Rating: 5/5 (1)
What is CTG in pregnant women? Cardiotocography (CTG) is a method of functional study of the state of the fetus in the womb of a pregnant woman, which is based on a sequential recording of the child’s heart rate and its changes in accordance with the contractile movements of the uterus, the influence of environmental factors and the activity of the baby himself.
This recording of the heartbeat is carried out within 15 minutes and can be carried out both in a calm state of a woman outside the labor process, and during labor and childbirth. This feature makes CTG quite an effective and useful method for resolving the issue of labor tactics.
Why is fetal CTG performed in pregnant women?
What does CTG show? First of all, this type of study is carried out to obtain information about the fetal heart rate , the regularity of its cardiac activity, as well as active movements.
In addition, the information content of CTG is very important in determining the frequency of contractions of the smooth muscle cells of the uterus and the child’s reaction to these contractions.
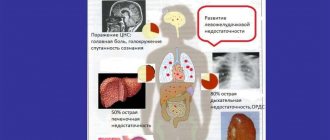
Cardiotocography is an effective research method for excluding or timely identifying pathological conditions of the mother and child that pose a threat to the course of pregnancy and to the future health of the newborn baby, such as hypoxia, intrauterine infection of the fetus, polyhydramnios, oligohydramnios, congenital abnormal development of the cardiovascular system, fetoplacental insufficiency and threat of labor starting earlier than planned.
Preparing for CTG
The procedure is carried out in a antenatal clinic. No special preparation required. It is enough to follow simple rules:
- Get enough sleep the night before the procedure. The mother's condition affects the motor activity of the fetus.
- Have a light snack before leaving the house. You need to take into account the road to the clinic so as not to be too full or, conversely, hungry.
- Upon arrival, you need to rest a little and sit to restore your heart rate.
- The procedure takes about 30 minutes, so the pregnant woman needs to worry about going to the toilet in advance.
- Smoking mothers need to abstain from the bad habit for 2 hours.
No other additional preparation measures are required.
Are there any contraindications?
The technique is non-invasive and does not affect the condition of the fetus or uterus. The harm of CTG can only appear when performing stressful functional tests. But at present, the level of technology and the qualifications of doctors makes it possible to determine fetal hypoxia and severe conditions without the use of special stimuli.
Main indications for CTG
- A woman with Rh-negative blood is at risk of developing hemolytic disease of the newborn.
- A history of premature labor, miscarriages and abortions.
- Feelings of decreased fetal movements in the pregnant woman herself.
- Complications during pregnancy (toxicosis, multiple fetuses, polyhydramnios, oligohydramnios, fever or low-grade temperature in the pregnant woman, malpresentation of the baby, post-term pregnancy).
- Disturbances in the child that were previously found by ultrasound (developmental delay, disturbances in the amniotic fluid, decreased activity, pathological changes in blood circulation in the placenta, the child’s size is too large or small, inappropriate for the month of pregnancy).
- Endocrine and systemic diseases in pregnant women (diabetes of the first and second types, diseases of the cardiovascular system, anemic manifestations).
This method of studying the condition of a child during his intrauterine life is safe, since the sensor produces an ultrasonic wave of weak strength that does not cause a negative effect on the baby .
In what cases is it done?
This method is used for early diagnosis of pathological conditions of the fetus. Starting from 28-30 weeks of pregnancy, the doctor at the antenatal clinic may prescribe you to monitor the fetal heartbeat using CTG.
1. CTG is recorded once, if nothing worries you and the doctor does not consider it necessary to record it.
2. With a pathological version of the recording. If the heartbeat is recorded with signs of pathology, the study will most likely have to be repeated.
3. In case of unfavorable course of previous pregnancies. If a woman’s obstetric history has dismal outcomes, then during the current pregnancy, even if it proceeds without any peculiarities, it will be necessary to record CTG more than once. For example: if a child died in the womb in the past, anomalies in the development of internal organs, genetic and chromosomal diseases.
4. In case of disturbances in the behavior of the unborn child. Every expectant mother feels and knows how her child behaves in the womb. Some children are very active and have very short periods of sleep. It happens that the child sleeps most of the day and is active at night. Changes in rhythms may be a sign that the fetus is experiencing discomfort.
5. When the mother herself is ill. For example, with influenza or ARVI, with acute conditions that lead to a deterioration in general well-being.
6. After the unborn child’s conditions have been suffered and treated. A CTG should be recorded for several weeks after inpatient or outpatient treatment.
7. When a woman has gestosis during pregnancy. This disease entails disturbances in the blood supply to the fetus, which can lead to delayed development of the unborn baby.
8. If a woman has a chronic infection.
9. Women who continue to smoke and drink alcohol during pregnancy. This group can also include women with drug addiction, including those in remission.
10. Women with chronic diseases of internal organs. For example, diabetes mellitus, arterial hypertension, heart defects, obesity, liver and kidney diseases.
11. Childbirth is most often carried out under heartbeat monitoring.
12. In case of post-term pregnancy.
At what stage is fetal CTG performed?
The use of cardiotocography can begin from approximately the 29th week of pregnancy, but high-quality and informative recording of the above parameters characterizing the condition of the child in the womb is possible only from the 32nd week of pregnancy.
This is due to the development of periodically alternating cycles in the baby, when he is active or calm in motor terms. The baby is most active in the period from 9 to 14 pm, as well as from 19 to 24 pm.
How to prepare for CTG during pregnancy? CTG is contraindicated after meals, since elevated blood glucose levels can significantly affect the fetus, increasing its movements and reaction to external environmental stimuli.
Is CTG harmful to the fetus during pregnancy?
CTG is a completely safe procedure that has no contraindications. Therefore, if an expectant mother is concerned about the question of whether CTG is harmful during pregnancy, the answer in this case is always categorical - not harmful. If necessary, examinations can be carried out over a fairly long period of time, even daily. Moreover, the examination is very, very informative, it allows you to identify possible threats to pregnancy and the fetus in a timely manner, and take the necessary actions in a timely manner. But, in any case, the obtained tests should be considered only in the context of the general course of pregnancy and in mutual connection with the results of other examination methods, in particular ultrasound and doppleometry.
Especially for beremennost.net – Tatyana Argamakova
How to do fetal CTG during pregnancy
Cardiotocography is carried out using a specialized sensor , which has an ultrasonic effect and is based on the Doppler effect.
This device is tightly secured to the front of the pregnant woman's abdomen, where the baby's heart sounds are most clearly heard. Such an area can be preliminarily determined without any problems using an obstetric stethoscope.
The sensor, producing a signal in the form of an ultrasonic wave, directs it towards the baby's heart in the womb. The wave is reflected from the heart, which is perceived again by the same sensor in the end. The information received is converted into fetal heart rate values per minute . The research results are reproduced sound, light and graphically on tape.
If the pregnancy is normal, CTG is performed no more than once a week. In case of a complicated pregnancy, but with good results from previous methods of fetal examination, this procedure is performed with a pause of an average of 6 days.
If hypoxia of the child in the womb, CTG is indicated for daily or every other day for constant dynamic monitoring of the child’s condition and timely adoption of measures for emergency childbirth.
How do you prepare for the examination?
Cardiotocography refers to research methods that allow one to assess the general condition of the child in the womb in a short time. Diagnosis of this type is carried out for the first time from approximately 28 weeks of pregnancy. At later stages, the procedure is often prescribed to determine false or true contractions. How to determine contractions using CTG can only be answered with accuracy by an experienced specialist. Mommy will not be able to decipher the obtained indicators on her own. Cardiotocography does not require any special preparation. A woman should only listen to some simple advice:
- Before starting the procedure, it is recommended to visit the toilet.
- You should not undergo the procedure on an empty stomach. Have a small snack.
- During the diagnosis, try to sit comfortably; you can use a pillow.
- Try not to be nervous, your breathing should be even.
To check the fetal behavior at rest and activity, the doctor may ask you to hold your breath for a few seconds.
Sometimes a woman is asked to perform basic physical exercises, for example, on a fitball. The total duration of the session is usually half an hour.
Interpretation of fetal CTG results during pregnancy
The results of the cardiotocography analysis are assessed by a specialist based on a number of indicators , which include basal rhythm, variability, acceleration, deceleration and, finally, the activity of the baby’s movements in the womb. All this is depicted at the end of the manipulation on paper in the form of graphs of various shapes.
How to decipher CTG? You should not try to decipher your CTG yourself, since you, not being a doctor, will make a mistake when deciphering the fetal cardiotocography in calculating points based on the results, which, of course, can harm the child.
The basal rate is the average value of the fetal heart rate. Normally, the basal rhythm reaches from 110 to 160 heart beats per minute when the baby and pregnant woman are calm. When the child moves, the frequency of contractions increases to values ranging from 140 to 190 beats.
All normal values of the basal rhythm indicate the absence of a hypoxic state in the baby’s body. And the increase, as well as the decrease, are a clear sign of fetal hypoxia, which, first of all, is detrimental to its nervous system, although it is not yet fully developed.
Variability (in other words, amplitude) is a change in the value of the heart rate frequency and its amplitude relative to the obtained values of the baby’s basal heart rate. Outside of pathology, the heart rate of a child in the womb should not be constantly the same and monotonous, which is clearly visualized by the continuous change of numerical values on the monitor during CTG. Normal changes in the relevant parameters should range from 5 to 25 beats per minute.
An increase in amplitude may indicate fetal hypoxia or entanglement with the umbilical cord , which is undoubtedly a pathology. Reduced amplitude values may be normal if the baby is in a calm state at the time of CTG. In order to “wake up” the baby, the mother can simply eat some sweetness.
Acceleration (increase) - an increase in the number of heart beats in comparison with the level of the basal heart rate. The amount of acceleration is expressed on the cardiotocogram in the form of teeth; normally it is at least 2-3 times within 15 minutes . It is permissible to increase the number of repetitions up to 4 times per half hour. What is pathological is their complete absence during the specified time period.
Deceleration (decrease) - a decrease in heart rate values in comparison with the level of basal heart rate. The magnitude of deceleration is expressed in the form of dips (“negative” teeth). Normally, such manifestations should not be present or should be insignificant in depth, duration and occurrence.
The deterioration of the baby's condition in the womb can be confirmed by the occurrence of decelerations after 20 minutes of examination. Also a bad result is their repetition and different appearance throughout the entire chart. All this may indicate decompensated fetal stress .
In general, the decoding of the norm for fetal CTG results is as follows:
- Basal rate – 120-159 per minute at rest.
- Variability from 10 to 25 beats per minute.
- 2 or more accelerations within 10 minutes.
- No decelerations.
Pathological CTG looks like this:
- Basal rhythm – less than 90 and more than 180 per minute.
- Variability less than 5 beats per minute.
- Absence or small number of accelerations.
- The presence of different types of decelerations.
CTG of uterine tone and fetal heart rate: 6, 7, 8, 9 points
Update: December 2018
When the expectant mother feels the movements of the fetus, it is wonderful: the pregnant woman knows that the baby is doing well. But it is impossible to assess the possible onset of intrauterine suffering in a child based on motor activity.
In order to detect and prevent problems in time, it is necessary to use ultrasound research methods (CTG, ultrasound and Doppler). Fetal cardiotocography (CTG) is a simple and accessible method for assessing a baby’s heartbeat, with which you can notice the initial signs of oxygen deficiency.
In addition, it is possible to identify changes in the muscle tone of a woman’s uterus, which can cause premature birth. CTG is a technique for recording uterine tone and heart rate on special calibration paper. That is, there are 2 graphs; some devices can record the child’s physical activity:
- heartbeats recorded by ultrasound
- uterine tone determined by a strain gauge
Is cardiotocography harmful to the fetus?
This is an absolutely safe procedure for both the fetus and the woman, does not cause discomfort and can be performed according to indications even daily (in case of fetal hypoxia), to assess the effectiveness of the therapy and make a decision on emergency delivery.
Indications for CTG
The most informative method is in the last trimester of pregnancy.
It is after 30 weeks that biori are fully established and a specific reflex is formed (increased heart rate with fetal movements), by which one can judge the full support and normal intrauterine development of the child (see calculator for calculating the gestational age). The main indications for CTG during pregnancy include:
| Complicated pregnancy:
|
Diseases in the fetus identified by ultrasound examination:
| Serious illnesses in a pregnant woman:
|
In the cases listed in the table, CTG should be performed more often, up to daily. The condition of the fetus and the effectiveness of labor can also be assessed by cardiotocography in real time.
Research methodology
Most often, the examination is carried out at 32 - 34 weeks of pregnancy. CTG is performed in the pregnant woman's supine position with a small bolster under her right side (the optimal position is a slight turn to the left side). It is possible to perform CTG in a position lying on your side, or sitting, leaning back in a chair.
- First, the doctor uses a stethoscope to find the point on the abdomen where the baby's heart can best be heard.
- An ultrasound probe is placed on this site, and a probe is placed on the fundus of the uterus to assess muscle tone.
- To notice the baby's movements, the woman is given a special device with a button that she will press when she feels intrauterine movements.
- Recording time is 40-60 minutes.
When CTG is done, the study is carried out using sensors with a frequency of ultrasonic waves of 1.5-2 MHz, which is absolutely safe for the fetus even with prolonged exposure. Any modern device has the ability to assess the vital functions of two fetuses at the same time, which is used in women with twins.
Types of devices
Medical facilities have various options for assessing your baby's heartbeat. Most often, the doctor simply listens to the baby’s heart rhythm using an obstetric stethoscope, but if there is any doubt (or if there is evidence), it is necessary to use a special device. What types of CTG devices are there?
- CTG without automatic analysis
These outdated devices are generally quite rare in modern hospitals, but they can still be found in remote corners of our country. The main inconvenience of these devices is that the doctor must independently evaluate the fetal heartbeat graph. If the doctor has experience and masters this technique, then the effectiveness of these devices is no lower than that of new CTG devices.
- CTG with computer analysis
Modern cardiotocographs not only record the graph, but also independently process the data. The doctor only needs to read the finished result and decide on the need for treatment. This version of CTG is used most often in medicine.
The modern mobile era offers an excellent option for monitoring the baby using a special sensor attached to the skin of the abdomen and a smartphone connected to the Internet. Information about the fetal heartbeat in real time is transmitted to the web portal, processed and provided in the form of a ready-made report to the doctor. Unfortunately, online CTG is still rarely used.
Interpretation of CTG: pathology or normal
The table below shows the assessment of the fetal condition according to CTG, proposed by Dr. Savelyeva, which takes into account all indicators:
- basal rhythm - average fetal heart rate
- variability - change in the frequency and amplitude of the heart rhythm (deviation from the basal rhythm frequency
- acceleration - acceleration of the heart rate from the basal rate by more than 15 beats, lasting over 10-15 seconds.
- deceleration - a decrease in the fetal heart rate from the basal rate by more than 15 beats, lasting more than 10 seconds.
- fetal motor activity
A bad CTG during pregnancy will occur if the following indicators are detected:
- prolonged increase in fetal heart rate (tachycardia) more than 160 beats per minute
- decrease in baby's heart rate to less than 110 beats per minute
- increased rhythm variability with an amplitude of more than 25 beats per minute
- reduction in variability below 5 beats per minute
- sinusoidal rhythm, in which a uniform and monotonous heartbeat occurs without any fluctuations or changes in variability
- appearance of decelerations
| 2 points | 1 point | 0 points | |
| Basal rhythm , beats/min | 110-160 | 100-110 or 160-170 | less than 100 or more than 170 |
| variability (number of deviations from the basal rhythm per minute) | more than 6 | 3-6 | less than 3 |
| Amplitude of oscillations (deviations from the basal rhythm) | 10-25 | 5-9 or more than 25 | less than 5 or sinusoidal rhythm |
| Accelerations | regular, 2 or more | intermittent or absent | none |
| Decelerations | absent, appear simultaneously with uterine contractions | rare and short | pronounced and long-lasting |
After counting the points, the condition of the fetus is assessed:
- 5 or less - state of fetal hypoxia, the child experiences oxygen starvation
- 6, 7 points - the first signs of fetal hypoxia
- 8, 9, 10 points - no hypoxia, the child feels well
Motor activity is not taken into account in Savelyeva’s method, but you should know that increased, excessive fetal mobility or, conversely, its absence, indicates the presence of oxygen starvation in the fetus.
However, even when deviations are detected, this does not always indicate serious problems in the child. It is necessary to take into account not only CTG during pregnancy, the interpretation of which will indicate the presence of hypoxia in the baby, but also the duration of pregnancy, the presence of complications in the pregnant woman, data from ultrasound examinations and Doppler measurements.
Fisher ten scale
The results of cardiotocography are assessed by specialists on a ten-point Fisher scale, which is based on assigning points from 0 to 2 to each of the above indicators. These scores are summed up, and a general conclusion is made about the information content of CTG and the presence of pathological changes in the fetus. so-called “fetal health indicator” (FSI) is assessed.
- If the total CTG from 1 to 5 , then the baby’s condition in the womb is poor, he is experiencing hypoxia (lack of air).
- What does it mean if the total CTG score is 6-7 ? The child shows initial signs of developing oxygen starvation.
- What does it mean if the sum of CTG points is from 8 to 10 ? This indicates the normal and good condition of the baby.
With a PSP of 1-5 points, immediate delivery is indicated; with a PSP of 6-7 points, repeat CTG is indicated; with a PSP of 8-10 points, continued periodic monitoring of the pregnant woman and fetus using this research method.
Norm of the result obtained
Upon completion of the necessary studies, clear boundaries of the norm were established, which are worth familiarizing yourself with, since medical institutions do not always give out deciphered data, and knowledge of at least an approximate CTG result is extremely necessary for women who are worried about the condition of their child.
If the patient can visit a specialist who can decipher CTG readings, it is better to take advantage of this chance: self-analysis of the test often becomes the reason for an erroneous conclusion
When independently analyzing the obtained indicators, you need to focus on the digital values of the norm:
- Basal rhythm: 110–160 beats per minute in a calm state for both the child and the mother. If the baby is active, the indicator can increase to 190.
- Accelerations: the corresponding “teeth” must appear at least twice in 15 minutes. The complete absence of accelerations indicates pathology.
- Decelerations: with proper development of the fetus, the indicator in question should not make itself known. The relative norm is considered to be insignificant depth and rare manifestation of decelerations on the cardiotocogram.
- Variability: ranges from 5 to 25 beats per minute.
- Fetal health indicator (FSI): up to one.
- Tocogram (uterine activity): a good indicator does not exceed 30 seconds.
What does it mean if the doctor does not approve the CTG results?
The fact that the doctor did not like the results of cardiotocography does not mean a final determination of fetal hypoxia and pathology in principle. There are cases when young doctors without sufficient work experience incorrectly interpreted the information contained in the received graph, although everything was completely normal for the baby and his mother.
Therefore, you should not rush and immediately panic when you get a bad result. But you shouldn’t relax, as this may actually indicate a real pathology that requires immediate treatment and action on the part of medical professionals.
Most likely, if the results show alarming deviations from the norm, the doctor will ask you to go to the maternity hospital , where they will conduct regular CTG and be able to quickly react in a dangerous situation.
Dates
Cardiotocography is indicated from 32 weeks of gestation. It is also possible to conduct CTG earlier, from 28 weeks, and in shorter periods of pregnancy CTG is not performed at all due to the impossibility of correct interpretation of the results. The indicated pregnancy periods for CTG are based on the fact that only by the 28th week does the fetal heart begin to be regulated by the autonomic nervous system, and its heart rate responds to the movements it makes. In addition, by the 32nd week of gestation, the cyclicity of sleep and wakefulness of the unborn child is formed.
If the pregnancy proceeds without complications, then CTG is performed once every 10 days; in case of complications, but “good” results of previous CTG, the study is repeated after 5-7 days. In the case of intrauterine hypoxia, daily or every other day CTG is indicated (either until the fetal condition normalizes, or until the issue of the need for delivery is decided).
During labor (without deviations from the norm), CTG is performed every 3 hours. In case of complications - more often, as determined by the doctor. It is advisable to conduct the period of contractions under the constant monitoring of CTG.
How contractions appear on CTG
This study will definitely indicate the presence of contractions , since normally the uterus should respond to the active motor activity of the baby with its spasms. In addition, the uterus has the ability to spontaneously contract. On CTG, in response to contractions, a decrease in the number of baby’s heartbeats and deceleration will be visible, which occurs in rare cases.
The second curve (hysterogram) reflects the increase in the force of contraction of the myometrium (muscular layer of the uterus) during contractions. The higher it is, the stronger the contractions. Some women in labor do not feel contractions; CTG helps determine their strength and frequency.
How to determine real contractions using CTG?
The readings from the device help the specialist see whether the woman in labor has uterine contractions (indicating that contractions are beginning), what is the interval between them and their strength. The fluctuations are visible in numbers on a special monitor and a curved line displayed by the device. So, let's find out how contractions are determined by CTG:
- Before the procedure, the initial designations of the woman are entered.
- The specialist records the interval during which there are no contractions of the reproductive organ and the tone of the uterus is not increased.
- To see the contractions, the woman in labor is asked to lie on her side.
- The sensor of the device is attached in the navel area. It is here that the fetal heartbeat can be heard most clearly.
- Using another device, contractions of the uterine walls are recorded. An experienced obstetrician can easily distinguish training contractions from real ones. In this case, the scale on the monitor will have characteristic fluctuations.
You might be interested in: Planning and preparing for pregnancy
The woman in labor is asked to press the button as soon as she feels the baby move. This helps the doctor obtain more accurate data during CTG.
If the cervix dilates too slowly during uterine contractions, the pregnant woman is given an antispasmodic. This does not affect the birth process, but helps to relax the muscle fibers, which leads to faster dilation of the cervix.
What is the Fetal Reactivity Index?
This indicator tells the specialist about the state of the fetus’s nervous system reactivity to external influences, which, first of all, affects the state of the cardiovascular system.
The calculation is made in a point system and is further interpreted:
- 0 points means an absolute lack of reactivity in the baby.
- 1 point means severe disturbances in the body's reactivity.
- 2 points mean severe disturbances in the baby’s reactivity.
- 3 points indicate a moderate degree of impairment in reactivity.
- 4 points indicate the initial stage of the pathology of the child’s reactivity.
- 5 points means normal reactivity in the fetus.
The influence of cardiotocogram results on medical tactics
Medical personnel treat the results of the study with all seriousness and responsibility. Each recording of the functional activity of the fetal heart is assessed by a qualified specialist, certified by his signature and seal indicating the date and time of examination of the pregnant woman. The film is glued into her exchange card.
Diagnostics has no contraindications and is a safe research method
For the objectivity of deciphering the final CTG data, there is an evaluation system based on assigning certain points to each indicator:
- 9–12 is considered the norm;
- at 6–8, signs of hypoxia are observed;
- a score of 5 is considered extremely unfavorable.
If deviations from normal results are detected, the condition of the expectant mother requires daily monitoring and appropriate treatment and preventive measures. Marked changes in indicators may indicate a terminal (critical) condition of the fetus requiring emergency delivery.
The fact that the doctor did not like the results of cardiotocography does not mean a final determination of fetal hypoxia and pathology in principle. There are cases when young doctors without sufficient work experience incorrectly interpreted the information contained in the received graph, although everything was completely normal for the baby and his mother.
Therefore, you should not rush and immediately panic when you get a bad result. But you shouldn’t relax, as this may actually indicate a real pathology that requires immediate treatment and action on the part of medical professionals.
Most likely, if the results show alarming deviations from the norm, the doctor will ask you to go to the maternity hospital, where they will conduct regular CTG and be able to quickly react in a dangerous situation.
What is a non-stress test?
This type of study of the condition of the baby in the womb is a test to determine cardiac activity in accordance with the movements of the child.
A good result is a negative non-stress test (the presence of 2-3 increases in the number of heart contractions by about 15 beats per minute for 15-20 seconds). In the case of a positive or no result at all, we can conclude that the baby is in a hypoxic state, which, in fact, may be a false phenomenon if at the time of the study the fetus was calm and sleeping. In this case, it is recommended to repeat the non-stress test.
Should I worry if the doctor did not approve the CTG data?
Sometimes patients who have undergone the corresponding procedure receive a rather unpleasant and disturbing report from the doctor, after which they fall into real panic. However, it is worth keeping in mind one very important rule: an alarming result is not always the cause of the presence of any pathologies in the child’s development. The human factor also plays an important role in such situations.
For example, young specialists who have just begun to practice their activities in a particular medical institution, due to the lack of necessary work experience, sometimes incorrectly decipher the information obtained as a result of cardiotocography. In such cases, the chart readings were interpreted incorrectly, although both the expectant mother and the baby were in excellent health.
If the baby was sleeping peacefully at the time of the study and, accordingly, did not show the necessary activity, then the CTG results are also distorted
Some women may simply have an appointment with a doctor who, being in a bad mood, wants to slander in front of people who have nothing to do with his problems. If the patient is confident that the doctor who performed the procedure is biased, she should, without succumbing to nervous stress, undergo CTG again with a more competent doctor.
In any case, you should not worry ahead of time; you need to consult with your doctor and follow all his recommendations regarding additional diagnostic methods that can clarify the current situation. It is worth noting that the results of CTG are significant only when the ultrasound procedure is carried out in parallel with other types of examination: only a comprehensive study of the child’s health will allow an objective picture of the course of pregnancy to be drawn.
Erroneous assessment of CTG results
Errors when interpreting information obtained using cardiotocography are certainly possible. For example, in the case of hypoxia , but despite the fact that the baby’s tissues have already managed to adapt to it, CTG is not able to show this pathological condition. The same can happen if there is a sufficient amount of oxygen in the bloodstream, but the tissues cannot adequately accept and use it, which indicates actual fetal hypoxia.
The presence of errors obliges specialists to evaluate the results of CTG only in conjunction with the results of other studies performed on a pregnant woman, and then make a final diagnosis.
How is the research conducted?
At 28 obstetric weeks, the formation of sympathetic innervation of the heart muscle is completed, leading to an acceleration of its contractions.
The opposing signals from the parasympathetic nervous and autonomic systems to the fetal heart influence heart rate. The cardiotocograph has ultrasound (detecting the movement of the fetal heart valves) and strain gauge (detecting uterine contractions) sensors. They transmit information to the fetal cardiac monitor, which processes the information and displays it on an electronic display and records it on thermal paper using a recording device.
Due to the physiological characteristics of the innervation of the heart muscle of the unborn child, CTG provides the most reliable information in the third trimester
The following parameters have the greatest diagnostic significance:
- Contractions of the uterus - they are considered a physiological norm.
- Basal rate - average heart rate.
- Variability – short-term deviations of the heartbeat from the basal rhythm.
- Spontaneous increase in heart rate - acceleration.
- Temporary slowing of the heartbeat - decelerations.
What does CTG show? First of all, this type of study is carried out to obtain information about the fetal heart rate, the regularity of its cardiac activity, as well as active movements.
In addition, the information content of CTG is very important in determining the frequency of contractions of the smooth muscle cells of the uterus and the child’s reaction to these contractions.
Cardiotocography is an effective research method for excluding or timely identifying pathological conditions of the mother and child that pose a threat to the course of pregnancy and to the future health of the newborn baby, such as hypoxia, intrauterine infection of the fetus, polyhydramnios, oligohydramnios, congenital abnormal development of the cardiovascular system, fetoplacental insufficiency and threat of labor starting earlier than planned.
Video about fetal cardiotocography (CTG)
We invite you to watch a video about fetal CTG. An obstetrician-gynecologist will tell you how and why this examination is carried out, how its results are evaluated, and what are the normal CTG indicators.
Any pregnant woman will sooner or later undergo a CTG procedure; some of the readers have already encountered this study. Therefore, tell us about your impressions of cardiotocography, how its results were deciphered for you, and what this painless manipulation gave you. Don’t forget to leave feedback and ask questions about CTG, the answers to which most concern you or are still unclear.
We recommend reading:
- Colostrum during pregnancy Ultrasound during pregnancy: at what time is it done HCG analysis during pregnancy: decoding Norm of protein in urine during pregnancy
Methods
CTG can be indirect (external) and direct (internal).
The examination is carried out with the woman either on her left side or half-sitting (to prevent compression syndrome of the inferior vena cava). The ultrasound sensor (which records the fetal heart rate) is treated with a special gel to ensure maximum contact with the pregnant woman's skin. The sensor is placed on the anterior abdominal wall in the area of maximum audibility of fetal heartbeats. A strain gauge sensor that records uterine contractions is placed in the area of the right corner of the uterus (it is not lubricated with gel).
The patient is given a special device in her hand, with which she independently notes the baby’s movements. The procedure takes 20-40 minutes, which is due to the frequency of periods of sleep (usually no more than 30 minutes) and wakefulness of the fetus. Registration of the basal rhythm of the fetal heart rate is carried out for at least 20 minutes until 2 movements are recorded lasting at least 15 seconds and causing an acceleration of the heart rate by 15 heartbeats per minute.
Internal cardiotocography is performed only during childbirth and under certain conditions:
- opened amniotic sac and discharge of water;
- the opening of the uterine pharynx is at least 2 cm.
To conduct direct CTG, a special spiral electrode is applied to the skin of the presenting part of the fetus, and uterine contractions are recorded either by inserting an intra-amnial catheter or through the anterior abdominal wall. This study is considered invasive and is not widely used in obstetrics.
When conducting non-stress cardiotocography, the fetal heartbeat is recorded in natural conditions, taking into account fetal movements. If unsatisfactory results of non-stress CTG are obtained, tests (functional tests) are used, which is called stress CTG. These tests include: oxytocin, mammary, acoustic, atropine and others.