General information
Ectopic rhythms are observed in almost 50% of pregnant women. Some rhythm disturbances are recorded in 60% of healthy people aged 40 years during daily monitoring. During pregnancy, the heart rate (HR) increases by 25%, so episodes of sinus tachycardia are not uncommon in the third trimester.
| Doctor's opinion A woman's heart carries 50% more blood to the uterus. By the end of the term, the fetus receives one fifth of the total blood volume, while cardiac output increases by 30-50%. There is an increase in heart rate from 70 to 80-90 beats per minute. At about 30 weeks of pregnancy, cardiac output decreases slightly, but during labor it increases by another 30%. Only 6 weeks after birth, a woman’s prenatal hemodynamic parameters are restored |
Sometimes women feel changes in their pulse, and most often this is a variant of the norm. Against the background of increased function, heart murmurs appear. Persistent diastolic murmurs and arrhythmias indicate heart disease.
Causes
Heart rate during pregnancy increases due to hemodynamic, hormonal, and also autonomic changes:
- An increase in effective circulating blood volume of 30-50% begins at 8 weeks of pregnancy and reaches a peak value by 34 weeks.
- Cardiac output increases by an average of 6.7 L/min in the first trimester and by more than 8.7 L/min in the third trimester. As a result, heart rate increases by 15%.
- An increase in plasma volume causes stretching of the myocytes of the atria, as well as the ventricles, which can lead to early depolarization - early conduction of the signal.
- The myocardium becomes less elastic, cell conductivity slows down due to early activation of ion channels. The large volume of the chambers leads to the appearance of possible “entrances” for re-excitation of cells.
Physiological acceleration of heart rate in the third trimester influences the risk of sinus arrhythmia in pregnant women. It has been proven that estrogen increases the number of adrenergic receptors in the myocardium and adrenergic reactions throughout pregnancy.
A heart rate of more than 100 beats per minute during pregnancy is considered tachycardia . This type of arrhythmia reduces the flow of blood and oxygen to body tissues. The result is ischemia and angina. The type of rapid heartbeat depends on the source of the rhythm:
- Sinus arrhythmia during pregnancy - forms in the sinoatrial node after stress and physical exertion.
- Non-sinus - occurs from the walls of the chambers, it can be ventricular and supraventricular.
Certain types of arrhythmia have different mechanisms during pregnancy:
| Types of arrhythmia | Manifestation mechanism |
| Supraventricular tachycardia | Attacks of pathological acceleration of the pulse with atrial fibrillation (flutter). Usually associated with congenital pathologies and diseases before conception. |
| Atrioventricular nodal tachycardia | The most common type among pregnant women. This type of arrhythmia does not affect the health of the fetus and mother, but causes hemodynamic instability in the nutrition of the placenta. |
| Atrioventricular tachycardia | With a re-entry mechanism, it occurs in women with congenital heart defects and seriously impairs hemodynamics in heart failure due to systolic or diastolic dysfunction. |
| Atrial fibrillation | Rarely occurs without congenital or acquired valvular heart disease. Attacks of atrial fibrillation in pregnant women occur against the background of thyrotoxicosis and can only be relieved with medications (Adenosine, Digoxin, Propranolol). |
| Ventricular tachycardia | Lasting more than 30 seconds is rare and occurs in women who are aware of heart problems. |
The most likely causes of tachycardia during pregnancy are: acute blood loss, anemia, anxiety, asthma, dehydration, ectopic pregnancy, fever, heavy work, heart and lung problems, infections, sepsis, severe injury, side effects of certain medications, and thyroid problems. Sometimes tachycardia is associated with obstetric problems such as amniotic fluid, hemorrhage, placental abruption, or uterine rupture.
Arrhythmia is caused by structural heart diseases :
- cyanotic diseases (tetralogy of Fallot);
- valve diseases (bicuspid aortic valve);
- atrioventricular septal defects.
Attacks are caused by acquired structural changes in the heart: valve pathologies after rheumatic fever or endocarditis, cardiomyopathy. Arrhythmia, not caused by structural pathologies, is usually associated with degeneration of the conduction system, as well as metabolic disorders.
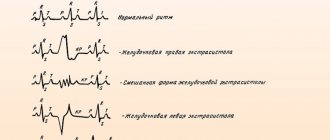
Extrasystole
It is extrasystoles that are more often observed during pregnancy. In most cases, they are not grouped, but single, and occur in the third trimester, when the diaphragm rises higher due to the growing uterus. Extrasystoles can be nodal, atrial or ventricular, sometimes they come from different foci.
Emotional stress, diseases of the nervous or endocrine system can contribute to their appearance at any stage of pregnancy. During childbirth, extrasystole is physiological and its appearance is provoked by contractions and pushing, pain, a feeling of fear and reflex effects of blood flows from the contracting uterus. Immediately after childbirth, such rhythm disturbances disappear.
In most cases, extrasystole during pregnancy is caused by organic heart diseases (myocarditis, heart disease, cardiomyopathy, etc.). Frequent rhythm disturbances of this nature can lead to the development of an attack of angina, heart failure and atrial fibrillation. In the future, the course of pregnancy and its outcome will depend on the severity of the underlying heart pathology.
Treatment
Rare and isolated extrasystoles do not require the use of antiarrhythmic drugs. If rhythm disturbances of this nature become frequent, group or polytopic and cause discomfort, then the woman is prescribed drug therapy. It may include the following drugs:
- infusion of motherwort or valerian;
- Potassium chloride;
- Panangin;
- Anaprilin;
- Verapamil.
Pregnant women are not recommended to prescribe antiarrhythmic drugs that contain belladonna or atropine.
In some cases, extrasystole may develop due to an overdose of cardiac glycosides. To stop such arrhythmias, it is necessary to discontinue these drugs and prescribe Difenin.
For polytopic and group ventricular extrasystole, the following drugs are recommended:
- Novocainamide;
- Lidocaine;
- Difenin.
Symptoms
A pregnant woman notices weakness and dizziness instead of arrhythmia. The feeling of a sinking heart and a strong sharp blow is subjective and rare.
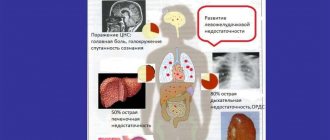
Heart rhythm disturbances are manifested by common symptoms :
- fatigue;
- chest pain;
- labored breathing;
- dizziness;
- spasm in the body;
- loss of consciousness.
In pregnant women, sinus tachycardia occurs due to anemia. Symptoms include anxiety and exercise intolerance . During an attack, women feel their own heartbeat, complain of malaise, sweating and faintness, and less often of shortness of breath or chest pain.
Why does it occur
Arrhythmia during pregnancy does not always indicate pathology.
Women are more at risk of developing disorders:
- with heart defects;
- have undergone surgery on an organ;
- with congenital pathologies of the conduction system, in which the tone of the sympathetic department increases and the autonomic nervous system is overloaded.
In most cases, if there are no health problems, heart rhythm disturbances occur due to:
- disorders of the gastrointestinal tract;
- disruptions in the functions of the nervous and endocrine systems;
- pathologies of the upper respiratory tract;
- metabolic disorders in the body;
- excessive physical and emotional stress;
- eating large amounts of fried, fatty and high-calorie foods;
- fluid abuse. It accumulates in the body and overloads the heart;
- drinking alcohol and smoking during pregnancy;
- anemia;
- severe form of toxicosis, disturbing throughout pregnancy.
Arrhythmia during early pregnancy
From the first days of pregnancy, estrogen and progesterone are produced in increased quantities by the corpus luteum of the ovary. An increase in estrogen, human chorionic gonadotropin, affects the activity of adrenaline receptors. As a result, autonomic activity increases, mainly of the sympathetic nervous system – the “flight and fight” reaction. The mechanism suppresses the parasympathetic nervous system, which regulates digestion. This partly explains the development of toxicosis. Due to the increase in the level of steroid hormones, the load on the liver increases, the function of which is reduced when the sympathetic nervous system is active. Women experience intoxication, and its main symptom is tachycardia.
Vomiting, as one of the manifestations of toxicosis, is accompanied by loss of electrolytes. A healthy blood potassium concentration is 3.5-5.2 mmol/L. The resting potential of the cardiac muscle cell membrane is determined by the ratio of potassium concentration in the intracellular fluid and outside the cell. Minor changes in plasma levels alter the resting membrane potential, affecting the electrical activity of the heart. Clinically, electrolyte imbalance is manifested by arrhythmias. Normal heart rhythm is disrupted by an imbalance of calcium and magnesium.
Diagnostic methods
The reason for contacting a doctor may be any ailment of a pregnant woman, characteristic of one or another type of arrhythmia.
After examining the complaints, the doctor prescribes a comprehensive examination. Diagnosis of arrhythmia during pregnancy includes:
- ECG is a diagnostic method in which the electrical activity of the heart is recorded using special electrodes;
- ECG using the Holter method - the study of heart activity is carried out throughout the day;
- ECHO-CG - ultrasound examination of the functioning of the pregnant woman’s heart;
- exercise test - an ECG is performed during a woman’s active physical activity;
- test with an inclined table - first the heart rate is examined in a horizontal position, then in a vertical position. Used for frequent loss of consciousness;
- electrophysiological study - a technique in which electrodes are inserted into the heart cavity;
- general clinical blood and urine tests;
- consultation with a cardiologist.
Arrhythmia in later stages
In the third trimester of pregnancy, the heart adapts to large volumes of blood. The ventricles and atria dilate. The mass of the left ventricle especially increases. Myocardial cells stretch. Because of this, they are more often ready to carry out an excitation impulse due to premature depolarization. The period of refractoriness - the insensitivity of cells to the nerve signal - is reduced. Any increase in heart rate can cause a dangerous attack of atrial fibrillation. Hormonal surges and stress on the eve of childbirth contribute to arrhythmia.
In later stages, an enlarged uterus anatomically and physiologically affects the heart area and chest. Resting heart rate increases with reduction of PR, QRS and QT intervals in the electrocardiogram of pregnant women. The heart moves up and to the left, the left axis deviates. Cell conductivity is disrupted due to stretching of the chambers. Supraventricular tachycardia and ventricular extrasystoles occur.
The growing uterus puts pressure on the dome of the diaphragm - the respiratory muscle. The vagus nerve passes through it, regulating the heartbeat. The growing belly prevents the ribs from expanding laterally as you inhale. Women begin to breathe “chest” with the collarbones and ribs rising upward. This causes tension in the neck muscles. The spasm irritates the vagus nerve, which normally keeps the heart rate at 90 beats per minute.
Arrhythmia in the fetus
Fetal heartbeat disorders occur in 2% of cases. The normal heart rate is 100-180 beats per minute. The most common arrhythmias in the fetus during pregnancy are atrial extrasystoles and supraventricular tachycardias - stable and unstable. Sustained supraventricular tachycardia causes non-immune fetal hydrops, provokes premature birth and perinatal pathologies. Treatment depends on gestational age, duration of tachycardia, maternal health and possible risks.
Develop your baby from 28 to 40 weeks
Scientists have determined the relationship between this fetal heart disease and chromosomal abnormalities at 10-14 weeks of pregnancy. A heart rate greater than 170 beats per minute is a risk factor for abnormal first-trimester genetic screening, regardless of other causes. It has also been proven that high levels of maternal stress and the release of the hormone cortisol influence structural abnormalities of the fetal heart.
Main types of arrhythmia
It is worth considering in more detail the most common forms of arrhythmia during pregnancy.
Extrasystole during pregnancy
Normally, the pacemaker that generates impulses to contract the heart is the sinus node. Thanks to this, the atria and ventricles work harmoniously. However, pathological processes can cause the formation of extrasystoles in other places due to an increase in the electrical activity of some cells. Such impulses can be single or group.
How to treat the disease
When is treatment required for this disease during pregnancy? It all depends on the frequency, duration of attacks and tolerance. The cardiologist always takes into account side effects caused by drug metabolism. The greatest risk increases during the period of organogenesis, which ends by the end of the first trimester. Initially, minimal doses of medications are prescribed under strict maternal and fetal monitoring. The following drugs are used in practice: Digoxin, Adenosine, Amiodarone, Flecainide, Procainamide, Propranolol, Propafenone, Quinidine, Sotalol and Verapamil. Pregnancy changes the pharmacokinetics of drugs. Many women who responded well to therapy before conception experience arrhythmias even with drug treatment.
List of approved and effective medications:
| "Adenosine" is safe for pregnant women, no effect on the fetus has been identified. Due to impaired deamination, low doses of the drug are prescribed. |
| "Verapamil " is safe, but when administered quickly it can cause bradycardia. |
| Sotalol causes minor complications in the form of transient fetal bradycardia. |
Amiodarone one of the most dangerous drugs for the child and mother. It disrupts the function of the thyroid gland and causes premature birth.
During pregnancy, this heart disease is treated conservatively. If no heart disease is detected, the woman is prescribed rest. Vagal maneuvers help relieve an attack: washing with ice water, massage of the carotid artery and exhalation with resistance to normalize the heart rhythm. Arrhythmias caused by physiological factors disappear immediately after childbirth.
Treatment methods
The choice of treatment for arrhythmia during pregnancy depends on its type. Extrasystole, as a rule, is treated by regulating lifestyle, proper nutrition and adequate physical activity, which are acceptable during the perinatal period. However, if the pathology is severe, adrenergic blockers may be prescribed.
The sinus type of arrhythmia requires taking special medications that normalize the heart rhythm. In addition, a woman should control weight gain and drink vitamin and mineral complexes that her doctor will prescribe.
Atrial fibrillation requires mandatory radical treatment. The expectant mother is administered Novocainamide. Then special procedures are carried out to protect the fetus in the uterus. Then the woman is given extra-pulse therapy.
Paroxysmal tachycardia is often treated by taking sedatives and stabilizing the emotional background of the pregnant woman.
Wolff-Parkinson-White syndrome is treated with the administration of Novocainamide. In most cases, it does not require specific treatment, it just needs to be kept under control.
Blockades in pregnant women require the installation of a pacemaker. Also, such mothers are prohibited from giving birth on their own, so they are prescribed a caesarean section.
Consequences and complications for mother and fetus
Arrhythmias, as a symptom of cardiac pathologies, affect the outcome of pregnancy. Studies confirm that obstetric complications occur in 35% of cases when there are structural changes in the mother’s heart. When choosing drugs to correct heart rhythm, the developmental period of the unborn baby is taken into account.
Premature birth in women with arrhythmias is caused by early rupture of the membranes and aging of the placenta. Complications are caused by a decrease in blood flow in a woman’s body. The disease increases the risk of postpartum hemorrhage. Therefore, during pregnancy, they offer stimulation of labor on a specific day. With persistent attacks against the background of an uncorrected atrial septal defect, the risk of developing preeclampsia increases.
Heartbeat disturbances in pregnant women are often physiological in nature and safe. They may be accompanied by weakness and dizziness. The causes are anemia, vomiting due to toxicosis. In case of frequent and persistent attacks, you should consult a doctor.
What contributes to the occurrence of the disease? Most common risk factors
Factors influencing the development of arrhythmia are:
- Changes in the circulatory system characteristic of pregnancy. In pregnant women, the total blood volume increases sharply and noticeably: firstly, this allows for adequate blood circulation in the mother-placenta-fetus system, and secondly, it prevents the serious consequences of inevitable blood loss during childbirth. However, such a load affects the functioning of the heart, causing disruptions, including arrhythmia.
- Emotional imbalance. Any stress or psycho-emotional stress during pregnancy feels completely different, and excessive emotionality or excitement inevitably leads to increased heart rate. Therefore, during such a sensitive period, it is better to avoid any shocks.
- Long-term toxicosis. Debilitating nausea and other symptoms of toxicosis exhaust the body, forcing it to work in “emergency” conditions. Such loads, coupled with a lack of nutrients, which is inevitable with constant nausea and vomiting, can lead to pathological heart rhythm.
- Anemia. During pregnancy, hemoglobin levels decrease, which can cause oxygen starvation in the mother and child. Defense mechanisms, trying to compensate for the deficiency, activate blood circulation by increasing heart rate, which causes frequent attacks of arrhythmia.
- Lack of microelements. The nutrition of a pregnant woman should be especially carefully thought out and balanced, because the incoming nutrients should be enough not only for the woman, but also for the fetus. Deficiency of iodine, potassium, and iron affects the patient’s well-being, and attacks of arrhythmia are one of the common symptoms of this condition.
- Reasons not related to pregnancy. Unfavorable heredity, a history of chronic diseases, thyroid pathologies, vegetative-vascular dystonia and dozens of other abnormalities can become associated risk factors for the development of arrhythmia during pregnancy.