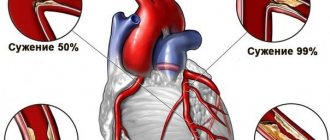
Mitral stenosis is a narrowing of the area of the left atrioventricular orifice, leading to difficulty in the physiological flow of blood from the left atrium to the left ventricle.
Clinically, heart disease is manifested by increased fatigue, interruptions in heart function, shortness of breath, cough with hemoptysis, and chest discomfort. To identify pathology, auscultatory diagnostics, radiography, echocardiography, electrocardiography, phonocardiography, catheterization of the heart chambers, atrio- and ventriculography are performed.
For severe stenosis, balloon valvuloplasty or mitral commissurotomy is indicated.
Etiology
The cause of mitral valve stenosis in 80% of cases is early rheumatism, and the remaining 20% is due to previous infectious diseases (infective endocarditis, cardiac injury, etc.). It forms at a young age and is more common in women. Mitral stenosis is a disease accompanied by dysfunction of the valve located between the left atrium and ventricle. The valve opens in diastole, and through it arterial blood from the left atrium enters the left ventricle.
The mitral valve consists of two leaflets. With mitral stenosis, the valve leaflets thicken, resulting in a decrease in the size of the atrioventricular opening. As a result, blood does not have time to be pumped out of the left atrium during diastole, and as a result, the pressure in the left atrium increases. Therefore, in order to ensure normal blood flow to the left ventricle, a number of auxiliary compensatory mechanisms are activated. In the cavity of the left atrium, the pressure increases (from normal 5 mm to 20-25 mm Hg). Due to the increase in pressure, the pressure gradient between the left atrium and ventricle increases, as a result of which the passage of blood through the opening of the mitral valve is facilitated.
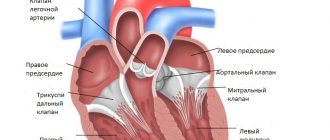
A little anatomy and physiology
The mitral valve (MV) in our heart looks like a dense muscle ring. It is located on the left side of the heart and separates the ventricle from the atrium. The valve consists of two leaflets and does not allow blood to flow back. If it functions normally, blood does not flow back into the left atrium and moves on through the vessels. With pathology of the valves of the heart valve, regurgitation occurs: backflow of blood and impaired circulation inside the cavities of the heart.
As a rule, this disease occurs due to rheumatic pathologies. The formation of the defect is observed in young people, often females. Dysfunction of the MV opening can take different forms:
- mitral valve insufficiency;
- narrowing (stenosis) of its ring.
If the MV is insufficient, its valve flaps weaken and poorly cover the valve opening. With mitral stenosis, the valve ring becomes smaller as its leaflets begin to fuse together. There is a gradual narrowing of the gap that connects the left atrium to the ventricle.
This is interesting!
The main symptoms of mitral stenosis were first described by the French physician Raymond Viessin in 1715.
Pathogenesis
Normally, the area of the mitral orifice is 4-6 square meters. cm, and its narrowing to 2 square meters. cm or less is accompanied by the appearance of disturbances in intracardiac hemodynamics. Stenosis of the atrioventricular orifice prevents the expulsion of blood from the left atrium into the ventricle. Under these conditions, compensatory mechanisms are activated: the pressure in the atrium cavity increases from 5 to 20-25 mm Hg. Art., the systole of the left atrium is lengthened, hypertrophy of the left atrium myocardium develops, which together facilitates the passage of blood through the stenotic mitral orifice. These mechanisms initially make it possible to compensate for the effect of mitral stenosis on intracardiac hemodynamics.
However, further progression of the defect and an increase in the transmitral pressure gradient are accompanied by a retrograde increase in pressure in the pulmonary vascular system, leading to the development of pulmonary hypertension. Under conditions of a significant increase in pressure in the pulmonary artery, the load on the right ventricle increases and emptying of the right atrium becomes difficult, which causes hypertrophy of the right chambers of the heart.
Due to the need to overcome significant resistance in the pulmonary artery and the development of sclerotic and dystrophic changes in the myocardium, the contractile function of the right ventricle decreases and its dilatation occurs. At the same time, the load on the right atrium increases, which ultimately leads to decompensation of the systemic circulation.
Forms of the disease
In official medicine, three stages of the development of the disease are distinguished. They are diagnosed depending on the area of the mitral orifice:
- light form - hole no less than 2 and no more than 4 square centimeters;
- moderate - hole from 1 to 2 square centimeters;
- heavy - the hole is less than 1 square centimeter.
As a rule, a mild form of mitral stenosis occurs without any symptoms. The disease can be diagnosed accidentally - during research for other diseases.
Statistics
Mitral stenosis is a commonly diagnosed acquired defect of the mitral heart valve:
- the disease is detected in approximately 90% of all patients with acquired heart defects;
- 1 person out of 50-80 thousand suffers from this disease;
- in 40% of cases this is an isolated pathology, in the rest it is combined with other anatomical defects in the structure of the heart;
- the risk of clinical manifestations of the disease increases with age: the most “dangerous” age is 40-60 years;
- women are more predisposed to this disease than men: among patients with this defect, 75% of the fairer sex.
Classification of types and degrees
The disease is classified according to 2 bases. As the area of the mitral orifice decreases, 5 successively worsening degrees of the disease are distinguished:
| Degree | Qualitative definition of stenosis | Mitral orifice area (in cm2) | Clinical signs |
| First | minor | more than 3 | no symptoms |
| Second | moderate | 2,3-2,9 | symptoms of the disease appear after physical activity |
| Third | expressed | 1,7-2,2 | symptoms appear even at rest |
| Fourth | critical | 1-1,6 | severe pulmonary hypertension and heart failure |
| Fifth | terminal | the lumen is almost completely blocked | the patient dies |
Depending on the type of anatomical narrowing of the valve opening, the following forms of mitral stenosis are distinguished:
- “jacket loop” type - the valve flaps are thickened and partially fused to each other, easily separated during surgery;
- “fish mouth” type - as a result of the proliferation of connective tissue, the valve opening becomes narrow and funnel-shaped, such a defect is more difficult to surgically correct.
Stages of the disease (according to A.N. Bakulev):
- compensatory – the degree of narrowing is moderate, the defect is compensated by hypertrophy of the heart, there are practically no complaints;
- subcompensatory - the narrowing of the hole progresses, compensatory mechanisms begin to exhaust themselves, the first symptoms of trouble appear;
- decompensation – severe right ventricular failure and pulmonary hypertension, which quickly worsen;
- terminal – stage of irreversible changes with a fatal outcome.
Reasons for the development of the defect and its classification
Etiology of MS:
- Rheumatism (in 80% of cases);
- Infectious, septic endocarditis;
SLE, rheumatoid arthritis, storage diseases, amyloidosis;- Asymmetrical LV hypertrophy in HCM;
- Congenital heart disease (Lutembashe syndrome, patent ductus Botall, myocardial fibroelastosis, coarctation of the aorta, subaortic stenosis);
- Myxoma;
- Thrombus in the left atrium;
- Carcinomatosis;
- Tertiary syphilis;
- Effect of medications (preparations based on wormwood);
- Restenosis after commissurotomy, MV replacement.
Types of mitral stenosis
According to the anatomical characteristics of the narrowing:
- Narrowing like a jacket buttonhole - the valve looks like a jumper with marginal fusion of fibrous valves, a slight shortening of the notochordal threads is visualized;
- Funnel-shaped narrowing like a “fish mouth” - the valve flaps are soldered low to the papillary muscles;
- Combined stenosis.
Degrees of mitral valve narrowing
In a healthy person, the area of the left AV ostium is 4-6 cm2. Clinically, stenosis manifests itself when the area decreases to 2 cm2.
When narrowing to 1 cm2, there is a sharp decrease in tolerance to physical activity. Based on the magnitude of the narrowing of the MV, stenosis is divided into:
- Minimal stenosis;
- Sharp – total area less than 0.5 cm2;
- Pronounced – area from 0.5 to 1 cm2;
- Moderate – narrowing from 1 to 1.5 cm2;
- Minor - the hole area is more than 2 cm2.
Symptoms of mitral stenosis
Symptoms of mitral stenosis are:
- increased fatigue;
- dyspnea;
- constant pain in the heart area;
- cough with phlegm;
- nocturnal asthma attacks;
- pulmonary edema;
- angina attacks;
- repeated bronchitis, bronchopneumonia, rosacea pneumonia;
- bacterial endocarditis;
- bluish-purple color of the cheeks (“mitral blush”);
- cyanosis of the lips;
- heaviness in the stomach;
- peripheral edema;
- swelling of the neck veins;
- dropsy of cavities;
- pulmonary embolism.
Symptoms of mitral valve stenosis tend to worsen as the disease progresses.
General symptoms
At the initial stage, the disease may not show symptoms at all. As the disease progresses, the following symptoms may occur:
- increased fatigue;
- shortness of breath, even with minor exertion;
- cough with blood;
- arrhythmia or tachycardia;
- asthma attacks at night.
At later stages of the disease, signs of mitral stenosis may be more pronounced. Especially the doctor can detect interruptions in the functioning of the heart using auscultation. At a late stage, a person experiences shortness of breath even at rest. Asthma symptoms become more frequent, and not just at night.
A symptom such as shortness of breath is the first and most sure sign of an illness. But, at the same time, such a symptom, as well as hemodynamics, may indicate other diseases. Therefore, you should consult a cardiologist for an accurate diagnosis.
The patient's appearance gradually changes. Cyanosis of the lips and even fingertips is observed. An unhealthy blush may appear on your cheeks. These are also characteristic symptoms of the disease.
Mitral stenosis can be fatal if not treated promptly. According to statistics, this disease leads to death in 40% of cases.
Stages and degrees
Based on the area of narrowing of the left atrioventricular orifice, 4 degrees of mitral stenosis are distinguished:
- I degree – minor stenosis (hole area > 3 sq. cm)
- II degree - moderate stenosis (hole area 2.3-2.9 sq. cm)
- III degree - severe stenosis (hole area 1.7–2.2 sq. cm)
- IV degree - critical stenosis (hole area 1.0–1.6 sq. cm)
In accordance with the progression of hemodynamic disorders, the course of mitral stenosis goes through 5 stages:
- I – stage of complete compensation of mitral stenosis by the left atrium. There are no subjective complaints, but auscultation reveals direct signs of stenosis.
- II - stage of circulatory disorders in the pulmonary circle. Subjective symptoms occur only during physical activity.
- III – stage of pronounced signs of stagnation in the small circle and initial signs of circulatory disorders in the large circle.
- IV - stage of pronounced signs of stagnation in the pulmonary and systemic circulation. Patients develop atrial fibrillation.
- V – dystrophic stage, corresponds to stage III of heart failure
Signs and symptoms
Mild mitral valve stenosis usually does not cause symptoms. Eventually the disease progresses and patients develop symptoms such as shortness of breath and easy fatigue. Patients with atrial fibrillation may experience palpitations (the sensation of the heart beating).
Diagnosis of mitral valve stenosis
The diagnosis of mitral stenosis is established based on the following data.
1. Clinical examination. Noteworthy is the pallor of the skin in combination with cyanotic coloration of the cheeks (“mitral blush”), swelling of the legs and feet, and an enlarged abdomen. Low blood pressure is detected in combination with a weak, rapid pulse. When listening to the chest organs (auscultation), pathological noises and tones (the so-called “quail rhythm”), caused by the flow of blood through a narrowed opening, and wheezing in the lungs are revealed. When palpating the abdomen, an enlarged liver is detected.
2. Laboratory examination methods. A clinical blood test can reveal an increase in the level of leukocytes (white blood cells) due to an active rheumatic process in the body, a violation of the blood coagulation system. In a general urine test, pathological indicators appear indicating impaired renal function (protein, leukocytes, etc.). A biochemical blood test determines indicators of liver and kidney dysfunction (bilirubin, urea, creatinine, etc.). Also in the blood, using immunological studies, it is possible to identify changes characteristic of rheumatism (C - reactive protein, antistreptolysin, antistreptokinase, etc.).
3. Instrumental research methods. — when performing an ECG, changes characteristic of hypertrophy of the left atrium and right ventricle and heart rhythm disturbances are recorded. — daily ECG monitoring allows you to identify possible heart rhythm disturbances during normal household activities that were not recorded during a single ECG at rest. - X-ray of the chest organs reveals congestion in the lungs, a change in the configuration of the heart due to the expansion of its chambers. — echocardiography (ultrasound of the heart) is carried out to visualize the internal formations of the heart, detects changes in the thickness and mobility of the valve leaflets, narrowing of its opening, and allows one to measure the area of narrowing. Also, with ECHO-CG, the doctor determines the severity of hemodynamic disorders (increased pressure in the left atrium, hypertrophy and dilatation (expansion) of the left atrium and right ventricle), assesses the degree of disturbances in blood flow from the left ventricle to the aorta (ejection fraction, stroke volume).
Based on the area of the atrioventricular orifice, minor stenosis (more than 3 sq. cm), moderate stenosis (2.0 - 2.9 sq. cm), severe stenosis (1.0 - 1.9 sq. cm), critical stenosis (less than 1.0 sq. cm) are distinguished. . Measuring this indicator is important in terms of patient management, in particular, determining surgical tactics, since stenosis with an area of less than 1.5 square meters. see is a direct indication for surgery.
- before surgical treatment or in cases of unclear diagnosis, catheterization of the cavities of the heart may be indicated, during which the pressure in the chambers of the heart is measured and the pressure difference in the left atrium and ventricle is determined.
Diagnostics
If these symptoms appear in the body, you should immediately contact a cardiologist to undergo diagnostics and confirm or refute the presence of pathology in the body. The fact is that the manifestation of these symptoms does not mean that the patient has mitral stenosis. Therefore, diagnosing yourself on your own is unacceptable in any case.
Diagnosis of the disease consists of personal examination, auscultation, laboratory and instrumental research methods.
Initially, the medical history is ascertained, when exactly the symptoms began to appear and whether there were any pre-existing factors for this - excessive physical activity, stress, previous surgeries, and so on. The doctor must perform auscultation (listening to the heart). The auscultation method allows a preliminary diagnosis to be made before a more in-depth diagnosis is carried out.
The standard diagnostic program for mitral stenosis includes the following:
- physical examination – personal and family history, auscultation;
- general blood analysis;
- general urine analysis.
Based on the results of this examination, the following procedures may be prescribed:
- blood chemistry;
- coagulogram (blood clotting test).
In addition, instrumental tests are required:
- ECG;
- ECHO (echocardiography);
- X-ray examination of the chest organs;
- transesophageal echocardiography - since the feeding tube passes very close to the heart, this research method allows you to see the outline of the heart and the size of the mitral orifice.
An ECG examination is mandatory if such a pathological process is suspected. Auscultation can only indicate approximately the extent of the lesion. By the way, an ECG study is mandatory if there is a suspicion of disturbances in the functioning of the cardiovascular system.
Auscultation of the heart
In addition to these research methods and consultation with a cardiologist, consultation with a rheumatologist and cardiac surgeon may be necessary. The doctor can give such prescriptions only if the narrowing of the hole has reached a moderate or severe form.
Complications
Regardless of the cause of mitral stenosis, the mechanism of development of this heart defect is the same. There is difficulty in the passage of blood from the left atrium to the left ventricle. As a result, there is an overload of blood volume in the left atrium, and it expands.
This leads to stagnation of blood in the pulmonary circulation, and therefore in the lungs. Stagnation of blood in the lungs leads to shortness of breath. In addition, enlargement of the left atrium may be accompanied by an abnormal heart rhythm (atrial fibrillation). In this case, each fiber of the atrium myocardium beats chaotically.
Like any other heart defect, mitral stenosis may cause weakness of the heart muscle and heart failure. With mitral stenosis, there is a decrease in blood flow in the systemic circulation.
If left untreated, mitral stenosis can lead to the following complications:
- Heart failure.
Heart failure is a condition in which the heart muscle is so weak that it does not adequately pump blood through the body.
With mitral stenosis, less blood enters the systemic circulation from the left ventricle, therefore the tissues receive less oxygen and nutrients.
In addition, there is stagnation of blood in the lungs. All this leads to the development of right ventricular failure, and swelling appears in the legs and abdomen.
- Expansion of the heart.
Mitral stenosis leads to overflow of blood into the left atrium, and over time, into the right chambers of the heart. As a result, all this leads to the appearance of heart failure and stagnation of blood in the lungs.
- Atrial fibrillation.
With mitral stenosis, dilation of the left atrium leads to a disturbance in the heart rhythm - atrial fibrillation. In this case, the atrium begins to contract in a chaotic manner.
- Thrombosis.
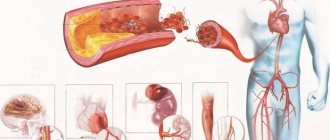
If left untreated, atrial fibrillation can cause blood clots to form in the atrium due to turbulent blood flow through the atrium as it passes through the narrowed opening of the valve.
Blood clots can be carried by the bloodstream to different parts of the body, causing serious problems (such as stroke). One of the effective methods for detecting the presence of blood clots in the atrium is transesophageal echocardiography.
- Stagnation of blood in the lungs.
Another complication of mitral stenosis can be pulmonary edema, a condition in which fluid (plasma) accumulates in the alveoli of the lungs. The result is shortness of breath and sometimes cough with hemoptysis. Source: “heartoperation.ru”
The main problem, which poses a danger to the patient’s health, ability to work and life, is that hemodynamics are disrupted with mitral stenosis. Mitral disease with a predominance of stenosis leads to the fact that oxygenated blood from the pulmonary vein cannot fully flow from the atrium to the ventricle.
Part of it penetrates the right atrium and enters back into the pulmonary circulation. This helps to expand the borders of the heart to the right. The electrical axis shifts, and the muscle effort aimed at pumping blood in the pulmonary circle weakens. In this case, additional loads are placed on the left ventricle due to an increase in the volume in the underlying atrium.
All this can lead to sudden atrial fibrillation. The condition is considered life-threatening and requires immediate defibrillation. In addition, there are phenomena of impaired blood flow, stagnation in the small circle, and venous insufficiency. Blood clots can form that clog various parts of the circulatory system.
Pulmonary embolism is a common cause of death in patients with this diagnosis. In most cases, chronic heart failure develops within several years with signs of oxygen starvation and ischemia of all parts and organs of the body.
Against this background, there is a further deterioration in hemodynamics with mitral stenosis, and fluid stagnation occurs in the lungs. Concomitant pathologies are added. The prognosis for the patient's life in the absence of proper treatment is quite serious.
Symptoms
The clinical picture of mitral stenosis is determined by increased pressure in the pulmonary artery. It occurs due to passive transmission of pressure from the left atrium, as well as through spasm of small pulmonary vessels, swelling of their walls or obliteration.
It can take up to 20 years from the attack of rheumatism to the characteristic signs of mitral stenosis. With a mild course, there are practically no complaints. As stenosis progresses, even minor physical exertion leads to coughing and shortness of breath, which worsen with exercise and in a lying position. More often at night, attacks of cardiac asthma and pulmonary edema occur.
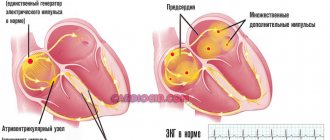
High pulmonary artery pressure, increased workload, and overdistension of the atria and right ventricle lead to electrical instability in the myocardium. This is manifested by various arrhythmias in the form of extrasystoles, paroxysmal tachycardias or atrial fibrillation.
Mitral blush appears - this is a bluish-pink coloring of the lips and cheeks. If you place your palm on the heart area, you will feel vibration - presystolic vibration, or the so-called “cat purr”. Mitral stenosis is characterized by hemoptysis. It is associated with rupture of the pulmonary veins due to high pressure in them. It should be noted that this symptom can occur with pulmonary edema, so its causes should be clearly clarified. Subsequently, congestion in the lungs weakens, but the increased load on the right ventricle causes weakness, heaviness in the abdomen due to an enlarged liver, edema, hydrothorax and ascites. An enlarged and dilated right ventricle creates the preconditions for thrombus formation. Pulmonary embolism is the most common cause of death in patients with mitral stenosis.
Read also Angina pectoris - classification, causes, symptoms, diagnosis, treatment
A persistent form of atrial fibrillation or prolonged paroxysm can cause a blood clot to appear in the cavity of the left atrium. In this case, thromboembolism is already possible in the arterial system of the systemic circulation. The most common targets for such embolisms are cerebral vessels with the development of ischemic strokes.
In 10% of cases, patients with mitral stenosis complain of chest pain. It is associated with pulmonary hypertension or cardiac ischemia under conditions of increased exercise.
Treatment
It is completely impossible to cure stenosis of the left atrioventricular orifice; drug therapy effectively delays progress, but does not interrupt it. As a result, the pathology is eliminated by surgical methods, but at stages when the manifestations of heart failure become obvious and irreversible (dilatation of the right ventricle), the functions of the heart are impaired and begin to complicate the patient’s life.
After surgical intervention at stages 2 or 3 of the disease, it is possible to improve the prognosis and life expectancy of the patient, however, stenosis tends to recover (restenosis, 30% within 10 years).
It is less common to operate at stage 4 - due to complications of cardiovascular failure, it is impossible to significantly improve the prognosis and prolong the patient’s life.
Drug treatment
The purpose of drug treatment for mitral valve stenosis:
- Suspend the progress of pathology (in the early stages).
- Eliminate symptoms of heart failure and oxygen starvation of tissues and organs.
- Prevent the formation of blood clots, the development of infectious complications (infective endocarditis), atherosclerotic plaques, reduce the risk of re-narrowing, restenosis after surgery and thromboembolism.
A complex of drugs is combined based on the stages of stenosis and the severity of symptoms of heart and pulmonary failure.
| Group of drugs, names of drugs | For what purposes is it prescribed? |
| ACE inhibitors (Prestarium, lisinopril) | Reduce blood pressure by blocking the conversion of angiotensin, increase the content of substances that have a beneficial effect on the functions of cardiomyocytes (heart cells) and blood vessels, increase cell resistance in conditions of oxygen deficiency |
| Adrenergic blockers (Corvitol, Coronal, Nebilet) | Normalize heart rhythm, regulate cardiac output, reduce blood pressure |
| Anti-ischemic drugs (nitroglycerin, sustak, nitrong) | Dilate blood vessels, stimulate peripheral microcirculation, enhance metabolism and gas exchange in tissues |
| Cardiac glycosides (digitoxin, digoxin) | Regulates the rhythm and strength of heart contractions |
| Antithrombotic drugs (thrombo, aspirin cardio, chimes) | Mitral valve stenosis is often complicated by thromboembolism; drugs in this group prevent thrombosis by reducing platelet aggregation (sticking together) and thin the blood |
| Anticoagulants (heparin) | Thin the blood, prevent the adhesion of blood cellular elements (platelets and red blood cells) |
| Diuretics (thiazide, indapamide) | In combination with antihypertensive drugs, they regulate blood pressure (lower it) and eliminate severe swelling |
| Antibiotics (penicillin series) | Suppress the development of bacterial microflora, prevent infectious complications in mitral valve stenosis |
All invasive procedures in patients with mitral valve stenosis should be carried out against the background of antibiotic therapy to prevent the development of bacterial infection. When the content of triglycerides and cholesterol is high, drugs from the statin group (lovastatin, atorvastatin) are used to prevent atherosclerotic plaques.
Surgery
When the mitral valve is narrowed, there are many contraindications to surgery:
- critical narrowing of the mitral valve (cardiac ejection fraction less than 20%, orifice area less than 1 sq. cm);
- terminal stage of the defect (increasing changes ending in the death of all tissues of the body);
- any acute processes (infectious diseases, exacerbation of chronic diseases, acute cerebrovascular accidents, myocardial infarction, etc.).
The goal of any operation is to restore hemodynamics, relieve the main severe symptoms, improve blood supply to organs and the patient’s prognosis.
| Name of methods | How to do it |
| Commissurotomy | Excise adhesions, adhesions, scars in the area of the mitral valve that prevent it from functioning |
| Balloon vulvoplasty | A special probe with an expanding balloon at the end is brought to the heart through large vessels. At the site of stenosis, it is inflated several times, enlarging the atrioventricular opening |
| Valve replacement | Used for severe deformations of the mitral valve, it is removed and replaced with an artificial or biological implant |
The risk of developing postoperative complications (early and late) increases depending on the degree of pathology and the severity of symptoms of heart and pulmonary failure (the earlier the operation is performed, the lower the risk):
- thrombus formation at the prosthetic site;
- thromboembolism;
- rejection or destruction of a biological implant;
- infective endocarditis;
- postoperative restenosis (re-narrowing)
Operated mitral stenosis is a good reason for regular examinations and monitoring by a cardiologist for the rest of your life.
Lifestyle with mitral stenosis
For a patient with this disease, it is imperative to follow the following recommendations: eat well and properly, limit the amount of liquid and table salt you drink, establish an adequate work and rest schedule, get a good night's sleep, limit physical activity and eliminate stressful situations, stay in the fresh air for a long time.
A pregnant woman needs to register with the antenatal clinic in a timely manner to decide on prolonging pregnancy and choosing a method of delivery (usually by caesarean section). With a compensated defect, pregnancy proceeds normally, but with severe hemodynamic disturbances, pregnancy is contraindicated.
Complications of the operation
Both in the early and late postoperative periods, there is also the possibility of developing complications:
- infective endocarditis (development of bacterial inflammation on valve leaflets, including biological artificial ones);
- the formation of blood clots as a result of the operation of a mechanical prosthesis with the development of thromboembolism - the separation of a blood clot and its release into the vessels of the lungs, brain, and abdominal cavity;
- degeneration (destruction) of an artificial biovalve with repeated development of hemodynamic disorders.
The doctor’s tactics boil down to regular examination of patients using echocardiography, monitoring the blood coagulation system, lifelong prescription of anticoagulants and antiplatelet agents (clopidogrel, warfarin, dipyridamole, chimes, aspirin, etc.), antibiotic therapy for infectious diseases, abdominal surgeries, and minimal therapeutic and diagnostic procedures in gynecology, urology, dentistry, etc.
Forecast
Stenosis of the left atrioventricular orifice is a severe acquired heart defect. It takes a long time to form; from infective endocarditis (forming factor) to pronounced symptoms of the disease can take an average of 15–20 years. The pathology during this period is completely asymptomatic and is diagnosed accidentally.
With pronounced narrowing of the valve (from 2.2 to 1.7 sq. cm), the life expectancy of 50% of patients is only 5 years (usually death occurs between the ages of 45 and 55 years). Surgical treatment improves the prognosis; the mortality rate in the postoperative period is only 15% over 10 years.
Repeated stenosis is recorded in 30% of patients within 10 years after surgery, which requires additional surgical intervention.
Typical course of mitral valve stenosis
In a typical situation, the first period of the disease remains unnoticed, since compensation for the emerging valve defect by increased work of the left pulmonary valve allows the patient to perform the usual load and not experience discomfort and shortness of breath. The vast majority of patients forget about ARF in childhood and voluntarily stop preventing the recurrence of ARF. Often at this stage, mitral stenosis is diagnosed with competent auscultation of the heart or routine echocardiography. Accidentally detected isolated mitral stenosis, as a rule, has an orifice area of >2.0 cm2 or slightly less, a feeling of lack of air during physical activity, palpitations, and weakness appear. Patients pay attention to a decrease in exercise tolerance (lack of increase in SV in response to physical activity). Significant shortness of breath during physical exertion, sometimes suffocation and a coughing attack are possible - the equivalent of acute circulatory failure. Auscultation of the heart at this stage always reveals mitral stenosis. It is important for the physician to remember that when the mitral orifice area is <1.0 cm2, the transmitral pressure gradient is high.
Due to the turbulent movement of blood on the mitral valve, IE may occur (in 8-10% of patients). In a significantly enlarged left atrium, blood clots form, which leads to embolic syndrome (the most common is embolism of the arteries of the brain, kidney, intestines, lower extremities), and atrial fibrillation. A large left atrium sometimes leads to anisocoria, hoarseness of the voice (compression of the recurrent nerve), and differences in the filling of pulse waves in the left and right radial arteries.
The next (conditionally terminal) period of the disease is marked by the predominance of the clinical picture of right ventricular failure. During this period, due to the addition of relative tricuspid insufficiency, the patient’s condition becomes “relief” and shortness of breath decreases. However, a careful examination will reveal ascites, liver enlargement, right-sided (typically right-sided, left-sided requires excluding pneumonia or searching for other causes) hydrothorax, dense symmetrical cold cyanotic edema of the lower extremities. Pneumonia, embolism, or primary cardiac arrest are the most common causes of death.
In the clinic, passive observation and only fixation of stability is unacceptable. The earliest possible surgical interruption of this stability is the standard of patient management. It is important to remember that there are no specific methods of conservative treatment.