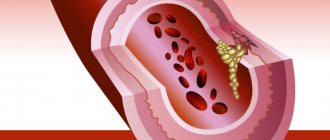
White mononuclear blood cells (monocytes) play the role of protectors in the functioning of the human body. Monocytes belong to a group of special blood cells that fight foreign cells that enter the human blood. Monocytes are formed by the bone marrow; they are quite large in size, and therefore the most active of all cells that provide protection from foreign particles. You shouldn’t take the word “defender” when addressing monocytes as an illustration from an advertisement, where a white cell smashes nasty black viruses with a shield. In fact, this cell absorbs foreign and dead cells, that is, in fact, eats them. When there are too many foreign or dead cells, the blood produces too many monocytes and disease occurs. There may be several causes of monocytosis in adults, but the disease also occurs in children.
Immune system and leukocytes
Leukocytes play an important role in protecting the body and the functioning of the immune system.
Leukocytes are called white blood cells. Although under a microscope the cells are of different shades: pinkish, bluish, purple. The designation was adopted for simplicity, to distinguish it from red blood cells - red blood cells, which give the red color to blood.
More than a hundred years ago, the German scientist Ehrlich developed a classification of leukocytes, which is still generally accepted today. Leukocytes are divided into two groups:
- granulocytes (granular) - contain granules in the cytoplasm;
- agranulocytes (non-granular) - no granules.
Neutrophil granulocyte
Granulocytes, in turn, are divided into:
- neutrophils;
- eosinophils;
- basophils.
Agranulocytes include:
- lymphocytes;
- monocytes/macrophages.
Lymphocytes are divided according to their functional characteristics:
- B cells;
- Killer T cells;
- NK lymphocytes (natural killer cells).
It is important to know! The IS refers to a complex system that unites organs and tissues that protect the body from disease through the identification and destruction of antigens.
There are three levels of IS operation.
- The first level is protected with the help of physical barriers: skin, specific reactions to foreign bodies (sneezing, coughing).
- The second is that if a pathogen penetrates barriers, innate immunity (initially inherent in a living organism) is activated. Reacts to strangers regardless of their characteristics. Forms a person's long-term immunity to a specific pathogen. VIS cells include: neutrophils, natural killers, monocytes, eosinophils, basophils.
B lymphocyte under a microscope
- Acquired immunity is the third protective level. The PI system tailors its response to a specific antigen. The response is stored in immunological memory. PIS provides a fast, strong response. The weapons are lymphocytes (B and T cells).
All leukocytes originate in the bone marrow.
IS organs are:
- Central (bone marrow, thymus gland);
- Peripheral (spleen, lymph nodes, lymphoid tissue and formations (nodes), lymphatic ducts).
Monocyte in company with neutrophil
Monocytes and their functions
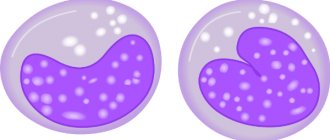
Monocytes are an important part of the innate immune defense. They are larger than all leukocytes - 0.018-0.02 millimeters. The shape is oval. They have one large bean-shaped nucleus, saturated with chromatin.
Produced in KM. Hemocytoblasts are formed first. Then promyeloblasts are formed, transforming into myelomonoblasts. The further stage of development is monoblasts, which are stem cells of monocytic growth of BM. Monoblasts are found exclusively in the BM and never appear in the peripheral blood. After passing the promonocyte stage, they become mature monocytes. The transformation of a monoblast into a monocyte takes about six days. The bulk of the resulting monocytes immediately enters the blood, the remainder turns into BM macrophages.
They move like amoebas - using outgrowths of the cytoplasm. They can migrate outside the blood vessels (extravasation), preferentially migrate to foci of inflammation, places of tissue damage (chemotaxis).
It is important to know! Monocytes circulate in the blood from one and a half to four and a half days, then migrate into tissues. There they become tissue macrophages and live for more than two months.
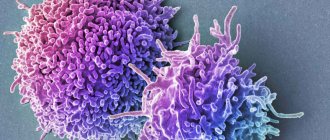
Macrophage
Macrophages are present in almost every organ and tissue. Most are found in the liver (more than half), lungs, and spleen (about 15 percent each).
Phagocytosis scheme
The word macrophages itself literally translates as big eaters. They got their name for their ability to actively capture and digest bacteria, dead cells and other large foreign particles. This phenomenon is called phagocytosis and is the main function of monocytes and phagocytes. Unlike microphages (neutrophils, eosinophils), which are capable of absorbing only small particles and dying after that, macrophages do not die after the completion of the phagocytosis process.
Monocytes differ from neutrophils in that they can phagocytose in an acidic environment. By devouring everything that is foreign, they cleanse the area affected by pathology, preparing it for restoration. If the foreign element is not destroyed, the cells form a limiting shaft around it.
In addition to this function, macrophages present the antigen to T lymphocytes - they stimulate the response to the captured foreigner from the PI. B lymphocytes do not need such a presentation, since they themselves are able to identify a foreign element.
Another function is the activation of cytokine synthesis. They are mediators of protein origin, serving as a kind of alarm signal for representatives of PI (T and B cells). Cytokines attract lymphocytes to the damaged area of the body. Cytokines are released by macrophages and damaged tissues.
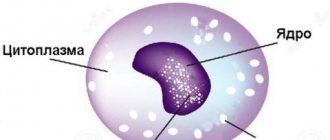
Normal monocytes
The concentration of monocytes is determined by conducting an extended clinical blood test and calculating the leukocyte formula (leukogram). The main indicator is the ratio of monocytes to the total number of leukocytes.
It is important to know! The normal percentage of monocytes is the same in men and women.
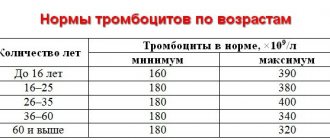
In adults, the norm changes little with age. It ranges from three to eleven percent. Such a wide range is explained by the fact that the concentration of cells can change under the influence of a number of factors (food, time of day, menstrual cycle, etc.).
Normal cell content is different up to 16 years of age. In newborns, the norm varies from three to twelve percent. Two weeks of age – 5-15%. Then the indicators gradually decrease.
There is a measurement of the absolute norm. The number of cells in one liter of blood is determined. The absolute content of monocytes in a healthy adult is 0.09-0.7 × 10⁹ units per liter. The highest absolute number of cells is normally recorded in newborns, 0.19-2.4 ×10⁹.
In the blood of pregnant women, it is allowed to reduce the lower limit of the relative norm to one percent, the absolute figure to 0.04 × 10⁹ due to changes that occur during pregnancy.
Taking a sample for research
Monocytosis: what is it, causes in children and adults, absolute and relative – Vessels Med
One of the most active fractions of leukocytes that take part in the body’s immune defense are fairly large blood cells - monocytes.
They develop in the monocytic germs of the bone marrow hematopoiesis and perform a phagocytic function, therefore they are also known as macrophages and phagocytic mononuclear cells. Simply put, the role of monocytes in the blood and tissues is to absorb foreign bodies (viruses, fungi, bacteria and even tumor cells) that enter the body for various reasons.
Thanks to monocytes, the blood is also cleansed of the remains of destroyed or dead, spent cells.
However, to activate phagocytic activity, a normal, standard number of monocytes is not enough.
Therefore, all kinds of infections or inflammatory processes in the body are accompanied by a quantitative surge in the monocytic fraction in the blood - this condition is called monocytosis.
Factors that provoke an increase in monocytes
Why does a pathological increase in the level of monocytes in the blood occur? The currently known causes of monocytosis can be divided into the following groups:
- infectious (for infective endocarditis, fungal, viral, protozoal, rickettsial infections);
- granulomatous (with various forms of tuberculosis, brucellosis, sarcoidosis, ulcerative colitis, enteritis);
- blood diseases (acute myeloblastic and monoblastic leukemia, lymphogranulomatosis, chronic monocytic and myelomonocytic leukemia);
- oncological (for tumors in any organs);
- systemic (with rheumatoid arthritis, polyarteritis nodosa, systemic lupus erythematosus);
- surgical (monocytosis in this case is most often observed during surgical interventions on the pelvic organs in women and during other operations);
- post-infectious (an increase in monocytes was noticed during the recovery period after a severe infection);
- toxic (in case of poisoning with tetrachloroethane or phosphorus).
Symptoms
Monocytosis refers to those conditions whose clinical indicators cannot be called pronounced symptoms. As a rule, the fact of an increase in the number of monocytes is detected during laboratory blood tests.
Monocytosis in children is especially lethargic, since this category of patients practically does not respond to most manifestations of the condition.
Observant parents may suspect monocytosis in their child if they notice that he has become less active, gets tired more often, and is capricious for no reason.
Such behavior with elevated monocytes is not often observed, but it should attract the attention of parents to the well-being of their child.
This is important for the speedy discovery of the true cause of this condition, which will allow treatment to begin as soon as possible.
In adults, an increase in monocytes can be manifested by the following symptoms:
- fatigue, general weakness;
- subfebrile body temperature (prolonged increase in temperature from 37 to 38 degrees);
- joint pain;
- feeling of pain.
Similar symptoms occur in most infectious (including respiratory) diseases, so talking about diagnosis only on the basis of detected monocytosis is inappropriate.
Types of monocytosis: absolute and relative
Despite the atypicality and rarity of the phenomenon (monocytes do not often increase in the blood without the participation of other leukocyte fractions in the process), monocytosis has 2 varieties or categories - absolute and relative monocytosis.
Characteristic differences in relative monocytosis
In the analysis results received in hand, the patient most often sees the relative value of the number of monocytes, which is determined by the percentage of the number of monocytes to the total number of leukocyte bodies of other fractions (basophils, neutrophils, eosinophils).
Normally, this value is 3-7%, which means that if the level of monocytes is determined to be 8% or more, we are talking about a condition called relative monocytosis.
At the same time, which is the most characteristic sign, the total number of leukocytes in the blood remains at the normal level. That is, against the background of elevated monocytes, the indicators of other fractions, for example, lymphocytes or granulocytes, may be reduced, which means that the balance in the leukocyte formula is maintained. This indicator has practically no diagnostic value.
Features of absolute monocytosis
Absolute monocytosis is characterized by an increase in the absolute number of monocytic cells (over 0.7 × 109 units per liter) with a simultaneous increase in the level of other leukocytes.
This deviation is pathological and requires additional diagnostic procedures to determine its exact causes. The most common causes of absolute monocytosis are infectious and oncological diseases, therefore therapeutic measures should be taken as soon as possible when it is detected.
Treatment
It is impossible to talk about treating monocytosis without eliminating the cause of this condition - there are no medications or folk recipes to reduce the level of monocytes.
To restore normal blood levels, it is first necessary to conduct an in-depth diagnosis, determine the source of inflammation or infection, and, based on these data, prescribe treatment procedures.
If the increase in monocytes is caused by an infectious disease, antibacterial drugs are prescribed, inflammatory processes are cured with appropriate medications, systemic diseases are treated with a whole range of therapeutic measures, and so on.
In order for the diagnosis of monocytosis, especially when it comes to monocytosis in a child, to give accurate results (in children, the level of leukocytes varies depending on the age and characteristics of the body), it is recommended to take blood tests strictly on an empty stomach. Source:
Source:
Why does monocytosis occur and how is it treated in adults and children?
White mononuclear blood cells (monocytes) play the role of protectors in the functioning of the human body. Monocytes belong to a group of special blood cells that fight foreign cells that enter the human blood.
Monocytes are formed by the bone marrow; they are quite large in size, and therefore the most active of all cells that provide protection from foreign particles.
You shouldn’t take the word “defender” when addressing monocytes as an illustration from an advertisement, where a white cell smashes nasty black viruses with a shield. In fact, this cell absorbs foreign and dead cells, that is, in fact, eats them.
When there are too many foreign or dead cells, the blood produces too many monocytes and disease occurs. There may be several causes of monocytosis in adults, but the disease also occurs in children.
What is monocytosis
With various diseases, patients experience increased levels of monocytes in the blood. This phenomenon is called monocytosis.
Any inflammation, virus, or cell death is usually accompanied by a sharp increase in the number of monocytes in the blood.
This means that the normal number of white blood cells can no longer cope with foreign particles and requires help. The activity of immune system cells necessitates a trip to the doctor.
Types of monocytosis: absolute and relative
An increase in the number of immune cells is usually not limited to just an increase in monocytes. Often the analysis also shows a pathological increase in other phagocytic particles. Despite this fact, monocytosis can be absolute or relative. The normal value for men and women is in the range from 3 to 11% or 0.09 – 0.6 * 109 per liter.
What to do if pathology occurs
Naturally, monocytosis is not a cause, but a consequence of a pathological process. Therefore, there is no point in treating him. Its occurrence is a completely adequate reaction of the body to the disease.
A high monocyte count is a kind of litmus test that helps determine that some processes are going wrong.
This means that it is necessary to treat the disease that provokes an increase in the number of these cells.
Source:
Monocytosis in adults and children: causes, types, symptoms
One of the results of a general blood test is the study of monocytes, or rather their absolute (MON#, MO#) and relative numbers (MON%, MO%). A condition in which the content of these cells exceeds the norm is called monocytosis. What is it, what can cause it and how to normalize blood composition, read below.
Monocytes are the largest and longest-living cells of leukocytes, white blood cells, responsible for immunity and blood purity. What you need to know about monocytes:
- They are produced in the bone marrow and released into the bloodstream not fully matured.
- After “birth,” monocytes circulate through the blood for only a couple of days. At this moment they are most active.
- They then enter tissues, where they transform into macrophages.
- In tissues, macrophages monitor cleanliness together with neutrophils (the remaining leukocytes, much smaller in size).
- The main function of monocytes is to destroy pathogenic and foreign cells.
Source: https://elit30.ru/simptomy/monotsitoz-chto-eto-prichiny-u-detej-i-vzroslyh-absolyutnyj-i-otnositelnyj.html
Donating blood for analysis.
A test for leukocytes and monocytes as part of a general blood test does not require special preparation; it is enough to abstain from food (breakfast) for four hours. The optimal time is considered to be morning. You can just drink water. If you have regular tests, you need to take them at the same time.
In children, blood is taken from a finger, in adults, from a vein. Both procedures are simple.
- Capillary blood is collected from the third or fourth finger. First, the nurse wipes the desired area with a swab moistened with alcohol. Makes a shallow incision. The first drop that emerges is not taken for analysis. Then the nurse gently applies pressure and collects the required volume of biological material. After the collection is completed, a sterile napkin is applied.
- In the second case, the health worker tightens the patient’s arm at the level of the forearm with a tourniquet. A special needle is inserted into the vein at the bend to draw the required volume of blood. After completing the procedure, a tampon is applied to the puncture site. The patient needs to hold his arm in a bent position for a while to stop the bleeding.
Both procedures can be called classic. New technologies make collecting biomaterial easier for the healthcare worker and less painful for the patient. For example, vacuum containers for collection, already containing the necessary anticoagulants and preservatives for each type of analysis.
Previously, white blood cell counting was done manually using a microscope. The technique required the laboratory assistant (doctor) to be able to visually identify the types of leukocytes by the shape of the nucleus. To automate the process, special counters with separate keys for all cells were used.
Modern medical technologies today use third-class machines that allow you to set up to hundreds of parameters of the material being studied. However, not all medical institutions are equipped with modern equipment. Therefore, in many of them the analysis is done the old fashioned way. The data obtained is deciphered by a doctor.
Deviations from the norm
The content of monocytes can deviate from the norm both to the lower (monopenia) and upper side. A rare pathology is the complete absence of monocytes. It's called monoMAC syndrome. The syndrome is caused by a genetic defect, which is characterized by the body's vulnerability even to those infections that the normal IS successfully resists.
Note! If monocytes are elevated, monocytosis is diagnosed.
Monocytosis
Symptoms
You can find out about this syndrome in your body based on test results.
But there are certain symptoms that indicate the development of monocytosis:
- general weakness;
- fast fatiguability;
- chronic fatigue;
- body temperature, which does not rise above 37.5° and lasts for quite a long time.
However, it is worth noting that such signs can also appear in other pathologies. Therefore, it is impossible to make a final diagnosis based only on these symptoms.
Classification of monocytosis
The state can be either absolute or relative. Relative monocytosis is recorded when the number of monocytes increases, but other indicators are normal. According to experts, it does not have any particular diagnostic value.
Interesting fact! Absolute monocytosis is diagnosed when monocytes in the blood are increased against the background of an increase in other leukocytes.
There are moderate and pronounced types, although any clear numerical values, as a rule, are not given. Usually the first type is associated with acute infectious diseases, postoperative conditions, the second type with chronic inflammatory processes (pre-leukemia, etc.).
Based on its origin, monocytosis is divided into:
- reactive;
- neoplastic or malignant.
The reactive type is observed in infectious, inflammatory pathologies.
Neoplastic type – myeloproliferative and lymphoproliferative pathologies.
Etiology
A syndrome such as monocytosis has various causes, namely:
- inflammatory and infectious nature of the disease;
- autoimmune pathologies;
- blood diseases;
- leukemia (blood cancer);
- other reasons (genetic diseases and individual characteristics of a person).
When visiting a doctor, he will look for individual factors that influenced the development of this syndrome.
Description of monocytes
Causes
Monocytosis is caused by a variety of reasons - from common ARVI to cancer.
- Monocytes are often increased during convalescence. This term refers to the process of recovery after an illness. Recovery from minor illnesses occurs quickly and unnoticed. After serious illnesses, the recovery process can take quite a long time. After a dangerous lobar pneumonia in a few days. Catarrh of the stomach - digestion may return to normal over several months.
- Typically, an increased level of monocytes is observed in the blood of children after an acute infection.
Characteristic signs of influenza
- Common causes of an increase in the number of monocytes are viral infections, especially in acute form (influenza and ARVI). As a rule, monocytes increase slightly above normal. Their number returns to the original level one to two weeks after the inflammation subsides.
- A different clinical picture is observed with infectious mononucleosis provoked by the Epstein-Barr virus. The disease is characterized by viral persistence, as a result of which an increased number of monocytes in the bloodstream persists for months and even years. Exceeding the norm is moderate.
- Monocytes in the blood are elevated in the following chronic bacterial infections: syphilis, tuberculosis, brucellosis, subacute endocarditis, rickettsiosis.
- The pathogenesis of monocytosis in such bacterial lesions differs from its viral pathogenesis. The reason for the prolonged increase in blood levels is associated with imperfect phagocytosis. Phagocytes capture bacteria, but cannot destroy them within themselves due to the fact that the latter are resistant to the lysosomal enzymes of the former. As a result, the bacterium finds itself surrounded by a peculiar shell in the form of the macrophage itself, which protects its attacks by lymphocytes. Staying in this position does not prevent the bacteria from multiplying, which leads to increased release of cytokines, and as a result, the synthesis of new monocytes with their subsequent transformation into protective shells.
- In very rare cases, monocytosis is a consequence of parasitic infections, such as malaria or cutaneous leishmaniasis.
- The mechanism of monocytosis in systemic inflammatory pathologies of a chronic and non-infectious nature is not entirely clear. The underlying cause of the cell-mediated IS response is not understood. Lymphocytes, macrophages, and mast cells accumulate in organs, forming giant cell granulomas. Macrophages continue to release cytokines and other mediators, thereby maintaining chronic inflammation.
- Monocytes are increased in adults, with Wegener's granulomatosis (systemic necrotizing vasculitis of small arteries and veins with the formation of granulomas of the walls, nearby tissues), sarcoidosis (systemic benign disease with damage to lymphatic, mesenchymal tissue, mainly the lungs). An increase in the number of monocytes in children with pathologies like this nature is associated with intestinal inflammation (Crohn's disease, ulcerative colitis).
Classification of hemoblastoses
- Monocytes in the blood are often elevated in hematological malignancies. This is what malignant blood diseases are called. In hemoblastoses, an increase in monocytes occurs due to malignant degeneration of BM stem cells. Monocytes are greatly increased - their number reaches half of the total number of leukocytes. Monocytes in adults increase mainly in chronic myeloid leukemia (a malignant pathology with predominant damage to the granulocytic lineage). In children, similar monocytosis is observed in lymphogranulomatosis and acute monocytic leukemia.
- Monocytosis is characteristic of collagenosis (diffuse connective tissue diseases). Such diseases include, for example, systemic scleroderma and lupus erythematosus. The reasons for this phenomenon have not yet been precisely established. The number of monocytes during the period of exacerbation is increased, during the period of remission it drops to reference values.
- Monocytes, mainly in children, are slightly increased in genetic neutropenia, when the BM produces a reduced number of neutrophils (childhood agranulocytosis, cyclic neutropenia, etc.). Monocytosis caused by neutropenia is combined with eosinophilia (a greater than five percent increase in eosinophils in the blood compared to normal).
- Quite rare, but still there are cases of monocytosis caused by long-term use of glucorticoids, poisoning with tetrachloroethane or phosphorus, restoration of hematopoiesis in the bone marrow after chemotherapy.
Monocytosis granulopenia what is it – We treat the heart
Monocytosis is a syndrome in which the level of monocytes in the blood increases.
Monocytes are white blood cells that are produced in the bone marrow. They help in the functioning of the immune system. Monocytosis occurs in children, and it can also be diagnosed in adults. This applies to people who have low immunity. If the level of monocytes has increased, this indicates the development of pathology in the body.
The patient needs to undergo diagnosis and appropriate treatment.
It should be noted that monocytosis detected in a pregnant woman in the early stages is considered normal, because during pregnancy, monocytes are the body’s immune defense.
Etiology
A syndrome such as monocytosis has various causes, namely:
- inflammatory and infectious nature of the disease;
- autoimmune pathologies;
- blood diseases;
- leukemia (blood cancer);
- other reasons (genetic diseases and individual characteristics of a person).
When visiting a doctor, he will look for individual factors that influenced the development of this syndrome.
Classification
Monocytosis is divided into two types:
- relative monocytosis;
- absolute monocytosis.
The relative type can be determined by the ratio of the number of monocytes to other leukocytes. In analyses, patients see a relative view. The normal level of monocytes is between 3 and 7%.
In a relative form, the level will be more than 8%. It has a distinctive feature - the number of leukocytes with this type is always normal. If there is an increase in monocytes, then the level of leukocytes decreases.
However, this is not considered in diagnostic methods.
In a newborn, the normal level is considered to be 12%. In the absolute form of the syndrome, the level of monocytes is too high. The number of other leukocytes also increases. When such a change in monocyte levels is detected, then the patient is referred for a full examination. This is the only way to make a correct diagnosis. In the test results, the laboratory technician indicates the absolute value.
Symptoms
You can find out about this syndrome in your body based on test results.
But there are certain symptoms that indicate the development of monocytosis:
- general weakness;
- fast fatiguability;
- chronic fatigue;
- body temperature, which does not rise above 37.5° and lasts for quite a long time.
However, it is worth noting that such signs can also appear in other pathologies. Therefore, it is impossible to make a final diagnosis based only on these symptoms.
Diagnostics
In order to identify a violation of the level of monocytes, a general capillary blood test is prescribed. It must be taken only on an empty stomach.
But to diagnose the pathology that influenced this condition, the following methods are used:
- ultrasonography;
- magnetic resonance imaging;
- computed tomography;
- General analysis of urine and blood.
If necessary, the doctor can prescribe a consultation with specialists.
Monocytosis is dangerous in the blood because immunosuppression begins to develop. This condition must be treated and appropriate preventive measures taken.
If infectious diseases are not treated, various complications may occur. They, in turn, will have a negative impact on existing pathologies. The patient’s general condition will also worsen.
Diagnosed oncology in the later stages also leads to serious consequences. Some become disabled. In addition, deaths are common. Therefore, when the first abnormalities appear in your blood results, you should consult a doctor.
Treatment
If monocytosis is diagnosed, then treatment without getting rid of the cause that influenced this syndrome is impossible. There are no medications or traditional medicine recipes that could reduce the level of monocytes in the blood. Therefore, it is necessary to diagnose the primary disease, and then select the appropriate treatment.
As with any other disease, you should not self-medicate. All medications, dosage and course of therapy are prescribed only by the attending physician. If monocytosis occurs in the blood, this means that a pathology is developing in the body or a relapse of a chronic disease has occurred. To find out what caused such a jump, it is necessary to be fully examined.
You can get rid of this syndrome in the following way:
- Taking immunomodulators. They will boost the patient’s immunity, and the body’s fight against infection will begin.
- A special diet is prescribed, which will contain enough amino acids, complex carbohydrates, microelements, vitamins and healthy fats.
- It is necessary to follow a daily routine.
- Doing physical exercise.
It is also necessary to take walks in the fresh air, ventilate rooms, and carry out wet cleaning more often. This will help maintain your health.
If the syndrome occurs in a child under one year old, this means that he is simply teething. In this case, the doctor prescribes symptomatic treatment. There are cases when absolute monocytosis is diagnosed in adults throughout life. Then treatment is not carried out, because this is an individual characteristic of the body.
Prognosis and prevention
The prognosis of such a syndrome will depend on the primary disease. As a preventive measure, it is necessary to prevent the development of pathologies that activate monocytosis.
MonocytosisICD-10ICD-9DiseasesDB
| D 72.8 72.8 |
| 288.8 288.8 |
| 22713 |
Monocytosis
- increase in the number of monocytes in the blood. It can occur in a variety of diseases, including some types of leukemia (monocytic leukaemias) and infections caused by certain bacteria and protozoa.
An increase in the level of monocytes (monocytosis) can be caused by the following reasons:
- Infections (viral, fungal, protozoal and rickettsial etiology), as well as the period of convalescence after acute infections;
- Granulomatosis: tuberculosis, syphilis, brucellosis, sarcoidosis, ulcerative colitis;
- Systemic collagenosis (systemic lupus erythematosus), rheumatoid arthritis, periarteritis nodosa;
- Blood diseases (acute monocytic and myelomonocytic leukemia, myeloproliferative diseases, myeloma, lymphogranulomatosis);
- Poisoning with phosphorus, tetrachloroethane.
One of the most active leukocyte fractions involved in strengthening the immune system are monocytes, large blood cells. They appear in the bone marrow, in monocytic germs of hematopoiesis and have a phagocytic function; they are also called phagocytic mononuclear cells or macrophages.
Monocytes absorb foreign viruses, bacteria, fungi and even tumor cells that have somehow entered the body.
They cleanse the blood of dead or destroyed cells and their excess residues. But to trigger phagocytic activity, more monocytes are needed than usual. Therefore, during inflammatory processes or infections, monocytosis occurs, that is, an increase in the number of monocytes in the blood.
Causes
There are several causes of monocytosis:
- Inflammation and infection. This is a common reason for the development of monocytosis. The body needs urgent help for immunity, and it begins to produce more monocytes. Tuberculosis and syphilis cause such a surge in the production of monocytes. It happens that monocytosis in children causes teething, but this reaction is quite rare. It happens that with the onset of pathology, abnormalities appear in the blood. To understand that a person has recently suffered an infection, you just need to look at the composition of the blood, where granulopenia also manifests itself. Granulocytes are white blood cells that have a different shape and size. To clarify the diagnosis, the test is repeated after half a month.
- Autoimmune diseases. For unknown reasons, the immune system destroys the body's cells, mistaking them for foreign. In this case, the one who must protect its immunity becomes a threat to the body. Autoimmune diseases are rheumatoid arthritis and lupus.
- Blood diseases. Lymphogranulomatosis, leukemia and mononucleosis themselves affect the number of monocytes in the blood.
- Cancer. Leukemia is one of the most dangerous and incurable cancers, which greatly affects the bone marrow and blood functions. People who have this type of cancer have virtually no immune system defenses.
- Other reasons. Individual characteristics of a child’s body can cause the development of relative monocytosis, as well as hereditary pathologies.
Symptoms
For the most part, people learn about their diagnosis based on the results of a blood test rather than based on symptoms.
But it can still be identified by certain symptoms:
- weakness;
- sudden fatigue;
- chronic fatigue;
- low-grade fever is a temperature of 37–37.5 degrees, which does not subside for a long time, but remains at this level.
But it is worth remembering that not only this disease has such symptoms, so you cannot make a diagnosis based only on them.
Types of disease
Monocytosis has 2 types: relative and absolute. Relative monocytosis is determined by the ratio of the number of monocytes to the remaining leukocytes, that is, neutrophils, basophils and eosinophils.
In most cases, the laboratory technician enters the absolute value into the blood test result form. Patients most often see a relative type of pathology in the analysis: monocytic cells in a normal state range from 3 to 7%, relative monocytosis increases from 8% and above.
It has a characteristic feature - the total number of leukocytes remains at a normal level.
If monocytes increase, then leukocytes or granulocytes decrease. But diagnostics does not take this fact into account.
Absolute monocytosis is characterized by a large number of monocytes, while other leukocytes also increase.
Such a change in monocytes requires a complete examination of the person in order to make an accurate diagnosis.
Why is monocytosis dangerous?
An increase in monocytes in the blood means the development of immunosuppression. This is characterized by the use of prevention or even therapy.
Infectious diseases without pathogenetic and etiotropic therapy can develop into complications and aggravate existing diseases and conditions.
Oncology that was detected late also leads to serious consequences, disability and death. So you need to contact a specialist when the first deviations from the norm of well-being appear.
Treatment of the disease
Treatment of this disease without eliminating the root cause is simply impossible, since there are simply no medications or folk remedies that could reduce the content of monocytes in the blood. To restore hormones to the proper level, you need to conduct a full diagnosis, identify the root cause, and based on the data obtained, treatment is prescribed.
As with other diseases, with monocytosis you cannot self-medicate and prescribe medications yourself, without a doctor’s prescription.
A sharp increase in monocytic cells means that a person is worsening an existing disease or developing a new disease. To find out the exact cause, you should undergo a complete examination of the whole body.
To help the immune system fight infection, doctors prescribe immunomodulators and courses of vitamins. In this case, a person’s diet should include all the necessary amino acids, complex carbohydrates and microelements, healthy fats, and vitamins. It will be equally important to follow a daily routine, that is, go to bed, get up, do gymnastics and eat at the same time.
At the same time, it is important to be in the fresh air every day, periodically do wet cleaning at home and constantly ventilate the premises as often as possible. All this is needed to maintain health.
Only a doctor can make an accurate diagnosis and prescribe the correct treatment.
When babies are teething, symptomatic treatment is required. There is also monocytosis, which is observed in the patient throughout his life. In this case, therapy is not needed, since this is simply a feature of the body.
In order to diagnose the most accurate result, especially in children (since in childhood, leukocytes vary depending on the characteristics of the body and the age of the child), you need to take a blood test exclusively on an empty stomach.
Source: //serdce-help.ru/monocitoz-granulopenija-chto-jeto/
Diagnostics
Monocytosis, as already mentioned, is detected during the calculation of the leukogram. Carrying out this procedure does not seem difficult. Diagnostic difficulties begin after its detection. At the first stage, the doctor studies the patient’s medical record, talks with him, listens to complaints about health problems, and conducts a general examination. All this allows the doctor to draw preliminary conclusions about the possible causes of monocytosis.
Further, depending on the clinical circumstances, additional research is prescribed. It may include a whole range of tests.
- By examining the blood, the presence/absence of virocytes is revealed - lymphocytes, which in their morphological characteristics are similar to monocytes. Their presence is typical in benign lymphoblastosis, although virocytes are present in other viral lesions. The level of autoaggressive antibodies to muscle cells, DNA, topoisomerases, C-reactive protein, and antigranulocyte antibodies is also determined. To determine tumor or surface specific DM markers, immunohistochemical examination and immunophenotyping of cells are performed.
New technologies have significantly improved the accuracy of microbiological tests
- Microbiological studies include culture for microflora, sputum microscopy, serological analysis (SA), enzyme-linked immunosorbent assay (ELISA), polymerase chain reaction (PCR).
- Bacteriological culture of bronchial secretions to identify sensitivity to antibiotics is needed to identify microbes and prescribe antimicrobial therapy. Analysis of sputum under a microscope is done in natural and stained smears to identify macrophages, epithelial cells, microorganisms, leukocyte cells, etc.
Interesting fact! Serum SA makes it possible to determine the presence of various antibodies secreted against infectious agents. The presence of highly specialized antibodies indicates the presence of a particular infection.ELISA is based on the antibody-antigen reaction. This is a technologically advanced method for identifying pathogenic agents.
PCR is a modern method for detecting DNA and RNA of pathogens in any sample of biomaterial.
- Histological examinations are useful for accurate identification of neoplasms. A lymph node biopsy followed by examination of the biopsy is informative for various lymphomas. In particular, Reed-Berezovsky-Sternberg giant cells are found in Hodgkin lymphoma. Very large Langerans cells with eosinophilic cytoplasm in the bronchoalveolar fluid indicate histiocytosis. The detection of a large number of blasts (immature cells) in the BM smear indicates oncohematological diseases.
- X-ray will help in making a diagnosis: sarcoidosis, tuberculosis, histiocytosis. In the lungs, X-rays show in tuberculosis an enlargement of the hilar lymph nodes, and in histiocytosis - bilateral small foci of opacities.
- An increase in the size of the spleen (less often the liver), detected by ultrasound examination of the abdominal organs, is characteristic of brucellosis and benign lymphoblastosis.
Monocytosis and Hodgkin's lymphoma
Hodgkin's lymphoma, or cancer of the lymphatic system, is characterized by Reed-Sternberg cells. The main symptom is swollen cervical lymph nodes. Most often, the disease affects the mediastinal, axillary and cervical nodes, but it tends to spread to other organs, sometimes metastases occur in the spleen and bone marrow.
Most patients are 15-35 years old. The detection of monocytosis in a blood test is usually associated with further diagnosis. Hodgkin's lymphoma requires histopathological examination. However, the prognosis for the disease is generally good and patients have a good chance of recovery.
Treatment
There is no specific therapy for monocytosis. Monocytes can be reduced by treating the disease that caused their abnormal numbers. Depending on the disease, conservative methods of therapy (anti-infective, anti-inflammatory), chemotherapy, and surgery can be used.
Sometimes treatment is not even necessary. A person who had the flu, a week later, for another reason, was tested, which revealed monocytosis. This is natural with the flu. Monocytes will return to normal on their own within a few days.
Antibiotics are irreplaceable, but dangerous when self-medicated
Anti-infective therapy
For bacterial infections of the body, antibiotics are prescribed. The choice of a specific drug, dosage, and duration of treatment are determined by the doctor.
For tuberculosis, anti-tuberculosis drugs are prescribed (rifampicin, isoniazid, kanamycin, etc.). Treatment is long-term, taking a year or more. Drug therapy is complemented by physical therapy.
Most infections of viral etiology do not require antiviral therapy. To recover, you need to stay in bed, gargle and mouth with antiseptic solutions, put vasoconstrictor drops in your nose, and drink plenty of fluids. Nonsteroidal anti-inflammatory drugs (NSAIDs) are sometimes prescribed.
One of the most famous glucocorticosteroids is Prednisolone.
Anti-inflammatory therapy
To relieve inflammation of collagen diseases, which are progressive and recurrent, several groups of drugs are used:
- Glucocorticosteroids, NSAIDs;
- cytostatics;
- gold preparations;
- aminoquinoline derivatives.
In case of exacerbation, plasmapheresis and other methods of blood purification are prescribed.
During remission, radon, hydrogen sulfide, carbon dioxide baths, and medicinal electrophoresis will be beneficial.
Chemotherapy
Used in the treatment of hemoblastoses. The specifics of the treatment course depend on the specific type of hemoblastosis. The common thing is that the patient is placed in a sterile room with increased protection against infections. At the first stage, high doses of cytostatic (antitumor) drugs are prescribed. Then a myelogram is done, if it shows positive dynamics in treatment, maintenance therapy with cytostatics is prescribed.
Chemotherapy can be supplemented by local irradiation of the lymph nodes and spleen, as well as its removal. In addition, blood transfusions are performed and preventive antifungal and antibacterial therapy is carried out.