Lymphocytes are white blood cells that are also one of the body's main types of immune cells. They originate in the bone marrow and exist in the blood and lymph. In this article, we'll look at the different types of lymphocytes, what normal levels of these cells should be in the blood, and what happens if the levels get too low or too high.
The article is based on the findings of 32 scientific studies
The article quotes authors such as:
- University of Pennsylvania, School of Medicine, Philadelphia, USA
- Tumor Immunology Group, Institute of Cancer Biology, Danish Cancer Society, Copenhagen, Denmark
- Department of Immunology, St. Jude Children's Research Hospital, Memphis, USA
- Laboratory of Immunology, Tokyo Medical and Dental University, Tokyo, Japan
- Service de médecine interne, Hôpital Cochin, AP-HP, université Paris-Descartes, faculté de médecine, Paris
Please note that the numbers in parentheses (1, 2, 3, etc.) are clickable links to peer-reviewed scientific studies. You can follow these links and read the original source of information for the article.
What are lymphocytes?
- Lymphocytes are a type of other immune cells called white blood cells (WBCs).
- Lymphocytes are cells of the immune system and help our body fight infection.
- Lymphocytes live in the lymph nodes, but also exist in the bloodstream and throughout the body.
- Lymphocytes come in three main types: B cells, T cells, and NK killer cells.
- An abnormal number of lymphocytes in the blood may be temporary or long-lasting.
- Too many lymphocytes in the blood is called lymphocytosis.
- Too few lymphocytes in the blood is called lymphopenia.
- Lymphocytes can be malignantly transformed in diseases such as chronic lymphocytic leukemia, acute lymphoblastic leukemia and some types of lymphoma.
- Lymphocytes originate from stem cells in the bone marrow.
- T lymphocytes mature, or grow, in the thymus, an organ in the neck.
Like all blood cells, both red and white, lymphocytes begin their life journey in the bone marrow . As soon as a person is born, the bone marrow becomes a factory for producing new blood cells. The different types of lymphocytes differ mainly in their site of maturation and function. ()
Functions of different types of lymphocytes:
- Natural killer cells (NK cells) kill tumor cells and virus-infected cells.
- B cells produce antibodies. Antibodies attack cells foreign to the body (bacteria, toxins and viruses).
- T cells destroy the body's own cells, including cancer cells or those that have been taken over by viruses.
Lymphocytes can produce cytokines , which are small proteins important for immune system response, development and suppression of inflammation, and suppression of infections. ()
TYPES OF BLOOD CELLS, INCLUDING 3 TYPES OF LYMPHOCYTES
Lymphocytes are part of the immune system. The innate immune system responds to pathogens in a general manner but does not provide long-term protection. The adaptive immune system responds to pathogens using memory from previous encounters with a specific pathogen, such as the measles virus. ()
Lymphocytes do not live forever. Mature lymphocytes undergo programmed death. This helps maintain homeostasis and tolerance in the body. ()
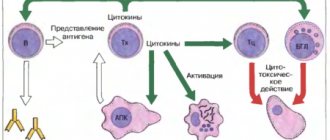
The work of cellular immunity
When a foreign agent enters, the body activates its defense systems, that is, immunity. First of all, macrophages begin to fight the harmful factor; their function is to absorb the antigen. If they cannot cope with their task, then the next level of protection is activated - cellular immunity. The first to recognize the antigen are T-killer cells - killers of foreign agents. The activity of T helper cells is to help the immune system. They control the division and differentiation of all cells in the body. Another of their functions is the formation of a relationship between two types of immunity, that is, helping B-lymphocytes secrete antibodies, activating other structures (monocytes, T-killers, mast cells). T-suppressors are needed to reduce excessive activity of helpers, if necessary.
Types of Lymphocytes
Types of T cells
T cells originate from the bone marrow and mature in the thymus and sometimes in the tonsils. The different types of T cells include killer T cells, helper T cells, regulatory T cells, memory T cells, and natural killer T cells.
Naive (just created) CD4+ T cells are the cells that will become Th1, Th2, Th17 immune cells and regulatory T cells. ()
Cytotoxic (killer) T cells
Killer T cells, also called CD8+ T cells , can scan the surfaces of other cells to see if they are cancerous or infected with viruses or bacteria. They destroy infected cells and help prevent autoimmune diseases.
Inappropriate killing activity of T cells can lead to survival of the infectious agent or to autoimmune disease. ()
T helper cells
Helper T cells, also called CD4+ T cells , on the other hand, help trigger and control the body's immune response. They are called assistants (helpers). These lymphocytes help in the activation of killer T cells, maturation of B cells, and release cytokines. They can only work when activated on the surface of antigen-presenting cells. ()
Helper T cells can be classified into different groups based on their target pathogens, such as Th1, Th2, and Th17.
- The Th1 response (T helper cell type 1) is characterized by the release of interferon-gamma and is more effective against pathogens that are found inside cells, such as bacteria and viruses. ()
- The Th2 response (T helper cell type 2) is characterized by the release of interleukin-5 (IL-5) and is more effective against pathogens that infect outside cells, such as certain bacteria and parasites. ()
- Th17 cells are the inflammatory counterparts of regulatory T cells. They produce interleukin-17 (IL-17), interleukin-6 (IL-6), interleukin-22 (IL-22), tumor necrosis factor TNF-alpha. Th17 lymphocytes protect against extracellular parasites that cannot be effectively suppressed by T helper cells types 1 and 2. Very often, when infections progress into autoimmune diseases, these Th17 cells are associated with the development of autoimmunity and allergies.
Regulatory T cells
Regulatory T cells, also called suppressor T cells , maintain tolerance, prevent autoimmune diseases, and limit inflammation. However, they also suppress immunity to certain pathogens and tumors. ()
Memory T cells
Memory T cells live for a long time (up to 15-20 years) after the end of an infection and help the immune system remember previous infections. They multiply quickly after re-infection with already known infections.
There are 3 types of memory cells including resident, central and effector. Memory T cells are especially important for vaccine development. ()
Helper T cells and cytotoxic T cells can become memory T cells. Memory T cells are stored in the lymph nodes and spleen, and in some cases can provide lifelong protection against specific infections.
Natural killer T cells
Natural killer T cells help bridge the adaptive and innate parts of the immune system. They can produce cytokines and regulate immune responses against self-antigens. ()
T cell deficiency can damage the immune system. Deficiency can cause hereditary diseases, severe fungal infections, cancer and other chronic infections. T cell deficiency is usually present in infants or toddlers. ()
B cell type
B cells primarily function in the adaptive immune system. They secrete (produce) antibodies and cytokines and mature in the bone marrow. They mainly interact with antigens, molecules that induce an immune response, to produce antibodies. ()
Memory B cells
Memory B cells circulate throughout the body to initiate a rapid antibody response when they detect an antigen. They help the immune system respond faster after reinfection. ()
Regulatory B cells
Regulatory B cells help stop lymphocytes that can cause inflammation. They also promote the formation of regulatory T cells. ()
T cells help activate B cells, although there are some B cells that do not require T cells for activation. ()
Error in B cell recognition of infection and its transformation can cause autoimmune diseases such as arthritis, type 1 diabetes, lupus, multiple sclerosis and cancer . ()
LYMPHOCYTES THAT ARE CONSTANTLY RESIDENT IN THE KIDNEYS (TISSUE RESISTANT LYMPHOCYTES), NK KILLER CELLS, CAN BE PARTICIPATED IN THE DEVELOPMENT OF VARIOUS KIDNEY DISEASES. (source)
Type of NK cells - natural killer cells
Natural killer cells (NK cells) work as part of the innate immune system. They provide a rapid response to infected cells. They do not need antibodies to form an immune response against an enemy. ()
Natural killer cells also play a role in the adaptive immune response to help with secondary infections. They are especially essential for fighting cancer and may exhibit innate resistance to viruses such as HIV. ()
Origin of tissue resident T cells
Where do tissue resident cells first appear? These are the descendants of effector cells that have lost their ability to recycle. Some tissues peripheral to the immune system, for example, the mucosa of the small intestine, the abdominal cavity, allow effector T lymphocytes to penetrate freely; others - very limited, a large flow of effector T cells into these tissues is observed only during an inflammatory reaction. The second type of tissue includes those separated by a barrier from the immune system, for example, the brain and spinal cord, as well as many others: peripheral ganglia, mucous membranes of the genital organs, lungs, epidermis, eyes. The difference between the two tissue types is the expression of additional homing molecules for effector T cells, for example, the epithelial infiltration adhesion molecule MadCAM-1 [3].
Figure 3. “To home or not to home?” - difficult choice of effector cell. To home is the process of homing, or migration of T cells, for example, to the place most familiar to naive cells - the lymph node. The alternative is to not travel through the body and become a resident tissue cell.
Lymphocyte count analysis
The simplest test for the number of lymphocytes in the blood is the count of leukocytes and their differentiation. To do this, blood is analyzed either by manual reading in microscopic chambers or by automated counters. Counting the number of lymphocytes in the blood is part of the General Blood Count. Bone marrow may also be used to better examine lymphocytes, but regular blood samples are most common. ()
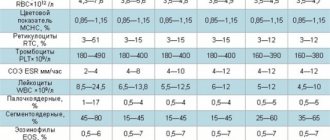
Laboratory results are usually displayed as a set of values known as the “reference range,” which is sometimes called the “normal range.” The reference range includes the upper and lower limits of a laboratory test based on the results of a group of healthy people. Blood for this test is taken from a vein in the arm.
Lymphocyte count: normal, increased and decreased number
Lymphocyte levels can vary depending on a person's race, gender, location, and lifestyle factors.
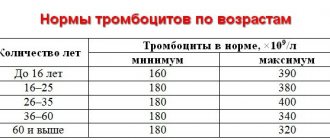
The normal range for lymphocyte counts in adults is 1,000 to 4,800 lymphocytes per microliter (µL) of blood. In children, the normal range is from 3000 to 9500 lymphocytes per 1 μl of blood.
For Caucasians (European race), the level of CD4+ T lymphocytes (helpers) can vary from 600 to 1000 lymphocytes/μl, while for Asian and Middle Eastern populations CD4+ range from 500 to 900 cells/μl. ()
The level of CD8+ T-lymphocytes (cytotoxic) in Caucasians normally ranges from 400 to 660 lymphocytes/μl, while in Chinese residents it ranges from 400 to 800 cells/μl. ()
Reference ranges used for blood tests in the USA:
- 690 – 2,540 cells/µl for CD3+ T-lymphocytes (optimal – ~1410 cells/µl)
- 410 – 1,590 cells/µl for CD4+ T lymphocytes (optimal – ~ 880 cells/µl)
- 190 – 1,140 cells/µl for CD8+ T lymphocytes (optimal – ~ 490 cells/µl)
Lymphocytosis
An abnormally high lymphocyte count (well above 3,000 cells per microliter), or lymphocytosis, may indicate a problem with the immune system
. Lymphocytosis can be caused by influenza, chickenpox, tuberculosis, rubella and other infections. Leukemia can also cause high levels of lymphocytes in the blood. Some medications can cause an increase in lymphocyte levels. (, )
Lymphocytosis does not necessarily mean there is a problem with the immune system and may be temporary
. Symptoms of lymphocytosis are extremely rare.
Lymphocytopenia
Too low a lymphocyte count, or lymphocytopenia, can occur due to AIDS, problems with bone marrow production of lymphocytes, steroid use, or brain disorders such as multiple sclerosis. Other causes of lymphocytopenia include inherited disorders. ()
Like lymphocytosis, lymphocytopenia does not necessarily indicate an immune system disorder. A similar condition can occur after the flu or other common infection. It can also be caused by extreme stress, intense exercise, or poor nutrition (fasting). ()
Diseases and conditions of the body that are most often associated with lymphopenia.
They can be divided into groups - pathogenic (associated with infection), cytotoxic (toxic to cells), congenital (caused by a genetic defect, rare) or nutritional.
- Aplastic anemia (a rare condition in which the body stops producing blood cells)
- Chemotherapy (cancer treatment)
- Radiation therapy (cancer treatment)
- Leukemia (a type of blood cancer)
- HIV AIDS
- Hypersplenism (premature destruction of blood cells by the spleen)
- Poor nutrition and vitamin deficiencies
- Myelodysplastic syndromes (a group of disorders that impair the production of blood cells)
- Rheumatoid arthritis (autoimmune disease)
- Lupus (autoimmune disease)
- Myasthenia Gravis (autoimmune disease)
- Tuberculosis
- Histoplasmosis
- Flu
- Malaria
- Viral hepatitis
- Sepsis
- Typhoid fever
According to the study, zinc deficiency may weaken immune function through the development of T cell lymphocytopenia. ()
Kidney disease, particularly late-stage kidney disease, can reduce the number of T cells in the blood, but lymphocytopenia can also occur with acute kidney inflammation.
How to distinguish resident tissue cells from admixtures of blood cells?
Resident T cells can be correctly, but inconveniently, determined each time by the ability of an individual cell to migrate to lymph nodes, so it is necessary to compile a list of characteristic features that can be used to determine membership in this subpopulation. Resident T lymphocytes in the body's natural barrier tissues (for example, in the lungs and small intestinal mucosa) are somewhat similar to classical effector blood cells: they express the activated cell marker CD69, and the expression is stable throughout life during adulthood and aging and is characteristic of all non-lymphoid tissues . But in addition, CD69 colocalizes with the marker CD103, which denotes a group of adhesion molecules - integrins, which promote the attachment of resident T cells to the epithelium and to fibroblasts in the submucosa of the selected organ. For effector T cells in secondary lymphoid organs, the expression of CD103 integrins is completely uncharacteristic: TEM cells constantly maintain a motile phenotype.
The map compiled by Donna Farber's team has a major flaw: it is unclear how cleanly T-lymphocytes can be isolated from an organ, and what proportion of the analyzed cells are actually blood T-lymphocytes from capillaries inside the organ.
The issue of contamination with blood cells is especially acute for the lungs; it is no coincidence that the subpopulation composition of T cells in the lungs is unexpectedly similar to T cells in the blood and lymph nodes. The issue of blood cell contamination was elegantly solved for mouse T cells: experimental mice were infected with lymphocytic choriomeningitis virus after transplantation of a transgenic P14 T cell clone specific for this virus. As a result, during infection, the majority of circulating cells were represented by the virus-specific P14 clone, and its presence in tissues could be monitored by immunofluorescence with a P14-specific antibody. Before the mice were killed, they were injected with an antibody to the killer T-cell marker anti-CD8, which quickly spread through the bloodstream and bound to all killer T-cells in the blood (but not in the tissues). By microscopy of organ sections, it was easy to distinguish resident killer TRMs from cells only recently released from the blood into the organ, labeled with an anti-CD8 antibody [7]. The number of resident cells calculated by this method was 70 times higher than the numbers determined by flow cytometry; a difference of less than twofold was observed only for resident cells of the lymph nodes and spleen: it turns out that standard methods for isolating lymphocytes from organs are poorly suited for the analysis of killer resident cells and significantly underestimate the population size.
Danger of Low Lymphocyte Count
A recent study by American scientists from the Cleveland Clinic and Cleveland University Hospital showed that there is a clear and consistent relationship between lymphocyte levels and mortality. () An increase in the risk of mortality was observed already at 2,000 lymphocytes/μl, at 1,500 cells/μl this risk increased by 50%, and with a lymphocyte count of less than 1,000, the risk increased by 3.9 times.
lymphocytopenia was found from heart disease, cancer, and respiratory infections (eg, influenza and pneumonia). a particularly negative effect on mortality while increasing red blood cell distribution width (RDW) and the amount of inflammatory C-reactive protein in the blood.
People with low lymphocyte counts, elevated inflammatory C-reactive protein and a red blood cell disorder (RDW) live about 10 years less than people with the same lifestyle but without these disorders. ()
SCHEME OF AN IMMUNE RESPONSE TO A PATHOGEN WITH THE PARTICIPATION OF DIFFERENT TYPES OF LYMPHOCYTES AND THE POSSIBILITY OF ITS REGULATION
Literature
- Clark RA (2010). Skin resident T cells: the ups and downs of on site immunity. J. Invest. Dermatol. 130 (2), 362–370;
- Husband and wife, one of Satan?;
- Iijima N. and Iwasaki A. (2015). Tissue instruction for migration and retention of TRM cells. Trends Immunol. 36, 556–564;
- Schenkel J. M. and Masopust D. (2014). Tissue-resident memory T cells. Immunity. 41, 885–897;
- Thome JJ, Yudanin N., Ohmura Y., Kubota M., Grinshpun B., Sathaliyawala T. et al. (2014). Spatial map of human T cell compartmentalization and maintenance over decades of life. Cell. 159, 814–828;
- Where did vision come from?
- Steinert EM, Schenkel JM, Fraser KA, Beura LK, Manlove LS, Igyártó BZ et al. (2015). Quantifying memory CD8 T cells reveals regionalization of immunosurveillance. Cell. 161, 737–749;
- Frost EL, Kersh AE, Evavold BD, Lukacher AE (2015). Cutting edge: resident memory CD8 T cells express high-affinity TCRs. J. Immunol. 195, 3520–3524;
- Park CO and Kupper T S (2015). The emerging role of resident memory T cells in protective immunity and inflammatory disease. Nat. Med. 21, 688–697;
- Schluns KS and Klonowski K. Diverse functions of mucosal resident memory T cells. E-book, 2015;
- Godfrey DI, Uldrich AP, McCluskey J, Rossjohn J, Moody DB (2015). The burgeoning family of unconventional T cells. Nat. Immunol. 16, 1114–1123;
- Castellana D., Paus R., Perez-Moreno M. (2014). Macrophages contribute to the cyclic activation of adult hair follicle stem cells. PLoS Biol. 12 , e1002002;
- Rodero M. P. and Khosrotehrani K. (2010). Skin wound healing modulation by macrophages. Int. J. Clin. Exp. Pathol. 3 (7), 643–653;
- Farber D., Yudanin N., Restifo N. P. (2014). Human memory T cells: generation, compartmentalization and homeostasis. Nat. Rev. Immunol. 14, 24–35..
How to change the number of lymphocytes
How to increase the number of lymphocytes
The most important thing is to work with your doctor to diagnose and treat the underlying health problems that may be causing your low lymphocyte count.
Depending on the condition of the body and diseases, your doctor may prescribe the following types of therapy:
- Combination antiretroviral therapy for HIV infection
- Antibiotics, antiviral, antifungal or antiparasitic drugs for various types of infections
- Gamma globulin for preventing infections in people with B-cell lymphocytopenia
- Bone marrow stem cell transplantation for certain types of cancer (such as leukemia, multiple myeloma, and some types of lymphomas)
- Medicines to reduce inflammation in autoimmune diseases
If any drug is causing your lymphocyte count to be low (such as immunosuppressants or steroids), your doctor can and should reduce your dose or stop taking it.
People with low lymphocyte counts should support their immune system by including foods rich in a variety of nutrients in their diet, providing adequate amounts of protein, vitamins and minerals. Doctors may prescribe a special diet for people with weakened immune systems.
For people with low lymphocyte counts, it is important to prevent infections:
- Wash your hands frequently with soap or sanitizer
- Avoid crowded places
- Avoid contact with sick people
- Stay away from animals
- Avoid activities that may cause cuts or scratches to the skin
The additional dietary supplements listed below may help you change your lymphocyte levels. Discuss with your doctor whether these supplements may be helpful for you. You should not take dietary supplements on your own, replacing them with standard treatment prescribed by a doctor . Dietary supplements are additional measures.
- Reishi mushroom extract stimulated the formation of CD4+ T lymphocytes by 40 football players for 28 days. ()
- An extract of the herb Holy Basil (Tulsi, Ocimum sanctum) increased the number of T-helper cells, NK killer cells, and Interferon-gamma after 4 weeks of taking the drug in 40 healthy volunteers. ()
- Creatine exhibits antioxidant activity and protects white blood cells from oxidative damage. Creatine and its byproduct, creatinine, help protect lymphocytes and help prolong their life. ()
- Vitamin A
: This vitamin has a direct effect on T lymphocytes and their activation. It also stabilizes Th1-type cells. Vitamin A deficiency, although rare, can cause immune system problems. () - Vitamin D
: This vitamin influences the development of intraepithelial lymphocytes (the bridge between innate and acquired immunity). Vitamin D deficiency is associated with the development of autoimmune and infectious diseases. ()
VARIOUS SUBSTANCES IN FOOD CAN STIMULATE LYMPHOCYTE DEVELOPMENT AND ACTIVITY (source): VITAMIN A , VITAMIN D , INDOLE (CROSFLOWER VEGETABLES)
Recent studies show that blue light and UV light increase T-lymphocyte activity . Just 5-10 minutes of sun exposure is needed to boost the activity of these immune cells. Sunlight stimulates the production of hydrogen peroxide, and this is what makes T cells move faster. ()
The healthiest blue light comes from the sun, as it is balanced by infrared radiation, which activates cytochrome C oxidase in your mitochondria and helps optimize the production of ATP (adenosine triphosphate), the source of energy throughout the body.
How to reduce the number of lymphocytes
The most important thing with a high level of lymphocytes (lymphocytosis) is to identify and treat the underlying cause (most often infections and leukemia). Lymphocytosis usually resolves after the underlying condition resolves. ()
Since high lymphocyte counts are often caused by infections, the main preventative strategy is to reduce their risk of occurrence: ()
- Wash your hands frequently with soap or sanitizer
- Avoid contact with sick people or sharing objects with them
- Disinfect frequently used items
Additional strategies listed below may help you lower your lymphocyte levels. Discuss these steps with your doctor to see if they may be helpful for you. But don't try these methods without your doctor's advice .
Medicines
The following medications may lower your lymphocyte count, but never start taking them or increase your dose for this purpose
. Always follow the treatment plan prescribed by your doctor.
- Steroids
, such as glucocorticoids, inhibit lymphocyte proliferation. Synthetic steroids inhibited both circulating T cells and B cells. () - Adalimumab
(Humira) affects the level and function of T lymphocytes in patients with rheumatoid arthritis. However, there are conflicting reports about whether this drug increases or suppresses lymphocytes. It is worth noting that the effects of this drug are temporary. () - Immunosuppressive drugs
have a lowering effect on the level of T and B lymphocytes in the blood. In one study of 60 patients, the drug cyclophosphamide given with azathioprine reduced the number of T cells. In turn, prednisolone, cyclophosphamide, methotrexate, mycophenolate mofetil and azathioprine reduced the number of B lymphocytes in mice by more than 60%. (, ) - Pentoxifylline
inhibits the early stages of T-lymphocyte activation. () - Azathioprine
- Carbamazepine
- Cimetidine
- Corticosteroids
- Dimethyl fumarate
- Imidazoles
- Interferons
- Methotrexate
- Opioids
- Bisphosphonate therapy for the treatment of osteoporosis
Biological additives (substances)
- Echinacea
: In healthy people, Echinacea reduces interleukin IL-2 (a Th1-type cytokine) and may inhibit T-cell proliferation. On the other hand, it increases levels of interleukin IL-10 (a Th2-type cytokine) and may reduce the inflammatory response. () - Fish oil
: Giving mice fish oil impaired T cell activity against the cold virus but improved lymphocyte proliferation. ()
Diagnostics of cellular immunity
Diagnostics of the T- and B-lymphocyte link allows us to assess the state of cellular immunity.
A basic study determining the percentage of T-, B- and null cells is carried out to identify primary or secondary immunodeficiencies, as well as to monitor immunostimulating treatment. Studying the main populations using markers CD3, 8, 19, 16+5b, as well as the ratio between helpers and killers, allows for a comprehensive assessment of the immune status. Venous blood is used for research.
Diagnostics is carried out by identifying and monitoring the course of:
- autoimmune diseases (increased content of CD3, CD4 helper cells);
- lymphocytic leukemia (increased number of CD3 T-lymphocytes);
- malignant neoplasms (increased number of NK);
- HIV (CD3, CD8);
- chronic infections, allergic reactions, bronchial asthma, etc.
source
Different roles of lymphocytes
May protect against cancer
A higher level of CD8+ T-type lymphocytes (directly in the tumor) indicates an increase in the overall survival of cancer patients. ()
Specialized tumor-infiltrating lymphocyte therapy can treat liver cancer and may help stop the cancer from coming back. ()
Supports Gut Health
Lymphocytes in the intestine play an important role in maintaining the homeostasis of this organ. They are also critical for early response to intestinal infections. ()
Protects against damage due to arthritis
Patients with arthritis and high levels of lymphocytes in their joints had less cartilage and bone damage than people with low levels of lymphocytes. ()
Affect blood pressure
CD8+, Th1-type, Th17 and T-regulatory lymphocytes have different effects on blood pressure. Inflammatory lymphocytes CD8+, Th1, Th17 – increase blood pressure through the production of reactive oxygen species and vasoactive cytokines, changing the inflammatory environment in the walls of blood vessels and in the kidneys. ()
Abnormal lymphocyte levels in various diseases
The body conditions we discuss in this article are usually associated with abnormal lymphocyte levels, but this symptom alone is not enough to make a diagnosis. Work with your doctor to determine exactly what underlying condition may be causing your lymphocyte count to be unusually high or low.
Lymphoma
Lymphoma can be the result of uncontrolled growth of lymphocytes in the body. Mutations in genes or disturbances in molecular pathways involved in tumor suppression can cause uncontrolled growth of B and T cells. ()
B-lymphocyte hyperactivity, associated with autoimmune diseases and impaired T-cell function, can also lead to the development of lymphoma. ()
HIV AIDS
A feature of HIV/AIDS is a decrease in the number and functions of CD4+ T-lymphocytes in the body. Most HIV-infected cells are also resistant (indifferent) to natural killer cells. ()
In studies conducted in HIV-infected patients, CD4+ T cells were most depleted in the intestine. () The HIV virus, when infected, causes dysfunction and death of CD4+ T lymphocytes.
HIV also causes T-cell apoptosis (programmed cell death), which leads to a weakened immune system and an inability to fight infections. ()
Multiple sclerosis
Patients with multiple sclerosis have higher numbers of T cells. CD4+, CD8+, Th17 lymphocytes and interferon-gamma play a major role in the formation of multiple sclerosis lesions in the brain. In addition, CD8+ T lymphocytes can initiate damage to the nervous system. ()
Type 1 diabetes
Cytotoxic T lymphocytes can destroy pancreatic cells that produce insulin, leading to increased blood glucose and the development of type 1 diabetes. In addition, with this disease, the interaction between Th17 and T-regulating lymphocytes is disrupted, with an increase in the number of Th17 in the lymph nodes. ()
Allergies and asthma
An imbalance of two types of immune cells – Th1 / Th2 (predominance of Th2) leads to the manifestation of asthma and allergies . Th2-type cytokines help support the inflammatory response in allergic diseases. ()
Dermatitis
Dermatitis is a chronic inflammatory skin disease. Th2 lymphocytes and their cytokines play an important role in the inflammatory response and may contribute to the development of dermatitis. ()
The information on this site has not been evaluated by any medical organization. We do not seek to diagnose or treat any disease. The information on the site is provided for educational purposes only. You should consult your physician before acting on information from this site, especially if you are pregnant, nursing, taking medications, or have any medical condition.
Rate this article
Average 3.9 Total votes (10)
The relationship between cellular and humoral immunity
Thanks to the release of interleukins, the immune system develops and protects us from harmful influences. Tumor necrosis factor prevents oncological processes, which is one of the most important functions of the body. All this is carried out by T helper cells. Despite the fact that they act indirectly (through other cells), their role in the immune system is very important, as they help organize the body's protective properties.
source