Pathogenesis
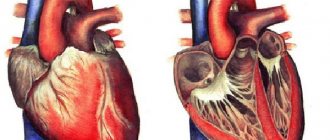
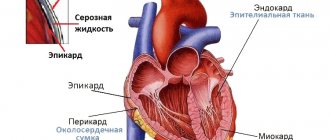
The slit-like space between the visceral and parietal layers of the outer shell of the heart is considered the pericardial cavity. The pericardial sac contains several isolated sinuses or sinuses:
- between the diaphragmatic part of the pericardium and the sternocostal part - anterioinferior;
- between the anterior and posterior parts of the pericardium - transverse;
- between the inferior vena cava and the pulmonary veins at the bottom of the posterior part of the pericardium - oblique.
Hemopericardium is characterized by accumulation of blood in the anterior inferior sinus.
Causes
Most often, hemopericardium develops as a result of:
- pericardial injury (isolated injury or combined injury);
- blunt and penetrating chest injuries (fall, blow);
- closed damage to large coronary vessels and the heart itself.
Blood can penetrate into the pericardial cavity after surgery on the heart and coronary vessels (including as a result of failure of sutures placed on the myocardium).
When performing heart surgery through transsternal access without opening the pleura, the development of growing hemopericardium can be provoked due to the lack of blood outflow into the pleural cavities.
The heart can be perforated and hemopericardium obtained during therapeutic and diagnostic procedures:
- angiography;
- probing of the heart cavities;
- pacemaker implantation;
- central vein catheterization;
- intracardiac injections;
- catheter ablation of additional pathways;
- biopsy of the pericardium and myocardium;
- sternal puncture.
Non-traumatic hemopericardium can develop with rupture of pericardial and coronary vessels, with rupture of an aortic aneurysm , as well as as a result of rupture of a chronic or acute post-infarction aneurysm. Hemopericardium, which develops as a result of cardiac rupture against the background of gummous myocarditis , echinococcosis and abscess , ends in fatal cardiac tamponade.
Pericardial effusion and acute conditions can occur with bleeding diathesis , hemophilia , and primary tumors of the myocardium or pericardium ( angiosarcoma , hemangioma ).
Exudative pericarditis
Exudative pericarditis
Exudative (effusion) pericarditis occurs as a complication or clinical manifestation of various diseases of the heart, lungs and other internal organs. The formation of exudative pericarditis in most cases includes the stage of dry pericarditis. less often, exudate accumulates in the pericardial cleft from the very beginning. The formation of exudate is caused by an increase in the permeability of the vessels of the serous membrane of the heart during the inflammatory process in the pericardium.
The hemodynamic significance of effusion in exudative pericarditis depends on the volume, rate of fluid flow and the adaptive potential of the outer layer of the pericardium. With the slow flow of exudate due to stretching and increasing the volume of the pericardium, intrapericardial pressure and intracardiac hemodynamics do not change noticeably for a long time. With exudative pericarditis, up to 1-2 liters of fluid can accumulate, leading to compression of organs and nerve pathways adjacent to the heart. With the rapid accumulation of effusion and the inability of the pericardium to increase its volume, a significant increase in pressure in the pericardial cavity and the development of cardiac tamponade are observed.
Effusion from exudative pericarditis may eventually undergo organization with replacement by granulation tissue, leading to thickening of the pericardium with preservation of the pericardial space or its obliteration.
Classification of exudative pericarditis
Based on the composition of the inflammatory fluid, they are divided into serous, serous-fibrous, and hemorrhagic. purulent. putrefactive, cholesterol types of exudates. Serous exudate is formed in the early stages of inflammation and consists mainly of water and albumin; serous-fibrinous has a significant number of fibrin strands; hemorrhagic is associated with severe vascular damage and includes a large number of red blood cells; purulent - contains many leukocytes and fragments of necrotic tissue. Putrefactive (ichorous) exudate occurs when anaerobic microflora enters the inflammatory effusion.
According to the clinical course, exudative pericarditis can be acute or chronic; accompanied by the development of cardiac tamponade or without it.
Causes of exudative pericarditis
Exudative pericarditis is rarely observed as an independent pathology; it is usually a private manifestation of polyserositis or a consequence of another disease leading to damage to the pericardium.
By origin, infectious (specific and nonspecific), non-infectious (immunogenic, toxic, mechanical) and idiopathic exudative pericarditis are distinguished. Nonspecific exudative pericarditis is often caused by coccal forms of bacteria (staphylococcus, streptococcus, pneumococcus) and viruses (influenza, ECHO, Coxsackie); specific – pathogens of tuberculosis. typhoid fever. brucellosis and tularemia. Less common are fungal (with candidiasis, histoplasmosis), protozoal (with amoebiasis, echinococcosis) and rickettsial lesions of the pericardium.
Tuberculous exudative pericarditis often develops with lymphogenous penetration of mycobacteria from the mediastinal and tracheobronchial lymph nodes into the pericardium. Purulent exudative pericarditis can develop after heart surgery, with infective endocarditis. against the background of immunosuppressive therapy, with a breakthrough of a lung abscess.
Non-infectious exudative pericarditis is observed in malignant tumors of the pericardium (mesothelioma), invasion and metastases in lung cancer. breast cancer. leukemia lymphoma; allergic processes (serum sickness), uremia in the terminal stage of chronic renal failure; diffuse connective tissue diseases (rheumatism, systemic lupus erythematosus); after irradiation of the mediastinum. Exudative pericarditis can occur in the early stages of myocardial infarction (epistenocardial pericarditis), with hypothyroidism. disorders of cholesterol metabolism (xanthomatous pericarditis).
In many cases, the etiology of pericardial effusion cannot be determined.
Symptoms of exudative pericarditis
Manifestations of exudative pericarditis depend on the rate of fluid accumulation, the degree of compression of the heart and the severity of the inflammatory process in the pericardium.
Initially, the main complaints are heaviness and aching pain in the chest. As fluid accumulates in the pericardial cavity, due to mechanical compression of nearby organs, shortness of breath, dysphagia, “barking” cough, and hoarseness occur. Characterized by swelling of the face and neck, swelling of the neck veins during inspiration, and the gradual development of symptoms of heart failure. A pericardial friction rub is not typical, but can be heard with moderate effusion in a certain position of the patient's body.
There are general manifestations associated with the cause of the development of exudative pericarditis: with infectious genesis - chills, fever. intoxication; In the chronic tuberculosis process, sweating is added. lack of appetite, weight loss, hepatomegaly. With purulent exudative pericarditis, infectious foci in nearby organs and a septic process are possible. Epistenocardial exudative pericarditis occurs within 4 days after myocardial infarction and is manifested by shortness of breath, orthopnea, and swelling of the jugular veins. Rheumatic pericarditis usually develops against the background of severe pancarditis; uremic – accompanied by the clinical picture of chronic renal failure.
In the case of tumor genesis, pericarditis is accompanied by profuse effusion, chest pain, and atrial arrhythmias. development of cardiac tamponade. With a large volume of effusion, patients are forced to take a sitting position, which alleviates their condition.
Diagnosis of exudative pericarditis
Examination data and chest radiography help to establish the diagnosis of exudative pericarditis and differentiate it from other heart diseases (acute myocardial infarction, acute myocarditis). ECG and EchoCG, multislice CT, pericardial puncture.
In patients with exudative pericarditis, there is a slight bulging of the anterior chest wall and slight swelling in the precadial region, weakening or disappearance of the apical impulse, expansion of the boundaries of relative and absolute cardiac dullness, dullness of percussion tone at the angle of the left scapula. The development of cardiac tamponade is indicated by an increase in central venous pressure, a drop in blood pressure, tachycardia with transient arrhythmia, and paradoxical pulsus.
On a radiograph, with a significant volume of fluid, an increase in the shadow and smoothing of the cardiac contour, a change in the shape of the heart (triangular - with long-term chronic exudate), and a weakening of the heart pulsation are observed.
The most accurate and specific method for diagnosing exudative pericarditis, even with a small volume of effusion, is echocardiography. visualizing the presence of echo-negative (free) space between the layers of the pericardium, diastolic separation of the parietal plate and epicardium, thickening of the pericardium. In severe cases, there is a disturbance in the rhythmic movements of the heart, and with tamponade, diastolic collapse of the right chambers of the heart.
An ECG in case of exudative pericarditis reveals a decrease in the amplitude of all waves. Multislice CT confirms the presence of pathological effusion and thickening of the pericardial layers.
To clarify the cause of exudation and verify the diagnosis of exudative pericarditis, a pericardial puncture and a study of the nature of the pericardial fluid are performed (general clinical, bacteriological, cytological, analysis for AHAT and LE cells). It is possible to perform a pericardial biopsy with a morphological examination of the resulting tissue.
Treatment of exudative pericarditis
Treatment of exudative pericarditis is carried out in a hospital, the management of patients is determined by the volume and etiology of the pathology, the severity of hemodynamic disorders. In case of an acute process in the pericardium, monitoring of blood pressure, heart rate, and central venous pressure is necessary. To relieve pain, fever and more rapid resorption of effusion in case of exudative pericarditis, NSAIDs (ibuprofen, indomethacin) and glucocorticosteroids (prednisolone) are prescribed. Active treatment of the underlying disease is carried out using antibacterial, anti-tuberculosis, cytostatic drugs, hemodialysis, etc.
Pericardial puncture for exudative pericarditis is indicated for the evacuation of large accumulations of fluid that do not resolve within 2-3 weeks; with cardiac tamponade and purulent pericarditis. If, after repeated punctures and drainage, the pericardial effusion continues to accumulate rapidly, pericardiectomy is performed.
Forecast and prevention of exudative pericarditis
The main complication of acute exudative pericarditis is cardiac tamponade; in 30% of cases, when inflammation spreads to the atrial myocardium, paroxysmal atrial fibrillation or supraventricular tachycardia may occur. The transition of exudative pericarditis to chronic and constrictive is possible. If cardiac tamponade develops, there is a high risk of death. The prognosis of exudative pericarditis depends on the cause of pericardial damage and the timeliness of treatment; in the absence of cardiac tamponade, it is relatively favorable.
Prevention of exudative pericarditis consists of prevention and early etiopathogenetic therapy of those diseases that can lead to its development. In this regard, the issue of preventing exudative pericarditis is relevant not only for cardiology. but also rheumatology. pulmonology and phthisiology, oncology, allergology.
Symptoms of hemopericardium
The severity of symptoms directly depends on the amount of blood poured into the pericardial cavity and on the degree of compression of the heart.
Significant disturbances in the functioning of the heart and its compression are observed when 150-200 ml of blood enters the pericardial sac. It is this volume of blood that is sufficient to increase intrapericardial pressure, change blood flow in the right atrium, decrease the volume of the left atrium, and reduce cardiac output. Disturbances in blood circulation affect the nutrition of all organs and tissues; the brain reacts primarily. When the heart is compressed, the coronary arteries are compressed, which leads to oxygen starvation with the subsequent formation of ischemia .
With hemopericardium, the following symptoms are observed:
- feeling of heaviness behind the sternum;
- severe weakness, apathy;
- severe shortness of breath;
- sweating;
- pain in the heart area of a burning, dull or pressing nature;
- swallowing disorders;
- fainting states;
- swelling of veins on the face, neck, upper limbs;
- fear of death and increasing anxiety;
- cyanosis of the skin and mucous membranes;
- sudden paleness of the skin.
When palpating the pulse, its weak filling and slight acceleration are noted. Due to heart failure, blood pressure . Auscultation reveals dullness of heart sounds. In certain cases, tones are not heard and the heartbeat is not detected. Percussion reveals an expansion of the boundaries of the heart.
With an increase in blood volume in the pericardial sac, the patient's condition sharply worsens, which is associated with increased tamponade. An accumulation of 400-500 ml of blood is considered extremely life-threatening. This volume of blood can cause cardiac arrest. With a rapid increase in blood in the pericardial sac, the risk of instant death increases (from several seconds to minutes).
With a slight accumulation of fluid in the pericardial cavity, the work of the heart is not impaired, and the patient’s condition remains satisfactory. The chronic course of hemopericardium can be manifested by the following symptoms:
- loss of appetite;
- ascites;
- swelling of the veins in the neck;
- poor tolerance to physical activity;
- increase in liver size;
- difficulty breathing when the body is in a horizontal position.
Symptoms of effusion pericarditis
Clinical pericardial effusion occurs acutely or chronically.
Acute form
Acute effusion pericarditis is characterized by the following symptoms:
- chest discomfort or pain;
- heartbeat;
- dyspnea;
- dry cough;
- Pericardial friction rub is not typical.
Chest pain is usually progressive and lasts for several hours. They have a clear dependence on breathing (pain intensifies with inspiration, especially with deep inspiration), changes in body position, movements, which is very similar to the clinical symptoms of pleurisy (inflammation of the pleura - the outer lining of the lungs). It is also possible for pain to radiate to the left supraclavicular region, shoulder and neck.
In acute effusion pericarditis, fluid accumulates quickly, pressure in the pericardial cavity increases at a high rate, which sharply increases the risk of cardiac tamponade occurring within minutes or hours.
Chronic form
Chronic effusion pericarditis is often asymptomatic because the pericardium has time to adapt to the accumulation of fluid - it gradually stretches. However, even for this scenario, there is an end point when the outer lining of the heart is no longer able to expand. In this case, intrapericardial pressure increases and symptoms of the disease begin to appear, which sooner or later will develop into cardiac tamponade.
Life-threatening symptoms
Before tamponade develops, it is important to note signs of a hemodynamically significant effusion that precedes a life-threatening condition. Its symptoms:
- Muffled heart sounds.
- Disappearance of pericardial friction noise, if it was heard initially.
- Swelling of the neck veins.
- A decrease in systolic (upper) blood pressure during inspiration by more than 10 mmHg during quiet breathing.
If the listed symptoms are detected, the doctor must act very quickly: perform an echocardiogram on an emergency basis and schedule a consultation with a thoracic or cardiovascular surgeon to determine further treatment tactics.
Signs of effusion in localized pericarditis
For encysted or localized pericarditis, other symptoms are also characteristic, which very rarely occur:
- hiccups;
- nausea;
- swallowing disorder;
- hoarseness of voice.
The appearance of these symptoms depends on the location of pericarditis and its pressure on nearby anatomical structures.
Tests and diagnostics
In addition to an objective examination with percussion and auscultation, the patient is prescribed the following basic research methods:
- ECG . There is a decrease in the voltage of the teeth, and signs characteristic of myocardial infarction .
- R-graphy of the chest organs. The image shows smoothness of the cardiac arcs, an increase in the shadow of the heart, and the absence or decrease of pulsation of the contours.
- EchoCG. There is a gap in the echo signal between the pericardium and the walls of the heart. Examination may reveal a small amount of accumulated blood.
Chronic hemopericardium requires dynamic monitoring based on the results of the examination methods described above.
To clarify the origin of the hemopericardium, additional examination methods are prescribed:
- pericardioscopy;
- biopsy ;
- bacterial examination of pericardial fluid;
- cytological analysis of pericardial fluid;
- angiocardiography;
- cardiac catheterization;
- puncture or diagnostic pericardiocentesis .
Additionally, differential diagnosis with other diseases is carried out:
- myocarditis;
- acute exudative (or hemorrhagic, serous-purulent) pericarditis ;
- pneumopericardium;
- non-inflammatory hydropericardium;
- chylopericardium.
Constrictive (adhesive) pericarditis
With constrictive pericarditis, the pericardial layers thicken and grow together, which leads to compression of the heart chambers, limiting diastolic filling.
Clinical picture, symptoms of constrictive pericarditis
Patients complain of increased fatigue, shortness of breath during exercise, loss of appetite, and weight loss. Later, heaviness, pain in the right hypochondrium, and swelling in the legs may occur.
With a pronounced clinical picture, patients have a characteristic appearance: thin with an enlarged abdomen.
You can detect dilatation of the neck veins that do not collapse on inspiration.
On palpation of the abdomen, the liver and spleen are enlarged.
When listening to heart sounds, they may be muffled. In some patients, a pericardial click is detected in diastole, indicating a sharp cessation of filling the ventricles with blood in diastole.
Results of laboratory and instrumental research methods
When significant liver dysfunction develops, a decrease in albumin (protein) levels and an increase in bilirubin may be detected.
The following changes may be detected on the ECG:
- double-humped P waves;
- low amplitude of QRS complexes;
- signs of atrial fibrillation;
- flattening or inversion of the T wave in several leads.
Echocardiography helps diagnose pericardial thickening.
An X-ray of the chest organs reveals enlargement of the left atrium in some patients. In half of the patients with a long course of the disease, a “shell heart” (calcification of the pericardium) is determined in the lateral projection.
Treatment of constrictive pericarditis
The main treatment method is pericardiectomy. This surgical intervention consists of complete removal of the pericardium between the phrenic nerves. In this case, the veins of the heart are freed from the surrounding connective tissue.
With a long course of the disease, involvement of the myocardium in the process, severe heart failure, diuretics and cardiac glycosides are prescribed.
Procedures and operations
If tamponade develops rapidly, emergency surgery is performed to stop bleeding and eliminate the causes of compression of the heart (cardiac tamponade).
In case of injury, a thoracotomy with suturing of the wound in the heart or vessel. Depending on the severity of the injury, the volume of surgical intervention is determined. Various suturing techniques are used to close wounds.
With a rapid increase in hemopericardium, to remove accumulated blood and eliminate compression, the following is carried out:
- Pericardiocentesis (puncture of the pericardial sac) . A needle is inserted into the pericardial cavity for further aspiration of blood.
- Emergency surgical drainage of the pericardial cavity. The puncture is performed under the xiphoid process and a catheter is installed at the site of maximum blood accumulation for drainage.
- Balloon percutaneous pericardiotomy. A special balloon is inserted into the pericardial cavity, which creates a window for blood outflow.
Pericardiocentesis and other minimally invasive surgical operations are performed under the control of ECG and EchoCG. During procedures and manipulations, hemodynamic parameters must be monitored.
In addition to removing accumulated blood and eliminating the causes of bleeding in the acute form of hemopericardium, additional measures are taken aimed at restoring homeostasis and replenishing lost blood volume:
- transfusion of plasma substitutes;
- oxygen therapy;
- transfusion of blood plasma, infusion solutions, leukocytes, erythrocytes and platelets.
Prescription of cardiac medications, nootropic drugs and hemostatic agents is mandatory.
After eliminating the phenomena of hemopericardium, therapy is carried out for the underlying pathology, which provoked the accumulation of blood in the pericardial cavity.
What drugs can be used: their mechanism of action and features of use
Basic treatment of cardiac pericarditis is based on eliminating symptoms. Additionally, medications are prescribed to neutralize the cause of the disease. Let's review the drugs for the basic treatment regimen.
Non-steroidal anti-inflammatory drugs. Anti-inflammatory analgesics: Aspirin, Ibuprofen, Indomethacin, Diclofenac. This group belongs to non-selective inhibitors of cyclooxygenase 1 and 2. Cyclooxygenase is an enzyme that is involved in reducing inflammatory processes. The drugs in question help thin the blood, eliminate the inflammatory process, relieve pain and increase effusion. Admission rules:
- Acetylsalicylic acid should be taken up to 8 times a day, 500 mg. The duration of the course is 14-21 days.
- Diclofenac is taken three times a day, 50 mg maximum. The course of treatment is 21 days.
- Ibuprofen is prescribed 400 mg four times a day.
- Indomethacin – 4 times a day, 50 mg.
These medications should be taken immediately after meals, as they have a negative effect on the stomach, developing gastritis and ulcers.
Non-steroidal anti-inflammatory drugs. Selective cyclooxygenase 2 inhibitors include Lornoxicam, Meloxicam, Celecoxib. The drugs have anti-inflammatory properties. Unlike the previous group, the effectiveness is slightly lower, but the drugs do not have a negative effect on the gastrointestinal tract. Therefore, they are prescribed even for ulcerative manifestations. Rules of application:
- Lornoxicam is produced in tablet and injection form. Tablets are taken twice a day, 8 mg. An injection solution is also used. The duration of the course is 21 days.
- Meloxicam should be taken twice a day, 7.5 mg.
- Celecoxib – 200 mg maximum once a day.
Painkillers. Morphine is considered the most highly effective and fastest acting. If dosages are artificially increased, addiction may develop. Negatively affects the respiratory system. Therefore, strictly adhere to the prescribed doses.
The drug is available in an injection solution that can be administered either intramuscularly or intravenously. The lower the intensity of the pain threshold, the lower the dosage required. The minimum dose is 2 mg, the maximum is 15. The injection solution can be used up to 2 times a day.
Pentazocine is administered intramuscularly or taken orally up to 8 times a day. The maximum dose of solution is 60 mg, tablets – 100. Use orally after eating.
Tramadol is used for intramuscular administration and oral administration. The duration of treatment is 14 days. Take 50 mg tablets twice a day. If the pain threshold is very strong, the dose may be increased to 200 mg. Injections are also administered 2 times a day, but 100 mg maximum.
This group of medications can be addictive, so exceeding the dosage on your own is strictly prohibited.
Many basic therapy drugs have a negative effect on the gastrointestinal tract, so appropriate medications are additionally prescribed. And the main therapy is prescribed depending on the cause of cardiac pericarditis.
Hemopericardium in the fetus
Pericardial effusion in the fetus can occur as a result of impaired intrauterine development of the left ventricle. A diverticulum is formed due to protrusion of the wall of the apex of the left ventricle. Fluid accumulates between the pericardial layers, which impedes the functioning of the fetal heart and can provoke tamponade.
The development of this congenital defect can be prevented through screening, observation by a doctor and timely fetal cardiography . Fluid from the pericardial area may disappear spontaneously and on its own. Otherwise, a pericardial puncture of the fetus is performed.
Pericardiocentesis is considered a very complex manipulation and is performed under ultrasound guidance. The complexity of the procedure lies in the high risk of injury to the pregnant woman and the fetus. Expectant mothers are not recommended to visit a forum where ordinary people share unverified data. You can get all the necessary information from your doctor and decide on further pregnancy .
Forecast
With hemopericardium, the prognosis depends on several factors:
- speed and degree of increase in tamponade;
- the volume of blood accumulated in the pericardial sac;
- timely provision of specialized assistance.
Properly selected therapy can prevent re-accumulation of blood during chronic hemopericardium. In the acute form, the prognosis is unfavorable, because accumulation of 400-500 ml of blood leads to death, caused by cardiac tamponade. The chances of saving the patient increase with timely surgical treatment. According to statistics, in 95-100% of cases, puncture performed on time was successful and guaranteed the patient’s salvation.
Hemopericardium is a serious complication of diseases of the cardiovascular system and chest injuries. At the slightest suspicion of hemopericardium, the patient is hospitalized in a hospital with a cardiac surgical profile. Treatment tactics are determined by the volume of accumulated blood and can be surgical or conservative.