Paroxysmal tachycardia is a disease of the heart muscle that manifests itself in the form of sudden attacks, they are called paroxysms. During attacks, the heart can beat at a rate of up to 220 beats/min. In this case, the rhythm is not disturbed. The heart rate in children can even reach 300 beats. Paroxysms last several seconds or even hours, and can be longer. This disease is quite common and can occur in all age groups of the population.
Paroxysmal tachycardia can be complicated by cardiogenic shock.
Varieties
Paroxysmal tachycardia can be of different types, depending on the area of the conduction system in which the problem occurs. The following types of this disease are distinguished:
- Supraventricular or supraventricular can be atrial or atrioventricular (the problem is localized at the atrioventricular junction).
- Ventricular tachycardia occurs in the tissues of the ventricles and can be unstable or persistent (lasting more than 30 seconds).
There is also a classification of the disease according to the nature of its course:
- acute;
- constantly returnable;
- continuously relapsing.
The last two varieties cause wear and tear of the heart, which, in turn, leads to the development of heart failure. In terms of danger, the ventricular form ranks first. It is this disease that can cause cardiac arrest.
The essence of pathology
Paroxysmal tachycardia is a type of cardiac arrhythmia. It is characterized by sudden attacks of rapid heartbeat, in which the ventricles or atria contract up to 200 times per minute.
Such attacks, or paroxysms, occur under the influence of ectopic impulses. Ectopic impulses are those that occur out of turn or are not generated by the main pacemaker - the atrioventricular node (photo).
Paroxysm occurs and stops suddenly and can last up to several hours. The heartbeat rhythm is correct. Pathology is detected in 20-30% of cardiac patients. During an attack, the heart consumes a large volume of blood, which leads to the formation of heart failure. The more often attacks occur, the faster it develops. According to ICD 10, the disease has code I47.
This is what a normal cardiac conduction system looks like
This is what an ectopic focus of excitation looks like
Classification
Paroxysmal tachycardia occurs in several variants, depending on the location of generation of ectopic impulses and the nature of the course.
Based on the location of impulse generation, the following are distinguished:
- supraventricular - atrial and atrioventricular;
- ventricular
According to the nature of the flow, they are distinguished:
- acute (the attack itself);
- chronic, lasting for years;
- constantly relapsing, leading to the development of cardiomyopathy.
The mechanism for the development of an attack of paroxysmal tachycardia is the principle of re-entry (literally “re-entry”). Paroxysmal AV nodal reentrant tachycardia occurs when an ectopic focus generates an impulse that travels around the heart and back to that focus. This is how a “vicious circle” is formed.
Causes
The causes of PT are the same as for extrasystole. The supraventricular form is caused by dysfunction of the sympathetic department. Ventricular tachycardia occurs against the background of inflammatory or dystrophic heart diseases.
Predisposition to the development of the disease is the presence of extra pathways for conducting impulses - the Kent bundle, the Maheim fibers. The idiopathic form of the disease occurs in newborns and adolescents.
Causes of paroxysmal tachycardia
Even though paroxysmal tachycardia is not a consequence of organic diseases of the heart muscle, it is necessary to search for the cause that led to such problems. There may be several causes of supraventricular paroxysmal tachycardia:
- Additional pathways for nerve impulses are a congenital problem that can make itself felt at any stage of life. There are several varieties of this pathology, among which the most significant are the Kent bundle and the James bundle. Additional bundles cause early reset of the impulse, which leads to premature excitation of the ventricles. Most often, the signal is sent in the opposite direction, circulating between two beams (main and additional). This condition causes supraventricular paroxysmal tachycardia.
- Cardiac glycosides can have a toxic effect on the body, the heart in particular, if an overdose is allowed. Antiarrhythmic drugs can have an arrhythmogenic effect.
- Neurogenic problems, stress and nervous shock.
- Alcohol and drugs.
- Excessive amounts of cardiotropic hormones.
- Problems with the stomach, kidneys, liver.
Ventricular paroxysmal tachycardia is caused by problems of a different kind; here organic heart lesions come to the fore:
- Coronary heart disease, myocardial infarction, which is accompanied by scar replacement of muscle tissue.
- Myocarditis, cardiomyopathy, myocardial dystrophy and congenital heart defects.
- Brugada syndrome, in which proteins mutate at the genetic level. In this case, the process of transporting sodium inside from the myocardial cell is disrupted, contractility decreases and the efficiency of impulse conduction decreases.
Paroxysm may occur due to the following factors:
- stress, strong emotional excitement, physical stress on the body;
- taking alcohol, drugs or smoking;
- hypertensive crisis;
- another dose of glycoside or antiarrhythmic drug.
Diagnostics
Currently, the diagnosis of tachycardia is carried out using several methods. The main one is electrocardiography (ECG). Thanks to the ECG, you can fully assess the work of the heart, identify rhythm disturbances, myocardial ischemia, and arrhythmias. The ECG is performed in standard 12 leads. 24-hour Holter monitoring of cardiac activity is also effective. The advantage is that it is possible to evaluate the work of the heart at rest, during physical activity, during sleep, and during changes in emotions. The next research method is echocardiography (EchoCG).
With echocardiography, it is possible to determine the thickness of the myocardial walls, contractile activity, and the volume of the cavities of the heart. Electrophysiological testing (EPS) is also often used. With this study, it is possible to find out how the impulse propagates through the myocardium, and whether there are conduction disturbances.
Treatment of attacks of tachycardia should be comprehensive. First of all, this is the use of medications that can only be prescribed by a doctor; in no case should you self-medicate
It is very important to follow a certain diet, namely avoidance of alcoholic beverages, strong tea, coffee, and all kinds of energy drinks. It is necessary to avoid conflict situations, quarrels, stress, and be calmer about the people and events around you.
But what to do if an attack of tachycardia occurs, and there are no medications at hand? How to relieve an attack? At first glance, the situation seems hopeless, but at home you can stop the attack. To do this, you need to either open a window or go outside, take fresh air into your lungs and hold your breath. Massaging the carotid artery on the right will also help. To do this, massage the place where the carotid artery divides into the cervical artery in the submandibular region. There are a large number of receptors here; exposure to them can lead to reflex bradycardia, which is what we need.
Another way is to use cold water. The principle of immersion is used. When diving into deeper waters, the fish's heart rate automatically slows down. To do this, you need to immerse your face in cold water.
A technique such as pressing on the eyeballs with the pads of your fingers can also help, but you need to apply pressure very carefully. Similar to the immersion effect, it is recommended to drink cold water, and the colder the better.
Thus, first aid for an attack of tachycardia is based on reflex connections.
Drug therapy for tachycardia attacks comes down to several groups of drugs. The first group includes sedatives. They, in turn, are divided into natural and synthetic. Natural ones include herbal tinctures, herbal remedies, such as persen and valerian. Synthetic ones include phenobarbital, diazepam. Only a qualified specialist can prescribe medications; any unauthorized actions can lead to disastrous results. The same drugs, in different forms, may be contraindicated, so you should not risk your health. The second group of drugs are antiarrhythmic drugs themselves. These include propafenone, cordanone. Each case of tachycardia attack is unique and therefore requires an individual approach. In the presence of chronic heart failure, the administration of cardiac glycosides, for example, digoxin, is indicated. When combined with hyperthyroidism, the prescription of beta-blockers is justified.
Why is paroxysmal tachycardia dangerous?
An attack of paroxysmal tachycardia is dangerous if it is prolonged. In such a situation, cardiogenic shock can develop; it entails a disturbance of consciousness and removes blood circulation in the tissues of the body from the normal state. Acute heart failure and pulmonary edema may also occur. The last problem arises due to congestion in the lungs. The situation is aggravated by a reduced cardiac output. This situation can lead to a decrease in coronary blood flow, which is responsible for supplying the heart muscle with blood. As a result, angina pectoris develops; it is manifested by acute but short-lived painful sensations in the area of the heart muscle.
Symptoms of tachycardia
Signs of paroxysmal tachycardia are not difficult to identify. They are expressed by the following symptoms:
- Angina-type pain in the area where the myocardium is located, radiating to the left arm or jaw.
- Sudden increase in heart rate.
- The manifestation of the clinical picture in the form of “spastic urine” syndrome - during paroxysm, a large amount of urethra is released.
- Patients who have experienced similar ectopic impulses more than once feel an aura of an approaching attack. Often, patients may notice a popping sound in the chest, weakness in the limbs, severe dizziness and a changing heartbeat.
When calling an ambulance, the doctor records the following signs of a person’s impending or beginning dangerous condition:
- Breaking cold sweat
- Pale skin
- Blue lip tint
- The neck veins swell
- Liver – enlarged
- A decrease in urine output is recorded (in the ventricular form)
- Cannot count beats per minute
- Devices record a strong drop in blood pressure
- Paroxysm often causes a state of fainting. This directly depends on changes in blood flow to the brain. Deterioration of the condition is recorded with serious pathological changes in the myocardium.
Symptoms and diagnosis of the disease
Paroxysmal tachycardia has ICD 10 – I47. The Russian system does not contradict this. The presence of paroxysmal tachycardia is indicated by severe symptoms. In some cases, even without special diagnostics, everything becomes clear. From a conversation with the patient, the doctor can identify the following symptoms characteristic of this pathology:
- an unexpected shock to the heart, followed by an increase in heart rate;
- pulmonary edema if a person has heart failure;
- general weakness, malaise and chills;
- body tremors and headaches;
- lump in the throat and changes in blood pressure;
- fainting is rare;
- chest pain, as with angina pectoris, appears with organic lesions of the heart muscle;
- copious urination (light discharge, low specific gravity) indicates the absence of heart failure.
Questioning and analyzing symptoms alone is not enough to make a final diagnosis. An electrocardiogram is required.
Paroxysmal tachycardia may not always be displayed on the ECG. At rest, the device may not register deviations from the norm. In this case, a study will be prescribed with loads that will provoke an attack.
Based on the results of the ECG, one can judge the form of the disease. The characteristics of the P wave are taken into account:
- if it is located in front of the QRS complex, then the focus has an atrial location;
- with a negative value of the tooth, the connection is atrioventricular in nature;
- an expanded QRS of a deformed shape and an unchanged wave is a ventricular shape.
If the problem was not recorded on the ECG and even physical activity did not help in diagnosis, then the doctor may prescribe daily ECG monitoring. In this case, the device will record short attacks, which the patient himself may not take into account. Less commonly, endocardial ECG, ultrasound, MRI and MSCT are recorded.
How to diagnose
Making a diagnosis is not difficult. Characteristic symptoms and objective examination data (HR) are taken into account. The diagnosis is confirmed using an ECG. It needs to be removed precisely at the moment of the attack, so the person undergoes 24-hour monitoring.
With paroxysmal atrial tachycardia on the ECG, the P wave is located in front of the QRS complex and can be positive or negative. If the ectopic impulse comes from the AV node, the wave is located behind the ventricular complex. Signs of an ECG of the ventricular form are a deformed QRS complex with a normal P wave.
An attack of atrial tachycardia on a cardiogram
Treatment of the disease
There is no single correct approach to the treatment of paroxysmal tachycardia. It all depends on its type and the complications present. Let's look at all the available cases:
- The ventricular form requires hospitalization and treatment in a hospital. Only idiopathies without complications do not require such radical measures. The hospital prescribes the administration of an antiarrhythmic drug or electrical pulse treatment if the first option was unsuccessful.
- Paroxysmal tachycardia requires outpatient monitoring by a cardiologist. Prescription of drugs is carried out under ECG control. To prevent the development of ventricular fibrillation, β-blockers are prescribed.
- Surgery for paroxysmal tachycardia is performed only in severe cases that cannot be eliminated with medications. The essence of surgical treatment is the destruction of additional pathways that are used to conduct impulses. Radiofrequency ablation and installation of stimulators/defibrillators can also be performed.
Treatment methods
The effectiveness of treatment depends on the established form of the disease and severity. The selection of drugs and other therapeutic methods takes into account the form of the pathological process identified during diagnosis.
Medications
Paroxysmal tachycardia requires an integrated approach, including the prescription of drug therapy. First of all, drugs belonging to the antiarrhythmic group are prescribed.
The most effective for various forms of the disease are:
- ATP. The drug is intended for intravenous administration. The main substance is triphosadenine. Refers to means that increase metabolic functions and provide energy replenishment. The action of the active components is aimed at stopping paroxysms of supraventricular tachycardia. The solution is prohibited for use in case of myocardial infarction and arterial hypotension. The dosage and course of treatment are calculated individually depending on the nature of the disease. Cost – from 281 rub. per package. There are 10 ampoules in a pack.
- Verapamil. Produced in powder form for the preparation of intravenous solution and capsules. The drug is an antiarrhythmic drug that acts as a slow calcium channel blocker.
Shows high effectiveness in the treatment of various forms of tachycardia. Before use, you should consult a cardiologist, since the drug has multiple contraindications, including myocardial infarction and bradycardia. The dosage and duration of therapy is calculated in each case separately according to the characteristics of the disease. The cost in the form of a solution is from 45 to 80 rubles, in the form of capsules – 17-245, depending on the dosage. - Novocainamide. The drug is produced in the form of tablets and solution for intravenous or intramuscular administration. The main substance is procainamide. The drug exhibits antiarrhythmic properties. Used in the treatment of ventricular tachycardia. The dosage per day for intramuscular administration is determined at the rate of 50 mg/kg of the patient’s body weight. In the form of capsules, the first dose is from 0.25 to 1 g, subsequent doses are from 0.25 to 0.5 g every 3-6 hours. Before use, be sure to read the instructions and consult a doctor due to some restrictions. Cost – from 23 to 200 rubles.
- Cordaron. A pharmaceutical agent aimed at eliminating signs of ventricular and supraventricular tachycardia. It is produced in tablet form, as well as in the form of an injection solution. The active ingredient is amiodarone hydrochloride. The product has multiple contraindications, which is why it is recommended to consult a doctor before use. The specialist determines the dosage and course of treatment depending on the characteristics of the patient’s body, the degree and form of the disease, as well as the form of treatment - outpatient or inpatient. Cost – 156-1550 rubles.
- Digoxin. Prescribed in addition to antiarrhythmic drugs in the treatment of recurrent forms of the disease. Refers to cardiac glycosides that exhibit cardiotonic effects. Available in the form of tablets or intravenous solution. The treatment regimen and dosage are established according to the characteristics of the disease and the age of the patient. The duration of the course is no more than 5-7 days. Cost – 30-55 rubles.
- Celanide. Used as part of complex treatment with antiarrhythmic drugs. The drug is effective in the nodular form of the disease. The medicine is produced in the form of tablets. The active substance is lanatoside C. There are some restrictions on the use of the product, which is why consultation with a doctor is necessary. The daily norm is calculated according to the established form of the disease, as well as the nature of the pathology. The duration is determined by the attending cardiologist, based on the age and other characteristics of the patient. Cost – from 24 rubles. per package.
All drugs are prescribed only according to the indications of the treating cardiologist. Self-prescription and use of funds can lead to various negative consequences and complications.
Traditional methods
Paroxysmal tachycardia can be treated using traditional methods. Traditional methods of treatment are used with a confirmed diagnosis and only with the permission of the attending physician.
Methods:
- Hawthorn berries. Take 100 g of dry fruits of the plant and pour in 1 liter of alcohol. The product is infused for several days and taken 40 drops before meals. The course is until complete recovery.
- Obvoinik (Greek). To prepare the product, you need to take the bark of a tree and grind it to a powdery mass. Then the mixture is poured with 0.1 liter of vodka and infused for several days. After time, the infusion is filtered and taken 5 drops 3 times a day. Use until signs of the disease are completely eliminated.
- Herbal collection. To do this, mix 2 parts of lovage herb and 1 part each of hawthorn flowers, calendula and chicory roots. Mix everything thoroughly, add 1 liter of water and put on low heat. Boil for 1 minute, then leave for 1 hour. The resulting mixture must be filtered and taken in 30 ml. 7 times a day. Use until the disease disappears completely.
- Valerian roots. Pour 2 tbsp into a container. roots of the plant and fill with warm water. The mixture is infused in a dark place for 8 hours, after which it is filtered and taken 1 tbsp. 1 time per day.
- Melissa. To prepare the infusion, take 2 tsp. plants and fill with water. Then the mixture is put on fire and boiled for 30 minutes. The infusion is cooled and filtered, after which it is taken several times a day warm.
- Herbal infusion. For pathology caused by arterial hypertension, the following remedy is recommended. To prepare it, plants such as mint, lemon balm, cucumber and calendula are taken in a ratio of 3:2:2:2. All components are thoroughly mixed. Then take 3 tbsp. the resulting mixture and add a little fragrant rue to it. Everything is poured with 1.5 liters of boiling water and put on fire. The collection must be boiled for 1 minute. and leave for at least 1 hour. The finished product is filtered and consumed 0.5 cups 3 times a day.
Before using one of the methods, you must make sure that you are not allergic to the components of the product.
Other methods
If there is no effectiveness or in more severe cases of the disease, surgical intervention is performed. Conservative treatment is based on radiofrequency ablation. The method consists in completely eliminating abnormal locations of impulses.
Additional treatments:
- Laser exposure - the action of the device is aimed at the destruction of ectopic foci that cause abnormal development and generation of impulses. The course of exposure is determined by the doctor, based on the form and degree of the pathological process.
- Electric current also allows you to remove areas that cause disruptions in the conduction of impulses. In this case, the lesions are exposed to low discharges of electric current. The frequency of courses depends on the severity of the disease. On average, 3-5 procedures are prescribed.
- Effect of temperatures. In most cases, exposure is carried out using low temperatures using a special apparatus.
In some cases, the patient is fitted with a pacemaker that regulates the frequency of heart rhythms and conducted impulses. The effectiveness of the methods depends on the stage and advanced stage of the disease and concomitant drug therapy.
Emergency care for paroxysmal tachycardia
If your loved ones have a similar problem, then you definitely need to know how to relieve an attack of paroxysmal tachycardia. Competent actions will help avoid sad consequences and prevent the development of complications.
- The patient should be reassured and allowed to take a horizontal position if there is weakness in the body and dizziness.
- Access to fresh air must be ensured; to do this, unfasten the collar and remove tight clothing.
- Vagal samples are collected.
- If there is no improvement or if the condition worsens, immediately contact an ambulance.
When to see a doctor
At the first signs of the disease, you should immediately contact a specialist. The disease is treated by a cardiologist or arrhythmologist.
Timely identification of pathology helps to avoid consequences and complications and prescribe effective therapy. The reason for contacting a specialist is short-term or prolonged attacks of rapid pulse and heartbeat, accompanied by a general malaise of the body.
Periodic disruptions (increases) in systolic pressure are also a sign of a developing disease. For any deviations from the norm identified during diagnosis, you must consult a doctor to develop and prescribe a treatment regimen.
A separate danger is posed by a recurrent form of the disease or a disease in the acute stage. The pathology is dangerous to the patient’s health and, in the absence of proper therapy, leads to death.
Complications of paroxysmal tachycardia
This disease is dangerous due to the presence of complications. Their list is given below:
- Ventricular fibrillation is a dangerous problem that can cause cardiac death;
- acute heart failure may be accompanied by cardiogenic shock and pulmonary edema;
- myocardial infarction and angina pectoris can also be provoked by paroxysmal tachycardia;
- existing chronic heart failure can progress and develop.
The condition of the heart and the presence of negative changes in the circulatory system are factors that determine the likelihood of developing heart failure. Particularly dangerous are prolonged attacks that last about a week.
How it manifests itself
A characteristic feature of paroxysmal tachycardia is the sudden onset and end of the attack. It can occur both under load and at complete rest.
The attack has the following symptoms:
- The patient feels the onset of an attack as a jolt in the heart area;
- then the rapid heartbeat itself develops, against the background of which the person feels weakness, dizziness, and tinnitus;
- Neurological symptoms may rarely be observed - clouding of consciousness, impaired speech and motor function;
- with VSD, sweating, nausea, and redness of the skin will be observed.
The attack lasts from several minutes to several hours. Prolonged course leads to hypotension and fainting.
The attack occurs suddenly
Complications
More common in the ventricular form:
- ventricular fibrillation or flutter;
- fibrillation;
- pulmonary edema;
- myocardial infarction.
With long-term paroxysmal tachycardia, chronic heart failure develops.
Prevention of paroxysmal tachycardia
Is it possible to protect yourself from such a diagnosis and avert the likelihood of complications? Of course yes. To do this, you need to follow simple rules that will determine your lifestyle:
- Emotional excitability must be reduced with sedatives.
- Seizures are excluded due to drug therapy, which differs depending on the type of tachycardia.
- A healthy lifestyle is the main rule that underlies the prevention of heart disease. This means a complete, healthy, comprehensive diet without junk food, alcoholic beverages, coffee and tobacco.
- Excess weight is a problem that must be dealt with. Otherwise, heart problems cannot be avoided.
- Cholesterol and blood pressure are indicators that should be normal. They need to be kept under control.
- If attacks occur and there is a high risk of cardiac mortality, a number of medications will be required. These include β-blockers, antiarrhythmics, and antiplatelet agents. Whether the appointment will be lifelong or short-term will be decided by your attending physician.
When such a diagnosis is made, many begin to worry about how they live with paroxysmal tachycardia. If you adhere to the recommendations described above, then life will not be overshadowed by anything. Again, it all depends on the form and degree of neglect of the disease.
Reasons for development
Should be assessed depending on the form of the process.
Supraventricular type
- Cachexia caused by malnutrition or anorexia. Leads to the development of a compensatory mechanism.
- Dehydration. This is especially noticeable during the summer months or in hot climates. In such conditions, even healthy people are susceptible to paroxysms.
- Thyrotoxicosis. Excessive production of thyroid hormones as a result of tumors, inflammatory diseases and poor diet. The process is clearly visible: weight loss occurs, a change in the relief of the neck, bulging of the eyes, and a constant rise in temperature.
- Overdose of cardiac glycosides (Digoxin, tincture of lily of the valley).
- Hypercortisolism in the classic form of Itsenko-Cushing syndrome.
- Smoking and alcoholism. Both one and the other on a long-term basis leads to a change in the nature of the activity of the entire system. At the first stages this may not be noticeable.
- Taking psychoactive substances. Heroin, and, a little less frequently, cocaine leads to complete destruction of the atria. This is the merit not of the opiates themselves, but of the harmful impurities in the “street” drug: washing powder, chalk, homemade anti-inflammatory drugs.
- Neurosis. Causes disruption of central nervous system inhibition processes. In this case, there is pathological stimulation of heart tissue, which is not necessary.
- Stress, physical overload. They provoke the release of catecholamines and corticosteroids (dopamine, cortisol, adrenaline, etc.).
Ventricular type
- Replacement of normal cardiac tissue with connective tissue as a result of a heart attack.
- Ischemic disease.
- Dystrophy of cardiac structures.
- Inflammatory processes, such as endocarditis or myocarditis.
- Acute tissue nutritional disorder.
The causes of the described type are relatively easily determined due to the specificity of the symptoms: shortness of breath, problems with coordination of movements, chest discomfort, tinnitus, fatigue.
Conclusion:
Paroxysmal supraventricular tachycardia is of non-cardiac origin, and the ventricular type is caused by diseases of the heart itself.
At the same time, to start the next attack, one or another trigger factor is needed.
This could be:
- Severe stress, psycho-emotional stress, nervous shock.
- Use of alcohol.
- Smoking.
- Lack of sleep.
- A jump in blood pressure.
- Drinking caffeinated drinks.
- Inappropriate physical activity.
How is the issue of disability resolved?
In the same section, we decided to consider the issue of disability. The criteria for disability are the following:
- CHF 1-2Ast. and higher;
- attacks of paroxysmal ventricular tachycardia, which are accompanied by organic damage to the heart muscle
- paroxysmal tachycardias of the supraventricular and ventricular type.
In the presence of the factors described above, people with paroxysmal tachycardia are considered disabled.
How to help
Before treatment, you must consult a doctor and undergo the necessary examinations. After differential diagnosis and confirmation of the diagnosis, the doctor prescribes treatment. Therapy methods are selected individually for each person, depending on the clinical picture of the disease. It should be remembered that self-diagnosis and self-medication often lead to severe complications and chronic forms of disease. Sometimes a person may need emergency help during an attack. To do everything correctly, you need to know methods that help relieve tachycardia.
First aid at home
In cases where there is a person in the family who is subject to attacks, it is necessary to know how to quickly provide assistance for tachycardia at home. If a person has an attack of tachycardia, it is necessary to take a sitting or reclining position and provide access to fresh air. If possible, it is necessary to take the person outside from the premises. All constricting items of clothing (tight collar, tie, belt) should be loosened or removed. To relieve an attack of tachycardia at home, it is recommended to take a deep breath, hold your breath in your lungs for a few seconds and exhale slowly.
In case of an attack of tachycardia, you should immediately call an ambulance.
For tachycardia, you can massage the artery to relieve negative symptoms.
It is recommended to massage the artery on the right yourself. To do this, you need to know its location and the correct point. A doctor can help with this during a consultation, who will tell you what first aid for cardiac tachycardia is most appropriate. Immersion in cold water (immersion reflex) has a good effect. To do this, fill a basin with cold water and immerse your face in it for a few seconds.
Ambulance
The Chermak-Goering test is considered an effective remedy. To perform this method and stop the tachycardia, you need to mechanically apply pressure to the point where the carotid sinus is located. This point is located at the site of the carotid artery (right). After an attack of tachycardia, continuing pressure is strictly prohibited, as ventricular asystole may develop.
Sometimes for an ambulance, when palpitations begin, the Aschner-Danyini test is used. It involves pressing on the eyeball. To perform the method, you need to take a semi-recumbent position or lie down and massage your closed eyes with your thumbs. Prohibited for use by patients diagnosed with eye diseases, especially myopia.
What should conscripts do?
This is another pressing issue that worries young people and their parents. Are they recruited into the army if they have paroxysmal paroxysmal tachycardia? This diagnosis makes it possible to recognize a young man as unfit for military service, but with some amendments:
- poor health serves as a reason for a delay, which is given for diagnosis and treatment;
- the rapid disappearance of tachycardia symptoms after taking sedatives does not give the right to classify a young man as unfit for military service;
- Accompanying tachycardia with severe cardiovascular diseases allows one to obtain relief;
- the presence of serious disturbances in the functioning of the cardiovascular, nervous or endocrine system, one of the symptoms of which is paroxysmal tachycardia, is also a reason for removal from service.
To summarize, we can say that paroxysmal tachycardia, not burdened by other diseases and complications, is not a reason to refuse military service.
Prevention
There are no specific and specially designed preventive measures.
However, you must adhere to the following recommendations:
- Organizing proper nutrition, including dieting. It is necessary to exclude heavy and fatty foods, and add more fresh fruits and vegetables to the diet.
- The use of prescribed medications to help eliminate signs of the disease. This group includes antiarrhythmic drugs.
- Treat existing diseases, especially cardiac ones, in a timely manner.
- Avoiding stressful situations and psycho-emotional stress. If necessary, it is recommended to take sedatives.
- Quitting bad habits - smoking, alcohol, and other drugs.
It is also recommended to undergo annual preventive examinations with a cardiologist and other related specialists. As a preventive measure, it is recommended to undergo special tests at least once a year to determine the presence of pathology. Diagnostics include daily mounting and the EPI method.
Daily monitoring helps to identify any, even minor, deviations in heart rhythm under various conditions, including the functioning of the organ during rest, sleep, and any physical activity.
The EPI method involves artificially provoking a disease and then administering a drug. The method is considered suitable if there are no changes.
Forecast
If we talk about supraventricular paroxysmal tachycardia, then in 85% of cases the course of the disease is favorable. This result is possible due to lifestyle correction, taking medications prescribed by a doctor, and regular monitoring by a cardiologist. If you do not take such actions, the disease will worsen and provoke the development of complications. Things are not so rosy with the ventricular form of the disease. The level of danger increases in the presence of myocardial infarction. In this case, 40–50% of patients die within a year. To increase the likelihood of a favorable course of the disease, it is necessary to use a surgical treatment method.
Timely consultation with a doctor, undergoing comprehensive diagnostics, strictly following the cardiologist’s recommendations and a healthy lifestyle - all this will help you cope with the problem and live a full life for many years.
How to treat tachycardia with home remedies
Traditional medicine can stop an attack and alleviate a person’s condition. To cure the patient, it is necessary to restore the proportion of electrolytes in the blood. Supraventricular paroxysmal tachycardia is characterized by a serious imbalance. It is necessary to restore the following substances: potassium, calcium and chlorine. This can be achieved through treatment with plant glycosides and herbs. These include: valerian, motherwort, mint, hawthorn and lemon balm.
You can be treated without pills with the following formulations:
- 40 g of lovage roots should be poured with a liter of hot water and strained after eight hours. Drink in small portions throughout the day until the condition improves.
- Pour three glasses of viburnum berries into a three-liter container, then pour two liters of boiling water, close the container, wrap and leave for six hours. The broth is filtered, the fruits are squeezed out, 0.5 liters of honey are added, and the jar is placed in the refrigerator. Drink a third of a glass before meals for a month. Then rest for ten days and resume treatment again. For paroxysmal arrhythmia, a total of three cycles are required.
Pharmacy tinctures of valerian, hawthorn and motherwort are mixed, one bottle each. The composition is placed in the refrigerator, you need to drink three times a day, before meals, a teaspoon.
Causes
This pathology is characterized by a multifactorial nature. This suggests that several provocateurs are needed for its appearance. The main reasons are:
- Against the background of pathological changes in the internal organs, constant irritation occurs. It can be a consequence of diseases of the spine, digestive and respiratory systems.
- Frequent stress can lead to a chronic increase in the concentration of adrenaline in the blood. Because of this, there is an increase in the tone of the sympathetic department.
- Toxic heart damage. May occur due to taking certain medications.
- Dystrophic changes in the myocardium in diseases such as myocarditis, cardiosclerosis, heart defects and a number of severe infections.
- Intoxication with drugs and alcohol, as well as industrial chemicals in acute and chronic forms.
- Congenital or acquired abnormal impulse pathways. This condition can be caused by myocarditis, cardiomyopathy.
The occurrence of PNT in adolescents and children most often occurs without cardiac damage. The causes of this pathology in most cases are:
- Electrolyte metabolism disorders.
- Unfavorable conditions that can be caused by poor ventilation or high humidity in the nursery, constantly elevated body temperature.
- Physical stress or emotional turmoil.
Drug treatment
Treatment of the disease with medications
If the examination reveals paroxysmal sinus tachycardia, the doctor prescribes a number of drugs to the patient that are related to the type of disease and are selected individually.
That is why it is impossible to name universal medications that will suit all patients with this disease. In addition, self-medication can be very dangerous, especially if the patient uncontrollably takes several medications at once. In some cases, these drugs may be mutually exclusive, which can lead to very serious consequences for a person.
For tachycardia that is not complicated by concomitant diseases, the doctor most often prescribes treatment aimed at its main cause - thyroid disease, hypotension, vegetative-vascular dystonia, anemia and other diseases.
Sedatives, beta blockers, potassium preparations, cocarboxylase, anti-inflammatory drugs, and physiotherapeutic procedures are used.
In case of cardiovascular failure, the doctor prescribes cardiac glycosides. It is very important to remain calm to alleviate the patient’s condition, so sedatives can be prescribed for especially nervous and unbalanced patients.
ATRIAL TACHYCARDIA
What types of atrial tachycardia can be distinguished?
What are the electrocardiographic signs of atrial tachycardias?
Atrial tachycardias account for approximately 20% of all supraventricular tachycardias. According to the electrophysiological mechanisms of development, three types of atrial tachycardia are distinguished: automatic, triggered (post-depolarization) and reciprocal (re-entry). Reciprocal atrial tachycardias are more often paroxysmal, and automatic ones are chronic (constant or continuously recurrent). In addition, almost all researchers agree that in children, a violation of automaticity can be considered the predominant cause of the development of atrial tachycardia, and the arrhythmia itself is quite often persistent or chronic, lasting months and sometimes years, and can lead to the development of cardiomegaly.
Electrocardiographic diagnosis and clinical manifestations
Electrocardiographically, atrial tachycardias are characterized by the presence of a P wave, the shape of which usually differs from its morphology in sinus rhythm, located before the QRS complex of a supraventricular type (PR interval less than RP interval). The frequency of tachycardia in adults usually ranges from 140 to 180 beats per minute. With an increase in the frequency of the atrial rhythm, the PR interval may increase, and the P wave merges with the preceding T wave. Deterioration of atrioventricular conduction is sometimes accompanied by the development of second-degree AV block (Samoilov-Wenckebach period) without cessation of tachycardia, which distinguishes atrial tachycardia from most atrioventricular reciprocal tachycardia. Although, based on clinical and ECG data, it is difficult to distinguish automatic atrial tachycardia from arrhythmia developing by the re-entry mechanism, there are also a number of differential diagnostic signs. Automatic atrial tachycardia cannot be caused or stopped by pacing, which is precisely typical for reciprocal arrhythmias. Stimulation of the atria at a rate higher than the rate of automatic atrial tachycardia only temporarily suppresses the arrhythmia; after cessation of stimulation, it resumes.
The first P wave of automatic atrial tachycardia is similar to subsequent P waves. In reciprocal tachycardia, the shape of the atrial extrasystole complex, with which the attack usually begins, differs from subsequent P waves, the morphology of which depends on the location of the impulse circulation. In contrast to arrhythmias caused by the re-entry mechanism, the frequency of automatic atrial tachycardias often gradually increases. This phenomenon in electrophysiology is figuratively called “warms up”. In clinical practice, determining the electrophysiological mechanism of the development of atrial tachycardia is necessary, mainly, only when deciding on the use of cardiac pacing.
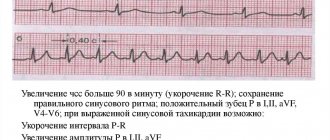
Vector analysis of the atrial ECG complex during tachycardia helps to establish its localization. A positive or biphasic P wave in lead aVL indicates the presence of an ectopic focus in the right atrium, while a positive P wave (“dome and dart”) in lead V1 and a negative one in leads V4-V6 indicate the origin of the arrhythmia from the left atrium.
Atrial tachycardia in some cases must be differentiated from sinus tachycardia. Differential diagnosis can be difficult, but it is important for choosing treatment tactics. Physical activity and vagal maneuvers significantly affect the frequency characteristics of sinus tachycardia and have little or no effect on them in atrial tachycardia. Long-term ECG recording in patients with chronic atrial tachycardia can reveal short periods of sinus rhythm (especially at night), which also helps in differential diagnosis.
Atrial tachycardias often develop in patients with organic heart disease. They are diagnosed with diseases such as coronary artery disease, myocardial infarction, arterial hypertension, heart valve lesions, dilated cardiomyopathy, cor pulmonale, etc. The role of digitalis intoxication, alcohol intake and hypokalemia in the appearance of atrial tachyarrhythmias is known. At the same time, a number of patients (primarily with automatic atrial tachycardia) are not diagnosed with cardiovascular diseases, which could be the cause of the arrhythmia.
In patients with atrial tachycardia, the prognosis is usually determined by the underlying disease. Mortality among them in the absence of other pathology other than heart rhythm disturbances is very low. However, if the arrhythmia occurs with high frequency and for a long time, then even in patients without organic heart damage, cardiomegaly develops, the ejection fraction decreases and congestive heart failure appears.
Treatment. Patients with asymptomatic, rare, short-lived paroxysms of atrial tachycardia do not require treatment. They need to be examined in order to identify the cause of the rhythm disturbance and eliminate it. Pharmacotherapy or non-drug treatment is necessary only for patients with severe attacks of arrhythmia, as well as in its chronic course, even in the absence of hemodynamic disturbances and good tolerance of the rhythm disturbance - due to the high risk of developing cardiomegaly and heart failure. Many cardiologists, when treating such patients, currently give preference not to antiarrhythmic drugs, but to interventional interventions, given their high effectiveness with a small number of complications.
Paroxysms of atrial tachycardia with unstable hemodynamics should be stopped by an EIT discharge of medium energies (50-100 J). Pharmacotherapy for atrial tachycardias has not been sufficiently developed, although, in principle, it is carried out as for other atrial tachyarrhythmias. When hemodynamics are stable, to reduce high heart rate, drugs that worsen atrioventricular conduction are used: calcium antagonists (verapamil, diltiazem), beta blockers, cardiac glycosides, or a combination thereof. The effectiveness of these drugs in terms of restoring and maintaining sinus rhythm is low. If the paroxysm remains, then restoration of sinus rhythm is carried out with the intravenous administration of antiarrhythmics of classes 1A, 1C and III (procainamide, propafenone, amiodarone, sotalol, etc.), and in case of reciprocal atrial tachycardia, pacing can be used for this purpose.
In order to prevent repeated attacks of arrhythmia, according to our experience and literature data, first of all, drugs of classes 1C and III (propafenone, flecainide, encainide, amiodarone, sotalol) should be used; class 1A antiarrhythmics such as quinidine, disopyramide, procainamide are less effective, ajmaline [1, 2, 3]. K. Koike et al. (13), having assessed for several years the effectiveness of 5 antiarrhythmic drugs of various classes, as well as digoxin and its combinations with propranolol, metoprolol, quinidine for automatic atrial tachycardia in children, they came to the conclusion that it is advisable to begin therapy for this cardiac arrhythmia with sotalol, since in 75% of cases it restored sinus rhythm or significantly reduced the frequency of ventricular contractions. If it is ineffective or there are contraindications, according to the authors, it is necessary to use class 3 antiarrhythmics (with the exception of ethmosin, which is ineffective with ALART) or amiodarone. Chronic atrial tachycardia in most cases is difficult to respond to mono- and combined antiarrhythmic therapy. EIT in this case is also ineffective. If antiarrhythmics do not work, in patients with chronic atrial tachycardia it is necessary to reduce the ventricular rate to prevent the development of congestive heart failure. For this purpose, verapamil, diltiazem, cardiac glycosides or even amiodarone are used (combinations of these are possible); in addition, the issue of non-drug treatment should be addressed.
Radiofrequency catheter destruction has been successfully used to treat atrial tachycardia, regardless of the electrophysiological mechanism of its development (automatic, triggered or reciprocal) and localization (right or left atrium). The main indication for radiofrequency catheter destruction is the ineffectiveness of pharmacotherapy or the patient's reluctance to take antiarrhythmic drugs for a long time. In the USA, according to some data, the effectiveness of such an intervention is 75%, and the number of complications is 0.8% [4]. Destruction of the atrioventricular connection with implantation of a pacemaker or its “modification” (partial destruction) is carried out if radiofrequency catheter destruction of the arrhythmia focus is ineffective or impossible. In patients with symptomatic recurrent supraventricular tachycardias that are controlled by pacing, in whom drug treatment and radiofrequency catheter destruction have been ineffective, implantation of an antitachycardial pacemaker is possible. Surgical interventions (isolation, resection or destruction of the arrhythmogenic zone) are now rarely performed in case of failure of radiofrequency catheter destruction or if another cardiac surgery is planned.
Sinoatrial reciprocal tachycardia
One of the forms of atrial tachycardia, which is somewhat different in its clinical course, electrophysiological and ECG diagnostics, as well as pharmacotherapy, is sinoatrial reentrant tachycardia (sinus nodal reentrant tachycardia). The development of sinoatrial reciprocal tachycardia is associated with the circulation of an excitation wave in the sinus node with the inclusion in some cases of a nearby section of the right atrium myocardium in the circulation circuit.
This arrhythmia, as a rule, is paroxysmal in nature, and the heart rate varies from 100 to 220 beats per minute, but in general it is less than with other supraventricular tachycardias, and in most cases does not exceed 150 beats per minute. Attacks of tachycardia in this case are most often short (from 5-20 complexes to several minutes), prolonged attacks are observed very rarely. It is difficult to talk about the true prevalence of sinoatrial reentrant tachycardia. The frequency of detection of sinoatrial re-entry, according to most researchers, ranges from 2 to 10% among all supraventricular tachycardias. There is much less data indicating its wider distribution. Thus, SART was diagnosed in 11 of 65 patients (16.9%) with supraventricular tachycardias who underwent intracardiac electrophysiological study [5].
Since the mechanism of development of sinoatrial reciprocal tachycardia is associated with the re-entry of the excitation wave, it is successfully caused and stopped by extrastimulation of the atria (sometimes even the ventricles) and increased stimulation of the atria. Unlike most atrial tachycardias, the P wave located before the QRS complex is identical or very similar to that recorded during sinus rhythm. The PR interval is shorter than the RP interval. The sudden onset and, in most cases, the sudden cessation of an attack, as well as the possibility of stopping it with vagal techniques (sinus tachycardia and PRT do not stop with them) can serve as important differential diagnostic signs of sinoatrial reciprocal tachycardia.
Since the frequency of attacks with sinoatrial reentrant tachycardia is usually small, and the attacks themselves are short-lived, it may be asymptomatic and do not require treatment. Curative and prophylactic antiarrhythmic therapy for symptomatic sinoatrial reciprocal tachycardia is similar to that carried out for atrioventricular junctional reciprocal tachycardia. Relief begins with vagal maneuvers (Valsalva maneuver, carotid sinus massage), and if there is resistance to them, antiarrhythmics are administered intravenously: ATP 10-20 mg (adenosine 6-12 mg, very quickly) or calcium antagonists (verapamil 5-10 mg or diltiazem 0.25-0.35 mg/kg for 2 minutes). Possible IV use of digoxin, beta blockers and amiodarone. If the patient's condition is unstable (severe anginal pain, significant decrease in blood pressure, cardiac asthma or pulmonary edema), emergency electrical cardioversion is performed (first shock with a power of 50-100 J). Paroxysms of tachycardia can be successfully stopped by cardiac pacing. To prevent attacks of sinoatrial reciprocal tachycardia, verapamil, diltiazem, beta-blockers, digoxin, as well as class III antiarrhythmic drugs - amiodarone and sotalol are primarily used. There are reports of the effective use of radiofrequency catheter destruction of the source of arrhythmia.
Multifocal (chaotic) atrial tachycardia
Multifocal atrial tachycardia is diagnosed in 0.13-0.4% of hospitalized adult patients. It most often affects older people (the average age is more than 70 years). This rhythm disturbance is recorded in approximately equal proportions in men and women. More than 60% of patients with multifocal atrial tachycardia are diagnosed with pulmonary disease. Chronic obstructive pulmonary diseases are the most common. Less commonly, arrhythmia acts as a complication of acute pneumonia, pulmonary embolism, and lung tumors. Medicines such as aminophylline and isoproterenol, used in the treatment of chronic obstructive pulmonary diseases, can play a role in the occurrence of arrhythmia, and also cause its more severe course. In addition to pulmonary pathology, such patients often have cardiovascular diseases (coronary artery disease, hypertension, less commonly valvular heart disease, etc.), accompanied by congestive heart failure. It is important to note that in many cases (according to some data, up to 70%), disorders of carbohydrate metabolism accompany multifocal atrial tachycardia. Mortality among adult patients with multifocal atrial tachycardia is high and ranges from 29-62%. The cause of death is usually severe illness, which affects most patients with multifocal atrial tachycardia, and not the rhythm disorder itself.
Electrocardiographic criteria for diagnosing multifocal atrial tachycardia are:
- the presence of three or more P waves of different morphology in one ECG lead;
- the presence of an isoline between the P waves;
- irregular PR, PP and RR intervals.
The shape of the P waves depends on the location of the ectopic focus of the arrhythmia and changes in intraatrial conduction.
Most often, multifocal atrial tachycardia must be differentiated from atrial fibrillation. In contrast to the latter, with multifocal atrial tachycardia, P waves of changing shape and the isoline between them are clearly visible.
In the management of patients with multifocal atrial tachycardia, an important place is occupied by the treatment of the underlying disease and the correction of factors predisposing to its development: combating infection during exacerbation of chronic pulmonary disease, treatment of heart failure, normalization of acid-base balance and electrolyte disturbances, streamlining the use of beta-adrenergic receptor agonists and methylxanthine derivatives. These measures sometimes make it possible to normalize the rhythm even without the use of antiarrhythmic drugs.
Antiarrhythmic therapy of multifocal atrial tachycardia is associated with great difficulties. Some studies have shown the ineffectiveness of quinidine, procainamide, lidocaine and phenytoin. Cardiac glycosides are also ineffective and often cause intoxication due to the presence of hypoxia and a number of severe metabolic disorders in patients. Electropulse therapy does not restore sinus rhythm and is therefore ineffective.
An analysis of works on antiarrhythmic treatment of multifocal atrial tachycardia shows that the most effective in slowing down, converting the rhythm and preventing relapses of arrhythmia are probably verapamil, beta-blockers (however, they are contraindicated in patients with bronchospastic syndrome) and amiodarone [6, 7, 11]. There is a small number of studies examining the effect of class 1C artriarrhythmics on multifocal atrial tachycardia. Thus, in particular, we describe a case of tachycardia relief due to intravenous administration of flecainide to a 57-year-old patient in whom verapamil, metaprolol, sotalol, disopyramide and some other antiarrhythmic drugs were ineffective [8]; the possibility of successful parenteral and oral use of propafenone for this type of arrhythmia in pediatric practice has been shown [9]. Interesting data were obtained regarding the high stopping effectiveness of magnesium sulfate (in some cases in combination with potassium preparations): in 7 out of 8 patients with multifocal atrial tachycardia (87.7%), sinus rhythm was restored when administered intravenously for 5 hours from 7 to 12 g MgSO4. It should be noted that a decrease in the level of magnesium and potassium in the blood plasma was observed only in 3 patients [10].
Thus, it is advisable to start pharmacotherapy of multifocal atrial tachycardia with beta-blockers (if there are no contraindications to them) or verapamil; if they are ineffective, use amiodarone and class 1C antiarrhythmics, and to relieve arrhythmia, intravenous administration of magnesium sulfate is also possible.
Features of relieving an attack
In adults
In adults, attacks of tachycardia are often caused by external causes, such as stress or physical activity. If we clearly grasp such a connection, then there is nothing to worry about: we simply calm the person down and let him rest.
If an attack occurs at rest, suddenly, you need to immediately sound the alarm and call an ambulance. This may be the first time a rhythm disorder has arisen, and it is very dangerous.
It is especially unpleasant when such attacks occur in young, apparently healthy men: unfortunately, in such situations, sudden cardiac death may develop.
If we understand that the attack is serious, then we do not try to relieve it ourselves, but immediately call an ambulance.
We can only provide minimal first aid, and then emergency care is provided by doctors using ECG and special medications.
In pregnant women
The main feature of pregnant women: they are regularly examined. As a rule, if they have hidden heart problems, the attending physician will find out about this and give appropriate recommendations.
In such situations, an attack of tachycardia is not an unpleasant surprise: the woman is informed in advance that this can happen and what first aid should be provided to her.
If a woman is healthy, and according to the results of a heart examination, everything is fine, then most likely her attack of tachycardia is caused by excessive emotional or physical stress. Again, you need to try to calm down and relax. If this does not help and the condition worsens, you should immediately call an ambulance.
It should be remembered that pregnant women should absolutely not take a number of medications, as they can have a negative effect on the fetus. Therefore, the general recommendation that we do not give victims any medications on their own without a doctor’s prescription becomes even more relevant here.
In older citizens
In the elderly, attacks of tachycardia are usually associated with heart disease. Therefore, if this is not the first time this happens, then we strictly perform the actions that the doctor previously recommended to us.
And then, if the condition has returned to normal, the next day we seek medical help as planned. If it was not possible to relieve the attack on your own, then we call an ambulance.
If tachycardia suddenly appears for the first time, then it is better not to delay calling an ambulance. The situation can be extremely serious.
Help for children
Fortunately, tachycardia in children, as a rule, is physiological. The attacks occur in response to stress and quickly go away on their own. Children simply don’t notice many of them.
Their appearance is especially typical in adolescence, when the body undergoes restructuring, and the appearance of short-term rhythm disturbances is normal.
In general, assistance to children during an attack of tachycardia is no different from that of adults. The dosage of drugs will be less, but this is the concern of the pediatrician. Parents should not self-medicate their child.
The main advice when tachycardia appears in a child: do not panic ahead of time. Serious heart disease in childhood is rare. However, just in case, it is better to get examined in the future - it will be calmer.
Tachycardia symptoms
Most often, an attack of tachycardia develops very quickly and without warning. A person may not even notice it until the heart rate reaches extremely high numbers. For the vast majority of people, a certain malaise is felt already at 110 beats per minute. The feeling of a frightening heartbeat prevents you from concentrating on work, and severe shortness of breath and dizziness occur with the slightest physical exertion.
Objectively, symptoms are determined by measuring the frequency and strength of pulsation of the vessels in the wrists and the carotid arteries in the neck. In addition to palpation of the pulse, with strong tachycardia, pulsation is also noticeable to the naked eye. Such pulsation in the carotid arteries, for example, is normally invisible. This phenomenon is called the “carotid dance.”
An important role is played by auscultatory listening to heart sounds and determining the pulse on the wrists at the same time. Such a study is carried out to determine the nature and completeness of blood flow. A characteristic symptom of tachycardia is the “pendulum rhythm” (although some authors compare it with a metronome) - the first and second tones are practically indistinguishable.
Another symptom of tachycardia is wetness of the skin, sweating even in the absence of physical activity in a normally ventilated area. This is due to the need to speed up water exchange through the skin, since the kidneys cannot function normally with accelerated blood flow.
For ventricular tachycardia, a characteristic symptom is a heart rate per minute from 149 to 189, and for the supraventricular form - 190-240.
In addition, with high heart rates, the need of the heart muscle for oxygen and the specific energy source ATP increases. In people suffering from coronary artery disease, tachycardia can aggravate the course of the disease and be complicated by myocardial infarction.
Tachycardia often occurs in combination with other symptoms, such as angina.
Angina is an attack of heart pain that comes and goes suddenly. The pain can be of a very diverse nature: dagger-like, pressing, diffuse. Often spreads to the left arm, left subscapularis, or left hypochondrium. Pain aggravates a person’s moral state and can cause severe fear, which will provoke increased tachycardia (due to the release of adrenaline).
To determine the severity of the condition and possible complications, the time-tested method of electrocardiography is used. Based on electrocardiogram readings, an experienced specialist can determine in which part of the myocardium the pathological focus of excitation occurs. And also on the ECG you can see early or late signs of necrosis of the heart muscle.
Diagnostic measures
- Taking anamnesis (simultaneously with diagnostic and therapeutic measures);
- Examination by an emergency medical technician (paramedic) or a medical specialist from a visiting emergency medical team of the appropriate profile;
- Registration of an electrocardiogram, decoding, description and interpretation of electrocardiographic data;
- Monitoring of electrocardiographic data;
- Pulse oximetry;
- General thermometry.
For unstable hemodynamics:
- Diuresis control;
For anesthesiologists and resuscitators:
- Control of central venous pressure (in the presence of central venous access).