In modern times, tumor diseases of the blood are quite common among people of different ages and genders, with chronic myeloid leukemia (CML) observed in every fifth case. This pathology is a dangerous oncological disease and bone marrow stem cells, which lose the ability to fulfill their purpose and begin to actively multiply, disrupting the activity of the hematopoietic system. If not treated in a timely manner, the pathology can lead to death.
Description of the disease
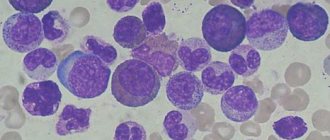
Chronic myeloid leukemia is a pathology that affects stem cells as a result of a gene mutation in immature myeloid cells that form red blood cells, platelets, etc. For this reason, an abnormal gene appears in the human body, which turns healthy blood cells into leukemia (blasts) in the bone marrow. After some time, bone marrow growth stops, and blasts spread through the bloodstream throughout the body, affecting internal organs. This pathology is popularly called leukemia, at the initial stage of development of which the number of leukocytes and basophils increases.
Note! CML develops gradually over a long period of time. The main danger in this case is the fact that without special therapy the disease takes on an acute form, as a result of which the patient dies within a few months.
Epidemiology
Myeloid leukemia develops in every fifth case of all tumor blood diseases. Worldwide, the disease occurs in one person in a hundred thousand. This pathology is observed to the same extent in both men and women, most often it is diagnosed in people aged thirty to forty years. The disease is found very rarely in children. The countries of North America and Europe are in third place in the number of patients with this disease, Japan is in second place. Over the past few decades, epidemiological data on chronic myelocytic leukemia have not changed.
Symptoms in children
Acute lymphoblastic leukemia (lymphocytic leukemia) is the most common type of oncology in children and adolescents (about a third of all malignant neoplasms). The clinical picture unfolds over several weeks.
The onset of leukemia manifests itself in nonspecific symptoms of malaise, characteristic of many relatively harmless diseases: the child becomes lethargic, quickly gets tired, loses interest in games, and the skin takes on a pale appearance. Children are most susceptible to leukemia:
- aged 1 to 5 years;
- Boys get sick more often.
Hematosplenomegaly causes abdominal pain and loss of appetite. A deficiency of white blood cells leads to increased infections. Multiplying blasts fill the bone marrow, bone cavities, accumulate in lymph nodes, and penetrate the brain.
The child feels severe pain (especially in the bones of the limbs and the area of swelling of the lymph nodes), general cerebral symptoms (headache, vomiting), visual disturbances, and paralysis develop. The symptoms of leukemia are individual in each child.
Causes of oncology
Modern medicine has not yet fully studied the causes of the development of myeloid leukemia. Possible causes include:
- an abnormal mutation of a stem cell, which begins to create similar blood cells (clones), which over time end up in internal organs and tissues;
- exposure to toxins and radiation on the body;
- results of radiation or chemotherapy for the treatment of other cancer;
- long-term use of medications whose action is aimed at eliminating tumors;
- infectious and viral diseases, Down or Klinefelter syndrome;
- hereditary predisposition when there is a mutation of chromosomes 9 and 22.
Due to chromosome mutations, new malignant DNA appears in bone marrow cells, which over time replaces healthy cells. New cells - clones begin to actively multiply uncontrollably, they do not die, they enter the blood from the bone marrow. In this case, there is a decrease in the number of mature leukocytes, and a predominance of immature leukocytes, which disrupt blood functions.
Causes of myeloblastic leukemia
The main cause of the disease is considered to be chromosomal abnormalities.
Risk factors include:
- genetic predisposition, chromosomal abnormalities (Down syndrome, Bloom syndrome);
- exposure to ionizing radiation (more than 1 Gy – zones of atomic explosions and accidents, working with radiation sources without the use of protective equipment);
- contact with toxic substances;
- use of a number of medications (Chloramphenicol, Doxorubicin);
- bad habits (smoking);
- a history of diseases of the hematopoietic system.
Stages of disease development
Chronic myeloid leukemia has three stages of development:
- The chronic stage develops in the absence of timely treatment; the disease at this stage is diagnosed in 85% of patients. During this period, stability in the patient’s condition is observed, signs of pathology appear in minimal quantities and do not cause discomfort. The duration of this stage is three to four years, depending on how early treatment was started. CML is usually discovered incidentally during a blood test. If treatment is not started on time, the next stage of the disease occurs.
- The accelerated stage, during which the active growth of abnormal blood cells begins. This phase lasts about one year, and the development of new pathologies in addition to the abnormal chromosome is possible.
Note! The number of immature leukocytes at this stage is constantly increasing, but it is possible to return the disease to the chronic phase with proper treatment. Otherwise, the last stage of the disease develops.
- Blast crisis or end stage, which is the last phase of the disease, is characterized by the presence of new chromosome abnormalities. Here the bone marrow is completely replaced by pathological cells. This phase of the disease is similar to acute leukemia; if treatment is ineffective, the prognosis is unfavorable, and the disease ends in death. The blast crisis usually lasts about six months.
Some patients are already at the terminal stage of pathology when diagnosed, so the risk of death in this case is very high.
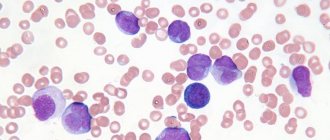
Blood picture in acute leukemia
Evaluation of the clinical picture during the initial examination does not make it possible to make a final diagnosis. Next, the diagnosis of acute leukemia is verified: a blood test (biochemical and cytological parameters) is one of the first tasks when checking suspected leukemia.
Acute leukemia at the onset of the disease is characterized by a decrease in hemoglobin and the number of red blood cells in the peripheral blood (in some cases, anemia may not be detected at the initial stage).
Deviations in the number of platelets and leukocytes are observed, both up and down (thrombocytopenia, less often - thrombocytosis; leukopenia or hyperleukocytosis, neutropenia), depending on the form and stage of leukemia.
The leukocyte formula shifts in favor of promyelocytes and blasts. Moreover, the leukocyte formula reveals a “failure” between blasts and mature leukocytes. Detection of more than 20% blast cells in blood smears is the basis for diagnosis.
Symptoms and signs of pathology
At the initial stage of development, the disease does not show symptoms. Sometimes general weakness and fatigue may occur. As a rule, patients do not pay attention to these signs and do not go to a medical facility. Pathology in the chronic phase can be detected through a blood test.
Over time, a person begins to lose weight, loses appetite, and sweats during sleep. Then pain appears under the left rib, which is caused by an enlarged spleen. For the same reason, the lungs and stomach are compressed, which leads to breathing problems and pain in the head area. The level of hemoglobin and platelets in the blood decreases significantly, so there is a risk of developing blood clots, myocardial infarction, stroke or splenic infarction, and visual impairment.
Then the disease enters the acceleration phase. In this case, the person begins to feel obvious signs of pathology. He experiences pain in the bones and joints, increased body temperature, enlarged abdomen due to pathology of the spleen, and intoxication of the body. Over time, itching of the skin and a feeling of heat appear.
Acute myeloblastic leukemia (AML), which appears at the terminal stage, is characterized by an increase in temperature to dangerous levels, the patient begins to lose weight, and a splenic infarction occurs. The person is in a very serious condition, and a blast crisis is gradually developing. Chronic myeloid leukemia (CML) causes the development of bone marrow fibrosis; the life expectancy of a person in this condition is quite short and depends on supportive therapy.
Note! Associated symptoms at different stages of pathology development are enlarged lymph nodes, the development of anemia, disturbances in the functioning of the central nervous system, thrombocytopenia, etc.
Reasons for the development of the problem
Leukemia, acute myeloid leukemia - all this is the same name for such a pathology. Naturally, many people are concerned about what leads to the development of such a problem. But, as is the case with other types of oncology, doctors cannot name the catalyst for changes in blood cells with 100% certainty. However, it is possible to identify predisposing factors.
Today, the main cause of the development of pathology is chromosomal abnormalities. Usually they mean the situation called the “Philadelphia chromosome”. This is a condition when, due to a disorder, entire sections of chromosomes begin to change places, forming a completely new structure of the DNA molecule. Then copies of such malignant cells are quickly formed, which leads to the spread of pathology.
According to doctors, this situation can be caused by:
- Exposure to radiation. For example, those at risk are those who are in production areas with a large amount of radiation, rescuers working at the site of removing rubble, as was the case at the Chernobyl nuclear power plant, patients who have previously undergone irradiation for the treatment of another type of oncology.
- Some viral diseases.
- Electromagnetic radiation.
- Impact of a number of drugs. Usually in this case they mean anti-cancer therapy due to its increased toxicity to the body.
- Heredity.
Those who are at risk should be screened regularly.
Diagnostics
CML, like other myeloid leukemia, is diagnosed by an oncologist. First, the patient takes a blood test, where an increase in the number of white cells that have not yet matured can be detected; attention is paid to the increased number of red blood cells and platelets. This analysis also makes it possible to determine abnormalities in the functioning of the spleen and liver. Based on the results of the analysis, a preliminary diagnosis can be made and the phase of the disease can be determined.
The doctor then orders a bone marrow biopsy, which is taken from the head of the femur or sternum. Together with the biopsy, bone marrow aspiration is performed, as a result of which the pathological chromosome can be detected. For the same purpose, PCR is used, as a result of which an abnormal gene is detected in the red bone marrow.
Cytochemical diagnostics are often carried out, which makes it possible to identify a pathological process in the body, but also to differentiate the disease from other types of blood oncology. Cytogenetic diagnostics are also used, in which the patient’s chromosomes and genes are studied.
Instrumental research methods include ultrasound, MRI and CT, which make it possible to identify metastases, as well as the condition of organs, tissues and the brain.
Blood chemistry
Biochemical blood tests are carried out to analyze enzyme activity, as a result of which damage to various organs and systems can be determined. In patients with leukemia, an increase in the activity of bilirubin, ALT and AST, urea, LDH and globulins is found. At the same time, there is a decrease in the amount of albumin, glucose and fibrinogen, which is responsible for blood clotting processes. Biochemical analysis using tumor markers will be more informative - they can determine the presence of metastases in distant organs.
Treatment of blood oncology
At the initial stage of development of the disease, drug treatment is used. Doctors often prescribe A-interferon and Myelosan. Relief occurs in the sixth week of taking the drugs. Then maintenance therapy is carried out; in case of exacerbation of the disease, courses of treatment with Myelosan are carried out. If this drug is ineffective, use Myelobromol for three weeks. As a last resort, the doctor prescribes Dopan or Hexaphosphamide.
Also, to treat pathology, chemotherapy is used using chemicals that reduce the growth of tumor cells and promote their destruction. This method is used at different stages of the disease. It has side effects, which are expressed in disruption of the gastrointestinal tract, the appearance of allergic reactions, muscle pain, and cramps. After a course of chemotherapy, the doctor prescribes Interferon to restore the immune system.
If chemotherapy is ineffective, radiation therapy is used. It can also be used to prepare a patient for a bone marrow transplant.
Note! In some cases, the spleen is removed due to severe pain in the abdominal area, significant enlargement of the organ, or the threat of rupture.
In order to prevent the development of microscopic thrombosis and swelling of the retina, doctors prescribe leukocytophoresis. In this case, the blood is purified from pathological cells.
Bone marrow transplantation
This procedure significantly increases the patient’s likelihood of recovery. The patient's relatives often act as donors. After conducting various compatibility tests, the patient begins to prepare for surgery for about one week. During this period of time, he undergoes radiation and chemotherapy.
During the operation, donor stem cells enter the patient's bloodstream, accumulate in the bone marrow and begin to function there within one month. During this period of time, the patient’s immunity is reduced, so he is prescribed medications to reduce the risk of rejection of donor cells. The doctor also prescribes antibacterial and antifungal medications. Gradually, the patient’s well-being improves, bones and soft tissues, blood are cleared of pathological cells and begin to function normally. Full recovery occurs after a few months, during which time the patient is under the supervision of the attending physician.
Note! Complete recovery is only possible with a stem cell transplant. In this case, they must be completely the same for the patient and the donor.
Treatment of myeloblastic leukemia
The mainstay of treatment for this condition is chemotherapy. It occurs in two stages:
At the induction stage, measures are taken whose goal is to reduce the number of pathologically altered cells and initiate the remission stage. The most common scheme is “7+3”. It involves the use of the drug Cytarabine for 7 days with the introduction of the antibacterial drug Rubomycin in the first 3 days.
The “5+2” scheme has also been used: Cytarabine – 5 days, Rubomycin – 2 days. The latter scheme is used in the treatment of persons over 60 years of age.
These tactics are repeated for 2-3 courses until incomplete remission is achieved (disappearance of symptoms caused by excessive proliferation of pathological cells, normalization of the blood picture).
Subsequent consolidation therapy is aimed at maintaining remission and includes 3 to 5 courses of chemotherapy.
To prevent infectious complications, antibacterial therapy is used. The most commonly prescribed drugs are Biseptol and Tsiprinol in combination with oral antifungal agents (for example, Diflucan).
To restore the blood picture, transfusion of blood components is used: red blood cells, platelets, blood plasma.
In severe cases, bone marrow transplantation is used.
Myeloblastic leukemia is an oncological pathology of the hematopoietic system. The prognosis of the disease is largely determined by age, the intensity of clinical manifestations, and adherence to treatment. For older people, the prognosis is less favorable than for young people, which is explained by the presence of somatic diseases, which may become a contraindication to intensive chemotherapy.
What is acute blood leukemia? Blood leukemia (leukemia) is a group of tumor pathologies of hematopoietic tissue, which is characterized by unregulated proliferation (reproduction) and lack of differentiation of white blood precursor cells (blasts). Normally, blast cells should mature into lymphocytes, neutrophils, basophils, eosinophils, macrophages, and megakaryocytes.
Content
Malignant blasts accumulate in the bone marrow, suppressing cell differentiation, and migrate to organs and tissues, causing symptoms of the disease. In the second half of the 19th century, leukemia was identified as a separate nosological form. The clinical picture characterizing acute leukemia was described: symptoms, in particular, included hepatosplenomegaly, changes in the color and consistency of the blood.
Subsequently, the characteristics of the myeloblast were given, the morphology and histochemistry of the types of acute blood leukemia: lymphoblastic and myeloblastic were detailed. The lymphoblastic variant of leukemia is more common in childhood (in 80-90% of cases), while the majority of adult patients with leukemia are diagnosed with the myeloblastic form.
Prognosis and prevention
If the chronic stage of the disease is diagnosed and a bone marrow transplant is performed in a timely manner, a complete recovery of the patient is possible. Most people die when they have an acceleration phase or blast crisis. In 10% of them, death occurs within two years of diagnosis. With the terminal stage of the disease, a person can live for another six months, but if the treatment gives positive results and remission begins, then life expectancy increases to one year.
Methods for the prevention of CML in modern medicine have not been developed, since the exact causes of the development of the pathology have not yet been clarified. Doctors recommend leading a healthy lifestyle, not abusing medications when treating various diseases, and also avoiding exposure to radiation.
( 2 ratings, average: 5.00 out of 5)
Life expectancy with chronic myeloid leukemia
The pathogenesis of myeloid leukemia originates in myelosis.
As a result of certain factors, a tumor-producing clone of the cell appears, which is able to differentiate into white blood cells, which are responsible for maintaining immunity. This clone actively reproduces in the bone marrow, excluding useful hematopoietic germs. The blood is saturated with neutrophils in equal quantities with red blood cells. This is where the name comes from – leukemia. The human spleen should act as a filter for these clones, but due to their large number, the organ cannot cope. The spleen is pathologically enlarged. The process of metastasis formation and spread to neighboring tissues and organs begins. Acute leukemia appears. Damage occurs to liver tissue, heart, kidneys and lungs. Anemia worsens, and the condition of the body leads to death.
Experts have found that CML is formed under the influence of the following factors:
- Exposure to radiation.
- Viruses.
- Electromagnetic fields.
- Chemical substances.
- Heredity.
- Taking cytostatics.
The majority of patients die in the second or third stage of the disease. Approximately 8-12% die after diagnosis of chronic myeloid leukemia in the first year. After the final stage, survival is 5-7 months. In case of a positive outcome after the terminal stage, the patient can survive for about a year.
According to statistics, the average life expectancy of patients with CML in the absence of the necessary treatment is 2-4 years. The use of cytostatics in treatment prolongs life to 4-6 years. Bone marrow transplantation prolongs life much more than other treatments.