Metabolic disorders are found in the practice of endocrinologists and others. These are very different conditions in nature, including those associated with excessive activity of the human body’s own immunity. Dangerous changes occur, and how much depends on the specific diagnosis.
Antiphospholipid syndrome is a pathological process associated with the production of special antibodies to the substance of the same name. Phospholipids are part of the structure of cell membranes, so disruption leads to generalized disorders in the functioning of the body. In particular, the circulatory system suffers.
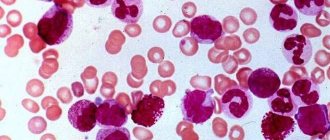
The “calling card” of the syndrome is a violation of the blood coagulation process, its shift towards hypercoagulation due to the destruction of platelets, precisely those cells that participate in the normal functioning of the body.
In addition, damage to the central nervous system, heart, kidneys and other structures is observed. Huge problems arise during pregnancy, miscarriages and other dangerous complications are possible.
Treatment presents certain difficulties. This is mainly due to the inability to quickly recognize the source of the disorder. However, with competent help, it is possible to correct the disorder and provide a positive outlook.
Development mechanism
The pathological process is based on a group of changes. The algorithm for solving the problem is approximately the following:
- The human body is influenced by a certain provoking factor. These may include a previous infectious disease, viral or bacterial, there are several options. Systemic disorders of an inflammatory profile, but not of a septic nature.
Also the influence of a toxic factor, poisoning with salts of heavy metals, vapors of other substances. What caused the onset of the pathological process needs to be clarified through diagnostics.
- As a result of the influence of a negative factor, a problem like an autoimmune reaction develops. It is false because there is no longer a real threat. Such a failure can be of varying degrees of severity: from minimal, which is practically unnoticeable or has no symptoms at all, to critical violations.
- As a result of an autoimmune reaction, a large number of antibodies to phospholipids are produced. These compounds enter the structure of cells and the substances provoke the destruction of membranes, which leads to catastrophic consequences.
It should be noted that in almost 3% of people it is possible to increase the level of antibodies without any health problems. This is not considered a pathology, the body copes with the disorder, but it may well indicate the initial phases of the disorder, so this phenomenon should absolutely not be ignored.
- Antibodies to phospholipids cause cell destruction by dissolving the outer membrane. All cytological structures suffer indiscriminately, depending on how immune substances circulate.
As a result of APS syndrome, platelets, the structures of the brain and central nervous system in general, the heart, kidneys are most affected; in pregnant women, the placenta is affected, creating a huge danger to the fetus.
Ultimately, this reaction leads to disruption of the entire body. How dangerous it is depends on the amount of antibodies synthesized and the aggressiveness of the body’s immune response. It is necessary to begin treatment as quickly as possible. Otherwise, it will be impossible to predict complications.
According to statistics, women under the age of 35-45 are mainly affected. They are at increased risk and therefore require careful monitoring, especially during fertile years and during pregnancy.
Antibodies to cardiolipins
Cardiolipins are phospholipids involved in cellular respiration and metabolism. Since they are located inside cellular structures, anticardiolipin antibodies (aCL) begin to destroy them, damaging the cells themselves.
The reason is the malfunction of the immune system, which “confuses” foreign tissues with “native” ones. In humans, the process of blood clotting is disrupted, clots and blood clots form in the vessels.
The norm of anticardiolipin antibodies in healthy people:
- IgG >19 IU/ml;
- IgA >15 IU/ml;
- IgM >10 IU/ml.
Increased levels are recorded in systemic diseases (lupus, vasculitis, rheumatoid arthritis), Crohn's disease and infections. But their concentration is incomparable with the irreducibly high levels in APS.
Therefore, if an increased level of antibodies is detected, a repeat examination is carried out after 6 weeks. In APS, the concentration of IgG and IgM remains high.
The level of antibodies is measured using an enzyme-linked immunosorbent method, identifying the concentration of immunoglobulins A, M, G, which cause thrombosis. However, it is not possible to detect an increase in the level of anticardiolipins in all cases of APS. Sometimes the indicators are within normal limits.
This form of the disease is called latent (hidden). The increase in aCL with it is not constant, so patients have to take tests several times. An increase in the concentration of even one antibody indicates the diagnosis of the syndrome. The frequency of increased concentrations of anticardiolipins in APS is indicated in the table.
| aKL | Exceeding level, % |
| IgM IgG | 5–33 39–44 |
| IgA | 17–57 |
Classification
The division of the process is carried out according to a complex criterion: etiology plus clinical picture and features of a particular condition.
Accordingly, the following points are determined:
- Primary form. Accompanied by spontaneous development. There are no third-party diseases that can cause the disorder. However, it may simply not be detected. Therefore, it makes sense to examine the patient several times at intervals of a couple of months; the diagnosis can be revised.
- Secondary pathological process. It occurs much more often. Antiphospholipid syndrome occurs against the background of other diseases. Including atypical ones, such as infectious processes. It is necessary to recognize them in order to then link them with the nature of the deviation.
- Idiopathic form. It is determined based on the results of repeated diagnostics. This is a condition whose cause is unclear. At the same time, doctors are forced to deal with the manifestations of the disorder, and not with the disease itself.
As the nature of the disorder becomes clearer, the diagnosis may be revised. The question remains open until further diagnosis. It is considered the least favorable form, since there is no way to influence the root cause.
- APL-negative or hidden. Occurs relatively often. Moreover, despite the typical manifestations of the pathological process and the presence of specific antibodies, other markers of the disease are not detected. Lupus anticoagulant and some other substances are not detected, which is strange for such a condition.
It is necessary to conduct a series of laboratory tests to confirm suspicions of a latent form. APS syndrome in a blood test is not the only sign, but the most characteristic, therefore it is assessed in this case.
- Critical or catastrophic type. It is characterized by massive hypercoagulation with the development of dangerous complications. A lot of blood clots appear, and without urgent medical care the patient is doomed.
This classification is complex; there are other methods of division, but they are not considered generally accepted, and therefore are used to a much lesser extent.
What tests are performed
To diagnose the syndrome, blood is donated to:
- lupus anticoagulant (LA)
- cardiolipin antibodies (aCL) to IgG, IgM, IgA and beta-2-glycoprotein;
- antibodies to phosphatidylserine;
- coagulation, thromboplastin time (aPTT), platelet and erythrocyte content.
If the test is positive, the blood is re-dated after 8-10 weeks. In APS, the concentration of IgG and IgM remains consistently high, and the level of lupus coagulant in plasma doubles.
The level of antibodies is measured using an enzyme-linked immunosorbent method, identifying the concentration of immunoglobulins A, M, G, which cause thrombosis. Isotype G is most often associated with serious complications of APS - blockage of large vessels and recurrent miscarriage. To determine the severity of the lesion, a general blood test is taken with a platelet count, the concentration of which is reduced in APS.
A blood coagulogram is prescribed. If the result is doubtful, a detailed test for coagulation is performed: tests for partial thromboplastin time (APTT), prothrombin + INR, antithrombin III, prothrombin time.
It is advisable to undergo such an examination at the stage of planning the birth of children in order to avoid miscarriages and stillbirths. During pregnancy, these tests are taken every 14 days and five days after birth.
Blood is taken from a vein in the morning before meals. The analysis is not prescribed during critical days, when the temperature rises and when you feel unwell. After recovery you need to wait a few days. Before the tests, you should not eat fatty foods or drink alcohol. You should tell your doctor if you are pregnant or suspect that you are pregnant.
Symptoms
The clinical picture is extremely heterogeneous, since antiphospholipid antibodies are present throughout the body at once, and changes in a whole group of systems are possible. Signs are named depending on the predominant localization of the disorder.
Circulation
Among the characteristic points:
- Thrombosis. Against the background of the disease in question, there is a high probability of the formation of clots that will not allow the tissues and organs to be nourished. This is an extremely dangerous condition, as it is fraught with cell death and gangrene.
- Feeling of numbness in the limbs. Manifestation of thrombosis. Occurs as a result of partial blockage. Accompanied by goosebumps and immunity to mechanical stimuli.
- Blindness, mono- or binocular. Develops as a result of retinal vein thrombosis. Vessel rupture and hemophthalmos are possible, but most often simple ischemia begins with destruction of the optic nerve and the development of a complete and irreversible loss of the ability to see. This is one of the most dangerous scenarios against the background of antiphospholipid syndrome.
- Disorders of sensitivity, motor activity. As a result of the same thrombosis.
- Changing the shade of fabrics. First to pale, then to violet, crimson or dirty brown. There are several options, depending on which vessels are affected.
- Intense pain. When moving and simply trying to lean on the affected leg, use the hand on the side involved in the process. Mainly the limbs are affected.
- Necrosis. Tissue death, gangrene.
There are lesions not only of veins, but also of arteries. The development of thrombosis of main and even distant vessels is accompanied by clot detachment, its migration and ultimately blockage of important trophic pathways (for example, the pulmonary artery) with a rapid fatal outcome. Sometimes the patient does not have time not only to react, but also to understand what happened.
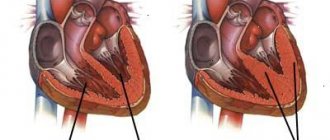
Heart
Cardiac structures are affected just as often. Clinical manifestations of antiphospholipid syndrome include the following symptoms:
- Intense pain in the chest. They are burning or pressing in nature. Which just indicates the ischemic origin of the discomfort. The strength is great, the duration is about several tens of minutes, then the sensation subsides.
- Rhythm disturbances. Tachycardia. Acceleration of the beat, as changes progress, heart rate may drop sharply. This is an unfavorable sign.
- Dyspnea. Even in a state of complete rest, without any physical activity. With mechanical activity, the manifestation becomes more and more intense.
- Nausea.
- Dizziness. Central nervous system disorder. Against the background of heart damage, the contractility of the muscular organ decreases; it is not able to sufficiently nourish the brain. This is the cause of poor health. In the future, loss of consciousness is likely, possibly repeated.
- Weakness. Asthenic syndrome. Characterized by weakness, drowsiness, and inability to carry out the usual active activities.
- A panic attack is possible. A feeling of intense fear with no apparent source of the problem.
The nature of the symptoms resembles the full clinical picture of angina pectoris, but the attack has a high probability of transformation into a heart attack. Patients are required to be hospitalized even before the outcome becomes clear.
The symptoms of a pre-infarction state are described in detail here.
Kidneys
Damage to the structures of the excretory tract is accompanied by a group of typical disorders:
- Painful sensations. Discomfort appears almost immediately, the intensity is usually insignificant. Character - nagging, aching.
- Dysuria. Determined by a lot of options. Violation of the urination process such as retention, a decrease in the amount of daily urine or, on the contrary, an increase in its volume. When excluding diabetes insipidus.
There may be pain during the process of emptying the bladder, and other issues. These are not normal phenomena. However, they are not specific enough; antiphospholipid syndrome is the last thing to be suspected. Hence the importance of carefully collecting anamnesis and analyzing complaints.
- Change in urine color. To dark, reddish. This is a clear indication of the development of hematuria or the appearance of protein.
- Increase in body temperature. Not always, depending on the specific situation.
Without urgent and high-quality care, kidney failure and other health and life-threatening phenomena are likely.
central nervous system
When the brain is damaged, the following manifestations are observed:
- Weakness. Asthenic syndrome.
- Impaired coordination of movements. The patient is unable to move normally, control his own activity, or physical manifestations. This is the result of a malfunction of the extrapyramidal system.
- Focal neurological symptoms. Depending on which area is affected. There are many forms.
- Headache.
Objectively, damage to the central nervous system resembles a stroke or a transient disturbance of cerebral blood flow. In different variations.
Skin signs
The main manifestation of APS syndrome from the dermis is the formation of reddish spots of multiple localization of small sizes. The shade varies from pinkish to deep purple or scarlet.
This manifestation is called livedo (network cyanotic pattern), purpura or petechial rash. This is the result of massive destruction of platelets with the development of hemorrhages.
Signs in pregnant women, reproductive system
Antiphospholipid syndrome poses a tremendous danger to mother and child.
With the development of the pathological process, toxicosis is detected, regardless of the phase of gestation, as well as problems with the liver, brain function, and critical surges in blood pressure (preeclampsia).
As a result, spontaneous termination of pregnancy, death of the child in the womb, and fetal development defects are possible.
The pathological process does not have its own clinical manifestations. It is determined by focal disorders.
Causes
The development of antiphospholipid syndrome is provoked by a group of factors.
Generally speaking, we can name the following categories:
- Taking certain medications. Among these are hormonal medications, drugs for treating depression and psychotropic drugs in general.
- Diseases of autoimmune origin. From systemic lupus erythematosus to periarteritis nodosa. There are many options. How even rheumatoid arthritis will make itself known, especially without treatment, no one can say.
- Infectious processes. From a simple cold with infection of the oropharynx by streptococcus to more serious disorders such as AIDS, tuberculosis and other variants.
- Malignant tumors. Not all. Mainly with localization in the organs of the endocrine system, hematopoietic structures, and others.
There is also a hereditary predisposition. It’s difficult to say exactly what role she plays. However, primary forms most often develop as a result of a spontaneous failure, when there is no apparent reason.
Analysis for VA
Lupus anticoagulant is a group of antibodies - immunoglobulins G. that prevent blood clotting. It got its name because it was first identified in patients with lupus.
An anticoagulant appears in the body due to impaired immune reactions. It inhibits the formation of thrombin from prothrombin, reducing blood clotting. This leads to bleeding and, oddly enough, to thrombosis. Blood clots are formed due to attacks of antibodies on blood vessels, which immunoglobulins mistake for foreign structures.
Normally, there should be no lupus coagulant in the blood, but in APS it is detected in various concentrations. The analysis can be:
- negative – VC not detected;
- weakly positive - VC content 1.2 - 1.5 c.u. (conventional units);
- moderate – VC 1.6-2.0 USD;
- positive – VC more than 2.0 c.u.
If the test is positive, the blood is re-dated after 8-10 weeks. With the development of APS, the level of lupus coagulant in plasma doubles.
Since different laboratories use different technologies for determining VC, its concentration may not be indicated in the analyses, but only the result obtained - negative, moderate or pronounced - may be recorded.
Positive VC is observed not only in APS. It has been reported in cases of lupus and long-term use of certain medications, such as phenothiazines. Therefore, other laboratory tests are needed to make a final diagnosis.
Diagnosis of APS
Patients with suspected phospholipid syndrome are examined by hematology specialists. Since the problem is complex, it is possible to involve other doctors in helping. The question remains open and depends on the specific clinical case.
List of events:
- Oral questioning of the patient. It is necessary to establish as accurately as possible all deviations in well-being. This is an important point, since symptoms reveal the essence of the pathological process and its localization.
Next, it remains to put forward hypotheses and exclude them one by one. Often, against the background of the disorder, there is a combination of several disorders, for example, kidneys + central nervous system or heart + venous problems and so on.
- Anamnesis collection. Study of factors that could potentially trigger the onset. Including previous illnesses and other issues.
- General blood test.
- Coagulogram. With the study of coagulation speed.
- Specific tests.
- Study of biomaterial for lupus anticoagulant and other substances.
Ultrasound of internal organs, chest X-ray, electroencephalography, ECG, ECHO-CG are indicated as auxiliary techniques.
These are not so much methods for identifying antiphospholipid syndrome, but rather a way to detect its consequences - the degree of disruption of the functioning of internal organs.
Attention:
The APS diagnostic cycle is carried out repeatedly. For at least three weeks, the disease is clarified with parallel restoration of the patient's condition.
Treatment methods
Correction is carried out through medication. Several types of drugs are used.
- Anticoagulants. Heparin-based products, as well as others.
- Actually thrombolytics. In short courses, so as not to provoke the opposite effect. Warfarin and similar.
- Antiargents. Aspirin and more modern options.
Moderate physical activity, cessation of smoking, alcohol, and prolonged sitting in one place are recommended. The problem is also solved through plasmapheresis, if there is a need for it.
The regime plays no less a role. During the first few days, the patient is in the hospital; hospitalization may be extended to a couple of weeks. Further, all activities are carried out on an outpatient basis.
Things are much more complicated during pregnancy. The mother is being preserved and undergoing regular, systematic treatment.
The goal of therapy is not only to relieve symptoms, but also to eliminate the root cause of the abnormal condition. The main forces are directed towards this.
Antibodies to beta-2-glycoprotein I
These autoantibodies are found in 70-80% of people suffering from APS. Since the substance is synthesized not only by liver cells, but also by the trophoblast of the embryo during pregnancy complicated by antiphospholipid syndrome, its concentration increases sharply.
The mechanism of action of antibodies to beta-2-glycoprotein I is still not clear, but it is known that these substances increase blood clotting, leading to blood clots, miscarriages and late toxicosis.
In addition to APS, such antibodies are detected in systemic diseases (lupus, vasculitis) and rheumatism, so the analysis is carried out only in conjunction with other studies.
Consequences
Among these are necrosis, tissue gangrene, pulmonary embolism, angina pectoris, heart attack, stroke, blindness, renal failure, and disability. Death from complications.
APS or antiphospholipid antibody syndrome (abbreviated as SAFA) is a dangerous condition; without treatment, it behaves unpredictably and most likely promises nothing but death.
Therefore, all suspicious symptoms should be grounds for contacting a doctor. Only with timely medical care can you count on recovery.
Test for antibodies to phosphatidylserine
This type of antibody works in the same way as aCL, affecting platelets and tissue of the vascular wall, this effect leads to thrombosis and blood clotting disorders
Normally, the blood contains no more than 16 units/ml. antibodies. An increase in the rate is observed in 40-60% of cases of APS.
Since a transient (transient) increase in antibody levels is observed with infections and taking certain medications, if the result is positive, the test is repeated after 6 weeks.