Normally, the human heart contracts rhythmically, after systole (contraction) comes diastole (relaxation).
Any disturbance of the heart rhythm (its rhythm, the duration of pauses between systole and diastole, additional contractions, etc.) is called arrhythmia.
The appearance of additional defective heart contractions - extrasystoles - is a pathology of the heart rhythm and can disrupt the functioning of the heart.
Supraventricular extrasystole - what is it, is it dangerous and why, what consequences can rare single or frequent attacks lead to?
What it is
Extrasystole occurs due to the appearance of an ectopic (abnormal) focus of trigger activity in the myocardium (heart lining) or its parts. Depending on the site of excitation, supraventricular (supraventricular - atrial and from the atrioventricular septum) and ventricular extrasystoles are distinguished.
The term “supraventricular” means that additional contraction occurs in the upper - supraventricular - part of the heart, that is, in the atrium or the septum between the atria and ventricles (antiventricular septum).
What to take for ventricular extrasystole
For extrasystoles that occur in the ventricles, take sedatives, antiarrhythmic drugs or a combination of 2 drugs. In asymptomatic cases, no medication is required. For single extrasystoles, diet, lifestyle changes, physical activity, sedatives and beta-blockers are recommended.
Drug of choice
The drug of choice for ventricular extrasystole is often a tranquilizer. It can be of plant origin - extract of valerian, hawthorn, motherwort, Fitosed, Persen, Novo-Passit. For neuroses and vegetative-vascular dystonia with a crisis course, synthetic drugs are also used - Afobazol, Clonazepam or Bellataminal.
How to treat single
For the treatment of single extrasystoles it is recommended:
- a diet rich in foods with potassium - dried apricots, baked potatoes, mushrooms, nuts, legumes, dried fruits, seaweed;
- cessation of smoking, abuse of coffee, diuretics, laxatives, alcohol;
- dosed physical activity - swimming, walking, light running (in the absence of contraindications);
- soothing - peony tincture, Corvalol phyto, Valocordin.
- beta blockers - Atenolol, Anaprilin.
Who has it?
Supraventricular extrasystole (SE) occurs in 60-70% of people . Normally, it can also occur in clinically healthy patients.
The presence of supraventricular extrasystole (SVES)
does not mean that a person is sick.
SE is more often registered in adults and older children , since young children are not yet able to describe their sensations and do not really understand what is happening to them.
In newborns and young children, supraventricular extrasystole is detected during an ECG during medical examination, general examination, or in connection with an alleged disturbance in the functioning of the heart (congenital defects, a sharp deterioration in the child’s condition in the absence of external factors).
Causes and risk factors
Supraventricular extrasystole can be idiopathic, that is, it occurs for no apparent reason. It occurs in practically healthy people of any age.
In middle-aged people, the main cause of SE is functional:
- stress;
- tobacco and alcohol;
- abuse of tonic drinks, especially tea and coffee.
SE of organic origin appears due to myocardial damage as a result of coronary heart disease (CHD), inflammation, dystrophy and manifestations of cardiosclerosis.
In the elderly, an organic cause of SE is more common due to an increase in the incidence of coronary artery disease, cardiosclerosis and other heart diseases with age. In such patients, there are profound changes in the heart muscle: areas of ischemia, dystrophy or necrosis, sclerotic areas, due to which electrical heterogeneity is formed in the heart muscle.
Organic causes can be divided into 5 groups:
- Heart diseases:
- acute myocardial infarction;
IHD;
- heart defects, congenital and acquired;
- high blood pressure;
- chronic heart failure;
- cardiac myocarditis (what is it?);
- cardiomyopathy.
- Endocrine system diseases:
- adrenal diseases;
- hyperthyroidism or thyrotoxicosis;
- diabetes.
- Long-term use of heart medications, including:
- glycosides;
- medications for cardiac arrhythmia;
- diuretics.
- An imbalance of electrolytes in the body is an imbalance of sodium, potassium and magnesium.
- Insufficient oxygen supply due to bronchitis, anemia, asthma, sleep apnea.
In young children, supraventricular extrasystole often develops due to congenital heart defects and endocrine diseases. In adolescence, stress, poisoning from tobacco, drugs and alcohol are added to them.
How to get rid of extrasystole forever
To get rid of extrasystole forever, patients without heart disease need to:
- make lifestyle changes - sleep at least 8 hours, stop working at night and shift work, and smoking;
- avoid physical, mental and emotional overload;
- stop drinking coffee, energy drinks and alcohol;
- reduce the use of drugs that can disrupt the heart rhythm (vasoconstrictor nasal drops with constant use, tonics, psychotropic drugs, potassium-removing diuretics, laxatives);
- complete a full course of treatment for the disease that caused the extrasystole;
- At least 2 times a year, a complete examination by a cardiologist is necessary, and, if necessary, an examination by a neurologist or endocrinologist.
Classification and types
Supraventricular extrasystoles differ in several ways.
According to the location of the source of excitation:
- atrial – located in the atria, i.e. upper parts of the heart;
- antrioventricular - in the atrioventricular septum between the atria and ventricles.
According to the frequency of extrasystoles in 1 minute:
- single (up to 5 additional contractions);
- multiple (more than 5 per minute);
- group (several extrasystoles one after another);
- doubles (2 in a row).
By the number of foci of excitation:
- monotopic (1 lesion);
- polytopic (more than one focus).
By appearance:
- early (occur at the time of atrium contraction);
- medium (between contraction of the atria and ventricles);
- late (at the moment of contraction of the ventricles or with complete relaxation of the heart).
By order:
- ordered (alternating full contractions with extrasystoles);
- disordered (lack of pattern).
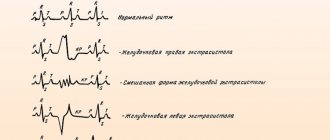
Signs of a problem on the ECG
- Early appearance of the P wave on the graph.
- Premature appearance of the QRST complex.
- The distance between the indicated indicators is 0.8-0.11 s.
- Peak polarity deviation.
- Small compensatory pause.
Manifestations should be assessed by a cardiologist and a specialist in functional diagnostics. If you have doubts about the competence of doctors, you should get a second opinion.
Symptoms and signs
Often supraventricular extrasystole is asymptomatic , especially if its origin is due to organic causes.
Patients may complain of strong tremors and beatings of the heart, a feeling of constriction in the chest, and a feeling that the heart has stopped.
Extrasystoles of functional origin are characterized by neuroses and autonomic disorders : a feeling of lack of air, anxiety, sweating, fear, pale skin, dizziness, weakness.
In children, supraventricular extrasystole often occurs without symptoms. Older children complain of fatigue, dizziness, irritability, and a feeling of “upheavals” of the heart.
In patients with an organic cause of SE, arrhythmias appear less in a supine position (the patient feels better) and more strongly in a standing position.
Patients whose cause of SE is functional feel better in a standing position and worse in a lying position.
Symptoms
Patients are often unaware of the presence of extrasystole. If arrhythmia is caused by heart pathologies, then it will have vivid manifestations. Most people with this diagnosis complain of:
- Feeling that the heart is not working properly. In a normal state, a person does not feel the heart beating. But sometimes it seems that the heart is turning over inside or jumping. This is due to the compensatory impulse coming after the extrasystole. It is he who is perceived as a revolution of the heart.
- Hot flashes and increased sweating.
- Constant weakness and dizziness.
- Periodic onset of shortness of breath and lack of air. At the same time, an unreasonable fear for one’s own life appears.
How pronounced the disease will be depends on whether the person has pathological processes in the heart.
Diagnostics and first aid
The presence of SE in itself does not indicate the presence of any heart disease .
The diagnosis is made based on:
- patient complaints;
- general examination with listening and measurement of heart rate (HR);
- data on the patient’s lifestyle, bad habits, past illnesses and surgical interventions, heredity;
- laboratory blood test (general, biochemical, thyroid and adrenal hormones).
If necessary, an ECG, Holter monitoring, ultrasound examination of the heart, stress tests with ECG recording before and after exercise are prescribed.
Differential diagnosis of SE is carried out using an ECG and electrophysiological study of the heart (EPS), which record intracardiac potentials.
First aid for SE: calm the person down, take off outer clothing (if the attack did not happen outside during the cold season) or unbutton the collar, give him a drink of water, and sit him in a cool, quiet place.
How to relieve an attack: first aid for extrasystole
To relieve an attack of extrasystole, use the following first aid measures:
- sit the patient in a comfortable position;
- ensure the supply of fresh air;
- give water with 20 drops of a soothing tincture (motherwort, hawthorn, mint, valerian, peony) or Corvalol to drink;
- Place a Validol tablet under your tongue.
If the attack is accompanied by panic, trembling of the hands, strong and rapid heartbeat, then breathing into a paper bag or tightly closed palms helps (there should be no gap between them and the face).
Treatment tactics
If the patient has no complaints, hemodynamic disorders (decreased cerebral, coronary and renal blood flow) and there are no organic lesions of the heart, specific treatment for supraventricular extrasystole is not carried out. Single extrasystoles are not dangerous to health and do not require treatment.
If symptoms of supraventricular extrasystole occur frequently and are poorly tolerated, sedatives can be prescribed.
Antiarrhythmic drugs are prescribed by a doctor in exceptional cases due to the large number of side effects. Rare SE (several tens or hundreds of additional contractions per day) does not require such serious therapy.
Thus, if there are no clinical manifestations, blood flow disturbances or heart disease, it is enough to reassure the patient and recommend:
- Establish proper nutrition, if possible, exclude fatty, salty, and hot foods from the diet. Consume more fiber, vegetables and fruits.
- Avoid tobacco, alcohol and energy drinks.
- Spend more time outdoors.
- Avoid stress and heavy physical activity.
- Ensure adequate sleep.
In the presence of a pronounced decrease in blood flow, heart disease and SE against their background, conservative treatment with antiarrhythmic drugs and glycosides is prescribed. Medicines are selected only by the attending physician individually for each patient.
When the underlying heart disease is treated, the symptoms of SE are weakened or disappear completely.
In extreme cases, if medications do not bring relief and the patient has difficulty with extrasystole, surgical intervention may be performed.
Currently, there are two options for surgical treatment of SE:
- Open heart surgery , during which ectopic areas are removed. Typically, such an operation is indicated in cases of intervention in connection with heart valve replacement.
- Radiofrequency ablation of ectopic foci - a catheter is inserted into a large blood vessel, an electrode is inserted through it, and the areas where pathological impulses occur are cauterized.
Treatment of cardiac extrasystole with drugs
Medicines for the treatment of cardiac extrasystole are prescribed for frequent, dangerous forms, poor tolerance of arrhythmia, myocardial diseases, and the most common drugs are Anaprilin, Corvalol, Isoptin.
Anaprilin
Anaprilin during extrasystole helps reduce the effect of adrenaline and other stress hormones on the heart. It is effective for rhythm disturbances that occur during emotional stress and heavy physical exertion.
The negative effect of the drug manifests itself in extrasystoles that appear after meals, at night, and at rest. The dose is selected individually, but it is not recommended to slow the pulse to 50 beats per minute, and for elderly patients the lower limit is 55.
Corvalol
Corvalol during extrasystole acts due to a general calming effect; it does not have a specific antiarrhythmic effect on the heart. The reaction to stress factors decreases, the heart rate normalizes (with initial tachycardia). The drug can only be prescribed to patients without myocardial diseases - with neuroses, vegetative-vascular dystonia. Use is contraindicated in patients with:
- damage to the kidneys, liver;
- low blood pressure;
- severe attacks of angina pectoris;
- myocardial infarction;
- heart failure.
Isoptin
The medication is prescribed for extrasystoles, high blood pressure, and rapid pulse. It is indicated for patients who cannot use beta-blockers (bronchial asthma, fluctuations in blood sugar in diabetes, a tendency to allergic reactions). It can be recommended for patients with angina at rest and exertion (variant) with resistance to nitrates.
Rehabilitation
No specific rehabilitation is required for supraventricular extrasystole.
General recommendations are the same as after any heart surgery:
- peace, no stress;
- minimal physical activity: walking, no heavy lifting;
- dietary nutrition;
- restful, long sleep;
- completely eliminate smoking, alcohol, energy drinks;
- do not overheat (do not go out in the heat, do not visit the bathhouse or sauna, dress according to the season).
Diagnostic methods used
To confirm the diagnosis it is necessary:
- Analyze patient complaints. The doctor asks about the existing symptoms, the time of their occurrence and the severity of the manifestation.
- Collect a life history. It is important to report all previous surgical interventions, lifestyle, bad habits, and genetic diseases.
- Conduct an external inspection. The doctor feels the pulse, listens to the heart to detect changes in rhythm and frequency, taps the heart to determine its clear boundaries, changes in which indicate cardiac diseases.
- Determine the indicators of general and biochemical blood tests, analyze the level of hormones in the blood.
- Obtain electrocardiography data. With their help, changes characteristic of all types of rhythm disturbances are identified.
- Conduct daily Holter monitoring. During this procedure, the patient wears a portable device throughout the day that records any rhythm fluctuations during sleep, physical activity, and eating. In this way, doctors learn how the heart works under normal human conditions.
- Order an electrophysiological study. In this case, the heart is stimulated using small electrical impulses. This helps to figure out how the conduction system works. The study is usually prescribed when the cardiogram does not provide accurate information.
- Perform echocardiography. This ultrasound examination is necessary to identify cardiac causes of arrhythmia.
- Analyze the results of load tests. To do this, an ECG is performed, after which the patient must squat, exercise on a treadmill or exercise bike. Then an ECG is performed again and it is determined how the indicators have changed and whether arrhythmia occurred during physical activity.
Also read: Extrasystole and osteochondrosis
If necessary, they can consult with a therapist and cardiac surgeon.
Prognosis, complications and consequences
According to some experts, frequent supraventricular extrasystole after a few years can lead to the development of heart failure, atrial fibrillation and cause a change in the configuration of the atria.
The prognosis for SE is favorable. This disease does not lead to sudden death, unlike ventricular extrasystole in combination with organic heart damage.
In rare cases, supraventricular tachycardia may develop.
Relapse prevention and prevention measures
Specific prevention for supraventricular extrasystole is not required. Doctors advise establishing a healthy lifestyle and diet:
- sleep in a cool room at least 7-8 hours a day;
- reduce salty, fried, hot foods in the diet to a minimum;
- smoke and drink alcohol as little as possible, it is better to eliminate energy drinks completely;
- walk in the fresh air for at least an hour a day, preferably 2 hours;
- moderate physical activity: swimming in the pool, taking the stairs instead of the elevator, skiing or jogging in the park. This is especially true for people with sedentary jobs.
Supraventricular (supraventricular) extrasystole occurs in people of any age. Mild cases do not require treatment. More serious ones may be accompanied by heart and other diseases and require drug therapy, and in extreme cases, surgical treatment. The main thing with this disease is to remain calm and lead a healthy lifestyle.
What is supraventricular (supraventricular) extrasystole and how to treat it
NVEs develop due to many reasons.
Even a simple sneeze or fear can cause extraordinary contraction of the myocardium. The most common culprits of extrasystoles are various heart diseases: coronary disease, cardiomyopathy, congenital and acquired defects, myocarditis, pericarditis, chronic heart failure, etc. Also, supraventricular extrasystole develops with the following factors, conditions and diseases:
- violation of autonomic regulation (autonomous dysfunction syndrome);
- physical and emotional stress;
- neurotic disorders;
- reflex irritation of the cardiac nerves in diseases of the gastrointestinal tract: duodenal ulcer, cholelithiasis;
- presence of bad habits;
- coffee addiction;
- taking pills: antidepressants, psychostimulants to reduce appetite, vasoconstrictor nasal drops, medications for high blood pressure. Even some antiarrhythmic drugs in some cases cause EVE;
- infectious diseases;
- severe diseases of the respiratory system: bronchial asthma, chronic broncho-obstructive pulmonary disease;
- pathology of endocrine organs: Graves' disease, Hashimoto's thyroiditis, diabetes mellitus;
- excess or deficiency of minerals in the body (calcium, magnesium, sodium);
- chest injuries.
In some cases, the cause of the rhythm disturbance cannot be identified. Then a diagnosis of “NVE of unknown etiology” is made.
Daily norm of supraventricular extrasystoles
Large-scale clinical studies were conducted, during which it was possible to establish the norm of LVE. In a healthy person without cardiac pathology, the norm of supraventricular extrasystoles per day is about 200-300. This amount of NLE does not pose a health hazard.
Classification and types
There are many types of NLEs, divided according to different characteristics.
Depending on the source of the impulse, atrial extrasystoles and extrasystoles (ES) from the atrioventricular (AV) connection are distinguished. Based on the number, they distinguish between single and double. Three or more ES in a row is already considered an episode of tachycardia (also called a “jog”).
In my patients, I often observe such an ECG phenomenon as allorhythmia - the regular occurrence of extrasystoles. There are the following types:
- bigeminy - the appearance of ES on the cardiogram after each normal contraction of the heart (read more about this phenomenon here)
- trigeminy - after every second complex;
- quadrigeminy - after every third complex.
Depending on the cause, the following types of NVEs are distinguished:
- functional - during physical activity, reflex effects;
- organic - for heart diseases;
- toxic - in case of drug overdose;
- mechanical - for injuries.
Single extrasystoles
The most benign variant of NVE, mainly found in healthy individuals, are single supraventricular extrasystoles. They almost always go unnoticed by humans and do not pose a threat to health.
Frequent symptoms
In most of my patients, supraventricular extrasystole occurs latently, without symptoms.
And yet, with a prolonged course of the disease, some people may experience a feeling of fear, an unpleasant sensation of freezing, interruptions in the functioning of the heart, and “rolling” in the chest.
Some patients suffering from heart disease complain of short-term difficulty breathing, dizziness and weakness. Sweating and fever are also sometimes observed.
Signs on ECG
Supraventricular extrasystole is very easy to recognize on a cardiogram. Main features:
- extraordinary (extrasystolic) appearance of a pathological deformed P wave and the following unchanged QRST complex;
- the presence of a compensatory pause, i.e. a straight line on the film.
If the P wave has a different shape in different leads, this phenomenon is called polytopic atrial extrasystole. Its detection is highly likely to indicate a heart or lung disease and requires a more thorough diagnosis.
It happens that after an extraordinary P wave there is no QRST complex. This happens when atrial extrasystole is blocked. ES from the atrioventricular junction differs in that the P wave is negative or not recorded at all due to overlap with the T wave.
When taking an ECG at rest, extrasystoles may not be detected. Therefore, in order to “catch” them and find out how often they occur, I prescribe Holter monitoring to my patients. In case of concomitant diseases, a person undergoes a cardiac ultrasound (EchoCG).
After supraventricular ES, the pause lasts less than with ventricular ES.
Treatment: when, how and with what
Supraventricular extrasystoles are almost always benign. If extraordinary contractions of the heart are single, are not accompanied by any symptoms and do not provoke the occurrence of severe rhythm disturbances, treatment of supraventricular extrasystole is not required. The main thing is to fight its cause.
When EVE worsens the patient's condition, I prescribe drug therapy. The most effective drugs for stopping SE are beta-blockers - Bisoprolol, Metoprolol.
If there are contraindications to their use (for example, severe bronchial asthma), I transfer the patient to slow calcium channel blockers - Verapamil, Diltiazem.
Read about how extrasystole is treated with medications here.
As for traditional methods, to date there is no convincing evidence of their effectiveness. In my practice, I recommend that patients under no circumstances replace traditional treatment with traditional medicine. But if you have a different opinion, we invite you to read the material here.
If the development of NVE is associated with emotional stress or a neurotic disorder, you can take sedatives and make an appointment with a psychotherapist.
The main criteria for the success of therapy are the cessation of symptoms and normalization of the patient’s condition.
In rare cases, when drug treatment does not have the expected positive effect, surgical intervention is used, in particular, a technique such as radiofrequency catheter ablation. I usually prescribe this operation to young patients, since with age the risk of developing severe complications, including death, increases.
It is extremely rare, for health reasons, that an open access operation is performed, with dissection of the chest and removal of the portion of the myocardium where extraordinary impulses are formed.
Why are supraventricular extrasystoles dangerous and what are their consequences?
Extraordinary supraventricular extrasystoles themselves do not pose a threat to human life and often go unnoticed.
However, they can provoke the appearance of more severe rhythm disturbances: supraventricular tachycardia, atrial fibrillation and flutter, which lead to a sharp decrease in blood pressure, deterioration of blood supply to the myocardium and an increased risk of blood clots in the heart. A combination is often observed .
Long-term polytopic and blocked ES are considered the most unfavorable.
The consequences of supraventricular extrasystole are determined by the presence of: coronary heart disease, chronic heart failure, etc. The rhythm disturbance itself almost does not cause any complications.
Despite the fact that most often EVEs are relatively harmless, if they occur frequently and are accompanied by symptoms (feelings of freezing, interruptions in heart function, dizziness, feeling of lightheadedness), you should consult a doctor to find out the cause, including examination for cardiac problems. and other diseases. I try to explain to my patients that eliminating the causative factor is of no small importance in the treatment of EVE. Therefore, I give recommendations for lifestyle changes: you need to quit smoking, try to avoid severe stress, and significantly limit the consumption of alcohol and coffee. If a person develops signs of EVE while taking medications, be sure to tell the doctor about it. Reducing the dosage or changing the medication often helps get rid of extrasystoles.
A 33-year-old man came to see me with complaints of rapid heartbeat, periodic sensations of “fading” and interruptions in heart function over the past 3 weeks. He does not take any medications on his own. Doesn't smoke, doesn't drink alcohol.
A general examination revealed a high heart rate (105 beats per minute) and increased blood pressure - 140/80 mmHg. Art. During the conversation, I noticed the patient’s uncharacteristic irritability and bulging eyes. When questioning about the presence of diseases in relatives, the man noted that his father suffered from Graves' disease.
Holter ECG monitoring was prescribed. Sinus tachycardia, atrial extrasystole of the bigeminy type, and a large number of single extraordinary contractions (967) were detected. A referral was issued to an endocrinologist to check the thyroid gland.
On the recommendation of a specialist, an ultrasound examination was performed and blood was taken for hormonal tests. The results obtained: diffuse enlargement of the thyroid gland, decreased TSH levels, increased concentrations of free T4, high titers of antibodies to the TSH receptor. Diffuse toxic goiter was confirmed .
Mercazolil therapy was prescribed with subsequent monitoring of hormone levels. To slow down the heartbeat and combat extrasystole, beta-blockers (Bisoprolol) are recommended.
Conclusion
When you hear the diagnosis of “supraventricular extrasystole,” there is no need to panic. With a high degree of probability, if you slightly adjust your lifestyle, NVE will go away on its own.
However, you should not take it too lightly, since if it lasts for a long time, adverse consequences may develop.
It is very important to focus on your own well-being: when attacks become more frequent and cause intense discomfort, you need to consult a cardiologist.
Source: https://cardiograf.com/ritm/nesvoevremenno/nadzheludochkovaya-ehkstrasistoliya.html