Development mechanism
To better understand what parasystole is, it is necessary to take a closer look at the features of the development of this disease. Normally, the heart rate is set by the sinus node located in the myocardium. This value is not constant and depends on a number of processes occurring in the body. With increased loads, the heart rate increases, and on the contrary, when a person rests, the heart rate slows down.
During parasystole, there is another source in the heart muscle that generates electrical impulses. It has its own rhythm, which does not depend on signals received from the body. This leads to the phenomenon of double rhythm formation, when the contraction of the heart muscle is influenced by impulses from either the sinus node or its competitor, depending on the speed of the signal.
In a patient, such disruptions may manifest as increased heart rate (tachycardia) or another type of arrhythmia. When impulses alternately enter the heart muscle, a person may feel heart revolutions, sharp shocks, and stops. According to ECG data, the heart of a patient with parasystole on average makes about 30 thousand incorrect contractions per day.
Reasons for appearance
All causes of the disease are divided into two groups:
- cardiac;
- extracardiac.
If the examination fails to detect any reasons for the development of such arrhythmia, then we are talking about idiopathic parasystole.
Cardiac causes include:
- cardiac failure;
- myocardial inflammation;
- heart defects;
- heart attack, etc.
Extracardiac:
- hormonal disorders (hypo- and hyperthyroidism, pathologies of the adrenal glands);
- overdose of certain medications;
- imbalance of electrolytes in the blood;
- disorders of the autonomic nervous system;
- hyperglycemia;
- anemia.
Thus, this type of arrhythmia can be caused by various reasons, including those not directly related to the heart. I would like to advise a person who experiences symptoms characteristic of parasystole to immediately consult a therapist or cardiologist.
Causes of the disease
This disease can develop in the body for several reasons, which can be divided into groups:
- cardiac, when the disease occurs due to cardiac diseases;
- extracardiac, not related to heart disease;
- idiopathic, when it is not possible to identify the source of the disease.
The most common cardiac causes are:
- Coronary heart disease, in which disruptions in the blood supply to the heart muscle occur due to damage to the arteries of the organ.
- Myocarditis, in which an inflammatory process is observed.
- Myocardial infarction, in which some of the cells responsible for contracting the heart muscle die.
- Mitral valve prolapse. With this disease, the valve flaps bend, preventing blood from flowing back into the chambers of the heart.
- Heart failure, which causes problems with the contractility of the organ.
- Cardiomyopathy, when a number of functional and structural changes in the heart muscle are noted.
Noncardiac causes include:
- Hormonal imbalances caused by diseases of the thyroid gland or adrenal glands.
- Increased blood sugar.
- Anemia (anemia).
- Problems with the autonomic nervous system.
- Overdose of drugs.
- Imbalance of electrolyte composition of the blood.
In healthy people and athletes, the disease occurs due to hypertonicity of the vagus nerve. This is a state of the body in which complete relaxation of the myocardium is not observed, which leads to a gradual weakening of the sinus node and activation of the parasystolic focus, which begins to actively compete, causing disruptions in the heart rhythm.
What it is
Ventricular parasystole is a type of arrhythmia in which, in addition to a normally functioning rhythm regulation system, electrical impulses are also produced by an additional pathological focus. This is the cause of double rhythm formation, manifested in two forms of arrhythmia:
- extrasystole (extraordinary heart contractions, controlled from a pathological focus);
- episodes of tachycardia (increased heart rate).
An additional center of rhythm formation is called a paracentre. Electrical impulses constantly emanate from it, the frequency of which can vary from 20 to 60 per minute. Parasystole occurs not only in patients with cardiac pathology, but, occasionally, in practically healthy people, and even in active professional athletes.
One study involved 200 patients with ventricular parasystole, ranging in age from 17 to 77 years. Of these, coronary heart disease was detected in 54% of patients; hypertension - 32%; mitral valve prolapse - 8%; without organic cardiac pathologies - 6%.
Forms
Depending on the location where the additional node is formed, the disease is divided into the following forms:
- Ventricular parasystole (ventricular), when the appearance of a competitive source of impulses occurs in the ventricle.
- Atrial, in the presence of an extra node in one of the atria.
- Multiple, if in one of the heart chambers there are several extra sources.
- Combined. In this case, additional impulses may occur in different parts of the heart.
Where should parasystole be classified in the classification of arrhythmias?
Classifications of arrhythmias are based on different characteristics, each with its own disadvantages:
- according to the anatomical location of the ectopic focus - the mechanism of development of disorders is not taken into account;
- according to the mechanism of violation of automaticity, conductivity or excitability - in most cases there is a violation of all functions at once;
- by rhythm frequency - the algorithm for determining the type begins with the diagnosis of normo-, tachy- and bradyarrhythmia, but it requires further clarification using electrocardiographic (ECG) studies;
- depending on the mechanism of impulse occurrence (in a normal and ectopic focus) - separate identification of conduction disorders and combined disorders.
Parasystole is closest to the last option. Let us clarify that we understand the term as additional contractions of the heart muscle in response to impulses coming from the “paracenter” located in any part of the heart.
Symptoms
Most patients experience the following signs of parasystole:
- frequent heartbeat that occurs for no reason;
- increased fatigue, lack of strength, dizziness, fainting, decreased productivity at work;
- heart pain, accompanied by a feeling of fear;
- cough;
- bradycardic, characterized by a decrease in heart rate.
In addition to the above symptoms, patients with parasystole complain of strong tremors and blows in the chest area, as well as a sinking heart, sudden lapses in rhythm and various interruptions in heart rhythm. The ventricular type of the disease can be asymptomatic, showing up on an ECG completely by accident.
Causes
Parasystole is caused by cardiac and extracardiac causes. There is also an idiopathic form of the disease, in which no cause is found.
Cardiac causes include:
- Myocardial ischemia,
- Acute coronary insufficiency,
- Myocarditis of various etiologies,
- Cardiomyopathy,
- Cardiosclerosis,
- Chronic heart failure,
- Heart defects.
Other causes: hormonal imbalance, hypothyroidism or hyperthyroidism, anemia, water and electrolyte disorders in the body, hyperglycemia, pathology of the autonomic nervous system, neuroses, drug abuse.
Cardiomyocytes, unlike other cells of a living organism, automatically produce impulses that arise in the sinus node. Under the influence of pathological factors, a parasystolic center can form in any part of the heart, causing premature contractions, extrasystoles and even atrial fibrillation.
In athletes and healthy people, the cause of parasystole is hypertonicity of the vagus nerve. The myocardium cannot completely relax in diastole, the sinus node weakens, and the parasystolic focus becomes active.
Parasystole and extrasystole: what are the differences?
In the presence of double rhythm formation, the patient may be misdiagnosed as extrasystole. The resulting treatment will be ineffective, although in some cases the symptoms of arrhythmia may be alleviated. Despite the fact that these two diseases are types of the same pathology, they require different approaches to therapy.
The difference between extrasystole and parasystole is that in the first case, the occurrence of additional impulses occurs in one zone, and therefore there is a stable interval between the extrasystole and the normal heart rhythm. With parasystole, there may be two or more sources of unplanned impulses, which leads to instability of the intervals between them.
Types of parasystoles
Depending on the location of the source of the second rhythm, the following types are distinguished:
You can also read: ECG signs of extrasystole
- ventricular parasystole;
- atrial;
- from the atrioventricular node;
- polytopic (from different places).
In addition, in relation to the normal contraction, extrasystole can be:
- early and late;
- single, group and allorhythmic (constant rhythmic alternation).
According to the frequency of the ectopic rhythm:
- rare (up to 10 per minute);
- medium (10–30);
- frequent (more than 30).
There are temporary and permanent forms. The type of parasystole can be clarified using the ECG picture.
A serious type of parasystole is atrial fibrillation in the form of atrial flutter or fibrillation. With this pathology, there are either many foci of excitation, or the process forms a vicious circle.
Modern diagnostic methods
Identification of the disease is based on the patient’s complaints, physical examination data and medical history. Often, parasystole is detected by a doctor when examining the patient’s pulse, when an irregular and rapid heartbeat is noted. To make a final diagnosis in this case, a number of instrumental and laboratory studies are necessary:
- Electrocardiography. This is the main technique used to identify this deviation. Signs of parasystole on the ECG appear most accurately. During the procedure, the specialist is able to identify the presence of two rhythms, independent of each other, the appearance of confluent contractions, and disturbances of sinus rhythm.
- Ultrasound of the heart, which allows you to see the process of contraction of the heart muscle on the monitor.
- Laboratory diagnostics, which involves conducting clinical studies of urine and blood, studying the hormonal profile of the body.
- MRI, which can show a three-dimensional image of the heart in several planes, allowing one to assess the degree of pathology.
- Bicycle ergometry is a load using an exercise bike, which is carried out using an ECG machine. Allows you to identify ischemic disease and insufficient blood circulation, against the background of which parasystole may occur.
- Holter monitoring allows you to accurately determine the location of the focus of parasystole and its type.
- Electrophysical research. It involves inserting a thin probe into the heart through the femoral vein. This diagnostic technique is recognized as one of the most informative, allowing not only to identify the presence of a paracentre, but also to determine its exact location. Most often, the procedure is performed for ventricular parasystole.
Diagnostic methods
As with any type of contraction rhythm disorder, ECG diagnosis is the most reliable. Signs of parasystole look like this:
- between anomalous complexes the distances are multiple;
- the interval from the ventricular complex to the extraordinary one is different;
- per minute parasystoles can be up to 60;
- when two complexes coincide, confluent complexes are formed.
Parasystoles are not always visible during normal examination; in such cases, Holter monitoring is indicated. Additionally, a biochemical examination is prescribed to determine the level of cholesterol, blood sugar, potassium, magnesium, and thyroid hormones.
Ultrasound of the heart, MRI or electrophysiological study helps to clarify the origin of the arrhythmia. To identify the latent form of parasystole, stress tests are used - treadmill, bicycle erogometer, pharmacological tests.
Watch the video about the Holter monitoring method and the results:
Features of treatment
Depending on the complexity of the course, parasystole can be treated with non-drug, medicinal or surgical methods. The first option assumes:
- complete cessation of alcohol and tobacco;
- a diet that involves eating foods high in fiber and avoiding hot and spicy foods;
- correct sleep mode.
Drug treatment involves the following methods:
- taking antiarrhythmic drugs that help stabilize the heart rhythm;
- metabolic therapy aimed at improving metabolic processes in tissues;
- Patients with nervous disorders are prescribed beta-blockers, which prevent the body from producing stress hormones.
If the above methods are ineffective, surgical treatment is performed. Its essence lies in the fact that a thin tube is brought to the heart through the vessels of the thigh, through which a radiofrequency pulse is delivered, which helps remove the parasystolic focus.
With timely and correct treatment of the disease, the prognosis for recovery is usually favorable. In most cases, it is possible to do without surgery.
Treatment
Since in most cases intermittent parasystole does not manifest itself in any way, many people do not receive treatment.
If parasystole is detected during the examination, you should contact a cardiologist. This is especially necessary if parasystole is manifested by symptoms (sensation of one’s own heartbeat and arrhythmic contraction of the heart). It is worth remembering that the irregular rhythm of the heart does not allow it to adequately relax between contractions. The heart suffers especially with the development of severe tachycardia. In this case, the time of diastole, during which the coronary vessels feeding the heart itself are filled with blood, is significantly reduced.
At the first stage, under the supervision of a specialist, antiarrhythmic drugs may be recommended (which ones are determined by the cardiologist in each specific case).
But if a constant parasystole persists, then it is worth remembering that the cause of this arrhythmia is primarily a structural restructuring of the myocardium. Drug treatment will not change the structure of the tissue. Therefore, ablation of the ectopic focus is often the method of choice for parasystole. This minimally invasive procedure is performed in high-tech centers. Using a special device, the angiosurgeon penetrates the heart and deactivates a pre-calculated source of ectopic excitation.
In emergency cases of the development of severe tachycardia in a patient with a confirmed diagnosis of parasystole, it is worth remembering that vagal maneuvers (stimulation of the vagus nerve to reduce heart rate) may not work, because innervation of the heart does not imply parasympathetic innervation of the ectopic focus of excitation. Thus, it will be possible to suppress only those impulses that originate from the SA node (see above the study of confirming parasystole using “vagal cardiac arrest”). If tachycardia is provided by impulses from the ectopic excitation center, then it will persist.
Possible complications of parasystole
The consequences of this disease can negatively affect the functioning of the heart:
- Ventricular fibrillation, characterized by frequent and irregular activity. This rhythm disturbance can be fatal.
- Heart failure. Such disturbances in the contractility of the heart muscle develop in the case of a long-term course of the disease.
Parasystole: treatment
Parasystole is a disorder that can cause serious problems and must be treated. To eliminate the problem, complex therapy is necessary. To restore heart function, it is necessary to eliminate the underlying cause of the arrhythmia.
The patient, first of all, is recommended to stop drinking alcohol and tobacco products. It is important to have a balanced diet.
You should eat more foods containing fiber and avoid junk food. Tea and coffee should be limited, or better yet, such drinks should be completely abandoned.
The patient should eat regularly and often, at least five times a day, eating small portions.
You should avoid overwork and excessive stress, sleep at least eight hours a day.
Medications are also prescribed. To normalize heart rhythm, it is recommended to use:
- Medicines to improve metabolic processes in the body.
- Preparations containing omega 3 polyunsaturated fatty acids.
- Beta blockers, which reduce the effect of adrenaline and norepinephrine on the heart.
- Antiarrhythmic drugs. They allow you to avoid any kind of rhythm that differs from normal.
In some cases, surgical procedures are resorted to. Such therapy is necessary if the patient does not tolerate attacks well and in the absence of effect from medications. The procedure is eliminated using radiofrequency ablation.
Preventive measures
To prevent the development of parasystole, you must follow the following medical recommendations:
- Maintain a sleep schedule.
- Eliminate stress from everyday life. The patient may be prescribed sedative decoctions and other folk remedies.
- Quit smoking completely.
- Follow a diet and control your body weight.
- Exercise regularly.
- Patients whose development of parasystole was provoked by another disease need to actively treat this disease.
Parasystole is a deviation in the functioning of the heart associated with a change in rhythm. Seemingly harmless, over time it can cause associated pathologies, which creates a risk of death. Therefore, if any symptoms of the disease are detected, the patient should immediately consult a doctor.
Signs of development
Many patients suffering from parasystole notice the presence of:
- Feelings that the heart is turning over or freezing, making sharp shocks. Contractions become more frequent from time to time.
- Low performance, fatigue, dizziness.
- Painful sensations in the heart area, loss of consciousness against the background of rapid heartbeat.
In some cases, parasystole has no manifestations. In such cases, the diagnosis is made accidentally during an electrocardiography procedure.
Also read: Sinus tachyarrhythmia: what is it, normal or pathology
Extrasystole on ECG
Extrasystole is a heart rhythm disturbance caused by premature contractions (extrasystoles) of the entire heart muscle or its parts. With an extraordinary contraction, the heart noticeably recedes into the chest, causing anxiety and lack of air. A decrease in blood volume during cardiac output can lead to disturbances in cerebral and coronary blood supply and provoke the development of transient cerebral circulatory pathologies (loss of consciousness, paresis) and angina pectoris. There is a high probability of severe forms of arrhythmia leading to sudden death. Extrasystole is diagnosed during an ECG.
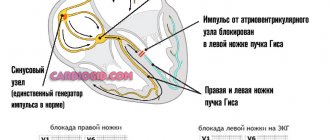
Keys to decryption
To correctly decipher a cardiogram, you need to know the basic principles of the functioning of the heart muscle. Electrical impulses come from the sinoatrial node, located on the wall of the right atrium. Having passed the muscles of this part of the heart, the signal moves to the atrioventricular node and the His bundle. Through the legs of the bundle, excitation passes through the ventricles, causing contraction of all parts of the heart. This is sinus rhythm - a standard, normal pattern of excitation of the heart muscle.
The electrical signals of the heart obtained during electrocardiography are translated into graphic data and reflected on a special tape. The process of work of the heart muscle looks like a curve with heterogeneous teeth reflecting excitation:
- P – atria;
- Q, R, S – ventricles (considered in combination).
Parasystole (confluent contractions)
June 10, 2009
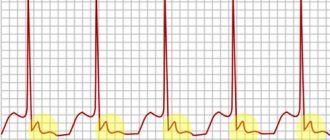
During parasystole, there are confluent contractions - these are combined complexes formed with the simultaneous occurrence of impulses from the main and ectopic pacemakers. In this case, one part of the myocardium is excited from one source, the other from the second, and a complex having an intermediate form is recorded on the ECG. These confluent contractions are one of the diagnostic signs of parasystole.
M. S. Kushakovsky (1981) distinguishes bradycardic and tachycardic forms of parasystole. In addition, atrial, atrioventricular and ventricular parasystole are distinguished. The bradycardic form, according to clinical and electrocardiographic signs, has much in common with extrasystole, and tachycardic forms - with non-paroxysmal or paroxysmal tachycardia.
In this regard, the following classification of parasystole seems appropriate:
- according to clinical manifestations - parasystolic extrasystole, parasystolic paroxysmal tachycardia, parasystolic non-paroxysmal tachycardia, parasystolic accelerated ectopic rhythm;
- according to the localization of the ectopic focus - atrial, atrioventricular, ventricular, combined.
The most common type is ventricular parasystole.
A typical example of parasystolic ventricular extrasystole is the ECG shown in the figure of a 72-year-old patient with a diagnosis of coronary heart disease, post-infarction cardiosclerosis. In the figure you can see right ventricular extrasystoles with a changing extrasystolic interval. Some extrasystoles appear after the next P wave. The distance between extrasystoles in milliseconds is indicated under the ECG. The interectopic spaces are equal and multiple, the 4th ventricular complex is confluent, as indicated by its shape, which has signs of both sinus and ectopic complexes.
Less commonly, parasystole manifests itself in the form of accelerated ectopic rhythms, non-paroxysmal or paroxysmal tachycardia. Sometimes a double, or combined, parasystole with two ectopic foci is observed.
An example of such arrhythmia is the ECG of a 67-year-old patient diagnosed with coronary heart disease, acute posterior phrenic myocardial infarction. Arrhythmia developed after electrical defibrillation performed for ventricular fibrillation. Both parasystolic centers were localized in the ventricles. On the upper segment of the curve there is a sinus rhythm of 76 per minute, polytopic ventricular extrasystoles.
The shape of extrasystolic complexes is variable, apparently due to the fact that some of them are confluent contractions (for example, the 3rd complex on the right). On the middle curve one can see three types of ventricular complexes: two types correspond to various types of ectopic ventricular contractions, the third corresponds in shape to sinus ones. In the interectopic intervals of complexes of the same type, it is possible to establish common divisors indicated above and below the curve, which indicates the parasystolic origin of these complexes. In this segment of the curve, only one sinus complex (6th) can be seen, followed by an atrial extrasystole and a drain contraction. The lower segment of the ECG showed non-paroxysmal ventricular tachycardia with a frequency of 115 per minute. The shape of the ventricular complexes corresponds to the shape of the complexes of one of the parasystolic rhythms, and the interectopic intervals have a common divisor. Thus, the patient had double ventricular parasystole and non-paroxysmal tachycardia. The arrhythmia lasted for several hours and then went away on its own.
Often, parasystolic arrhythmias have a very long and persistent course, persist for many years and are difficult to treat with antiarrhythmic drugs.
“Practical electrocardiography”, V.L. Doshchitsin
Read further:
Sick sinus syndrome
Combined arrhythmias are understood as combined disorders of impulse formation and conduction. Among them, several main clinical and electrocardiographic syndromes are distinguished, in particular sick sinus syndrome, escape contractions and rhythms, atrioventricular dissociation, reciprocal contractions and rhythms, premature ventricular excitation syndromes and parasystolic arrhythmias. This term refers to the weakening of the function of the sinus node as a pacemaker. The main symptoms of this syndrome...
Sick sinus syndrome (attacks of asystole)
The most dangerous manifestation of sick sinus syndrome is attacks of cardiac asystole due to arrest of the sinus node and other sources of rhythm. Such attacks are called sinoatrial syncope. The figure shows an ECG of patient R., 72 years old, with a diagnosis of coronary heart disease, atherosclerotic cardiosclerosis, stage II hypertension, sick sinus syndrome. The patient experienced periods of sharp slowdown in rhythm due to...
Elusive contractions and rhythms
Escaped, or jumping out, are rhythms that occur when the formation or conduction of impulses from the main source of the rhythm is disrupted, when more or less long pauses appear. Escaping contractions, unlike extrasystoles, do not appear prematurely, but are delayed in relation to the complexes of the main rhythm. The so-called slip interval (the distance between the next and ectopic contractions) is equal to or greater than the distance between the complexes...
Atrioventricular dissociation
Atrioventricular dissociation is the uncoordinated activity of the atria and ventricles, not associated with complete transverse block, but resulting from the fact that the ventricles are excited by ectopic impulses, more frequent than sinus impulses, and the atria are activated by another rhythm source (usually the sinus node). Just like escaped contractions, atrioventricular dissociation is not an independent type of arrhythmia, but is associated with other rhythm disturbances...
Reciprocal contractions and rhythms
Reciprocal, recurrent, or echo contractions are explained by the fact that the atria or ventricles are excited repeatedly by the same impulse. This is a particular manifestation of the phenomenon of re-entry of excitation. A necessary condition for the occurrence of reciprocal arrhythmias is the functioning of two channels in the atrioventricular junction, conducting impulses at different speeds and in opposite directions. Reciprocal arrhythmias also occur during the functioning of additional pathways in...