What is agranulocytosis?
Agranulocytosis is a serious syndrome that occurs when the body does not produce enough granulocytes (a type of blood cell).
Relationship between neutrophils and granulocytes
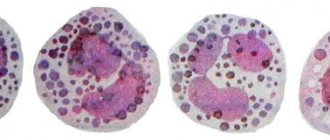
Granulocytes are a group of leukocytes (white blood cells). This is the most numerous type of cell, their size is much larger than that of red blood cells (red cells), approximately 12-15 microns in diameter. They have a large number of cytoplasmic granules (i.e., granules in the cell substance outside the nucleus). Leukocytes without granules in the cytoplasm are called agranulocytes.
There are three types of granulocytes: neutrophils, eosinophils and basophils. Each type in this group is identified by the color of the granules when the cells are stained with a chemical dye. Neutrophil granules are pink, eosinophil granules are red, and basophil granules are blue-black. About 50 - 80% of leukocytes are neutrophils, while eosinophils and basophils make up no more than 3%.
A decrease in the number of blood granulocytes, namely neutrophils, eosinophils and basophils, is called granulocytopenia. However, the term granulocytopenia is often used synonymously with neutropenia (lack of neutrophils), since neutrophils are the most numerous type of granulocyte. The term "agranulocytosis" is used when talking about a critical decrease in the number of cells.
Functions of neutrophils in the body
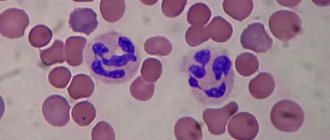
In a healthy person, approximately 100 billion neutrophils are produced in the bone marrow every day. A mature neutrophil is formed from a myeloid cell, their life is extended after transition to tissue. To protect against the rapid depletion of short-lived neutrophils (for example, during infection), the bone marrow retains a large number of cells in its reserve so that they can promptly come to the body’s defense.
In the body, neutrophils move to an infected or injured area.
Neutrophils are active phagocytes; They protect the body by absorbing bacteria, other microorganisms and microscopic particles. Cell granules are microscopic containers containing powerful enzymes that can digest different types of cell material. A neutrophil absorbs a bacterium; it is enclosed in a vacuole (a space in the central part of the cell filled with cell sap).
Granule enzymes are released into the vacuole where the pathogen resides. They carry out the final processing of the harmful organism. Neutrophils also produce interferon (a powerful antiviral agent) and activate the first stage of the blood clotting process.
Thus, neutrophils are a powerful shield of the body. A decrease in the number of these granulocytes increases susceptibility to infectious diseases.
Clinical picture
Symptoms of agranulocytosis are caused by a sharp decrease in the number of cells responsible for the body’s adequate immune response to various factors. In addition, they also inhibit the development of conditionally pathogenic flora; these are microorganisms that are normally present on the mucous membranes of the oral and nasal cavities, the gastrointestinal tract, and the genitourinary system. In the absence of neutrophils to restrain their spread, bacteria begin to multiply, causing infections of various localizations. In most cases, agranulocytosis develops vomiting and stool upset, accompanied by ulcerative lesions of the stomach and intestinal walls, sometimes this can cause perforated bleeding. And also the following signs:
- lesions of the mouth, these are gingivitis, stomatitis, ulcerations on the gums and palate, cheeks;
- the appearance or exacerbation of chronic tonsillitis, pharyngitis;
- infectious liver damage with the appearance of symptoms of jaundice;
- an inflammatory process in the organs of the genitourinary system, which is manifested by pain in the lower abdomen, fever, discomfort when urinating (a similar clinical picture can often develop in women).
An acute decrease in the body's defenses manifests itself in frequent acute respiratory viral infections, resulting in bacterial complications. So, in children, a common runny nose and redness of the throat quickly develops into bronchitis and then into pneumonia (pneumonia). It is characterized by a sharp increase in temperature, painful cough, shortness of breath, and loss of appetite. Due to the breakdown of a large number of cells, symptoms of general intoxication develop. It is manifested by weakness, fatigue, decreased ability to work, nausea, and dizziness. These are the symptoms of agranulocytosis that should alert you and force you to go to a medical facility.
What causes agranulocytosis?
External factors
Agranulocytosis develops due to:
- infectious diseases;
- chemotherapy;
- radiation therapy;
- lack of vitamin B12 and folic acid;
- taking certain medications.
Internal factors
These include:
- autoimmune diseases;
- diseases affecting the bone marrow (aplastic anemia, leukemia);
- tumor metastasis to the bone marrow;
- splenic granulocytopenia (neutrophils are destroyed by the spleen);
- congenital disorders of bone marrow function.
Pathogenesis of the condition
Mature neutrophils are produced by progenitor cells in the bone marrow. The total volume of neutrophils in the body can be divided into three compartments: bone marrow, blood and tissue. In the bone marrow, neutrophils exist in two compartments: the proliferative compartment (ready to be released into the blood) and the storage compartment.
Neutrophils leave the storage compartment and enter the blood without re-entering the bone marrow. There are also two compartments present in the bloodstream, the marginal compartment and the circulation compartment. Some neutrophils do not circulate freely in the bloodstream, but adhere to the surface of blood vessels and they make up approximately half of the total number of neutrophils in the blood.
Neutrophils leave the bloodstream randomly after 6-8 hours and enter tissues where they perform their function or die. Thus, if the process causing agranulocytosis is unknown, measurement of the number of neutrophils in the blood should be supplemented by bone marrow testing to determine the rate of neutrophil production or increased neutrophil destruction.
The site and mechanisms causing agranulocytosis may be limited to any of three compartments: bone marrow, bloodstream, or tissue.
Agranulocytosis can occur as a result of the following events, alone or in combination:
- decreased or absent production of cells in the bone marrow;
- Bone marrow infiltration: when the bone marrow is “hijacked” by pathogenic cells;
- the body's need for a large number of neutrophils;
- decreased neutrophil survival;
- destruction of neutrophils by autoantibodies;
- excessive destruction of mature neutrophils in the bloodstream;
- hereditary periodic decrease in neutrophils.
Risk factors
The risk group primarily includes patients who are frequently exposed to severe infections, as well as unusual, rare infections. Another risk group is patients who, as part of the treatment of other diseases, receive drugs or therapy (for example, radiation therapy), which can cause the development of agranulocytosis. Patients at risk should be especially attentive to their well-being and pay attention to alarm bells. Accurate laboratory diagnostics are required to confirm the diagnosis.
Classification of agranulocytosis
Character of the current
Acute
Acute agranulocytosis, developing over several days, often occurs when neutrophils are used up too quickly and production is compromised.
Chronic
The chronic form develops over months or years and may occur due to decreased production, increased destruction, or excessive movement of neutrophils from the bloodstream into tissues.
Origin
Congenital (hereditary)
Many hereditary disorders are caused by mutations in the gene encoding neutrophil elastase (a group of enzymes in granules), ELA2. Other genes may also be affected.
Acquired
The causes of acquired agranulocytosis are complex, but most are related to three main categories: infection, medications, and autoimmune diseases.
Infections associated with agranulocytosis
| Type of infection | Diseases |
| Viral | Respiratory syncytial virus, dengue fever, mumps, viral hepatitis, Epstein-Barr virus, influenza, measles, rubella, chickenpox, cytomegalovirus, HIV |
| Bacterial | Whooping cough, typhoid fever, tuberculosis (spreading), brucellosis, tularemia, bacterial sepsis |
| Fungal | Histoplasmosis |
Mechanism of development of the syndrome
Myelotoxic agranulocytosis
This type occurs when the growth of myeloid cells (the precursors of granulocytes) in the bone marrow is inhibited.
The reasons are as follows:
- acute leukemia;
- chronic myeloid leukemia of the last stage;
- metastasis of cancer in the bone marrow.
External factors:
- radioactive exposure;
- poisoning with chemicals that suppress the production of blood cells (mercury, benzene, arsenic);
- the use of drugs that inhibit the growth of myeloid cells.
Thus, in myelotoxic agranulocytosis, tumor toxins suppress normal hematopoiesis, and cancer cells displace healthy cellular components. On the other hand, the development of the disease is determined by the degree of sensitivity of the bone marrow to the effects of exogenous factors.
Immune agranulocytosis
The syndrome develops due to excessive destruction of granulocytes by antibodies acting against them. Antibodies destroy cells in the blood and bone marrow. Death of myeloid cells is also possible. As a result, the decay products of dead cells poison the body.
Autoimmune agranulocytosis
This is a symptom of some systemic immune diseases (systemic lupus erythematosus, rheumatoid arthritis, etc.). With these disorders, antibodies are formed in the body to its own cells.
Hapten agranulocytosis
Occurs when haptens (semi-antigens) settle on the membranes of granulocytes. When haptens and antibodies combine on the cell surface, an agglutination reaction (gluing) of granulocytes occurs, and as a result, the cells die. The role of haptens is usually played by various pharmaceutical agents.
Drug-induced agranulocytosis
This is a complication that can be observed after the use of a number of medications, including antipsychotics, antibiotics, antithyroid drugs, but most importantly, chemotherapy drugs. Pathogenesis may be due to direct toxic effects of drugs and/or the formation of drug-dependent antibodies directed against glycoproteins (complex proteins) located in the cell membrane of granulocytes.
Medicines that lead to the development of agralulocytosis are as follows.
Myelotoxic (suppressing the growth of myeloid cells) drugs
These drugs include cytostatics (cyclophosphamide, methotrexate, etc.)
They inhibit the process of cell division.
These medications are used in the treatment of cancer, severe autoimmune disorders, as well as in transplantation to prevent rejection of transplanted organs.
Other drugs that can rarely have a detrimental effect on myeloid cells include chloramphenicol (a broad-spectrum antibiotic) and the antipsychotic aminazine.
Medicines that cause hapten agranulocytosis
Almost any drug under certain circumstances can lead to the death of granulocytes. However, there are categories of pharmaceuticals, the use of which especially often develops agranulocytosis:
- sulfonamides;
- metamizole sodium;
- dimethylaminopyrazolone;
- phenylbutazone;
- barbiturates;
- certain anti-tuberculosis drugs (tubazid, ftivazid);
- procainamide;
- dioxomethyltetrahydropyrimidine;
- macrolides;
- thyroid drugs (used for hyperthyroidism).
The main manifestations of agranulocytosis
Most patients have no obvious symptoms.
However, this syndrome makes a person more vulnerable to infections.
Symptoms associated with infection include:
- high temperature;
- chills and trembling;
- headache;
- sweating;
- a sore throat;
- mouth ulcers;
- inflammation of the gums;
- enlarged tonsils;
- prostration;
- flu-like symptoms.
Laboratory diagnostics
Diagnosis of agranulocytosis is done using a simple blood test to check the number of white blood cells in the blood.
Typically, doctors diagnose agranulocytosis when the absolute neutrophil count is less than 100 per microliter (µL) of blood.
The normal absolute number of neutrophils is at least 1500 per 1 μl of blood.
If the number of neutrophils is between 100 and 1500 per microliter of blood, granulocytopenia or neutropenia is diagnosed.
If a patient's neutrophil levels are abnormal, further tests, such as a bone marrow biopsy or genetic tests, are ordered to determine the cause of the syndrome.
Symptoms of the disease
Agranulocytosis is manifested by the following symptoms:
- feverish condition;
- general weakness;
- the appearance of shortness of breath;
- rapid heartbeat;
- skin damage;
- sore throat of necrotic type;
- pneumonia.
Necrotizing tonsillitis
Symptoms of the disease differ depending on the type of disease and the patient’s health status. In some cases they can be very pronounced, while in others they can be practically absent. It is very important to promptly notice the manifestation of the first symptoms of the disease in order to seek medical help as soon as possible.
Treatment of agranulocytosis
Treatment of agranulocytosis is based on the etiology, severity and duration of the syndrome. Fever and infections that occur as complications of the disorder require special treatment. Surgery is not usually required but may be used in certain cases.
Treatment of infectious complications
For infectious complications of agranulocytosis, antibacterial drugs that do not inhibit myeloid cells are used. As a rule, broad-spectrum antibiotics of 2–3 different groups are prescribed. Specific antibacterial therapy to combat infections begins with the use of third-generation cephalosporins or their equivalents.
Agents from other classes of antimicrobials (eg, aminoglycosides, fluoroquinolones, vancomycin) may be added to treat complications (eg, pneumonia).
The choice of antibiotics depends on the pathogen identified and its sensitivity to the drugs. If the organism is not identified, empirical broad-spectrum antibiotic coverage is used.
Therapy is complemented by the introduction of antifungal drugs.
Integrated approach to treatment, main groups of drugs
Stopping medication
If a particular drug is found to be the cause of the syndrome, you should stop taking it and consult your doctor about choosing an alternative drug.
Use of granulocyte colony-stimulating factor (G-CSF)
G-CSF is an injection that stimulates the bone marrow to produce more white blood cells. This drug is effectively used for cancer patients undergoing chemotherapy. Three forms of G-CSF are currently available: filgrastim, pegfilgrastim and lenograstim.
Medicines that suppress the immune system
This type of pharmacological agent is used for agranulocytosis caused by an autoimmune disorder. Some steroids may be used to reduce immune attack on white blood cells and bone marrow.
Granulocyte infusion
In rare cases, a person needs a granulocyte transfusion, which is similar to a blood transfusion. The cells are taken from a suitable donor, ideally a close relative. He is given steroids and G-CSF to increase granulocyte production. After blood is taken, granulocytes are isolated from it for transfusion into the recipient.
Bone marrow transplantation
When medications and other measures don't work, a bone marrow transplant is needed. The bone marrow of a person with agranulocytosis is replaced with donor bone marrow so that the body can produce healthy white blood cells.
Complications
The most common are sepsis (often staphylococcal), intestinal perforation (usually the ileum, since it is more sensitive to cytostatic effects), mediastinitis, pneumonia, noma; less often - severe swelling of the intestinal mucosa with the formation of obstruction and peritonitis. A serious complication is acute epithelial hepatitis, which often develops after the elimination of AGRANULOCYTOSIS. The absence of granulocytes gives a unique character to the course of infectious complications - the absence of ulcers, the predominance of necrosis. Pneumonia occurs against the background of scanty physical data: dullness is barely noticeable, there may be no wheezing or pronounced bronchial breathing, only crepitus is heard over the affected area. X-ray changes are very scarce.
Features of childhood agranulocytosis
In infants 2 weeks to 1 year of age, the lower limit of normal neutrophil count is 1000 µm. After a year it is 1500 microns, as in adults.
The most common form of agranulocytosis in infants and young children is transitional, that is, occurring with or after a viral illness. The syndrome goes away within 2 weeks. If it lasts longer or if the child is very sick, then appropriate treatment is required.
The most common type of chronic agranulocytosis (lasting 3 months or more) in children is chronic benign agranulocytosis (with no identified cause).
The average age at diagnosis for this type of disorder is 6-12 months, with a range of 3-30 months. Spontaneous recovery occurs by age 5 years, and the average duration of agranulocytosis is approximately 20 months.
Prevention and prognosis
Prevention of agranulocytosis involves providing the patient with careful hematological monitoring. This is especially important during therapy with myelotoxic drugs. It is necessary to exclude repeated use of medications that previously caused symptoms of immune agranulocytosis in the patient.
In chronic agranulocytosis, the prognosis depends on its course. In the acute form, the degree of leukopenia and timely initiation of treatment play a special role. The outcome of the disease is unfavorable with repeated development, severe septic complications, in the first weeks of life.
Prevention of septic complications in agranulocytosis
Recommendations include:
- careful adherence to oral hygiene;
- regular dental examinations;
- using an antibacterial mouthwash;
- timely immunization;
- taking antibiotics and antifungals as prescribed;
- thorough hand washing;
- high-quality treatment of cuts and scratches;
- avoiding large crowds of people;
- exclusion from the diet of undercooked or raw food, fruits and vegetables that cannot be peeled or thoroughly washed;
- proper storage and preparation of food;
- avoiding contact with soil and animals.
These protective measures will help reduce the potential complications of agranulocytosis.