not only behind the sternum, but also radiates to the arm and other parts of the body;
- Seizures can occur spontaneously without reference to your activities, even at rest;
- Heart rhythm is disturbed;
- Unpleasant sensations often occur at night, symptoms become more intense;
- Emergency medications, for example, nitroglycerin, do not bring relief, or slightly dull the pain, and the attacks continue to progress;
- Weakness, pressure surges, and a feeling of panic are signs that may indicate a heart attack or pre-infarction condition.
This negative picture is not the only problem. So, if the patient ignores treatment, the prognosis will be extremely unfavorable. But with timely contact with specialists, you can count on improvement.
How to distinguish progressive angina from myocardial infarction? In case of a heart attack, the duration of attacks is more than half an hour, in case of angina pectoris – up to 20 minutes.
Thus, if you suspect that you are developing a dangerous pathology, you should not delay your visit to the doctor. When the attack has already begun, and the pain is only getting worse, call an ambulance, because jokes with coronary diseases are unforgivable and fraught with serious consequences.
What is progressive angina and how is it treated?
According to statistics, the largest number of deaths in adulthood occurs due to pathologies of the cardiovascular system. Among them, the most common today is progressive angina, which appears as a reaction of the body to coronary heart disease.
According to statistics, the largest number of deaths in adulthood occurs due to pathologies of the cardiovascular system. Among them, the most common today is progressive angina, which appears as a reaction of the body to coronary heart disease.
What are the manifestations of coronary artery disease?
Chest pain is a common manifestation of poor myocardial perfusion and presents with discomfort in the center of the chest, which may be accompanied by tingling, burning, or pressure. Angina pectoris provokes pain that is felt in both arms, neck, lower jaw and in the epigastric region.
Manifestations of coronary heart disease include:
- Period without symptoms. The process of atherosclerosis does not cause symptoms. Additionally, patients with severe coronary artery stenosis may not experience symptoms despite the presence of atherosclerotic lesions in the coronary arteries. It should be noted, however, that in many patients, despite the presence of severe coronary artery stenosis, no warning symptoms are observed (especially in patients with diabetes mellitus). This kind of manifestation of coronary heart disease is especially “insidious” and dangerous. Another reason why warning signals do not appear may be that as the lumen of the coronary vessel gradually becomes blocked, the adjacent arteries feeding the neighboring areas maintain the overall blood flow, thereby helping to compensate for the stenosis and meet the needs of the heart muscle. This intertwined vascular network helps protect many patients from a possible heart attack by bypassing what is essentially a blocked artery. The lateral network of vessels can also proliferate after a heart attack, helping to normalize erratic blood flow and allowing repair of the defective area.
- Persistent angina. Angina occurs during exercise or during intense emotional stress. Persistent angina is usually a relatively mild clinical condition and usually offers the opportunity to select and apply appropriate treatment.
- Unstable angina. This is the appearance of lower back pain at rest. This is a more dangerous form of coronary heart disease, so it has been characterized as preventive angina. It is clear that such an unstable situation should be treated by admission to the hospital in order to avoid unwanted progression of myocardial infarction by applying appropriate treatment.
- Acute myocardial infarction. This is necrosis of the heart muscle area. It manifests itself as typical angina, which has a long duration, does not stop after rest and lasts more than half an hour. Immediate transport of the patient to the hospital is necessary because only in a specialized clinic and with qualified personnel can such a serious medical problem be resolved safely.
Classification
Angina pectoris has 3 options for the manifestation of symptoms with an individual clinical picture, but similar processes of myocardial pathology:
- Angina pectoris. It manifests itself when emotional stress, overload at work and during sports appear in the patient’s life.
- Angina at rest. Its causes may be different, but the disease manifests itself in a calm state of the patient - with normal pulse and blood pressure, even during sleep.
- Unstable angina. The disease with the highest probability of myocardial infarction, the most common condition is considered progressive angina. During an attack, the pain increases quickly, and the state of health sharply worsens even after stopping physical activity, sometimes at rest. Nitroglycerin stops working, increasing the dosage or switching to narcotic painkillers is required.
Doctors distinguish 4 classes of angina severity:
- Latent, discovered randomly, without symptoms or attacks.
- A mild form that requires minor restrictions on sports and exercise.
- A form of moderate severity, with a partial ban on physical labor and physical education.
- Severe form with a complete ban on physical activity due to the huge risk of attack and heart attack.
Treatment
Doctors strongly recommend comprehensive treatment of angina for maximum effect.
Drug therapy
After examination and diagnosis, the doctor prescribes the following medications to a patient with progressive angina:
- Nitroglycerine. The drug relieves attacks well in the early stages of the disease. The dose is 0.5 mg, the tablet is placed under the tongue for resorption, and if the effect is weak, it is taken again.
- Treatment of angina pectoris accompanied by hypertension is supplemented with drugs to lower blood pressure (Indapamide, Anaprilin).
- For unbearable headaches, analgesics (Nurofen, Ketanov, Diclofenac) are prescribed.
- In severe forms of the disease, beta-blockers are prescribed to reduce the intensity of the heart and stop the attack (Metoprolol, Propranolol).
- Anticoagulants in case of threat of thrombosis (Heparin, Phenilin).
Lifestyle change
It is the wrong lifestyle, lack of exercise and bad habits that in most cases lead to the appearance of cardiovascular diseases. With drug treatment alone, the symptoms of the disease can be relieved, but relapses cannot be avoided. Therefore, patients need:
- stop smoking, alcohol, and taking drugs;
- gradually increase physical activity, exercise regularly and monitor your well-being during exercise, avoiding overload;
- spend more time in the fresh air, sleep with the window open, ventilate the bedroom before going to bed.
- adhere to proper nutrition: diversify your diet with fresh fruits and vegetables, avoid fatty, fried and spicy foods, reduce salt intake, control body weight.
Alternative medicine
Patients undergoing a course of bloodletting with leeches note a significant improvement in their condition and pain relief. The course consists of 12-14 procedures with 6-9 leeches per session.
ICD 10 code for exertional angina: symptoms, causes, treatment – Vascular health
Angina pectoris refers to the clinical forms of coronary heart disease (CHD).
It is a disease characterized by pain in the chest that occurs during physical activity, stress, and strong emotions. Predisposing factors for the development of the disease include:
- Reasons beyond the control of the person:
- floor;
- age;
- heredity.
- Directly dependent on the patient:
- obesity;
- smoking;
- sedentary lifestyle;
- poor nutrition.
- Concomitant pathology:
- Hypertonic disease;
- Diabetes;
- Hypercholesterolemia (increased content of the “bad” cholesterol fraction in the blood).
What happens in the vessels of the heart during angina pectoris?
The main mechanisms that determine the clinical picture come down to the following points:
- Blockage of the lumen of the heart vessels with atherosclerotic plaque.
- Local or diffuse spasm of the affected arteries.
- Microvascular damage.
- Disruption of the normal functioning of parts of the heart (primarily the left ventricle).
Taking into account the mechanisms described above, damaged arteries are not able to cope with this task. As a result of this imbalance between the need for oxygen and the inability to supply the heart with it, a classic pain syndrome for angina pectoris develops - “angina pectoris”.
Classification
In cardiological practice, angina pectoris is divided into two types:
- stable;
- progressive.
This clinical classification is important for selecting adequate therapy, which is carried out on an outpatient or inpatient basis.
When formulating a diagnosis, the doctor always indicates the functional class. This division helps determine the severity of the disease.
Functional classes (FC) of angina according to the international classification of the Canadian Society of Cardiology.
Functional class Characteristics of daily physical activity
I Cardiac - bothers you under heavy loads. Normal physical activity is not affected.
II There is a slight limitation in daily physical activity. For attacks to occur, physical activity in the form of fast walking more than 500 m on level ground or climbing more than one flight of stairs is sufficient.
III There is a marked decrease in usual physical activity. Seizures are triggered by walking less than 500 m or when climbing one flight of stairs.
IV Severe form, characterized by the occurrence of pain with minimal load and at rest
Formulation of diagnosis
The ICD code for angina is I20.0.
- In a stable form, the diagnosis is as follows:
- IHD: angina pectoris I-IV FC.
- If unstable:
- IHD: progressive angina pectoris resulting in angina pectoris of class I-IV.
Clinical picture
- Localization: behind the sternum, in the left half of the chest. It can radiate under the left shoulder blade and into the lower jaw.
- Duration up to 10 minutes.
- The attack resolves on its own with rest or with the use of short-acting nitrates.
- Accompanied by general symptoms - shortness of breath, nausea, dizziness. There is often a feeling of fear.
They also note a decrease in performance, rapid fatigue, and general weakness.
Diagnostics
- clarification of the patient's complaints;
- collecting anamnesis of life and the development of the disease, identifying risk factors;
- objective examination data;
- laboratory and functional examinations.
According to national clinical guidelines, the “gold standard” for diagnosing CAD is coronary angiography (CAG). The essence of the procedure is to visualize the heart vessels after administration of a contrast agent.
If large atherosclerotic plaques are detected, coronary angiography can also become a therapeutic operation.
Additional methods (ultrasound of the heart, ECG, Holter study) give the doctor the opportunity to suspect exertional angina. They are non-specific.
A little about coronary angiography
The correct name for this procedure is percutaneous transluminal coronary angioplasty with or without stent placement. Refers to radiopaque research methods.
During the procedure, a puncture is made in the femoral or radial artery. A special conductor is inserted through it to the heart. The patient does not experience pain.
Then a contrast agent is injected and the coronary arteries are observed on the monitor using an angiograph. In this case, vascular spasm may occur, accompanied by pain in the chest. The attack is short-lived and goes away on its own or after adding nitrates.
If the study reveals complete blockage (occlusion) of the coronary artery, then stenting is performed. For these purposes, a special device is introduced along the guide to the desired location, which increases the lumen, restoring it. This expander is called a stent.
After the procedure, the patient is prescribed bed rest. If CAG was performed through a puncture on the femoral artery, then it is strictly forbidden to get up during the day. This measure is an effective prevention of bleeding.
Treatment
The main goals of therapy are:
- prevention or relief of pain;
- prevention of the development of dangerous complications;
- improving prognosis and quality of life.
- General recommendations:
- to give up smoking;
- weight loss;
- informing the patient in special schools for coronary heart disease;
- proper nutrition;
- healthy sleep;
- treatment of associated pathology.
- Medication prescriptions:
- aspirin – cardiomagnyl, cardioASK;
- beta-blockers – concor, betaloc ZOK, nebilet, carvedilol, nipperten;
- statins – Atoris, Torvacard, Crestor, Vasilip;
- ACE inhibitors – Enap, Diroton, Prestarium, Perineva, Lisinoton, Amprilan.
This prescription of drugs is called ABCD therapy. When a person is diagnosed with exertional angina, all of the listed groups of drugs are prescribed simultaneously! In case of drug intolerance, the doctor adjusts the prescriptions on a case-by-case basis. You need to take medications for life!
Cardiologists strongly recommend having in your first aid kit the medications necessary for emergency cessation of severe pain.
They are taken sublingually (under the tongue). Their effect develops almost immediately.
- Surgical intervention:
- CAG with stent installation (coronary artery dilator);
- coronary artery bypass grafting.
Treatment of progressive angina must take place in a hospital setting, since this condition is regarded as pre-infarction.
Complications
The most important and formidable consequences are:
- myocardial infarction;
- sudden death.
Prevention
It is necessary to prevent, identify and treat angina pectoris with the participation of a cardiologist and a therapist. The patient's compliance with all recommendations is an important part of the treatment process. To do this, it is necessary to explain to patients the reasons for such numerous prescriptions. It is unacceptable to self-medicate this disease. This can lead to dire consequences.
Source:
Stable angina: symptoms, causes, treatment, ICD 10 code
Coronary heart disease (CHD) is damage to the myocardium (the muscular middle layer of the heart) caused by a decrease or complete cessation of arterial blood flow into the heart.
It is caused by damage to the coronary arteries - narrowing or complete blockage due to cholesterol deposits on the inner walls of the vessels. For many years, IHD has been the leading cause of death in developed countries.
A particularly frequently diagnosed form of IHD is exertional angina (ICD 10 code I20.8), mainly stable angina.
Description and classification
To determine the severity of angina pectoris, the Canadian Heart Association classification is used. There are 4 functional classes (FC):
- Angina pectoris is caused only by very intense and prolonged exercise.
- Load limitation. Angina is caused by fast walking, fast climbing stairs or uphill; walking in the cold and wind, after eating; with strong emotions.
- The load is limited to a large extent. Angina is caused by walking 100-200 m or climbing 1 flight of stairs.
- Minimal physical activity causes pain. Seizures occur even with complete rest.
Attention!
Angina is a condition in which a person experiences paroxysmal chest pain. It is caused by physical activity, stress and even cold or overeating.
There are new-onset (lasting less than a month before detection), stable and progressive (with more frequent attacks) angina pectoris. In the future, angina at rest may develop, when attacks occur even in the absence of any stress.
An attack of stable angina is caused by a load of the same level and goes away within 1-5 minutes after stopping the load. If such attacks are repeated within 3 months from the moment of the first manifestation, then angina is defined as stable.
Symptoms
The main symptom of angina is chest pain. The pain can be pressing, burning, squeezing. In mild cases, chest discomfort is felt. Usually the pain is localized at the top and middle of the sternum, less often - in the projection of the heart or in the epigastric region (the area corresponding to the projection of the stomach).
The pain radiates (radiates) usually to the left arm, shoulder, collarbone, scapula, and to the left side of the lower jaw. Occasionally the pain radiates to the right side of the body. Sometimes there is radiating pain without chest pain. Increased sweating, difficulty breathing, nausea, and vomiting are often observed.
Typically, an attack occurs during physical exertion or stress. In addition to stress, it can be triggered by increased blood pressure, an attack of tachycardia, exposure to cold and wind, and too much food.
Usually an attack has a beginning and an end, the pain increases gradually, passes quickly, leaving no discomfort. The typical duration of an attack is 1-15 minutes.
As a rule, stable angina quickly goes away from taking Nitroglycerin under the tongue.
Causes
When the diameter of the main coronary artery narrows by 70% due to cholesterol deposits (sclerotic plaques), the blood passing through the artery can still provide the myocardium with oxygen, but at rest.
However, such an artery is not capable of meeting the increased demands of the myocardium caused by stress. With increasing load, the heart rate (HR) increases, blood pressure (BP) increases, and myocardial contractions intensify.
Therefore, the myocardium needs more oxygen delivered by arterial blood.
Occasionally, angina pectoris occurs without visible narrowing in the coronary arteries, but in such cases, angiospasm (periodic spasm of small arteries) or dysfunction of the endothelium (cells of the inner surface) of the coronary vessels is almost always observed. Sometimes angina is caused by valvular heart defects, inflammatory or allergic vascular diseases, mechanical compression of blood vessels due to the development of scars, anemia, and so on.
On a note!
An attack of angina can also be caused by the influence of the esophagus, biliary tract, spine, if there are diseases of these organs.
Signs of the disease
The pathology often affects people of retirement age, mainly men. But recently, doctors have noticed that the disease has begun to occur in younger people. And this trend is growing.
Progressive angina is a complication of unstable angina. A distinctive feature of the disease is that attacks that previously occurred after increased physical activity now begin during normal physical activity or spontaneously, even at rest.
The frequency and severity of attacks increase, and the progression of the disease can occur very quickly.
Signs
It is impossible not to notice the symptoms of progressive angina. The main symptom is pain in the heart area. The feeling of pain in the chest can also occur with other diseases, so below are all the symptoms of progressive angina:
- painful attacks become more frequent and last longer;
- attacks occur with minor physical exertion;
- during an attack there is a feeling of suffocation;
- nausea may develop into vomiting;
- the area of pain becomes wider;
- to numb the pain, you need to increase the amount of the drug, the previous dosage does not help;
- an attack may have no connection with stress, but may appear for no reason even at rest;
- The doctor will notice changes in the ECG results.
Important!
Progressive angina can take a person by surprise even at night, when the body is completely relaxed. Due to their intensity, attacks at night are much more difficult to bear than those that occur during physical activity.
The disease may also be characterized by other, less pronounced symptoms. Above are the most common ones that you need to pay attention to before seeing a doctor.
Clinic
All patients suffering from unstable angina describe a typical pain syndrome. The nature of the sensation is burning, pressing, squeezing. They are localized in the upper or middle third of the sternum, the apex of the heart, and sometimes in the upper abdomen.
A characteristic feature is pain radiating to the left arm, scapula, collarbone, and lower jaw. However, there are rare cases when such sensations appear on the right side. An important clinical and diagnostic criterion for both coronary artery disease and progressive angina is the connection with certain factors.
An attack is provoked by physical activity, psycho-emotional stress, cold weather, heavy food intake, a sharp increase in blood pressure, and a transition to a horizontal position from a vertical one.
We must not forget about the equivalents of the disease, when anginal pain is accompanied by shortness of breath, fainting, and weakness in the left arm.
The sensations last for several minutes and are quickly relieved by taking nitroglycerin. Each type of unstable angina has its own clinical characteristics.
What is ischemic disease
IHD and angina accompany each other, but the symptoms may be different. The heart is the main and most important organ in the blood circulation. It is a kind of muscle pump, thanks to which blood reaches all organs of the body through blood vessels. The heart has its own blood flow (coronary), which provides a constant flow of oxygen and essential substances necessary for its functioning.
It develops when the blood vessels that supply blood to the heart become clogged or narrowed. The result of this is the lack of sufficient oxygen needed by the heart. Therefore it starts to work incorrectly. IHD with an accompanying sensation of pain radiating to the lower jaw, neck and arm indicates the need for emergency care.
The most common and main cause of coronary heart disease is atherosclerosis of the coronary arteries. It is a disease that develops very slowly as one ages.
Atherosclerosis itself is a complex process of deposition of various substances on the inner walls of blood vessels. As a result of thickening of their walls and decreasing lumen, blood flow in the heart muscle is significantly reduced. Blood flow may be obstructed by a sudden spasm or blockage by a blood clot.