Ventricular arrhythmia is a disordered rhythm, heart rate and the sequence of contraction and excitation of the heart muscle. The functionality of the myocardium is caused by a source of impulses located under the His bundle in the muscle layers of the cardiac ventricles.
In most cases, arrhythmia does not pose a threat to a person’s life and can occur for trivial reasons: overeating, uncomfortable clothing, fast walking, etc. The patient experiences rapid heartbeat, disruptions in cardiac function, or the absence of several contractions. Sometimes disorders can significantly affect a person’s quality of life and be a consequence of a serious disease of certain body systems.
Extrasystole
This form of the disease is one of the most frequently recorded; it is caused by premature contraction of the heart. Ventricular arrhythmia (extrasystole) is found in 70% of people of different ages; its appearance is often caused by stress, consumption of alcohol and nicotine, and coffee. Also, arrhythmia of this form can occur when the myocardium is damaged due to the development of various diseases.
There are five classes of extrasystole, the presence of one of them can be detected using an ECG within twenty-four hours:
— class zero assumes the absence of extrasystoles;
- the first class is characterized by the appearance of no more than thirty single contractions over one hour;
- the second class is characterized by the appearance of more than thirty single contractions over one hour;
— the third class assumes the presence of polymorphic extrasystoles;
— the fourth class assumes the presence of paired polymorphic or monomorphic abbreviations;
- the fifth class is characterized by group contractions, at times attacks of tachycardia are possible.
What is ventricular extrasystole
Against the background of the correct heart rhythm, almost 5% of people experience premature contractions of the heart chambers, called extrasystoles. According to their place of origin, they are divided into atrial or supraventricular and those that appear in the ventricles. They all occur suddenly without previous clinical signs or sensations.
The source of excitation of ventricular extrasystole is located in the His bundles and Purkinje fibers, located deep in the heart muscle.
Tachycardia
Ventricular arrhythmia of this form is manifested by an increase in heart rate (more than 90 beats per minute). Tachycardia can manifest itself both as a pathology and as a physiological phenomenon during attacks of fear, physical activity, and so on. Most often it is a symptom of the development of various disorders of the endocrine and autonomic nervous systems. Tachycardia as a pathology can lead to bad consequences. Thus, blood pressure drops, blood flow to organs slows down, blood supply to the body and the heart deteriorates, which leads to the risk of coronary artery disease or heart attack. There are several classes of tachycardia:
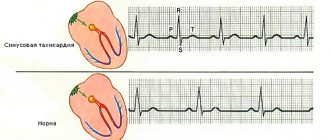
1. Sinus - there is a disturbance in the transmission of impulses to the ventricles from the sinus node. This can be the result of malfunction of the unit itself, or due to stress, fear, and so on.
2. Paroxysmal - there is an attack of heart rate up to 300 beats per minute, which appears and disappears suddenly. This may be due to an increase in the activity of the sympathetic nervous system, as well as changes in the myocardium. Most often it occurs in the second case and is observed in most cases in men. Such tachycardia can develop into ischemia, hypotension, and ventricular fibrillation. Constant attacks of tachycardia have a detrimental effect on the body's circulation, increasing the risk of mortality.
How is the disease treated?
If a rhythm disturbance is detected, treatment with antiarrhythmic drugs is carried out only in very severe cases - the drugs have many side effects. For many cardiac pathologies, they are contraindicated; for example, after a recent myocardial infarction, drugs for arrhythmia cannot be prescribed; they can cause death due to cardiac arrest. Therapeutic measures begin with the elimination of factors provoking the arrhythmic state:
- normalization of sleep and rest patterns;
- creating a diet that includes all the necessary nutrients;
- rejection of bad habits;
- reducing the amount of caffeine-containing products in the diet;
- elimination of stressful situations;
- increasing time spent in fresh air.
For benign arrhythmias, such treatment almost always has a positive effect. If during this period freezing or heart tremors negatively affect the patient’s emotional state, then they are prescribed mild tranquilizers or sedatives.
Drug treatment is prescribed in the following cases:
- a malignant form of pathology has been identified and there is a high risk of developing ventricular fibrillation;
- severe heart failure appeared, accompanied by congestion in tissues and organs;
- attacks of tachycardia are painful for the patient.
But treatment begins not with prescribing drugs for arrhythmia, but with improving myocardial function. To do this you need:
- treat the heart disease that caused the disruption of the normal rhythm (stabilize hypertension, restore full respiratory function, etc.);
- normalize the chemical formula of the blood (in severe cases, potassium or magnesium supplements are prescribed; in the lungs, it is enough to change the diet).
The psychological state of the patient is also important; sometimes the patient’s calmness and positive attitude have a greater therapeutic effect than taking medications. People prone to depression and hypochondria are recommended to be referred to sessions with a psychoanalyst in addition to the main treatment.
In severe cases, surgical treatment is possible, when cauterization or excision of the ectopic focus is performed. Surgery is also indicated when mitral valve insufficiency affects the contractility of the heart.
As a rule, if valve replacement is performed, the pathological focus of excitability is immediately removed.
But surgical operations for the treatment of ventricular arrhythmias are not performed often; as a rule, conservative therapy in most cases gives a stable therapeutic effect. After eliminating the provoking factors and with the correct selection of medications, patients are able to get rid of painful attacks.
Fibrillation
Ventricular atrial fibrillation, or fibrillation, is characterized by a heartbeat of up to 480 beats per minute, the ventricles contract uncoordinated, the heart eventually stops, and the person dies. Fibrillation is often a consequence of a heart attack. In medicine, it is customary to distinguish several classes of atrial fibrillation:
- Primary – appears in the first two days after a heart attack and is a common cause of sudden death in people.
- Secondary atrial fibrillation of the heart develops as a result of cardiogenic shock in patients suffering from a heart attack.
- Late fibrillation appears in the fourth week of the disease.
Fibrillation in all cases begins suddenly. Three hours after its appearance, dizziness begins and weakness appears. After twenty hours a person loses consciousness, after forty hours convulsions begin, the pupils dilate, breathing gradually becomes less frequent, and then stops altogether, and clinical death occurs.
Ventricular pathology
Ventricular extrasystole (arrhythmia) is a deviation from the norm of the heart rhythm, the localization of conductive impulses is in the zone of the ventricle, namely below the His bundle.
Ventricular pathology in its clinic can manifest itself in malignant forms, which can lead to sudden death or the development of severe consequences.
This pathology can also develop so that no symptoms appear; as a rule, no complications arise with this course.
Kinds
There are such varieties of this disease:
- Ventricular extrasystole:
- rare isolated;
- polymorphic;
- group;
- early.
Ventricular extrasystole
frequent;
- salvo;
unstable;
Ventricular tachycardia
- primary;
- secondary.
Ventricular fibrillation
Ventricular extrasystole is when premature impulses are sent from different parts of the ventricular system, which lead to premature excitation of the heart.
Ventricular tachycardia is a sudden increase in ventricular contractions, which manifests itself in attacks. The ventricular heart rate is 150-180 beats per minute, but can be more than 200 (in rare cases). But at the same time, the correct heart rhythm is usually maintained.
Symptoms
Symptoms of ventricular arrhythmia:
- fainting;
- dizziness, general weakness;
cramps and pain in the heart area;- cerebral ischemia;
- nausea and vomiting;
- low blood pressure;
- gastrointestinal disorders;
- circulatory disorders (stagnation);
- hard breath.
Classification
Depending on what consequences can develop after ventricular arrhythmia of the heart appears (symptoms will be discussed in this article), it is customary to distinguish:
1. Functional arrhythmias are characterized by the absence of heart lesions, which are serious. There are practically no complications observed afterwards.
2. Arrhythmias, which are dangerous to humans and develop against the background of heart disease, the mortality rate in this case increases.
3. Malignant development of cardiac arrhythmias, appears in cases of serious heart disease and often leads to death.
Etiology of ventricular arrhythmias
Ventricular arrhythmia can occur without any prerequisites or previous diseases; such arrhythmia is called idiopathic or functional. Despite the absence of reliably confirmed causes of ventricular arrhythmia, a number of conditions have been identified in which this type of arrhythmia is observed more often:
- Smoking (cigarettes, hookah, pipe);
- Stress is acute and chronic;
- Overwork;
- Increased temperature (hyperthermia);
- Caffeine abuse (coffee, energy drinks);
- Alcohol abuse;
- Neurocirculatory dystonia (NCD);
- Osteochondrosis in the cervical spine.
Much more common is ventricular arrhythmia, which is determined or was a background to severe illness:
- Coronary heart disease (CHD);
- Myocardial infarction;
- Cardiosclerosis (post-infarction and atherosclerotic);
- Arterial hypertension;
- Inflammatory heart diseases (myocarditis, endocarditis, pericarditis);
- All types of cardiomyopathies;
- Chronic heart failure;
- Pulmonary hypertension;
- Endocrine diseases (thyrotoxicosis)
- Congenital and acquired heart defects.
Special mention should be made of iatrogenic (associated with medical interventions) ventricular arrhythmias:
- The use of cardiac glycosides (digoxin, corglycon, strophanthin and others);
- Abuse of loop diuretics (furosemide);
- Taking beta-agonists (dopamine, dobutamine, fenoterol and others);
- Taking certain antiarrhythmic drugs (lidocaine);
- The use of tricyclic antidepressants (amitriptyline, imipramine, desipramine and others)
Reasons for appearance
The development of arrhythmias can occur for various reasons, sometimes they are unknown. In the latter case, it is customary to talk about the disease, which is idiopathic in nature. Most often, ventricular arrhythmia (symptoms, treatment and prognosis will be discussed below) occurs as a result of the development of cardiac disease: ischemia, infarction, cardiosclerosis, damage to the mitral valve, as well as myocardial inflammation, hypertension, which is malignant, and pulmonary pathology. In some cases, VSD, hernia and osteochondrosis can also cause the development of arrhythmias. Idiopathic arrhythmia is provoked by external factors: smoking, drinking alcohol and coffee, and frequent use of heart medications.
Causes
The following pathological processes in the heart muscle and blood vessels can influence the development of ventricular arrhythmia:
- Diseases manifested by an inflammatory process (myocarditis, pericarditis, endocarditis).
- Coronary heart disease resulting from lack of nutrition, for example, against the background of the development of atherosclerosis. It is characterized by extrasystoles.
- Cardiosclerosis, that is, the replacement of muscle tissue with connective tissue, occurs mainly after a heart attack.
- Defects of the valve separating the left atrium from the ventricle.
- A malignant form of hypertension.
- Pathologies of the respiratory system that promote hypertrophy of certain parts of the heart muscle.
Sometimes in people with a diseased spine (cervical spine), the cervical artery that supplies the brain is pinched, which causes disruptions in blood circulation and arrhythmias. In more rare cases, disturbances in the resting state are provoked by excessive activity of the parasympathetic nervous system. The heart rhythm returns to normal when receiving physical activity.
It is not always possible to identify the cause. If no pathological abnormalities were found, then doctors can only make a diagnosis of “idiopathic form of ventricular arrhythmia.” It is often associated with external factors:
- drinking alcoholic beverages;
- stress;
- overloads;
- smoking;
- coffee abuse;
- taking heart medications.
Single extrasystoles are often detected on the cardiogram even in healthy people. In the absence of internal pathologies, there is nothing particularly to worry about, but it is advisable to be examined annually to monitor the development of arrhythmia.
Symptoms and signs
Ventricular arrhythmia has no clearly defined symptoms. Different people may have different sensations that do not depend on the cause of the disease. Most often, patients experience weakness, shortness of breath, and dizziness. The manifestation of symptoms is clearly visible on the ECG. First of all, there is an increase in size and deformation of the tooth that is part of the ventricular complex. More than three heartbeats in a row also indicate the presence of arrhythmia. Extrasystole is characterized by pallor, a feeling of anxiety, increased sweating, a feeling of shortness of breath, and interruptions in the functioning of the heart. With tachycardia, dizziness (to the point of loss of consciousness), pain in the heart, palpitations, shortness of breath, hypotension, and convulsions are observed. Fibrillation often manifests itself in the form of fainting, chest pain, pulmonary edema, and pulse deficiency. Its symptoms are due to the fact that the ventricles contract quickly and irregularly.
What is the danger of the disease
The degree of threat that a malfunction of the heart can pose directly depends on the type of arrhythmia. Ventricular arrhythmia can cause coronary artery disease, in which 80% of patients die. The pathology is especially dangerous if observed in patients who have suffered a myocardial infarction. In such cases, the direct cause of death is called ventricular fibrillation. A person having an attack can only be saved by emergency cardiac care. To achieve a long-term stable condition, drug therapy or the installation of a pacemaker will be required.
Classification of ventricular arrhythmia
The main danger of ventricular arrhythmia is sudden death. To predict the likelihood of fibrillation, a hardware examination will be required. For these purposes, an electrocardiogram and Holter monitoring are used.
Possible changes in extrasystoles have a gradation scale shown in the table.
By assessing the grade, the cardiologist will be able to determine the risk of sudden death.
Classification
Such cardiac dysfunction is divided into three key groups:
- fibrillation - contraction of single muscle fibers;
- tachycardia – increased contraction frequency;
- extrasystole - extraordinary contraction of the heart.
Tachycardia
Has a clearly defined classification. According to the degree of stability, tachycardia is divided into:
- unstable paroxysms - they are characterized by several ectopic impulses in a row;
- stable - differ in duration. Lasts more than half a minute.
Important!
Ventricular tachycardia greatly affects blood circulation. The likelihood of sudden death increases significantly.
There are also other forms that provoke the development of fibrillation:
- polymorphic. Occurs as a result of the formation of numerous ectopic foci that cause the heart to contract;
- recurrent. The disease is periodic;
- bidirectional. There are chaotic impulses arising in two sections of the ventricles;
- pirouette. An exceptional form, which is characterized by unstable increases in the amplitude of contractions.
Sinus tachycardia on ECG
Fibrillation
The pathology is characterized by incomplete contractions that activate some muscle fibers. There are the following stages of the disorder:
- Convulsive. The flickering lasts for 20-50 seconds. At this time, frequent contractions occur in local areas.
- Tachysystolic. The attacks last no more than 1-2 seconds.
- Flickering. Failures continue for 2-3 minutes. At this time, numerous irregular contractions of individual muscle areas occur.
- Atonic. This period begins a few minutes after the atrial stage begins. The atonic phase is characterized by irregular contractions. Then the amplitude decreases, the number of muscle fibers not involved in contractions increases.
Important!
Considering the clinical signs, ventricular fibrillation is divided into paroxysmal and permanent forms.
Ventricular fibrillation on ECG
Extrasystole
There are several extrasystolic classes. To establish the type of pathology, it is necessary to monitor electrocardiographic data within 24 hours. Rhythm disturbances are as follows:
| Violation class | Description |
| Null | Extrasystoles are not observed |
| First | Up to 30 single contractions are observed in 60 minutes |
| Second | More than 30 extrasystoles per hour detected |
| Third | Presence of polymorphic extrasystoles |
| Fourth | Paired monomorphic or unpaired polymorphic contractions appear |
| Fifth | Group contractions were detected. At this stage, the first manifestations of ventricular tachycardia can be observed. |
Types of Extrastoll on ECG
Important!
The first class does not have pronounced symptoms and does not affect blood flow. This arrhythmia is functional. It does not require medication or instrumental treatment. Extrasystole, starting from the second class, is considered dangerous to health. In these cases, the risk of fibrillation and tachycardia increases, which can lead to sudden death.
Diagnosis of the disease
Ventricular arrhythmia can be confirmed with ECG monitoring, and a stress ECG, VEM, or treadmill test may also be performed. The study involves recording heart impulses using electrodes that are placed on the skin of a person's chest, as well as on his arms and legs. The readings are recorded on the monitor, after which they are transferred to a printing device and printed on paper. With VEM, indicators are taken during exercise; an exercise bike is used for this. The treadmill test uses a treadmill. When making a diagnosis, it is necessary to take into account those factors that influence the onset and cessation of attacks. This includes the emotional and mental state of the patient, physical activity, taking medications, etc. Additional methods of research for the presence of arrhythmias are: radiography, tomography, ultrasound of the heart. Further treatment of the disease will depend on the results of these tests.
Complications and prognosis
The consequence of supraventricular arrhythmia can be sudden cardiac death. This occurs if acute symptoms and loss of consciousness are present within 1 hour of the onset of symptoms.
Also, with supraventricular pathology, complications may appear in the form of atrial fibrillation, heart failure, changes in the myocardium (namely in structure).
If symptoms appear frequently, you should definitely consult a doctor. Only with timely treatment can dangerous complications be avoided.
Ventricular extrasystole (arrhythmia) is dangerous if there are concomitant diseases of the cardiovascular system and various myocardial dysfunctions. With these disorders, sudden cardiac death is quite possible. Since persistent ventricular tachycardia and ventricular fibrillation may occur. But if there are no pathologies, then the prognosis is quite favorable, even with frequent attacks.
It should be noted that the most susceptible to this disease are:
- overweight people;
- people who abuse alcohol, smoking and drugs;
- patients with diseases of the cardiovascular system, in which pathologies can be either congenital or acquired;
- patients with thyroid disorders, etc.
A diagnosis of supraventricular or ventricular arrhythmia is made when:
- Examination by a doctor;
Certain indicators of such laboratory tests as general blood and urine analysis, biochemical analysis of blood and urine, analysis of hormone levels;- For certain changes detected on electrocardiography, it is also possible to use Holter electrocardiography;
- Changes in the myocardium identified by echocardiography;
- Carrying out an MRI. This examination is prescribed if all previous ones turned out to be uninformative.
Treatment of extrasystole
In frequent cases, this disease is associated with a lack of electrolytes in the human body, which is detected by a blood test. Therefore, a magnesium-potassium diet is often recommended for extrasystole. It is also worth paying attention to sleep and rest patterns, diet, bad habits, frequent coffee consumption, stress, and so on. Sedatives may be prescribed. If ventricular arrhythmia is severe, medication is prescribed, and in some cases surgery is required. The patient is prescribed electrolytes, ACE inhibitors, nitrates, etc. Anti-arrhythmia drugs are of great importance here.
Treatment methods
Not all patients who have been diagnosed with the disease are indicated for inpatient treatment. If the disease is benign, drug therapy is not prescribed. The patient is given a number of recommendations that are aimed at changing lifestyle:
- eliminating bad habits;
- normalization of sleep and wakefulness time;
- prolonged exposure to fresh air;
- complete balanced diet.
Prescribing potent antiarrhythmic drugs to the patient is inappropriate. In case of functional pathology, therapy will do more harm than good, since most drugs have strong adverse reactions.
Taking medications is indicated for patients in the following cases:
- for malignant pathology;
- negative impact of arrhythmia on blood circulation;
- the patient has difficulty withstanding the attacks and complains of deteriorating health.
In this regard, the doctor must first determine the need to prescribe medication. The main goal of therapy is to improve the quality of life. It is sometimes impossible to eliminate cardiac problems.
Antiarrhythmic drugs
Medicines of this class are intended to relieve attacks and eliminate underlying disorders. Most often, cardiotherapists prescribe the following drugs:
| Type of drug | Actions |
| Beta blockers | Reduce the effect of adrenaline and calm the rhythm. They help patients well after a heart attack. Popular from this group are Biprol and Atenol. |
| Cardiac glycosides | Normalize blood pressure and reduce the load on the heart muscle. |
| Sedatives | They consist of plant components that eliminate nervous tension and restore the natural rhythm of the heart. |
| Antidepressants | Prescribed for arrhythmia that occurs against the background of a psychosomatic disorder. |
| Omega-3 | Indicated for ischemic diseases and brain hypoxia. |
| Medicines containing magnesium and potassium | Normalize the functioning of the heart muscles, stabilize blood pressure. |
| B vitamins | Used to increase nerve conduction. |
Surgery
Surgical intervention becomes advisable when drug therapy is ineffective and recommendations for correcting quality of life. In this case, the surgeon uses catheter ablation . This procedure stops the ectopic signal. The scheme for carrying it out is as follows:
Scheme of catheter ablation
- the catheter is inserted into the femoral artery;
- lead into the cardiac ventricle;
- cauterize the source of the ectopic signal.
Strip surgery is performed if the patient needs to have an artificial valve implanted or an aortic aneurysm removed. Along with these goals, the ectopic impulse is eliminated.
Sometimes a patient needs to have a pacemaker installed. With the help of this drug, you can artificially set the rhythm of the heart. Install it this way:
- in a state of anesthesia, electrodes are inserted into the heart chambers;
- The device is installed through the chest incision. Then they connect.
Folk remedies
For functional disorders, it is strongly recommended to use traditional medicine. However, the use of any decoctions and tinctures should be under the supervision of the attending physician.
Hawthorn fruit tincture
There are many recipes that can be prepared at home. Here are some of them:
- Equal parts of cornflower, valerian and calendula are mixed. A tablespoon of the collection is steamed with half a liter of boiling water. Infuse for three hours with the lid closed. Take 50 ml before meals.
- Three tablespoons of dry horsetail are poured with boiling water. Drink the cooled medicine no more than 7 times a day.
- 100 grams of dried hawthorn fruits are poured with a liter of alcohol. They insist for 10 days. Half a teaspoon is diluted in a third of a glass of water and drunk three times a day.
- Equal amounts of radish juice and honey are mixed and drunk three times, 30 ml each.
Ready-made tinctures and mixtures should be stored in a cool place. If you have an allergy, you should stop treatment with traditional recipes and see your doctor.
Ventricular arrhythmia develops due to the formation of a source of ectopic impulses. The cause can also be heart pathologies and external factors. Functional failures are not dangerous, you just need to reconsider your lifestyle, use folk remedies and register with a doctor. For serious disorders, the patient will need medical treatment consisting of antiarrhythmic drugs. The course and treatment regimen is selected by the doctor based on the diagnostic results. If drug therapy is ineffective, the patient will be prescribed surgery.
Prognosis for arrhythmias
The prognosis for such a disease will depend on its form, the presence of heart pathology, and circulatory disorders in a person. Ventricular and supraventricular arrhythmias, which are not associated with heart disease, do not threaten the life and health of people. If the disease develops against the background of heart pathology, the prognosis will be unfavorable. Life expectancy here will depend on timely treatment. Therefore, it is recommended to monitor heart function and follow all medical recommendations, then the disease can be stopped. At the same time, one should not forget about preventive measures, since taking care of one’s health can play a big role, and in some cases, even save a person’s life.
Therapy for cardiac arrhythmia
Treatment of neurogenic extrasystole is carried out with sedatives - motherwort, valerian.
For arrhythmia associated with organic heart disease, the following drugs are prescribed:
- β-adrenergic stimulants – Obzidan, Anaprilin,
- for bradycardia, anticholinergic drugs are used - Ergotoxin with belladonna or phenobarbital,
- For tachyarrhythmia, antiarrhythmic drugs are used - Amiodarone, Sotalol, Procainamide.
For frequent attacks of extrasystole, the method of radiofrequency catheter ablation is used.
Traditional treatment
Ventricular arrhythmia is quite difficult to cure, and the tactics of prescribing therapeutic therapy are determined by the factors that caused the pathological condition. You can easily cope only with class 0 extrasystole, which does not manifest itself (if no intra- or extracardiac pathologies have been detected in a person, treatment may not be carried out at all).
If ventricular arrhythmia has a well-defined clinical picture, therapeutic therapy is prescribed aimed at maintaining electrolyte balance and control over blood pressure levels.
To avoid serious exacerbations during treatment, you should avoid factors such as:
- Strong psycho-emotional stress.
- Alcohol abuse.
- Smoking.
In addition to medications, the patient needs a proper diet, which will contain significant amounts of potassium salts. A moderate increase in physical activity will have a positive effect in the fight against physical inactivity.
Antiarrhythmic therapy includes the following groups of drugs :
- Fast sodium channel blockers. Drugs in this group, in turn, are divided into classes 1A, 1B and 1C, the choice between which will depend on the patient’s tolerability of the drug, the required level of bioavailability, half-life and side effects of the drugs.
The mortality rate in patients who have had a myocardial infarction and taken medications is increased, which has been proven in clinical studies.
- Beta blockers. They reduce the functions of all 4 main functions of the heart: automaticity, conductivity, excitability (contractility) and refractoriness.
- Amiodarone and Sotolol. They are used only in extreme cases, when arrhythmia already directly threatens a person’s life.
- Calcium channel blockers. Use only with strict prescription in connection with the factors that provoked the arrhythmia, and in small doses.
Radiofrequency ablation (RFA) for ventricular arrhythmia is not prescribed to every patient, but only to those people for whom drug treatment has not helped, and they have monomorphic ventricular extrasystole. RFA is a low-risk catheter procedure that is excellent at restoring heart rhythm in patients. The intervention is performed under X-ray control.
Also, people with ventricular arrhythmia can undergo implantation of cardioverter defibrillators . It is most often used if the patient's life is in danger of sudden cardiac death.
Folk remedies
Folk remedies can also help in the fight against ventricular arrhythmia, but you should understand that taking them cannot independently cure a serious pathological condition, and you should take traditional medicine only after consulting with your doctor.
Recipes that can help treat ventricular arrhythmia:
- Valerian infusion. Thanks to the sedative effect of the plant, it can be used by people whose lives, for one reason or another, are associated with frequent stressful situations. To prepare the infusion, you need to pour 1 tablespoon of valerian roots with a glass of boiling water. Then let it brew in a dark container for 12 hours, strain, and you can take 1 tablespoon 3 times a day.
- Cornflower infusion. A particularly effective remedy for combating acute attacks of ventricular arrhythmia. To prepare the infusion, you need to pour 1 tablespoon of blue cornflowers into 200 ml of boiling water. Next, we infuse the liquid in a tightly closed container, filter and store in a dark place. Drink a quarter glass 10-15 minutes before meals. It is best to use on the day when the arrhythmia attack occurred.
- Infusion of lumbago. The plant has a positive effect on cardiac activity. To prepare the infusion, pour 2 teaspoons of lumbago with 1 glass of boiled water and let the liquid infuse for 12 hours. Afterwards we filter the product and store it in a dark corner. Take a third of a glass 3 times a day.
- Calendula infusion. Has a positive effect on cardiac arrhythmias. To prepare the infusion, pour 2 teaspoons of calendula into two glasses of hot water. Next, let it brew for an hour and filter the resulting liquid. You need to take half a glass 4 times a day.
Classification of pathology severity
In order to determine how often ventricular arrhythmias occur, taking an ECG alone is not enough; a person undergoes 24-hour ECG monitoring, during which the heart’s work is recorded at certain intervals throughout the day. Depending on the data obtained, the following classes of violations are distinguished:
- 0 – there are no extrasystoles at all or single rare contractions were recorded (1-5 during the entire examination period). It is considered a variant of the norm.
- 1 – less than 30 contractions of the ventricular region are recorded every hour.
- 2 – over 30 additional contractile impulses of the lower myocardium are determined.
- 3 – polymorphic extrasystoles occur (more than 2 extrasystoles, according to the ECG it appears without a break for atrial contraction) at long intervals.
- 4 – frequent paired (2 at a time) extrasystolic manifestations are observed. They may appear either from time to time or have a polymorphic nature of occurrence.
- 5 – the ECG records burst (3-5 in a row for 30 seconds) extrasystoles or periodically occurring attacks of ventricular paroxysmal tachycardia.
Class 0-1 has no clinical manifestations and is not accompanied by organic changes in myocardial tissue (if class 0-1 is detected, the patient is put on preventive registration with a cardiologist without prescribing treatment procedures). Grades 2-5 can provoke the development of organic changes in the structure of the heart, which increases the risk of ventricular fibrillation.
According to the course of the disease there are:
- Benign (functional). There are no organic heart lesions, the risk of complications and development of fibrillation is minimal.
- Potentially malignant. The volume of cardiac blood output is reduced by 25-30%. Changes in myocardial adductibility are diagnosed, and the risk of developing life-threatening conditions increases.
- Malignant. There are multiple organic lesions of the heart, in which the appearance of arrhythmia leads to a life-threatening condition and death.
The severity of the course and the tendency to develop fibrillation are determined only after a series of clinical examinations.
Classification of ventricular extrasystoles
Ventricular arrhythmia is a violation of the frequency, rhythm, sequence of propagation of excitation and contraction of the myocardium, caused by an impulse source that is localized below the His bundle: in the region of the branches of the His bundle, in the Purkinje fibers or directly in the muscular thickness of the ventricles of the heart (ectopic focus of excitation).
Ventricular tachycardia is three or more ventricular complexes on the electrocardiogram arising from an ectopic focus of excitation and having a frequency of 100 to 240 beats per minute.
Ventricular fibrillation and flutter are mutually uncoordinated contractions of individual muscle fibers that involve the entire volume of the ventricular myocardium, which entails such a disruption of the heart that the pumping function of the heart almost immediately stops.
Ventricular arrhythmia can occur without any prerequisites or previous diseases; such arrhythmia is called idiopathic or functional. Despite the absence of reliably confirmed causes of ventricular arrhythmia, a number of conditions have been identified in which this type of arrhythmia is observed more often:
- Smoking (cigarettes, hookah, pipe);
- Stress is acute and chronic;
- Overwork;
- Increased temperature (hyperthermia);
- Caffeine abuse (coffee, energy drinks);
- Alcohol abuse;
- Neurocirculatory dystonia (NCD);
- Osteochondrosis in the cervical spine.
Special mention should be made of iatrogenic (associated with medical interventions) ventricular arrhythmias:
- The use of cardiac glycosides (digoxin, corglycon, strophanthin and others);
- Abuse of loop diuretics (furosemide);
- Taking beta-agonists (dopamine, dobutamine, fenoterol and others);
- Taking certain antiarrhythmic drugs (lidocaine);
- The use of tricyclic antidepressants (amitriptyline, imipramine, desipramine and others)
To determine the degree of danger of ventricular arrhythmia, and, consequently, the choice of treatment tactics, a clinical classification of ventricular arrhythmias has been developed, named after the scientists who developed it (Lown-Wolff-Ryan):
- The first type: single (each extrasystole is followed by a normal heart contraction), monomorphic (having the same appearance on the ECG), monotopic (the source of pathological excitation is the same), rare (no more than thirty extrasystoles in any hour of control).
- Second type: extrasystoles have a characteristic similar to the first type, however, more than thirty extrasystoles are recorded in any hour of monitoring.
- Third type: this type of extrasystoles is established regardless of the frequency of registration of extrasystoles and is diagnosed in the presence of polymorphic (polytopic) extrasystoles.
- Fourth type A: paired (not separated by normal heartbeat) monomorphic extrasystoles.
- Fourth B type: paired polymorphic extrasystoles.
- Fifth type: jogging ventricular tachycardia - three consecutive extrasystoles are recorded on the cardiogram; polymorphic or monomorphic does not matter.
Other classifications of ventricular arrhythmias have mainly academic and educational significance than the one described, which is used in practical medicine.
Ventricular arrhythmias of the first type, as a rule, are functional or idiopathic, do not have any hemodynamic or clinical significance, being incidental findings during an ECG and in most cases do not require drug treatment. The second type requires an in-depth diagnostic search, since it can be either a functional arrhythmia or indicate the presence of an organic pathology of the heart.
Symptoms of ventricular arrhythmia are largely determined by etiology and their type.
The general manifestation of any ventricular arrhythmia can be only two subjective symptoms:
- A feeling of the heart sinking, stopping, which occurs as a result of the so-called compensatory pause - an increase in the time of diastole (“rest of the heart”) after an extrasystole;
- The feeling of a jolt, an excessively strong heartbeat, usually occurs after a compensatory pause, since the heart, “overflowing” with blood, needs to perform a forced systole to expel the blood.
The first type of ventricular extrasystoles is characterized by the complete absence of any clinical manifestations; a person simply does not notice rare extrasystoles.
In the presence of a pronounced neurogenic component (VSD, NCD), various nonspecific manifestations are often observed:
- Increased fatigue;
- Irritability;
- Headache;
- Feeling of fear, high anxiety;
- Pallor;
- Subjective feeling of lack of air.
Symptoms of ventricular arrhythmias of types 3-5 are often accompanied by a hemodynamically significant decrease in cardiac output, which has the corresponding clinical picture:
- Arterial hypotension;
- Frequent pulse of weak filling;
- Cyanosis (blueness) of the skin;
- Dyspnea;
- Oligouria (decreased amount of urine excreted);
- Pain in the liver area;
- Chest pain
- Collapse.
https://www.youtube.com/watch?v=OmS-uAfbJNI
The most important role for identifying ventricular arrhythmia, as well as determining its type, is played by electrocardiography, and in particular its variety such as Holter monitoring - “Holter”.
To diagnose the morphological causes of ventricular arrhythmia, the following examinations are necessary:
- Ultrasound of the heart – detects a wide range of heart diseases;
- Bicycle ergometry (or treadmill test) study of heart function during physical activity;
- Myocardial scincigraphy – identifies the area of myocardial ischemia;
- Coronary angiography – to assess the degree of atherosclerosis of the heart vessels;
- Biochemical blood test (creatine phosphokinase (CPK), lactate dehydrogenase (LDH), blood electrolytes, inflammatory mediators, thyroid hormones, and others).
In the case of functional ventricular arrhythmia, it is necessary to combat the causes that cause it, but since an objective connection usually cannot be established, a multifactorial, one-stage approach is required:
- Fighting bad habits: smoking, excessive consumption of alcohol, coffee, tea, overeating;
- Compliance with the work and rest regime: sufficient, but not excessive sleep, moderate physical activity;
- Stress management: training, sedatives.
More severe cases require the work of a cardiologist or at least an appropriately qualified emergency physician. The first urgent step in the treatment of ventricular arrhythmia is the restoration of sinus rhythm.
At the very beginning of medical care after diagnosing ventricular arrhythmia (that is, the ECG machine is already connected), you need to ask the patient to cough, which sometimes leads to rhythm restoration, since this simple manipulation improves coronary circulation. It is not recommended to use the “pericardial shock” method.
Further treatment is carried out depending on the characteristics of the detected arrhythmia, using antiarrhythmic drugs and other methods of stopping the arrhythmia.
Procainamide (novocainamide) is a drug that has pronounced antiarrhythmic activity, but has much fewer side effects than lidocaine. It is administered intravenously in a total dose of 500-1000 mg and an administration rate of 20-30 mg per minute.
Amiodarone is used in cases where there is a slight drop in blood pressure, there are signs of heart failure and cardiac conduction disturbances. The scheme of its administration is as follows: amiodarone at a dosage of 150 mg is dissolved in 100 ml of glucose and injected drip into a vein for 10 minutes, after which 900 mg of amiodarone is dissolved in 500 ml of glucose and dripped for the first 6 hours at a rate of 1 mg per minute, then reduce the speed to 0.5 mg per minute.
Since this form of ventricular arrhythmia has a high risk of developing into ventricular fibrillation, electrical pulse therapy (EPT) is immediately performed.
If for some reason it is not possible to carry out EIT, amiodarone is administered according to the above-described scheme.
Treatment is carried out by administering a 25% solution of magnesium sulfate 8 ml for one minute, which restores sinus rhythm almost instantly (if there is no effect, it can be repeated after 10-15 minutes).
In this case, antiarrhythmic drugs are not effective, and the introduction of some of them of classes 1A and 3 (quinidine, procainamide, disopyramide, amiodarone, sotalol, dofetilide) is extremely dangerous and unacceptable.
The next stage of medical care is maintaining sinus rhythm, which is achieved by the following actions:
- Identify the cause of ventricular arrhythmia and treat it purposefully: in case of atherosclerosis of the heart vessels, it is advisable to perform bypass surgery or angioplasty; in case of coronary heart disease and decreased left ventricular function, ACE inhibitors (lisinopril, ramipril, etc.) and beta blockers (atenolol, metaprolol, etc.) are used .), and diuretics are often used, which requires monitoring of blood electrolytes;
- In case of persistent ventricular tachycardia, frequent relapses, accompanied by heart failure, fainting, severe hypotension, implantation of a cardioverter-defibrillator is indicated; if implantation is impossible for any reason, a combination of drugs is used on an ongoing basis: amiodarone and beta-blockers;
- At the current stage of development of medical science, to maintain sinus rhythm, preference is given to two drugs: amiodarone and sotalol, the prescription and selection of dosages of which is often carried out under the control of Holter monitoring;
- In some cases of ventricular arrhythmia (with a reentry mechanism), radiofrequency catheter ablation, a minimally invasive procedure, the effectiveness of which in some cases reaches 95%, can be extremely effective, which allows you to completely stop taking antiarrhythmic drugs.
Conclusion
Objectively identified ventricular arrhythmia requires the work of a qualified specialist who will conduct a deep diagnostic search and prescribe appropriate treatment.
Why does the disease develop?
The causes of additional pathological excitability of the heart are different. Most often, ventricular arrhythmias are a complication of severe heart disease:
- ischemic disease;
- myocardial infarction;
- post-infarction cardiosclerosis (large areas of scar tissue appear in the myocardium);
- mitral valve defect;
- inflammation of the myocardium or pericardial sac;
- malignant hypertension (A/D often rises to high levels and does not decrease for a long time);
- lung pathologies leading to stagnation in the pulmonary circulation.
In some cases, ventricular arrhythmia can be provoked by changes in the cervical spine (hernia, osteochondrosis) or VSD, when there are serious disorders of vascular function.
But external factors can also provoke arrhythmia:
- smoking;
- alcohol abuse;
- excessive consumption of tea, coffee or other caffeine-containing products;
- poor nutrition (imbalance in the electrolyte balance of the blood can provoke the occurrence of pathology);
- use of heart medications without medical supervision;
- frequent stress (if a stress factor is to blame, then at rest the symptoms of gastric arrhythmia completely disappear).
External factors cause the benign course of the disease. As a rule, after their elimination, the symptoms of the disease disappear.
Signs of ventricular fibrillation
Patients do not feel isolated pulse loss. Extrasystoles of grades 2–5 are felt in the form of cardiac arrest, tremors or interruptions. Functional arrhythmia in vegetative-vascular disorders is combined with headaches, rapid fatigue, and emotional lability (unstable mood).
With frequent extrasystoles, pulsation of the veins of the neck is noticeable. A reliable clinical sign of extrasystole is an electrocardiogram (ECG).
The patient’s complaints with this pathology depend on its type. Single and rare extrasystoles from the ventricles are often asymptomatic and can only be detected using Holter monitoring. With more frequent episodes of rhythm disturbances, the patient may indicate the following sensations:
- feeling of lack of air;
- “fading” of the heart;
- weakness and dizziness;
- chest pain;
- fear and panic;
- flickering and fluttering are accompanied by loss of consciousness.
During the examination, a decrease in pressure, pale skin and cyanosis of the nasolabial triangle are noted. The pulse becomes irregular, and with fibrillation it can be practically unpalpable.