Why is vasoconstriction dangerous?
If the changes in the lateral surface of the bloodstream are small and the blood flow is not greatly reduced, then they say that the lesion is hemodynamically insignificant. When the walls have serious changes, low velocity and high flow density are observed, this means a hemodynamically significant lesion.
What is stenosis
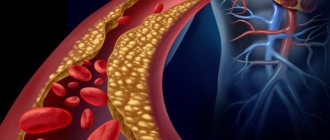
Stenosis means a decrease in the light lumen of the bloodstream. Occlusion is the complete blocking of the canal diameter. The presence of cholesterol deposits on its walls affects the reduction in internal size.
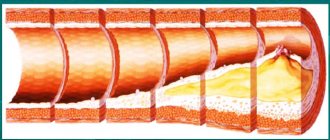
A person has two carotid arteries - on the left and on the right in the neck. These blood “rivers” supply blood to the vessels of the brain and heart. When the walls are damaged, the diameter gradually narrows.
If the narrowing reaches more than 80%, then the movement of blood flow becomes the same as at rest. This is a serious prerequisite for the development of myocardial ischemia.
Diagnosis of the disease
When diagnosing this disease, the doctor listens to the sound of blood flowing through the affected areas. A procedure is prescribed - Doppler ultrasound of the central (main) arteries of the head. This method is named after the Austrian physicist Doppler.
Ultrasonic reflections from moving particles, such as blood cells, can determine the speed, volume of blood flow per minute, the location of stenosis or complete blockage of the blood channel. To obtain a detailed picture, an examination method is used - angiography. It is performed using a catheter in the femoral artery or on the wrist.
To identify pathology during examination, a computer research method is used - magnetic resonance imaging (MRI) using the physical phenomenon of magnetic resonance. This method is suitable if changes in the blood vessels of the brain are suspected. This examination is much more expensive than others.
Symptoms and treatments
Lesions of the blood channel may be minor, then no symptoms occur.
With extensive foci, ischemic attacks are observed and the following symptoms appear:
- Dizziness
- Limbs go numb
- Tingling on your fingertips
- Vision weakens
- There is weakness in the arms and legs
- The attack lasts no more than half an hour
Types of surgical treatment
This disease can only be helped by surgery. This is done in two ways:
- Carotid endarterectomy is an open operation. In places of narrowing, under anesthesia, part of the affected area with cholesterol compactions is removed.
- Stenting is the insertion of a stent into the affected artery through a catheter. A stent is a special endoprosthesis. It opens and expands the inner diameter of the canal, restoring normal blood flow. It does not allow the diameter of the lumen to narrow.
The system includes a special filter with a membrane that prevents blockage of microscopic vessels during surgery. After the operation is completed, the filter and probe are removed.
To see what stenting is, watch this video:
Source: organserdce.com
Causes and risk factors
The carotid arteries are paired large arterial vessels that supply blood to the brain in those sections where the centers of thinking, speech, personality, sensory and motor function are located. The carotid arteries run through the neck and enter the brain through openings in the skull.
When fatty substances and cholesterol accumulate, an atherosclerotic plaque is formed, which narrows the carotid arteries. This reduces blood flow to the brain and increases the risk of ischemic stroke. A stroke occurs when blood flow does not reach any part of the brain. During a stroke, some brain functions are suddenly lost. If the lack of blood flow lasts more than three to six hours, then these disorders become irreversible.
Why does a stroke develop when the carotid artery narrows?
- Significant narrowing of the carotid artery reduces blood circulation in the brain, and with a sudden drop in pressure (suddenly getting out of bed, flying, overheating in the sun or major surgery), the blood flow suddenly stops, which leads to the death of nerve cells.
- Tearing off a piece of atherosclerotic plaque with its transfer by the bloodstream into small arteries of the brain, which leads to their blockage.
- Acute thrombosis (formation of a blood clot) due to narrowing of the carotid artery with complete cessation of blood flow in certain areas of the brain.
Risk factors
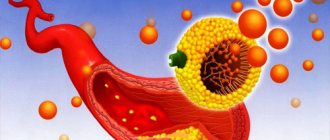
An atherosclerotic plaque forms on the wall of a vessel and contains cholesterol, triglycerides and platelets. Risk factors for this process are nutritional disorders (abundance of animal fats and simple carbohydrates in the diet), obesity, type 1 and 2 diabetes, smoking.
As it increases, it can independently block the lumen of the vessel or a blood clot breaks off from it, which moves with the blood into the internal arteries of the brain, causing their blockage. The plaque itself can also break off and, in the form of an embolus, disrupt the nutrition of deeper cerebral structures.
In addition to atherosclerosis, carotid artery stenosis is caused by:
- connective tissue diseases (fibromuscular dysplasia);
- autoimmune arteritis;
- traumatic injuries;
- blood diseases - increased platelet count, sickle cell anemia;
- thrombus formation in heart defects, endocarditis, atrial fibrillation, tumor processes;
- abnormal structure, including kinking (increased tortuosity).
Risk factors for carotid atherosclerosis
Risk factors for carotid artery disease are similar to those for other types of cardiovascular disease. They include:
- Age
- Smoking
- Hypertension (high blood pressure) is the most important risk factor for stroke
- High cholesterol
- Diabetes
- Obesity
- Sedentary lifestyle
- Family history of atherosclerosis
Men under 75 years of age have a greater risk of developing carotid artery stenosis than women in the same age group. In the group over 75 years of age, women have a greater risk of stroke. In patients suffering from coronary artery disease, narrowing of the carotid artery is often detected.
Types of tricuspid regurgitation
There are 2 main classifications of this pathology - according to the time of appearance and the reasons for its occurrence.
- By time of appearance: congenital and acquired.
Congenital is registered during the intrauterine development of the child or in the first months after birth. In this case, heart valve function may return to normal over time. In addition, it is much easier to keep a congenital anomaly under control if you take care of the heart and follow measures to prevent cardiovascular diseases.
Acquired disease appears in adults already during life. This pathology almost never occurs in isolation; it can be caused by a variety of diseases - from dilatation (expansion) of the ventricle to obstruction of the pulmonary arteries.
- For reasons: primary and secondary.
Primary tricuspid anomaly is diagnosed against the background of heart disease. The patient does not have any problems with the respiratory system with this diagnosis. The main cause of secondary disruption of blood flow in the tricuspid valve is pulmonary hypertension, that is, too high pressure in the pulmonary artery system.
Regurgitation of the tricuspid valve traditionally goes hand in hand with insufficiency of the valve itself. Therefore, some classifications divide the types of reverse blood flow based on the form of tricuspid insufficiency, that is, the valve disease itself:
- Organic (absolute) failure, when the cause is damage to the valve leaflets due to a congenital disease.
- Functional (relative), when the valve is stretched due to problems with the pulmonary vessels or diffuse damage to the cardiac tissue.
Clinical forms
Atherosclerotic lesions of the carotid arteries most often differ according to the localization of the main process:
- Atherosclerosis of the common carotid arteries - rarely contributes to ischemic stroke; even with complete blockage of the common carotid artery, blood flow through the internal carotid artery can be preserved. However, there may be general cerebral disorders - poor memory, general weakness, headaches.
- Atherosclerosis of the bifurcation of the common carotid artery - atherosclerotic plaques narrow the entrance to the internal carotid artery and can completely block it. This is the most common form of damage. With this localization, transient ischemic attacks and ischemic strokes most often develop.
- Atherosclerosis of the intracerebral sections of the carotid artery - plaques are located in the carotid arteries and their main branches. Ischemic stroke often develops due to thrombosis of narrowed arteries.
Ultrasound identifies two main types of atherosclerotic plaques:
- Stable plaque - the narrowing of the artery has smooth contours, without undermined edges, with a slight acceleration of blood flow on the plaque.
- An unstable plaque is often a calcified plaque with jagged contours; moving elements and significant turbulence of blood flow during Doppler sonography may be observed.
Based on the degree of narrowing of the carotid artery, there are:
- Hemodynamically insignificant stenosis (narrowing of the artery by less than 70%, without local acceleration of blood flow)
- Hemodynamically significant stenosis (narrowing of the artery by more than 70%, with accelerated blood flow)
- Occlusion - complete blockage of the carotid artery
Complaints and symptoms
Atherosclerosis of the carotid arteries can be asymptomatic or cause complaints associated with impaired cerebral blood flow. Most often, patients may complain of temporary impairment of brain function (transient ischemic attack) or persistent loss of brain function (ischemic stroke).
Transient ischemic attack (TIA)
A TIA occurs when blood flow to the brain is briefly interrupted. This is the initial phase of acute cerebrovascular accident, which is reversible. It has the same symptoms as a stroke, but these symptoms go away within minutes or hours.
A TIA requires emergency medical attention because it is impossible to predict whether it will progress to a stroke. Immediate treatment can save lives and increase the chances of a full recovery.
Modern research has shown that patients who have had a TIA are 10 times more likely to suffer a major stroke than a person who has not had a TIA.
Ischemic stroke has the following symptoms:
- Sudden loss of vision, blurred vision, difficulty in one or both eyes.
- Weakness, tingling, or numbness on one side of the face, one side of the body, or one arm or leg.
- Sudden difficulty walking, loss of balance, lack of coordination.
- Sudden dizziness.
- Difficulty speaking (aphasia).
- Sudden severe headache.
- Sudden memory problems
- Difficulty swallowing (dysphagia)
Ischemic stroke and transient ischemic attack begin in the same way, so any ischemic stroke can be called an ischemic attack if the symptoms completely resolve within 24 hours of the onset of the disease. The presence of a time interval between the onset of stroke symptoms and the death of parts of the brain allows for urgent surgery to restore cerebral blood flow.
Course of the disease
Once atherosclerotic plaques appear, they will no longer be able to resolve, but only gradually progress. The rate of growth of an athersclerotic plaque depends on many risk factors, including cholesterol levels. All people over 50 years of age are recommended to undergo an annual ultrasound of the carotid arteries in order to exclude the development of atherosclerotic plaques and the risk of ischemic stroke.
With the development of complications of atherosclerosis of the carotid arteries, discirculatory encephalopathy quickly progresses. Frequent TIAs, and even more so ischemic stroke, contribute to the death of part of the brain tissue and disruption of brain function. Patients with atherosclerosis of the carotid arteries often develop vascular dementia (dementia).
After restoration of the patency of the carotid artery, the phenomena of cerebrovascular insufficiency are stopped, and the likelihood of repeated cerebrovascular accidents is significantly reduced.
Treatment of tortuosity of the internal carotid artery (ICA)
Treatment of ICA tortuosity must begin at an early stage. You should not wait until an attack of cerebrovascular accident occurs. As soon as pathological tortuosity of the internal carotid artery is diagnosed, treatment begins using manual therapy techniques. Electromyostimulation of the neck muscles allows you to normalize posture and the state of cervical lordosis. With the help of reflexology, the internal state of blood vessels is affected, and blood pressure levels are normalized.
The doctor develops an individual course of therapy. It may include therapeutic exercises and kinesiotherapy, osteopathy and massage, reflexology and physiotherapy. Traction traction of the spinal column shows good results, especially if the ICA syndrome is associated with the development of cervical osteochondrosis and its complications.
Forecast
Carotid atherosclerosis carries a significant risk of ischemic stroke. With asymptomatic narrowing of the internal carotid artery of more than 70%, the risk of ischemic stroke exceeds 5% per year. If the patient has had episodes of cerebrovascular accidents, then this risk is already 25% per year.
The risk of ischemic stroke in asymptomatic atherosclerotic plaques with a narrowing of less than 70% does not exceed that in patients without atherosclerosis.
After adequate restoration of blood circulation in the carotid arteries, the risk of ischemic stroke is reduced by more than 3 times.
Source: angioclinic.ru
S and C shaped tortuosity of the internal carotid artery
There are several types of pathology. More common is the s-shaped tortuosity of the ICA with a smooth transition from one dislocation site to another. Usually with this type there is a deviation at two points. Most often, s-tortuosity of both ICAs occurs with deformities of the cervical spine. Straightening the cervical lordosis and static overstrain of the neck muscles entails a change in the position of the bed of this cerebral vessel.
S-shaped tortuosity of the internal carotid artery in most cases does not give pronounced clinical manifestations. It is discovered during a study for another disease. If left untreated for 2-3 years, the disease will progress. In this case, the clinical picture worsens and emergency treatment of vascular pathology is required.
C-shaped tortuosity of the internal carotid artery develops in people suffering from high blood pressure. This type is typical for elderly patients suffering from atherosclerosis of cerebral blood vessels.
Children and adolescents are characterized by this type of pathology called kinking. This is a bend of the cerebral blood vessel at an angle of 45 degrees. It is a congenital vascular pathology. Gives attacks of acute cerebrovascular accident during excessive physical exertion. Such children and adolescents often complain of attacks of dizziness and fainting during physical education lessons. Parents should pay attention to the appearance of such complaints and conduct an examination.
Causes of narrowing of the carotid artery
Narrowing of the carotid artery owes its rather high prevalence to risk factors that affect a large number of people, especially the elderly. Vascular pathologies contribute to:
- Heredity;
- Bad habits, in particular smoking;
- High blood pressure;
- Disorders of carbohydrate metabolism (diabetes mellitus);
- Old age and male gender;
- Excess weight, lack of physical activity.
If the family already has patients suffering from atherosclerosis and narrowing of the carotid arteries, then it is likely that other blood relatives may have a hereditary predisposition to the pathology.
Apparently, genetic mechanisms of susceptibility to lipid metabolism disorders are the basis. Such common conditions as hypertension, diabetes, obesity also provoke atherosclerosis of the carotid arteries. Excessive pressure changes the structure of the vascular walls, making them dense and vulnerable, promoting the accumulation of lipids there, and the combination of atherosclerosis with high blood pressure significantly increases the risk of acute disorders of blood flow in the brain.
With age, the likelihood of structural damage to the walls of the carotid arteries increases, so the pathology is usually diagnosed in the 6th-7th decade of life. In men, this process occurs earlier, and in women, the protective function is performed by the sex hormones estrogens, so they get sick later, after menopause.
Stenosis of the carotid artery against the background of atherosclerosis can be aggravated by congenital anomalies of vascular development, among which kinks, loops, and tortuosity are quite common. In these zones, there is an increased likelihood of damage to the endothelium by turbulent blood flows, atherosclerosis progresses and hemodynamically significant stenosis can manifest earlier, compared to the direct course of the vessel.
The morphological basis of stenosis of neck vessels is cholesterol plaque. The pathology of the metabolism of fats and carbohydrates provokes the deposition of fat not only in the aorta, coronary and cerebral arteries, but also in the vessels of the neck, which makes it difficult to deliver blood to the brain.
A plaque in the carotid artery does not manifest itself for the time being, especially if it is localized on one side. With its gradual increase, the lumen of the vessel narrows more and more, and signs of a lack of blood flow in the head appear - chronic ischemia, clinically expressed in dyscirculatory encephalopathy.
With relatively preserved blood flow through the main arteries of the neck, the phenomena of chronic ischemia will gradually progress, but when the plaque is destroyed, thrombosis will inevitably develop with complete blockage of the vessel. This is one of the most dangerous manifestations of carotid artery stenosis, which is accompanied by necrosis of brain tissue (stroke).
Depending on the extent of damage to the vascular walls, focal atherosclerosis is distinguished (over one to one and a half centimeters) and prolonged, when plaques occupy more than 1.5 cm of the length of the artery.
To assess the degree of risk of vascular accidents and determine indications for surgical treatment, it is customary to distinguish several degrees of narrowing of the carotid arteries, determined by the percentage of stenosis of the lumen of the vessels:
- Up to 50% is a hemodynamically insignificant narrowing, which is compensated by collateral blood flow;
- 50-69% – pronounced narrowing, manifested clinically;
- Stenosis up to 79% is subcritical, the risk of acute circulatory disorders is very high;
- Critical stenosis, when the lumen of the artery is narrowed by 80% or more.
The most susceptible to the atherosclerotic process are the initial sections of the common carotid artery, the place of its division into external and internal branches and their mouths.
Hemodynamically significant tortuosity of the common carotid arteries in adult patients
Bakhmetyev A.S., Dvoenko O.G., Makarova Ya.I., Sukhoruchkin V.A. State Budgetary Educational Institution of Higher Professional Education “Saratov State Medical University named after. IN AND. Razumovsky” of the Ministry of Health of Russia, Saratov
Purpose of the study
To identify the incidence of pathological tortuosity (PI) of the common carotid arteries (CCA) in adult patients who complained of headaches.
Material and methods
The study included 2150 patients (4300 CSA in 1455 women and 700 men, average age 50.7 ± 12.3 years) who underwent routine triplex scanning of the brachiocephalic arteries (TS BCA) at the Department of Ultrasound and Functional Diagnostics of the Clinical Hospital named after. S.R. Mirotvortsev SSMU in the period from June 2012 to July 2016. The study was conducted on an expert-class device Philips HD11 XE.
Hemodynamically significant PI of the CCA was considered in the presence of turbulent blood flow in it, an increase in peak systolic velocity (PSV) of more than 150 cm/s at the inflection point of the CCA, and also with a PSV gradient of more than 2.5 (the ratio of PSVmax to PSV in the proximal part of the CCA).
results
PI OSA was detected in 850 (39.5%) patients (1120 OSA in 600 women and 250 men, mean age 57.4 ± 8.7 years). 135 (6.3%) of those who applied had PI OSA on both sides. The structure was dominated (720 patients – 33.5%; 930 arteries) by hemodynamically insignificant C-shaped PI CCA. S-shaped PI CCA at an obtuse or right angle – in 80 (3.7%) cases (125 arteries).
In 2 (0.1%) patients there was a hemodynamically significant PI at a right angle (PSC gradient 2.65). Kinky tortuosity of the CCA - in 48 (2.2%; 63 arteries) patients (in all cases - hemodynamically significant; average PSC gradient - 2.69 ± 0.22; average PSC in the inflection - 154.35 ± 31.5 cm/s ). In 2 (0.1%) patients there was a loop-shaped hemodynamically significant tortuosity of the CCA (2 arteries; average PSC - 2.73; average linear systolic velocity at the inflection - 179.4 cm/s).
Note that out of 52 (2.4%; 67 arteries) patients with hemodynamically significant PI CCA, 48 (2.2%) suffered from uncontrolled arterial hypertension for at least 5 years. There was no correlation between hemodynamically significant PI CCA and gender and age.
conclusions
Hemodynamically significant PI OSA in the population of adult patients occurs only in 2.4% of cases. The main share of significant PIs is due to kinking and loop-like tortuosity of the CCA. TS BCA is the leading non-invasive method for identifying hemodynamically significant PI CCA.
- Views: 1286
- Comments:
Did you like the post? Do you find it useful or interesting? Support the author!
You must log in to the site
To perform this action, you must log in to the site or register. Interesting 5
Manifestations and diagnosis of carotid artery stenosis
There are no specific symptoms that indicate carotid artery stenosis. Since the narrowed artery cannot deliver the required volume of blood to the brain, the symptoms will consist of signs of ischemia in the brain. The narrowing of half the lumen of the vessel does not cause hemodynamically significant disorders, and therefore proceeds unnoticed by the patient. As the degree of stenosis increases, clinical signs will appear.
The first “bells” indicating trouble may be transient ischemic attacks (TIA), which are accompanied by:
- Headache;
- Dizziness and imbalance;
- Feeling of numbness in the face and limbs;
- Slurred words, impaired understanding of spoken speech, which makes contact with the patient difficult;
- Vision disorders;
- Fainting.
The listed symptoms are short-lived, usually lasting about half an hour, and then gradually regress, and by the end of the first day not a trace remains of them. However, even if the condition has completely returned to normal, you need to consult a doctor to clarify the cause of ischemia in the brain. If you have had a TIA in the past, the risk of stroke increases tenfold, so these attacks can be regarded as harbingers of cerebral infarction and should not be ignored.
Chronic cerebral ischemia due to stenosis of the neck arteries is manifested by decreased performance, weakened memory, difficulty concentrating, and behavioral changes. Signs of such discirculatory encephalopathy may become noticeable, first of all, to others, who will begin to note that their loved one or colleague’s character is changing, it is more difficult for him to cope with his usual responsibilities, it is more difficult to achieve mutual understanding when communicating, while the patient himself will try to maintain his usual image life, “attributing” symptoms to fatigue or age.
Critical stenosis of the right or left carotid artery can lead to much more serious consequences than TIA. A large atherosclerotic plaque can rupture with the release of its contents onto the surface of the vascular wall, in which case thrombosis will necessarily develop, and the resulting clot will completely block the artery, leaving it without the opportunity to deliver blood to the brain.
The result of a complete cessation of blood flow through the carotid artery is an ischemic stroke - cerebral infarction , in which nerve cells die in the area of the blood supply to the affected artery. A thrombus or its fragments can break off and move into smaller vessels - basilar, cerebral arteries, and then the symptoms of a stroke will be caused by damage to a specific vascular area.
Symptoms of a stroke include paralysis, paresis, loss of consciousness, speech disorders, swallowing, and sensitivity. In severe cases, cerebral coma occurs and the activity of the cardiovascular and respiratory systems is disrupted. These symptoms often occur suddenly, against the background of a severe headache, and can take a person by surprise at the workplace, on the street or at home. It is important that those around you quickly get their bearings and call an ambulance, because both life and the prognosis of the disease depend on the speed of providing qualified assistance.
Based on the predominant symptoms, several options for the course of the pathology can be distinguished:
- Asymptomatic form, when there are no signs of ischemia in the brain, but stenosis has already been identified through additional examination;
- Discirculatory encephalopathy – chronic ischemia without focal symptoms of brain damage;
- Transient ischemic attacks - can occur with focal neurological disorders that disappear within a day;
- Consequences of a mini-stroke - symptoms disappear within a month;
- Stroke (cerebral infarction) is an acute disturbance of blood flow with cerebral and focal symptoms.
The prognosis of the disease depends not only on the severity of the stenosis, but also on how early the pathology is detected. In this regard, timely consultation with a doctor, even if the symptoms of the disease have disappeared without a trace, is necessary.
One of the first signs of stenosis, which can be detected already during the initial visit to the doctor, is considered to be a kind of noise above the artery when listening to it. To confirm the diagnosis, a variety of instrumental examinations are used - CT, MRI, ultrasound, angiography.
The most accessible, safe and cheap way to diagnose stenosis of the neck arteries is the ultrasound method, supplemented by Doppler ultrasound. The specialist evaluates the structure of the vessel wall and the nature of blood flow through it.
CT and MRI make it possible to exclude other causes of circulatory pathology, and radiocontrast angiography helps to accurately localize the site of narrowing. Contrast is also used at the stage of surgical correction of stenosis.
What does the absence of hemodynamically significant renal artery stenosis mean?
How is renal artery stenosis treated?
Treatment for renal artery stenosis can be surgery, pharmaceuticals, angioplasty, or stenting.
What are the main causes of renal artery stenosis?
The two main causes of renal artery stenosis are atherosclerosis and fibromuscular disease.
What are the symptoms of renal artery stenosis?
Renal artery stenosis has no obvious symptoms. Eventually, untreated renal arterial stenosis causes secondary complications such as chronic renal failure,
What is the prognosis for renal artery stenosis?
Left untreated, renal artery stenosis can cause hypertension (high blood pressure) and can eventually lead to chronic kidney failure (end-stage renal disease).
What does it mean if the umbilical cord only has 1 vein and 1 artery?
congenital renal artery stenosis
Do ace inhibitors cause kidney failure in renal stenosis that is irreversible?
my 70 year old mother was on asa inhibitors, diarrhea and diuretics. Could she still experience sudden pulmonary edema due to renal artery stenosis? she was diabetic.
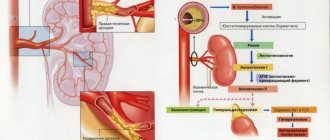
Why is an ACE inhibitor contraindicated in renal artery stenosis?
In the presence of renal artery stenosis, resistance in the afferent arteriole increases. To compensate, Angiotensin II acts to constrict the efferent arteriole to achieve adequate glomerular replenishment. ACE inhibitors block the conversion of angiotensin I to angiotensin II. Without its vasoconstrictive effect, the efferent arteriole becomes dilated. This results in a decrease in GFR and can lead to kidney failure.
What are the functions of the renal vein and renal artery?
The renal vein is the vein that drains away from the kidney. The renal artery is the artery that leads to the kidney.
What does the renal artery do?
The renal artery supplies blood to the renal system or kidneys. The renal artery differs from the renal vein in that it contains a lower concentration of co2 and a higher concentration of urea.
To what organ is the renal artery attached?
The renal artery attaches to the kidneys.
What is the function of the renal artery in a frog?
The renal artery brings oxygen to the kidneys.
Does the renal artery serve
Yes, the renal artery serves the kidneys
What veins and arteries pass through the renal sinus?
segmental artery, renal artery, renal vein, arcuate vein, interlobular vein, interlobular artery
Which artery does not anastomose?
Where would you find the renal artery?
The renal artery supplies the kidneys with oxygenated blood.
What is the first major branch of the renal artery?
The first major branch of the renal artery is the renal hilus. The answer is actually interlobar.
How can you prevent renal artery stenosis?
Strategies to prevent vascular disease include eating a healthy diet, maintaining a desired weight, quitting smoking, managing stress and exercising regularly.
What is the path of a glucose molecule from the renal artery to the renal vein?
The path of glucose and other molecules from the renal artery to the renal vein is as follows. 1 renal artery, 2 arcuate arteries, 3 interlobular arteries, 4 afferent renal arterioles, 5 glomeruli, 6 efferent renal arterioles, 7 peritubular capillary networks, including the rectum, 8 interlobular veins, 9 arcuate veins and 10 renal veins.
Function of the renal artery in the frog?
The renal artery supplies oxygen to the blood from the heart to the kidneys.
Which artery serves
What is the artery that serves to>
renal artery
Which artery supplies
Which artery delivers to>
What kind of blood does the renal artery and renal vein carry?
The renal artery carries blood to the kidney, and the renal vein carries blood that has been cleared by the kidney.
Which artery serves to>
I think his kidney is: | I think his kidney is: | I think his kidney is: |
Which artery takes care of the
What is the name of the artery that serves
Which artery serves to>
This would be the renal artery.
Name the artery that serves the
What is the difference between the pulmonary artery and the renal artery?
The pulmonary artery delivers deoxidized blood from the heart to the lungs. The renal artery delivers oxygenated but dirty blood to the kidneys.
How is the blood in the renal vein different from the blood in the renal artery?
Blood in the renal vein: * Low oxygen content. * Returns to the heart. Blood in the renal artery: * Contains large amounts of oxygen. * Pumped from the heart.
How is the blood in the renal artery different from the blood in the renal vein?
The blood in the arteries will be saturated with oxygen, and the blood in the veins will be deoxidized.
How does blood flow through the brain to the heart?
trace the blood flow through the kidney from the renal artery to the renal vein? blood flow through the kidney from the renal artery to the renal vein
Give one structural difference between renal vein and renal artery?
the renal vein has. greater clearance. smaller elastic layer. smaller muscle layer than the renal artery
How does the composition of blood in the renal artery differ from the renal vein?
The renal artery delivers blood to the kidney. The renal vein takes blood from the kidney. The kidneys filter urea waste from the blood. Thus, the main difference is the amount of urea in the blood: high in the renal artery and low in the renal vein.
Which artery carries blue blood to the lungs?
renal artery
Renal artery - definition?
The medical term "renal" refers to the kidneys, so the renal artery would be the artery (a type of blood vessel through which oxygenated blood passes) that leads to the kidneys and supplies them with blood.
What transports arterial blood to
Renal artery or renal columns - the arterial supply to each kidney is the renal artery. As the renal artery approaches the hilum, it divides into segmental arteries, each of which gives off several branches called interlobar arteries, which pass through the renal columns to reach the cortex.
Does an increase in blood pressure increase or decrease the glomerular filtration rate?
Generally speaking, it will increase. However, this depends on the cause of hypertension. For example, if there is obstruction or narrowing of the renal artery (stenosis, malignancy, etc.), the physiological effect will increase the body's BP. This is due to the fact that the obstacle is a decrease in hydrostatic pressure in the glomeruli and a temporary decrease in GFR. The body compensates by increasing blood pressure to increase GFR. Patients who present with renal artery… Read More
Based on materials from the site: www.answers.com
Treatment of carotid artery stenosis
To treat stenosis of neck vessels and the resulting blood flow disorders in the head, medication and surgery are used.
Conservative therapy is aimed at improving brain activity, protecting it from the harmful effects of hypoxia, for which nootropic and metabolic drugs are prescribed - piracetam, mildronate, B vitamins.
Blood pressure correction becomes an obligatory component of drug therapy. Hypertensive patients should take antihypertensive drugs constantly, according to the regimen suggested by the doctor. Hypotonic patients should be careful and also control their blood pressure, as reducing it will worsen oxygen starvation of the brain.
For atherosclerotic plaques in the carotid arteries, and this is the most common cause of pathology, drugs that normalize fat metabolism (statins) are indicated, diet and rational physical activity are necessary.
Drug treatment can somewhat improve brain activity in non-critical stenosis and plays a supporting role after surgery, but in case of decompensated narrowing of the artery, repeated ischemic attacks or a stroke, surgery is not necessary.
Indications for surgical treatment are:
- Arterial stenosis of more than 70%, even not accompanied by obvious clinical symptoms;
- Conditions after a stroke associated with damage to the carotid arteries;
- Recurrent TIAs with stenosis of 50% or more.
Surgery for carotid artery stenosis is aimed at restoring normal blood flow and can be radical or minimally invasive. Radical interventions are carried out openly, minimally invasive - without a large skin incision.
Radical treatment - carotid endarterectomy - an open operation in which an incision is made in the neck in the area where the vessel passes, the artery is isolated, the surgeon finds the site of narrowing and removes plaques together in a section of the vascular wall, then the integrity of the vessel is restored by plastic surgery, and the wound is sutured. With concomitant bending, looping, and tortuosity, the entire affected fragment of the artery can be removed. The operation requires general anesthesia.
Stenting is a more gentle method of treatment, which consists of introducing a special tube into the lumen of the vessel, which expands it and maintains it in a straightened form, ensuring blood flow. The purpose of such an operation is to prevent possible vascular accidents and minimize the manifestations of chronic hypoxia, therefore it is indicated for subcritical narrowings.
Stenting is performed under local anesthesia with constant monitoring of the patient's blood pressure and pulse. The femoral artery through which the guidewire is inserted is punctured, a catheter and contrast agent are placed into it to accurately determine the location of the stent. The operation is performed under fluoroscopic control, but the dose of radiation received is minimal and does not pose any danger.
A stent is installed at the site of stenosis of the left or right carotid artery, it expands, and it is possible to use special balloons that inflate the vessel at the site of narrowing. To prevent thromboembolic complications with damage to smaller arterial vessels of the brain, during surgery, special filters are installed in the artery that do not interfere with blood flow, but retain the smallest particles of blood clots.
Once the stent is in place, the filters and catheter are removed and the stent remains in place at the site of the stenosis. The intervention lasts no more than an hour, after which the patient can be sent to intensive care for some time or immediately transferred to the ward. Strict bed rest is recommended for the first day; there are no restrictions on food and fluid intake in the postoperative period.
The duration of hospitalization for surgical treatment is determined individually. After stenting, the patient spends 2-3 days in the hospital, after which he can go home. Open surgery requires longer observation - about a week, at the end of which the skin sutures are removed.
The prognosis after timely correction of blood flow is favorable, but the patient should know that the operation does not protect against recurrent damage to this vessel or other arteries of the head and neck, therefore maintaining a healthy lifestyle, normalizing nutrition, maintaining a normal level of pressure are the most important preventive measures that cannot be neglected.
Prevention of carotid artery stenosis against the background of atherosclerotic lesions includes a special diet, rational physical activity, weight loss, smoking cessation and drug treatment of existing cardiovascular and metabolic pathologies. In addition, you should regularly visit doctors for routine medical examinations.
Life-threatening condition of the patient - carotid artery stenosis
If the lumen of the carotid artery is blocked by a blood clot or cholesterol plaque, then the nutrition of the brain is disrupted. This condition (stenosis) may be accompanied by transient ischemic attacks if the blockage is incomplete or a bypass has formed. In the complete absence of blood flow, ischemic stroke occurs, and in some cases, sudden death.
What is carotid artery stenosis
Impaired blood flow through the carotid artery due to narrowing of its lumen is called stenosis. This disease is found in every second patient with cerebral ischemia and in a third of patients with stroke. The disease, as a rule, occurs against the background of the formation of an atherosclerotic plaque inside the vessel. Depending on the degree of damage, the following options are distinguished:
- limited stenosis up to 1.5 cm, widespread more than 1.5 cm;
- segmental - up to a quarter of the circle, concentric - more than half the lumen;
- with complications (hemorrhage, blood clot formation) and without them.
We recommend reading the article about atherosclerosis of the neck vessels. From it you will learn about the pathology and symptoms of its development, causes, diagnosis and treatment.
And here is more information about examination for atherosclerosis.
Risk factors
An atherosclerotic plaque forms on the wall of a vessel and contains cholesterol, triglycerides and platelets. Risk factors for this process are nutritional disorders (abundance of animal fats and simple carbohydrates in the diet), obesity, type 1 and 2 diabetes, smoking.
As it increases, it can independently block the lumen of the vessel or a blood clot breaks off from it, which moves with the blood into the internal arteries of the brain, causing their blockage. The plaque itself can also break off and, in the form of an embolus, disrupt the nutrition of deeper cerebral structures.
In addition to atherosclerosis, carotid artery stenosis is caused by:
- connective tissue diseases (fibromuscular dysplasia);
- autoimmune arteritis;
- traumatic injuries;
- blood diseases - increased platelet count, sickle cell anemia;
- thrombus formation in heart defects, endocarditis, atrial fibrillation, tumor processes;
- abnormal structure, including kinking (increased tortuosity).
Symptoms of the onset of pathology development
If the lumen of the carotid artery is blocked gradually, then bypass pathways for blood supply begin to form in the brain, cells adapt to oxygen starvation and lack of nutrition, therefore, with unilateral and local stenosis, there may be an asymptomatic course and a relatively favorable prognosis. Sudden obstruction leads to an acute cessation of blood flow, that is, a stroke.
The first signs of obstruction of blood flow to the brain are called transient (temporary) cerebral attacks. Their main features:
- weakness (paresis) in one arm or upper and lower limb on the opposite side of the blocked artery;
- numbness of half the face and fingers;
- visual impairment on the side of the stenosis - darkening in the eyes, flickering dots or spots;
- difficulty pronouncing words;
- headache;
- fainting;
- difficulty swallowing;
- local convulsive muscle twitching.
Degrees of carotid artery stenosis
To determine treatment tactics and prognosis of the disease, a criterion such as the degree of stenosis is used. It is calculated in relation to the reference size of the vessels:
- internal carotid artery superior to the bulb;
- common carotid artery before branching at 1 cm and 3 cm.
To calculate, measure the minimum lumen of the artery and divide it by the proper size. The data obtained can be as follows: moderate (above 50%), hemodynamically significant (from 70%), critical (up to 99%), complete occlusion. Moreover, narrowings of more than 75 percent are indications for surgical treatment.
What are the special types of pathology?
Depending on the effect of the degree of narrowing on the blood circulation of the brain, several clinical forms of the disease are distinguished.
Hemodynamically significant
Due to the blocking of more than 70% of the lumen of the artery, before the narrowing there is an increase in blood pressure, and after it the blood flow drops significantly, which causes a deficiency of nutrients and oxygen in the area of the branches of the middle cerebral artery and adjacent areas.
Clinical manifestations occur in the form of severe ischemic attacks, which may still have a reversible course. There are paresis of the limbs, decreased reflexes and sensitivity, visual and speech disturbances. With timely drug therapy, partial or almost complete restoration of functions occurs. 5% of patients develop a stroke within a year.
Critical stenosis
If the lumen is narrowed by 70 to 99 percent, then this is considered dangerous for the occurrence of extensive ischemic strokes. At this stage, atherosclerotic changes lead to massive damage to the arteries, which makes it difficult for the formation of collateral pathways to supply the brain.
Blood clots and emboli are formed that block small branches of blood vessels, so the course of the disease is resistant to conservative treatment methods, and complete rehabilitation of patients is difficult to achieve.
Watch the video about carotid artery stenosis:
Diagnosis of the right and left arteries
In addition to the neurological status of the patient, instrumental methods are used to determine the diagnosis of stenosis:
- Ultrasound of the vessels of the neck: accelerated reverse flow through the external branches; when blocked, blood flows through them to the ophthalmic artery. When the temporal artery is compressed, the blood velocity decreases.
- Angiography of cerebral vessels is used only for preoperative examination. It is being replaced by magnetic resonance imaging.
- MRI with vascular contrast is the most valuable method. Ischemic foci in the brain and sites of vascular embolism are determined.
The difficulty in diagnosing a stroke is that in about a third of patients on the first day of its development there are no visual manifestations in the brain tissue.
Treatment as a chance for life
In order to completely restore blood supply to the brain during stenosis, only surgical treatment methods can be used. But if the operation is performed when a stroke has already occurred, then the mortality rate for such patients is about 40 percent. Therefore, radical therapy is recommended for the following indications:
- suffered a transient cerebrovascular accident;
- cured stroke with minor neurological abnormalities;
- blockage of more than 70% of the artery lumen (even in the absence of manifestations);
- presence of sources of thromboembolism;
- decreased cerebral blood flow.
Operation options
When the lumen of the vessels is completely closed, an anastomosis is created between the external and internal cerebral arteries to bypass the area of stenosis. To do this, connect the subclavian and common carotid or external carotid arteries.
If there is partial occlusion, then surgical treatment options may include:
The first method has a large evidence base for its effectiveness in preventing strokes for 3 to 5 years. To carry it out, the artery is dissected at the location of the plaque, which is separated from the vascular wall. Then a Teflon shunt is installed into the lumen of the vessel, which is removed after the plastic surgery.
The eversion method involves isolating the carotid artery, inverting it like a stocking, and layer-by-layer separation of the plaque. After this, the original tightness of the vessel is restored.
Carotid endarterectomy
Recovery after
For the first two days, the patient is in the intensive care unit, where basic vital functions and cerebral hemodynamics are monitored. Particular attention is paid to blood pressure and blood electrolyte balance. Before discharge, duplex scanning, CT and Doppler ultrasound are performed. As a rule, the patient goes home after a week of hospital stay.
Complications of the operation may include heart attack, stroke, bleeding, vascular thrombosis, and nerve damage. In the long term, a relapse of the disease may occur.
To prevent such conditions, preventive treatment is prescribed:
- Plavix,
- Warfarin,
- Acetisalicylic acid,
- Chimes.
Anticoagulant therapy is carried out under the supervision of blood clotting tests.