Use of the troponin test to diagnose myocardial infarction
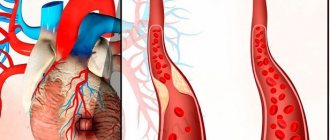
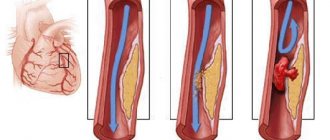
During a heart attack, as a result of acute thrombosis of the coronary vessels, ischemia and necrosis of the myocardium develop. Heart failure with progressive narrowing of the arteries and poor circulation also leads to a heart attack. The patient’s life depends on the timely detection of coronary pathology. Early diagnosis includes a cardiogram, ultrasound and determination of specific proteins - troponins. The troponin test for myocardial infarction allows one to identify changes in the first hours, confirm the diagnosis and transport the patient to the hospital.
Biochemical
A biochemical blood test for myocardial infarction does not allow one to determine specific indicator values. During the study, the maximum and minimum values are determined and the difference between them is determined. If an acute attack of ischemia occurs, then the following is determined:
- The level of total protein albumin and globulin, the concentration of which increases during the active development of ischemic disorders. This occurs due to a violation of metabolic processes in the body.
- Urea and creatinine. These indicators increase during an attack, which indicates serious disruptions in the functioning of the heart.
- Cholesterol. An increase in cholesterol concentration also indicates acute pathology. Normally it should be from 3.5 to 6.5 mmol/l. If coronary heart disease and atherosclerosis develop, the values increase several times.
- Enzymes aspartate aminotransferase and alanine aminotransferase. Their sharp increase always indicates a necrotic process in the heart muscle.
- Amylase and phosphatase enzymes. They increase if tissue dies in the heart muscle. Deviation from the norm may also indicate improper treatment.
- Myoglobin. Previously, it was believed that its presence in the blood indicates a complicated course of a heart attack. But this theory was refuted through numerous tests. Doctors have found that the period of myoglobin elimination is several hours. Therefore, it cannot provide accurate information about the development of the pathological process.
Also read: Deciphering a blood test for cholesterol It is impossible to diagnose acute ischemic disorders without a biochemical blood test.
Using these indicators, you can confirm the presence of a problem and choose the appropriate treatment. With cardiovascular diseases, the level of heavy metals in the blood often increases. If there is more cadmium or aluminum in the body, then these substances have a toxic effect. At the same time, the amount of microelements important for health decreases. This is noticeable by a drop in the level of chromium, copper, and manganese.
High content has a negative effect on the body:
- Lead. This substance causes serious disruption to the endocrine system. In addition to damage to the heart and blood vessels, there is a deterioration in the condition of the liver. Large amounts of lead cause arterial hypertension and atherosclerotic changes in blood vessels.
- Cadmium. Excessive content of the element is accompanied by liver poisoning and the development of cardiomyopathy.
- Arsenic. Because of it, there is a decrease in vascular permeability. If their walls thicken, the likelihood of cardiogenic shock increases.
Changes in the concentration of heavy metals occur in connection with an attack of myocardial infarction. This significantly increases the risk of complications.
When should you do a troponin test?
Myocardial infarction is an acute, life-threatening condition caused by a circulatory disorder in the myocardium as a result of complete or partial blockage of a coronary artery by a thrombus. This leads to ischemia and necrosis of part of the heart muscle. Subsequently, the chances of a successful outcome depend on the timeliness of medical care.
The myocardial infarction test is performed at the first symptoms of a heart attack:
- pain in the chest and heart area, aggravated at rest, of a compressive nature, with a feeling of squeezing or burning;
- pain in the arm, neck, jaw, on the back in the area of the shoulder blades or between them, discomfort in the abdomen;
- severe weakness and shortness of breath with a feeling of lack of air, fear of death;
- sticky cold sweat, chills, trembling in the arms and legs;
- nausea, vomiting, unstable blood pressure against the background of heart pain and a general progressive deterioration of the condition.
Also, the use of a rapid heart attack test is recommended for patients with angina pectoris, coronary artery disease with frequent attacks of chest pain.
Troponin analysis is used:
- at home, if it is impossible to see a doctor for heart pain;
- when severe pain occurs, in patients with chronic cardiac pathology;
- within 2-4 hours after the first symptoms of a heart attack appear;
- at the prehospital and hospital stage, to confirm the diagnosis.
Characteristic features of a pain attack during myocardial infarction
| Feature of the attack | Characteristic |
| Localization of pain | Behind the sternum, less often in the heart area |
| Nature of pain | Pressing, squeezing, burning, cutting pain for a long time |
| Patient position | Frozen in place - afraid to make any movement due to increased pain |
| Patient behavior | Anxiety, fear, worry |
| Radiation of pain | In the left shoulder, left hand, left half of the neck and head, under the left shoulder blade |
| Duration of attack | The painful attack is prolonged, is not relieved by taking nitroglycerin or goes away for a short time and reappears |
In every fifth patient, a heart attack occurs without the occurrence of clinical symptoms.
Execution technique
Currently, pharmacies offer various rapid tests for detecting heart attacks. A diagnostic kit for the qualitative determination of troponin I or a combination kit that additionally determines myoglobin and creatine phosphokinase, markers of necrosis (death) of the heart myocardium.
This test kit contains:
- hermetically sealed test cassette and test strip;
- pipette for single use;
- scarifier for piercing a finger;
- buffer solution in a vial;
- instructions.
The analysis technique is quite simple; you need to:
- Use reagents and rapid test kit at room temperature.
- Remove the test card-cassette, scarifier and pipette from the packaging, read the instructions to understand the algorithm.
- Wash your hands with soap, dry and warm by rubbing your palms.
- A scarifier needle is used to pierce the lobe; one press on the inner surface of the middle or ring finger is enough.
- Massage your finger towards the edge to form the first drop of blood, then remove it with a cotton swab and alcohol.
- Place your finger over the cassette, but do not touch it, and squeeze the second drop of blood into the center of the rapid test window under the number indicated in the instructions.
- If possible, use a pipette to collect blood.
- Add the buffer solution from the bottle into the window on the cassette under the corresponding letter.
- After carefully putting the test cassette aside, apply a cotton swab with an antiseptic to your finger.
- Wait 15-20 minutes until reaction marks clearly appear in the window on the cassette.
The test must be scored according to the instructions. Standard troponin tests should consider:
- two red marks opposite the control zone with marks of the letters “C” and “T” mean a positive result;
- the appearance of a line opposite the “T” mark of any intensity, even weak, indicates a positive test and the presence of troponin in the blood;
- the only red risk opposite the “C” zone indicates a negative analysis;
- the complete absence of a line opposite o means the test is unsuitable, the deadline has expired, or an error has occurred.
What is the diagnostic value of the test
Troponin is a special protein that is found in the cells of cardiomyocytes of the heart and is almost undetectable in the blood under normal conditions. The main reason for the increase in its concentration is myocardial necrosis. In modern medicine, the determination of troponin in the diagnosis of myocardial infarction occupies a leading position.
The markers rise in the blood 3-6 hours after a heart attack and remain in the bloodstream for up to two weeks. Troponin I has a peak concentration after 12-24 hours with normalization of values within 1-2 weeks, when the test becomes negative. Therefore, rapid tests are suitable not only for home use, but also for identifying dynamics in hospital treatment. This test is also indicated to determine cases of recurrent infarction.
The value of the express method itself is as follows.
- Labeled antibodies are located on the surface of the test cassette.
- When a drop of blood with a high content of troponins is added to their surface, the antibodies form a complex and immediately react.
- The signal strips, which determine the result of the reaction, are colored with special proteins.
- During myocardial infarction, the troponin level increases tens and thousands of times, the test strip reacts to a high concentration of heart attack markers and turns red.
Other research methods
In addition to these basic studies, other additional research methods are used in the diagnosis of myocardial infarction:
- Myocardial scintigraphy is a diagnostic method in which a radioisotope substance enters the body. It tends to accumulate in the damaged area.
- Positron emission tomography is an additional diagnostic method that identifies areas of reduced blood supply to the myocardium.
- Magnetic resonance imaging allows you to assess the condition of the heart muscle for the presence of hypertrophy and areas of insufficient blood supply.
- Computed tomography is an x-ray diagnostic method that evaluates the size of the heart, its chambers, the presence of hypertrophy and blood clots.
Diagnosis of myocardial infarction
The fundamental task of cardiology is to reduce the time required for accurate diagnosis of myocardial infarction.
The speed of diagnosing a heart attack is not just the effectiveness of treatment - although it is quite obvious that the earlier specific anti-infarction therapy is started, the more reliable it is to overcome a dangerous disease and the less severe the consequences it will leave. But first of all, the speed and accuracy of diagnosis is necessary to save human life. Myocardial infarction poses the greatest mortal threat at the initial stage. But even if the patient “climbed out,” untimely treatment still leaves a risk of sudden cardiac arrest in the subsequent period. Even years after the heart attack.
General blood analysis
In addition to biochemistry analysis, laboratory diagnosis of acute myocardial infarction includes a general blood test. Although this method does not identify specific markers, it can identify signs characteristic of the inflammatory process.
CBC indicators for laboratory diagnosis of myocardial infarction:
To increase the likelihood of a favorable prognosis, it is important to conduct all studies in the first hours after the first symptoms of the disease.
Golden hour for diagnosing myocardial infarction
The German Heart Foundation (DeutscheHerzstiftung) strongly recommends avoiding delays in the event of a heart attack. Qualified assistance should be called immediately. A specific resuscitation program, including anti-infarction measures, should be launched within the first hour. The later, the worse!
Cardiologists in Germany call the first sixty minutes of a heart attack goldeneStunde. The concept of golden hour is used in global clinical practice. In both cases we are talking about the golden hour. If it is missed, things may turn out badly (or even fatally).
The problem, however, is that during the first hour after the onset of a heart attack, doctors do not have an accurate idea whether they are dealing with a myocardial infarction or an acute outbreak of another, symptomatically similar ailment.
According to German cardiology methods, a diagnosis of myocardial infarction can be made when the level of specific biomarkers in the blood is elevated and at least one of the following three factors is present:
- characteristic bursts of the electrocardiogram
- characteristic chest pain
- confirmed coronary insufficiency due to stenosis of the heart arteries
Any of the three points can be identified immediately. But even if all three points are present, this is not yet proof of a heart attack. Final confirmation can be obtained with blood test results showing high levels of specific biomarkers. But such analysis, alas, does not happen quickly.
The fight for the clock when diagnosing myocardial infarction
The main biomarker indicating the development of a heart attack is cardiac troponin (international abbreviation cT), a special protein complex intensively produced by cardiac muscle cells when it is damaged. Another biomarker indicating a heart attack is the enzyme CK-MB (international abbreviation CK-MB), which is one of the isomers of a whole group of enzymes collectively called creatine kinase (Creatin-Kinase, or CK). CK-MB is also found in cardiac muscle cells, but also in other tissues (brain, lungs, skeletal muscles, thyroid gland).
Elevated levels of both of these substances in the blood indicate myocardial infarction.
Normal values for both biomarkers are:
- cardiac troponin – less than 0.1 nanogram per milliliter
- CK-MB - less than 6 percent of the total mass of creatine kinase
Higher values are already a formidable sign. It's a heart attack.
Why are both biomarkers taken into consideration? The fact is that the level of the CK-MB enzyme can increase not only during a heart attack, but also when other tissues are damaged, for example, skeletal muscles. A more accurate indicator of a heart attack is an increase in cardiac troponin levels (more than 0.1 ng/ml). However, its concentration increases in the blood very slowly. The first signs of growth appear only three hours after the onset of a heart attack. Equally slowly, cardiac troponin increases over the next 20 hours - and then gradually begins to decrease.
Waiting for the maximum increase in cardiac troponin to diagnose a heart attack means wasting a whole day! Therefore, the first diagnosis is made on a reduced basis. If a blood test done three hours after the onset of a heart attack shows a CK-MB level greater than 10 percent of total creatine kinase and at least one element of the triad "cardiogram - chest pain - coronary artery stenosis" is present, this is considered sufficient for the initial diagnosis myocardial infarction.
How clinical blood and urine tests react to the development of myocardial infarction
Considering that the main pathomorphological manifestation of this disease is acute necrosis of areas of the heart muscle, a general blood test during myocardial infarction will show a picture of the presence of an inflammatory process in the body. Already 4 - 6 hours after the onset of the acute phase of heart disease, the number of leukocytes in this study will increase by 2 - 3 times. The growth of white blood cells occurs mainly due to young forms of neutrophils. A similar symptom in clinical laboratory diagnostics is called a neutrophilic shift of the leukocyte formula to the left.
Read also: Myocardial infarction in dogs
The following picture is observed with the percentage of eosinophils in the blood: 24 hours after the onset of the disease, their number drops sharply and is practically undetectable in a blood test. As soon as the patient’s body begins to receive appropriate treatment, and the regeneration processes in the myocardium intensify, these blood elements are restored to normal values. The process may take up to 2 - 4 weeks.
As soon as the inflammatory process in the heart muscle begins to subside under the influence of specific treatment, the ESR returns to its normal numbers.
A general urine test does not carry any special meaning for this disease. Specific changes in this study may occur if myocardial infarction is accompanied by the development of acute renal failure.
In this rather rare case, the general analysis of urine may contain a large number of white blood cells, mucus, and a rapid increase in specific gravity will also be characteristic.
A new method for rapid diagnosis of myocardial infarction
"fits" into the golden hour!
The effect of a bomb exploding in cardiology was the message that a new biomarker had been found that allows reliably diagnosing myocardial infarction WITHIN AN HOUR. This is a cytosolic GPBB enzyme, belonging to a group of substances with the general name glycogen phosphorylase involved in polysaccharide metabolism.
In the body of a healthy person, GPBB enzymes are concentrated in high concentrations in the cells of the heart muscle. They are present there in a bound state, regulating the level of glycogens - polysaccharides formed by glucose residues. When the heart muscle is damaged, the active process of glycogen breakdown begins. The released GPBB enzymes immediately enter the bloodstream. A rapid blood test can detect an increase in GPBB levels. This is a reliable indication of a heart attack!
The new diagnostics used in Germany fit into the golden hour, which makes it possible to begin targeted treatment of a heart attack in an optimal time.
Electrocardiographic study - ECG
ECG recording
ECG is an accessible diagnostic method that allows you to identify damage to the heart muscle and determine treatment tactics. An ECG during a heart attack always looks in dynamics, i.e. this study is repeated at certain intervals to assess the course of the disease. The method allows you to assess the extent of damage, identify complications of a heart attack in the form of various rhythm disturbances, and the formation of a cardiac aneurysm.
Myocardial infarction enzyme. Diagnosis of myocardial infarction
During myocardial infarction, there is a significant release of various substances (cardiomarkers) from areas of necrosis and damage. And this yield is more significant, the greater the mass of the affected myocardium. Measuring cardiac marker levels speeds up and refines activities such as the diagnosis of myocardial infarction . as well as the ability to predict its further development. The main biochemical markers used in the diagnosis of myocardial infarction are myoglobin, troponin I, troponin T, creatine phosphokinase and lactate dehydrogenase.
Myoglobin is an oxygen-binding protein of striated skeletal muscle and myocardium. Its molecule contains iron, is structurally similar to the hemoglobin molecule and is responsible for the transport of 02 in skeletal muscles. Myoglobin is one of the earliest markers of myocardial damage, since an increase in its level in the blood is detected within 2-4 hours after the occurrence of acute myocardial infarction. The peak concentration is reached within 12 hours, and then decreases to normal within 1-2 days. Due to the fact that the release of free myoglobin into the blood can be caused by a number of other pathological conditions, this marker alone is not enough to accurately diagnose myocardial infarction.
The most specific and reliable markers of myocardial necrosis are cardiac troponins T and I (they allow us to detect even the most minor myocardial damage).
Troponins are proteins involved in the regulation of muscle contraction. Troponin-I and troponin-T of the myocardium and skeletal muscles have structural differences, which makes it possible to isolate their cardiac-specific forms using immunoassay methods. Approximately 5% of troponin-I is found free in the cytoplasm of cardiomyocytes. It is due to this fraction that troponin-I is detected in the blood plasma within 3-6 hours after damage to the heart muscle. Most of the troponin-I in the cell is in a bound state and is released slowly when the myocardium is damaged. As a result, the increased concentration of troponin in the blood persists for 1-2 weeks. Troponin-I concentrations typically peak between 14 and 20 hours after the onset of chest pain. In approximately 95% of patients, 7 hours after the development of acute myocardial infarction, an increase in the concentration of troponin-I is detected.
A slight increase in cardiac troponin-I levels should be interpreted with considerable caution, as it may be due to various pathological conditions that cause damage to myocardial cells. That is, an increased troponin level in isolation cannot serve as a basis for a diagnosis of myocardial infarction.
If a patient with suspected non-ST segment elevation acute coronary syndrome has elevated levels of troponin T and/or troponin I, then this condition should be regarded as myocardial infarction and appropriate therapy should be provided.
Determination of troponins allows detecting myocardial damage in approximately a third of patients who do not have an increase in CF-CK. To detect or exclude myocardial damage, repeat blood draws and measurements are necessary within 6 to 12 hours after admission and after any episode of severe chest pain.
Creatine phosphokinase (creatine kinase)
Creatine phosphokinase (creatine kinase) is an enzyme found in the myocardium and skeletal muscles (small amounts are found in the smooth muscles of the uterus, gastrointestinal tract and brain). The brain and kidneys contain predominantly the BB isoenzyme (brain), the skeletal muscles contain the MM enzyme, and the heart contains the MB enzyme. Creatine kinase MB has the greatest specificity. There is a high correlation between the level of its activity and the mass of necrosis. When the myocardium and skeletal muscles are damaged, the enzyme is released from the cells, leading to an increase in creatine kinase activity in the blood. 2-4 hours after an anginal attack, the level of creatine kinase MB in the blood increases significantly, and therefore the determination of creatine phosphokinase and creatine kinase MB in the blood is widely used in the early diagnosis of myocardial infarction. Normal level of creatine kinase in the blood in men Breathing myocardial infarction, myocardial infarction, left ventricle
Patient examination
In addition to laboratory methods for diagnosing myocardial infarction and the instrumental methods listed above, other methods for making this diagnosis are widely used in medicine.
Examination of the patient is the simplest method of examination, which the doctor can begin immediately after arriving on call. Without requiring additional devices, this technique includes a number of manipulations aimed at recognizing cardiac muscle necrosis in the early stages.
Methods of physical examination as part of the clinical diagnosis of myocardial infarction:
- Anamnesis collection. To obtain a complete picture of the disease, the doctor needs to collect an anamnesis - obtain information about the symptoms of the current condition and diseases suffered in the past.
- Palpation method. To check the correct functioning of the heart muscle, a point of the myocardium is palpated, the displacement of which indicates disturbances in the functioning of the heart. Using the same method, the patient’s pulse rate is measured and the lymph nodes are checked for the presence of hypertrophy.
- Percussion or tapping of the chest to determine the cardiac boundaries. The high diagnostic accuracy of the method lies in the fact that during myocardial infarction, dilatation of the left ventricle of the heart is observed (it increases in volume), which causes a shift of the borders of the heart to the left side.
- Auscultation. This procedure involves listening to the patient's chest using a stethoscope. At the same time, the rhythm of the heart, the presence of noise, weakened tones, which is characteristic of a heart attack, are assessed.
- Measuring body temperature. As a rule, during myocardial infarction the patient experiences a low-grade fever in the range of 37.1-37.4 °C.
- Changes in blood pressure can also indicate myocardial necrosis. Since the pumping function of the heart weakens due to necrosis, the pressure drops by an average of 10-15 mm Hg. Art.
Laboratory methods for studying myocardial infarction can show a complete picture of the disease, but most often they cannot be carried out immediately after the attack. In situations where a diagnosis needs to be made as quickly as possible, examining the patient comes to the rescue.
Express test for diagnosing myocardial infarction Troponin I
Timely diagnosis of the disease increases the chances of a quick and complete recovery. It is very important to have a research device on hand if the matter concerns life and death. An express test for diagnosing myocardial infarction will help predict its development within 2-3 hours after the first symptoms appear.
How the Troponin I express test works
In order for the heart muscle to work without interruption, it has a special regulatory complex, which consists of the proteins troponin T and I. They are specific, which is why they are also called cardiac.
When a heart attack develops, which means necrosis of muscle tissue begins, proteins are released into the blood in large quantities. Normally, there are practically no troponins in human blood. Therefore, it is advisable to conduct a troponin test during a heart attack if there is reason to suspect the development of the disease. The main symptoms of cardiac dysfunction are:
- Sharp pain behind the sternum.
- General weakness.
- Dizziness and loss of consciousness.
Express diagnosis of myocardial infarction is performed using tests that are sold in pharmacies. They work on the same principle as pregnancy tests. The biological material used is distinctive. Blood is used to determine abnormalities in the heart.
A small amount of biological material is applied to the test strip.
A temporary pause is maintained so that the substances can react.
Evaluate the result. If one line appears, then there is no disease. If two, you need to urgently seek medical help. If there are no marks on the test strip, the result is considered unreliable. This may indicate an expiration date or a manufacturing defect. The study needs to be repeated.
Reliability of results
It is important to understand that in the first minutes after the onset of symptoms, the amount of tropins in the blood is small. They have not yet had time to enter the bloodstream, since the process of necrosis is slow. If the test result is negative, but the symptoms are clear, then the test should be repeated after 3-4 hours.
If suspicions are confirmed, you should immediately consult a doctor. But when the test result is negative again, and the symptoms do not go away, this is a completely different disease, and clinical studies are needed.
Late diagnosis
Very often, doctors are faced with the fact that people do not pay attention to mild symptoms and suffer the disease “on their feet.” When the symptoms reappear, then the patient runs to a medical facility for help. A standard echocardiogram will show that there are abnormalities in the heart, but will not be able to accurately determine the cause.
In this case, a troponin test for infarction will help. In the first 4-6 hours, the amount of proteins increases sharply, the peak concentration usually occurs after 14-20 hours. Once in the bloodstream, they remain there for 10-15 days. Therefore, it is possible to determine the past disease even after a week.
A set of reagents for immunochromatographic detection of cardiac markers in whole blood.
Set contents:
- Test plate in sealed packaging 1 piece
- Buffer in a test tube 1 piece
- Scarifier 1 piece
- Alcohol wipe 2 pcs.
- Pipette 1 piece
- Instructions 1 piece
Store in a dry place at a temperature of 2 to 28 degrees
Physical examination
A physical examination involves the use of research methods that do not require the use of additional equipment. To make a diagnosis during a physical examination, a highly trained specialist is required.
During the physical examination, the specialist may use the following methods:
- To make a diagnosis, a specialist needs to know how long ago the chest pain began and its nature;
- in some cases, it is possible to clarify the factor that provoked the pain;
- it can be physical or psycho-emotional stress.
- represents palpation of tissues;
- when it comes to myocardial infarction, it is necessary to detect a point of the myocardium tightly pressed to the anterior chest wall;
- if there are no anomalies, then it is located in the fifth intercostal space on the left, perpendicular to the clavicle;
- the area of this point can be from 2 to 4 cm2;
- displacement can be observed with some complications, for example, myocardial aneurysm;
- enlarged lymph nodes may indicate the development of an inflammatory process; as for a heart attack, such changes can be detected in the acute and subacute period;
- The pulse rate is also determined by palpation;
- a heart attack may be accompanied by a weakened heartbeat, the pulse is difficult to feel, and, as a rule, an arrhythmia is detected.
- the specialist taps the front wall of the chest to determine the boundaries of the heart;
- as a rule, no specific changes are detected;
- due to disruption of the myocardium and congestion, expansion of the left ventricle may be observed, then a shift of the myocardial border to the left will be recorded;
- expansion of the boundaries is observed with pericarditis and aneurysm.
- in other words – listening;
- To do this, the doctor uses a stethoscope to determine abnormal noises by ear;
- a heart attack is characterized by a weakening of the first sound, the presence of a systolic murmur at the apex of the heart;
- detection of 3 and 4 pathological tones indicates left ventricular failure;
- several days after the attack (3-4), you can hear a pericardial friction rub.
Read also: Angina pectoris myocardial infarction
Temperature and pressure are also measured. The pressure is usually reduced, which is caused by improper implementation of the pumping function.
Myocardial infarction Express test “CARD-INFO”, pcs.
The only immunochromatographic express test in Russia for myocardial infarction using the BSJK protein “Card·Info” - which allows you to diagnose myocardial infarction at the earliest stage using 1 drop of blood from a finger in 10-15 minutes .
Already in the first hour to an hour and a half after the onset of a heart attack, the test will detect damage to heart muscle cells by increasing the cardiac marker in the blood - BFA, which is the very first to respond to changes.
Manufacturer: OFK-Cardio LLC, Russia
We work with orders from 10 thousand rubles.
Methods of diagnostic studies for suspected myocardial infarction
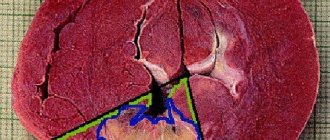
Myocardial infarction, an acute form of coronary heart disease (CHD), is characterized by the development of local necrosis (death) of the heart muscle. The death of myocardial tissue is caused by an absolute deficiency or relative insufficiency of blood supply in this area. Modern research methods make it possible to diagnose a critical condition at the initial stage and differentiate myocardial infarction from other diseases with similar symptoms.
Simplicity and ease of early diagnosis of Myocardial infarction
- Using the CARD-INFO test kit makes it possible to carry out analysis at home, in an ambulance, in the intensive care unit, in the laboratory, at the patient’s bedside (at the place of treatment):
- visual recording of the result;
- 1 drop of capillary blood is used;
- test evaluation time 10 minutes;
- the test kit contains everything necessary for diagnostics;
- the analysis can be performed by both nursing staff and the patient himself at home
Cardiac markers
If an acute form of ischemic disorders in the myocardium is suspected, then to determine the problem, an analysis is performed for:
- Creatine phosphokinase. This enzyme is found in the muscles of the heart and skeleton. If his indicators deviate upward from the norm, then this indicates an injury. Therefore, if it is necessary to identify a necrotic process, it is necessary to determine the level of the CPK-MB fraction. It is found in brain and lung tissue. A significant increase in the main indicator and its fraction confirms the presence of a heart attack.
- C-reactive protein. He says that an inflammatory process develops in the human body. This occurs in many diseases, including heart attack. A protein test is prescribed to assess the risk of developing pathology. It is normal if CRP in the body is from 0 to 5 mg/l.
- Troponina. They are tissue enzymes. Contained only in myocardial muscles. If a blood test shows an increase, this always indicates the development of a heart attack. Under normal conditions, this substance should not be present in the blood. If cardiac necrosis occurs, the protein leaks into the bloodstream. Using this test, a diagnosis can be made within a few hours after the attack. After two or four hours, its content rises and remains at a high level for two to three weeks.
Laboratory tests alone do not provide an accurate diagnosis. If a heart attack is suspected, the patient must be prescribed ECG monitoring. If necessary, an ultrasound examination of the heart is performed. Identification of a suspected heart attack is carried out only in a hospital setting. If the diagnosis is confirmed, the patient is immediately provided with appropriate assistance. In case of acute circulatory disorders in the myocardium, it is important to carry out treatment as soon as possible. The size of the necrotic lesion and the severity of complications, as well as the patient’s chances of maintaining working capacity and life, depend on this.