Transmural myocardial infarction (penetrating myocardial infarction) is a cardiac disease in which necrosis of the entire thickness of the heart muscle occurs against the background of an acute lack of blood supply to the organ, followed by replacement of the necrosis focus with connective tissue.
If you suspect a myocardial infarction, you should immediately call an ambulance, without waiting for the full clinical picture to unfold - it is impossible to make an accurate diagnosis without an instrumental examination.
Myocardial infarction is a serious pathology that is one of the main causes of death among the population. In the age group of 40 to 50 years, myocardial infarction is more often found in men. After 50 years, the incidence in men and women is comparable. The prognosis for this disease largely depends on the timeliness of diagnosis of the pathology and treatment, but primarily on the type of heart attack and the degree of damage to the heart muscle. About 20% of the total number of sudden deaths occurs in the transmural form of myocardial infarction, which is the most dangerous variant of this disease, since the entire wall of the organ is affected. It is in this form that medical care often does not have time to be provided. Another 20% of patients die in the first month after suffering a heart attack of this form.
Most often the anterior wall of the left ventricle of the heart is affected, less often the right ventricle and atrium. You can see what the macroscopic specimen looks like for this form of heart attack in the photo.
The gross specimen shows the affected area of necrosis, spreading throughout the entire thickness of the heart muscle.
Peculiarities
The prefix “trans” in medicine and biology means “through”, “through” . Transmural differs from other types of heart attack in that with it, cell death occurs not only in the middle cardiac muscle, but also in other layers of the heart - the epicardium and endocardium.
The necrotic focus, that is, the zone in which the cells have died and undergone necrosis, penetrates the wall of the heart through and through. Other forms of myocardial infarction do not affect the outer and inner membranes of the heart, being limited only to the middle, muscular layer.
About 1/5 of all sudden deaths occur due to transmural infarction . The disease is 5 times more common in men than in women. Of all those who have suffered this form, up to 19-20% die in the first month.
Development mechanism
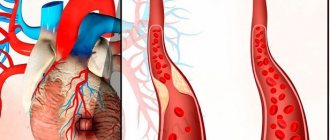
Approximately 9 out of 10 heart attacks progress against the background of atherosclerotic lesions of the coronary arteries. A protein-lipid tumor (atherosclerotic plaque) forms inside the wall of a large vessel through which blood flows to the heart (mainly to the coronary artery). This process develops as a result of impaired metabolism (for example, with an increased amount of cholesterol in the blood, hyperlipidemia).
Due to unstable blood pressure, the integrity of the inner wall of the vessel is compromised, while the contents of the plaque block part of its lumen, forming a barrier to full blood flow. This phenomenon is called fat embolism.
There is also another development scenario: red blood cells with platelets adhere to the damaged vessel wall, as a result of which a blood clot (thrombus) appears, which over time increases in size and blocks the lumen of the vessel.
Under such conditions, the heart muscle does not receive a sufficient volume of blood, which under normal conditions ensures its full functioning.
Causes and risk factors
Heart attacks occur as a result of insufficient blood supply to an organ or its area.
Deprived of access to oxygen and nutrients, cells begin to die, that is, necrosis occurs. Transmural myocardial infarction occurs according to the same pattern. Blood supply disturbances occur due to the fact that the lumen of the coronary artery is blocked by an atherosclerotic plaque . As a result, the heart does not receive enough oxygen and nutrients, but in a calm state this is not dangerous.
When a stressful situation occurs or a person is engaged in intense work , the speed of blood flow increases, and a turbulent vortex appears around the plaque. It damages the inner surface of the vessel and causes the formation of a blood clot, which further complicates the blood supply to the heart.
As a result of the lack of oxygen, which is supplied to the cells of all three layers of the heart along with the blood, the death of these cells begins.
The root cause of this type of heart attack is the presence of sclerotic plaques in the coronary arteries. Risk factors are:
- Age (transmural infarction – a disease of people over 45 years of age);
- Genetic predisposition;
- Increased blood cholesterol;
- Obesity;
- Smoking tobacco;
- Physical inactivity;
- Stressful situations;
- Wrong diet;
At the same time, more than 35% of cases are associated with smoking , which makes it the most important risk factor.
Transmural myocardial infarction: complications and prognosis for treatment
Transmural myocardial infarction is a very severe acute cardiac disease characterized by the death of a large volume of tissue. Lack of timely assistance can cause death. Often, death can occur from early or late complications during intensive care.
What is a heart attack
The term infarction defines tissue death, which is caused by a sudden cessation of the supply of nutrients and oxygen from the blood. Cardiac muscle cells (myocardium) perform a very large amount of work, so they quickly die under starvation conditions.
Conventionally, the pathological process in the heart can be divided into several stages:
- A sharp disruption in cell nutrition, occurring as a result of the almost complete cessation of blood flow into the microvasculature. Usually the condition develops against the background of blockage of one or more coronary arteries that supply the myocardium. The larger the caliber of the blocked vessel, the worse the prognosis, since a significant amount of tissue dies.
- Direct death of myocardial cells (myocardiocytes), accompanied by the development of an inflammatory reaction and severe clinical symptoms.
- Gradual restoration of the functional state of the heart with the replacement of dead cells with connective tissue (scar formation).
The triggering factor of the pathological process is blockage of the artery by a thrombus against the background of vascular atherosclerosis (deposition of cholesterol in the walls of the arteries in the form of plaques, narrowing the lumen and increasing the likelihood of thrombus formation). A high risk of death with a large infarction exists at the stage of tissue death, as well as scar formation.
Causes
The main pathogenetic mechanism for the development of a heart attack is a sharp restriction or complete cessation of blood flow in one or more coronary arteries. This most often occurs due to blockage by a blood clot against the background of the development of atherosclerosis, which is possible due to the influence of several common provoking factors:
- Gender – Men have a higher risk of developing a major heart attack than women.
- Age – in people over 45 years of age, the likelihood of a cardiovascular accident increases significantly.
- A genetic hereditary predisposition that determines an increase in cholesterol levels with its subsequent deposition in the walls of the arteries, as well as an increase in systemic blood pressure. At the same time, the risk of the pathological process may increase at a younger age.
- Long-term exposure to stressful situations, negative emotions, chronic lack of sleep and overwork are factors that are a frequent companion of modern man.
- Low physical activity throughout life.
- Obesity, passion for fatty, fried foods.
- Bad habits - smoking, systematic drinking of alcohol cause changes in blood vessels with subsequent thrombus formation in them.
Important! In 35% of cases, the development of transmural myocardial infarction is diagnosed in smoking men over 40 years of age.
Knowledge of provoking factors allows a person, if necessary, to change his lifestyle and prevent the development of cardiovascular pathology.
Classification of myocardial infarction involves differentiation of the pathological process based on certain criteria:
- The duration of the course is acute (up to 6 hours), acute (up to 14 days), subacute (up to 12 months) periods from the onset of the disease and the late stage of scar formation.
- The volume of the lesion is small-focal, large-focal infarction.
- Anatomy of changes - transmural (tissue death affects the entire thickness of the heart wall), non-transmural, subendocardial or subepicardial infarction.
- Localization – damage to any (anterior, posterior) wall of the left ventricle, apex of the heart, septum.
- The course is protracted, recurrent (periods of improvement followed by deterioration), cyclical.
Classification makes it possible to carry out high-quality, reliable diagnosis of the disease, as well as predict the further course. Damage to the anterior wall is characterized by a higher incidence of complications.
Signs of a heart attack
In most cases, the possible development of myocardial infarction is indicated by characteristic clinical signs:
- Acute pain is the most common and characteristic manifestation of myocardial malnutrition. With transmural damage to the heart, it is characterized by significant intensity. Usually radiates to the left arm, shoulder, ear, jaw. In case of changes in the lower wall of the left atrium, pain may mimic stomach problems.
- Emotional changes - against the background of severe unbearable pain, a feeling of anxiety and fear of death appears.
- A feeling of discomfort in the form of palpitations, which may be replaced by freezing.
- Severe shortness of breath, even suffocation (the result of circulatory disorders in the pulmonary system).
Pain during a transmural infarction may be present for a long time, until the initiation of adequate medical care aimed at improving blood circulation in the myocardium.
Important! In a small number of cases, a painless clinical form of the course of a heart attack is noted, in which timely diagnosis of the pathological process is difficult.
Diagnostics
The main method for reliably identifying, determining the localization and severity of transmural myocardial infarction is electrocardiography (ECG). A functional study makes it possible to determine the severity of the pathological process, its localization in the right or left ventricle, as well as on the anterior, inferior or posterior wall.
Additionally, the cardiologist may prescribe the following studies:
- Visualization of the heart using ultrasound (echocardioscopy).
- Laboratory determination of infarction marker enzymes in the blood (when myocardiocytes are damaged, the enzymes creatine phosphokinase and aspartate aminotransferase are released into the blood).
- Analysis of total cholesterol, as well as various classes of lipoproteins - research is necessary to predict the possible development of cardiovascular pathology in the future.
- A clinical blood test in which an increase in leukocytes indicates the development of an inflammatory reaction.
If necessary, consultations are held with doctors of related specialties. Based on the results of a comprehensive diagnostic examination, the cardiologist determines further therapeutic tactics.
First aid
In order to alleviate the condition of a sick person, as well as minimize the possibility of complications, if a myocardial infarction is suspected, several measures should be taken:
- Call an ambulance.
- Place the person on a horizontal surface and ensure peace. If there is severe shortness of breath or the appearance of wheezing, indicating the possible development of pulmonary edema, the patient should be transferred to a semi-sitting position.
- Provide fresh air flow.
- If possible, give a Nitroglycerin tablet under the tongue. If the pain in the heart area does not decrease within 5 minutes, you can give one more, but no more than 3 pieces.
- To reduce the likelihood of further thrombus formation, aggravating the course of the pathological process, you can give an Aspirin tablet.
Further activities include specialized care, which is carried out in a medical hospital.
Health care
Treatment of transmural infarction is carried out in an intensive care unit or infarction unit.
It includes several main areas:
- Reducing the severity of pain and combating shock, for which analgesics and sedatives are used.
- Normalization of hemodynamic parameters (heart rate, systemic blood pressure).
- Thrombolytic therapy – dissolution of a blood clot that has blocked a coronary artery (streptokinase, fibrinolysin are used).
- Prevention of the formation of new blood clots with Heparin.
- Treatment of arrhythmia (irregular heartbeat), which increases the risk of blood clots in the cavities of the heart. For this purpose, medications from the beta blocker group are usually prescribed.
The dosage, regimen of drug administration and duration of therapy are determined individually by a cardiologist.
Restoration of the body
Life after a transmural infarction requires some modification.
After discharge from the medical hospital, rehabilitation measures are carried out:
- Follow a diet excluding fried and fatty foods.
- A diet with frequent but small meals at least 5 times a day.
- A gradual expansion of physical activity, which is carried out through walking.
Rehabilitation is recommended to be carried out in a special sanatorium. This will allow you to restore the functional state of the heart as much as possible, as well as avoid complications.
Forecast
The completeness of restoration of the functional state of the heart and the patient’s quality of life after a major heart attack depend on the location and extent of tissue damage.
The pathological process is often accompanied by the development of complications, which include:
- Pulmonary edema due to a decrease in the intensity of blood flow in them.
- Severe arrhythmia.
- Re-formation of blood clots in various vessels with subsequent complications in the form of repeated cerebral infarction or stroke.
- Infectious complications, including pneumonia (pneumonia) and sepsis (blood poisoning).
- Acute heart failure.
- Changes in the properties of the heart wall, which is accompanied by rupture and development of hemopericardium (hemorrhage into the pericardial cavity).
The development of any of the complications significantly worsens the prognosis and can cause death.
A very important measure is the prevention of cardiovascular pathology and transmural myocardial infarction, which makes it possible to increase the duration and quality of human life.
Sources: https://kardiobit.ru/bolezni-serdtsa/infarkt/transmuralnyj-infarkt https://cardiograf.com/ibs/nekroz/transmuralnyj-infarkt.html
Complications and consequences
Of all the types of heart attack, this type is the most dangerous, as it affects all three linings of the heart. Depending on the area of nektrotic changes, small-focal and large-focal transmural infarction are distinguished. The latter is characterized by numerous and very dangerous complications , including:
- Thromboembolism;
- Pulmonary edema (causes, clinical picture, treatment tactics);
- Paralysis of limbs;
- Speech disorders;
- Ventricular fibrillation, which leads to death;
- Failure of various organs and systems;
- In severe cases, heart rupture.
Small blood clots, which form in large quantities during a heart attack, can be carried through the bloodstream into the brain or spinal cord, clogging the capillaries and depriving certain parts of these organs of blood supply. This is what causes speech impairment or paralysis .
Blockage of blood vessels with blood clots can lead to failure of any organs and is one of the most dangerous complications.
Cardiac rupture occurs suddenly and represents a violation of the integrity of the heart in the area affected by necrosis. The larger the area, the greater the likelihood of a rupture.
Ventricular fibrillation is a phenomenon in which, instead of normal contractions, the ventricles of the heart begin to tremble randomly . At the same time, they cannot push out blood, which is why the blood supply to all organs and systems is stopped, which are left without oxygen and nutrients.
Ventricular fibrillation can soon turn into flutter - a trembling with a frequency of up to 400 Hz. In this state, the heart also cannot provide blood circulation, and therefore death soon occurs.
Causes
Development factors are approximately the same and do not depend on the form of the pathological process. Acute transmural infarction is the result of atherosclerosis of the coronary arteries. The disease occurs in two clinical forms.
- The first is narrowing (stenosis) of blood vessels. Develops in chronic hypertensive patients with extensive experience, patients who smoke, abuse alcoholic beverages and psychoactive substances.
The process is stopped using conservative methods. If ineffective, surgery is prescribed for stenting, ballooning (mechanical expansion of the lumen) or prosthetics of the affected vessel.
- The second possible form is blockage or occlusion of a coronary artery by a blood clot or cholesterol plaque. Statins and drugs to dissolve blood clots are used.
With urgent help, necrosis does not have time to form. You need help in the first 4-6 hours, preferably earlier.
Other factors cause only atherosclerosis or impaired blood flow.
Hypertonic disease
A persistent increase in blood pressure in the patient. It develops as a response to congenital genetic factors, poor lifestyle, excess salt and other factors.
High blood pressure levels affect vascular tone. They become sharply stenotic within minutes. Acute ischemia occurs.
Depending on the extent of the lesion, different types of infarction may form. This cannot be allowed. Hypertension responds well to treatment only in the initial stages (first and second), problems arise in the third. But the issue is also solvable.
Metabolic defects
Generalized name of pathological processes. The main objective sign is a violation of lipid metabolism and fat storage. Such patients often have increased body weight. But heavy weight is not the culprit in itself. This is a consequence.
Hypoxia
As a result of carbon monoxide poisoning, mechanical asphyxia, and other issues associated with insufficient cellular metabolism. Restoration is carried out urgently.
The likelihood of such an outcome is relatively low. About 7-12% of cases result in transmural infarction.
Hyperthyroidism
Excessive production of thyroid hormones. T3, T4, also pituitary TSH. It’s hard to say what the reasons are. Organ tumors, inflammatory autoimmune pathologies (Hashimoto's thyroiditis), a diet high in iodine or living in areas with an excess of this element.
Therapy under the supervision of an endocrinologist. A heart attack does not develop overnight; it takes a long time. We are talking about a late complication.
Diabetes
Chronic illness. Associated with insufficient insulin production or decreased tissue sensitivity to it.
Lifelong therapy. Vessels throughout the body are the first to be affected. Deep vein thrombosis of the lower extremities leads to gangrene, disturbances in the anatomy of the retinal arteries - angiopathy and blindness. And damage to the structures of the heart ends in a heart attack.
The likelihood can be reduced only with constant treatment under the supervision of specialists.
Excessive cortisol production
Adrenal cortex hormone. The disease is the result of tumors of the paired organ itself or a pituitary adenoma, the so-called corticotropinoma. The clinical variant of the pathological process is Itsenko-Cushing syndrome.
Patients with this diagnosis are clearly visible during the initial examination. Gynecomastia, obesity, moon face, high blood pressure, shortness of breath, constant fatigue, problems with the musculoskeletal system.
Smoking
Long-term consumption of tobacco products. Provokes chronic vascular stenosis. After 3-5 years, the risk of metabolic abnormalities also increases almost threefold.
Giving up a bad habit when the body becomes addicted no longer gives a 100% effect. Long-term rehabilitation will be required, from 3 months to a year.
Alcohol abuse
Alcohol does not have a positive effect, this is a myth. According to some studies, cholesterol begins to be more actively absorbed by the body and deposited on the walls of blood vessels, which leads to atherosclerosis even with small amounts of food consumption rich in fat.
Congenital and acquired heart defects
Not detected in the early stages. Sometimes there are no symptoms at all for many years. The problem is revealed after the development of an emergency condition: a heart attack or cardiac arrest.
Some anatomical defects are more obvious: stenosis or prolapse, regurgitation of the mitral, aortic and tricuspid valves.
In the short term (several years) they lead to hemodynamic disturbances. The blood is not completely ejected into the systemic circle, and myocardial ischemia develops. This is the only factor that is not related to atherosclerosis.
Over time, the heart changes at the cellular level. Insufficient trophism leads to thickening of the cardiac structures, and stagnation of blood in the chambers ends with their expansion (dilatation). Cardiomyopathy is diagnosed.
Sex and age characteristics
Patients aged 40-50 years and older are at greater risk. The reason is insufficient synthesis of specific hormones.
Disturbances are especially noticeable in the body of representatives of the fairer sex, because estrogen and progesterone are no longer synthesized in normal volumes. Namely, these substances dissolve lipid structures, cholesterol and prevent vascular stenosis.
Statistics:
Transmural infarction is more common in men. The ratio is approximately 4:1, as is the case with other forms of the disease process. Women suffer less often, but the mortality rate of the condition is almost three times higher.
Symptoms
Symptoms can be different and depend on the characteristics of the disease. But there is also a group of symptoms common to most survivors of acute transmural myocardial infarction:
- Frequent, painful heartbeat (tachycardia);
- Feeling of “fading” of the heart;
- Acute compressive pain that radiates to the left arm, left shoulder blade, left half of the lower jaw, teeth, left ear;
- Pallor of the skin and mucous membranes;
- Wave-like, prolonged pain that may not go away from several hours to days;
- Asthma-like asthma attacks (cardiac asthma).
Features of treatment
Treatment of extensive transmural infarction begins as soon as possible. First aid must be provided immediately after the onset of the attack; the patient must be transported to the hospital no later than 6 hours later. Surgical treatment is effective only during the first 12 hours after the onset of pain, sometimes 24.
First aid
The main tasks of first aid are to minimize myocardial ischemia and quickly call a doctor. First of all, the patient must be persuaded to stop current activities and take a semi-sitting position. This way you will already reduce the load on your heart. Then it is advisable to provide an influx of fresh air, replace tight clothing with loose ones, or at least unfasten the belt or collar. Try to calm the victim.
If you have an aspirin tablet on hand, give it to the patient and ask him to chew it. A nitroglycerin tablet is placed under the tongue. Nitroglycerin administration is repeated twice with an interval of 5 minutes. Low blood pressure is a contraindication to taking the drug.
Acute transmural myocardial infarction is usually very severe and is characterized by a high rate of prehospital death. Therefore, the patient should not be left alone for a minute. There is a high chance that he will need CPR. You need to be prepared for this.
Medications
The administration of medications begins while the patient is being transported. This allows you to minimize the area of necrosis foci. In the first few days, the patient is administered the following medications:
- Painkillers, sedatives. Relieves pain and improves blood supply to the heart muscle. Typically, the presence of IMT involves the administration of narcotic analgesics: morphine, fentanyl with droperidol.
- Drugs that prevent blood clot formation. They help stabilize the size of an existing blood clot and prevent the formation of a new one. The drug of first choice is regular aspirin. Its use can significantly improve the prognosis. Clopidogrel, ticagrelor, heparin, and bivalirudin are also used.
- Thrombolytics. Dissolves a blood clot (55% probability), reduces mortality. The main representatives are streptokinase, tenecteplase, alteplase, purolase.
- Beta blockers. They reduce the oxygen demand of the myocardium, make the heart work more economically, and prevent rhythm disturbances. The most commonly used drugs are esmol, propranolol, and metoprolol.
- Inhibitors of the renin-angiotensin system. Lower blood pressure and improve the functioning of the heart muscle. The drugs of choice are captopril, ramipril, valsartan, spironolactone.
Surgical procedures
Transmural infarction requires immediate percutaneous coronary intervention (PCI), a surgical procedure that reverses thrombosis in the coronary arteries. PCI is performed within the first 12 hours after the onset of the attack. This allows us to minimize the consequences of myocardial infarction for the patient.
Stenting procedure.
The surgeon inserts a catheter equipped with a balloon into a large vessel of the limb. Then it moves it to the narrowed area, controlling the movement using a computer. Having reached the pathological area, the surgeon performs a series of balloon inflations. The lumen of the vessel expands, blood flow is restored.
Typically, after ballooning, stenting of the artery is performed. Through the same vessel, the doctor inserts a miniature frame. Installing a stent helps prevent re-narrowing of the artery.
Diagnostics
In order to diagnose transmural myocardial infarction, you need to perform an ECG . Since electrocardiography is based on the study of electrical potentials in different parts of the heart, and with necrosis, the pattern of distribution of these potentials changes dramatically, an experienced specialist will be able, based on the ECG, to find out where the lesion is located, and approximately its area, and to distinguish transmural infarction from other types of necrotic changes in heart.
The area of the affected area can be determined based on a blood test . So, after a heart attack, the number of white blood cells (leukocytes) increases. Leukocytosis can last up to 14 days, and when the number of leukocytes begins to decrease, the sedimentation rate of red cells (erythrocytes) increases.
How to localize transmural infarction using ECG
Most often, transmural infarction develops in the left ventricle, on the anterior, posterior, lateral, inferior walls, and apex. The right ventricle is much less likely to suffer. Below I have placed a table that shows changes in the electrocardiogram with different localization of the lesion, as well as information about the blockage of which particular vessel led to this situation.
| Localization of transmural infarction | Which vessel is blocked? | Characteristic signs of a lesion in standard leads of an electrocardiographic study |
| Front wall | Left coronary artery or its branches | Chest leads V4-V6 |
| Bottom wall | Right coronary artery or circumflex branch of the left | II, III, aVF - ST is elevated with positive T, sometimes large Q |
| Tops | Anterior interventricular artery | II, III, aVF, V1-V6 - ST elevated, T inversion, Q - deep |
| Right ventricle | Right coronary artery | III, right V1-V4 - ST elevated |
| Rear and side | Circumflex branch of the left coronary artery | V5, V6, - deep S, drop in amplitude R; II, III, aVF, V5, V6 - jagged QRS; V1, V2, V3 - reciprocal changes; Reliable transmural myocardial infarction on ECG in III, aVF, V5, V6 - QS complexes |
| Lateral basal | aVL - ST is raised, V1-V2 - high R, the ST segment is lowered. | |
| Posterior basal | Right posterior descending artery or left circumflex artery | Reciprocal only: V1-V2 - amplitude R increased, depth S decreased; V1-V4 - decrease in ST; V1-V4, aVR - positive high T |
| Extensive along the back wall | Right coronary artery, above the origin of branches to the AV and sinus nodes | II, III, aVF - pathological Q, elevated ST, altered T; V6 - deep S. Reciprocal: V1 – V2 - increase in R, decrease in S; V1 – V3 - positive elevated T; V1 – V4 – ST decrease |
The most pronounced symptoms are acute transmural infarction of the anterior wall of the left ventricle myocardium.
If, with an extensive transmural infarction, conduction blocks develop along the posterior wall of the left ventricle, it means that necrosis has spread to the septum between the ventricles.
First aid
Transmural infarction is a very dangerous condition; death can occur suddenly and at any time, therefore, assistance measures must begin before the doctor arrives. Here is a list of such events:
- Call an ambulance;
- Place the patient in a horizontal position;
- The patient should take nitroglycerin - 1 tablet. If the pain does not go away, take another one after 5 minutes. You should not take more than 3 tablets;
- You should also take an aspirin tablet;
- If there is shortness of breath and wheezing in the lungs, the patient should be placed in a sitting position, and a bolster or pillow should be placed under his back.
For more information about helping a patient with a heart attack and loss of consciousness, watch the video:
These simple measures will help save the patient’s life before specialists arrive.
Diagnosis of the heart disease in question
The main symptom that you will encounter at the prehospital stage is a sharp pain in the chest that does not go away on its own. The patient is unable to move, complain, or help himself. There may be shortness of breath, acceleration of respiratory movements, and sometimes loss of consciousness must be noted.
Read on the topic: Lymphostasis of the lower extremities - what it is and how to treat it, photo
There will be characteristic changes on the cardiogram - pronounced elevation of the ST segment, followed by depression of the Q wave. In addition, there is another laboratory diagnostic method that clearly indicates myocardial infarction - this is the troponin test.
After it is carried out, we can say for sure that there is necrosis of the heart muscle, however, the result of this study has more legal significance as a confirmatory diagnosis, since no one will wait to receive it, it is too long. Its essence lies in the detection of proteins that can appear in the body only due to necrosis of the heart muscle.
Treatment tactics
At the hospital stage, treatment is based on three areas:
- Fighting pain and psychological consequences;
- Fighting blood clots;
- Combating heart rhythm disturbances.
To relieve the patient of pain, strong narcotic drugs , including morphine and promedol, and to combat fears and agitation, tranquilizers are used, for example, Relanium.
Thrombolytic therapy is aimed at eliminating blood clots in the coronary vessels and restoring normal blood supply to the heart. For this purpose, drugs such as fibrinolysin, alteptase, and heparin are used. The fight against blood clots must begin in the first hours after a heart attack.
To combat arrhythmias , drugs that block beta-adrenergic receptors (atenolol) and nitrates (nitroglycerin, already mentioned) are used.
In this case, maintenance therapy can continue for the rest of the patient's life.
Treatment methods
In the first few hours, the patient is hospitalized in the cardiology department of the hospital. Urgent measures are needed to stabilize the condition. There is no time to think.
The list of diagnostic measures is minimal: ECG, assessment of blood pressure, heart rate, auscultation and palpation of the pulse.
Then the use of Epinephrine and Adrenaline is indicated to restore heart rate. The method also has the opposite effect - asystole (cardiac arrest) is possible, so the feasibility is determined by the extent of the lesion.
The pain syndrome is relieved with Nitroglycerin, narcotic analgesics and non-opioid drugs. Depends on the intensity of the discomfort. Embolism is eliminated by taking thrombolytics.
After initial measures, the patient is transferred to intensive care. Cardioprotectors, agents for restoring cerebral blood flow, painkillers, and diuretics are prescribed as needed.
Elimination of the root cause of the condition is indicated in the short term, after partial compensation. Operations are the problem. A patient who has had a heart attack may not be able to withstand anesthesia. The issue is resolved after careful evaluation.
Rehabilitation
During the rehabilitation period, proper nutrition is very important . Food should be non-rough, easily digestible and taken in small portions 5-6 times a day. At first, the diet should consist of cereals, dried fruits, juices and kefir. Dried apricots, beets and other foods that promote bowel movements are also useful.
Over time, the diet expands and the eating pattern becomes normal, but fatty foods high in cholesterol should be avoided throughout life.
Physical rehabilitation involves gradually returning the patient to physical activity . In the early stages, it is important to prevent congestion in the lungs, muscle atrophy and other consequences of an immobile lifestyle. Gradually, as the patient recovers, exercise therapy and walking begin.
It is advisable to carry out rehabilitation measures in sanatoriums . The rehabilitation period is individual and depends on both the area of cardiac damage and complications.
Emergency care volume
The most important condition, without which there can be no question of the patient’s survival, is timely care provided at the prehospital stage, as well as his timely hospitalization in the intensive care unit. What is difficult is that the provision of medical care falls to people who are far from medicine. There are a few important things to remember:
- Sharp pain in the chest is a reason to suspect the presence of penetrating myocardial infarction or a milder form of this disease and begin the necessary measures.
Drugs that are indicated in the treatment of extensive penetrating infarction (as well as other clinical forms of this disease) are fast-acting nitrates (Nitroglycerin), beta blockers (preferably selective - Bisoprolol, Metoprolol), as well as painkillers. According to all clinical standards of treatment, the use of narcotic analgesics is recommended, but they can only be provided by emergency doctors, so ordinary people will have to be content with only non-steroidal anti-inflammatory drugs (dicloberl, movalis and others). In addition, it would be a good idea to use sedatives (gidazepam) in order to neutralize the effect of the sympathetic nervous system.- An equally important task is the timely hospitalization of a victim with a posterior wall myocardial infarction - even if the symptoms of this disease can be miraculously relieved, subsequent treatment should still be carried out in a specialized hospital department.
Even at the slightest suspicion of the development of an attack of unstable angina pectoris, it is necessary to take the patient to the hospital, since this condition can have the most unfavorable consequences.
Prevention
Prevention measures boil down to eliminating the risk factors listed above. To avoid transmural infarction, you must:
- Stop smoking;
- Follow a low-cholesterol diet;
- Reduce table salt consumption;
- Fight obesity;
- Monitor blood pressure (it should not exceed 140/90 mmHg);
- Avoid severe stress;
- Avoid heavy physical activity.
Transmural infarction differs from other types of myocardial infarction in that it affects not only the myocardium, but also two other cardiac membranes (epicardium and endocradium), consisting of connective tissue. For this reason, the likelihood of heart rupture and thromboembolism increases.
Prognosis, complications
Transmural infarction is the most severe form of myocardial infarction and has an extremely poor prognosis. Most patients do not even survive until the ambulance arrives; another 15% die on the first day from related complications. After completing the rehabilitation period, 4 out of 5 patients are diagnosed with chronic heart failure.
Main types of complications:
- cardiogenic shock;
- ventricular fibrillation;
- ventricular tachycardia;
- acute heart failure;
- blockade of the atrioventricular node;
- rupture of the wall of the left ventricle or interventricular septum;
- post-infarction angina;
- Dressler's syndrome;
- left ventricular dysfunction;
- heart rhythm disturbances;
- atrial fibrillation.
Health care
Treatment of transmural infarction is carried out in an intensive care unit or infarction unit.
It includes several main areas:
- Reducing the severity of pain and combating shock, for which analgesics and sedatives are used.
- Normalization of hemodynamic parameters (heart rate, systemic blood pressure).
- Thrombolytic therapy – dissolution of a blood clot that has blocked a coronary artery (streptokinase, fibrinolysin are used).
- Prevention of the formation of new blood clots with Heparin.
- Treatment of arrhythmia (irregular heartbeat), which increases the risk of blood clots in the cavities of the heart. For this purpose, medications from the beta blocker group are usually prescribed.
The dosage, regimen of drug administration and duration of therapy are determined individually by a cardiologist.
Causes of transmural infarction in children and adults
In the clinical picture of the transmural form of infarction, the following periods are distinguished:
- Premonitory.
- Acute (stage of ischemia).
- Acute (necrosis stage).
- Subacute (stage of organization).
- Post-infarction (scar stage).
Myocardial infarction has several course options and can be characterized by various symptoms. This largely depends on the type, type and stage of the disease. Depending on the affected area, it can be:
- Large-focal. Several extensive lesions are noted. Clots form in the vessels, which travel through the bloodstream to various organs. This causes an aneurysm or heart rupture. It is most often installed in cases of transmural infarction. The resulting scar does not dissolve over time.
- Finely focal. Based on the diagnostic results, one or more small foci of the pathological process are identified. Can transform into macrofocal. In some cases, thromboembolism and heart failure occur. This type is not characterized by serious circulatory disorders.
Based on the changes observed on the electrocardiogram, there are:
- Q-infarction. This form is characterized by the formation of a pathological scar.
- Not a Q-heart attack. There is no scarring stage and is manifested by negative T-waves.
Based on location and depending on the damage to certain areas of the coronary arteries, the following are distinguished:
- Left ventricular. There may be an infarction of the lateral, posterior or anterior wall, as well as the interventricular septum.
- Right ventricular.
DETAILS: Anteflexio uterine position: normal position of the uterus in the pelvis
Depending on the location of the pain, several forms are distinguished. These include:
- Typical. Pain occurs behind the sternum or in the precordial region.
- Atypical.
- Peripheral. Pain sensations radiate to the lower jaw, left shoulder blade and arm, and larynx.
- Asymptomatic. Signs of the disease are not clearly expressed.
- Combined. Symptoms can occur in different parts of the body.
- Painless.
The stages of a heart attack in accordance with the stage and dynamics of development include:
- Stage of ischemia. The most acute is when the strongest pain occurs.
- Stage of necrosis. An acute period when the pain gradually subsides.
- Organization stage. Irreversible changes begin to occur in the body, and a pathological process develops.
- Scarring stage. Scars form.
With a transmural infarction, there are often several foci of development of the pathological process, which poses a danger to the patient’s life.
Large lesions are the most difficult to treat, since the lesion not only affects the upper layers of muscle tissue, but also penetrates deeper, causing irreversible consequences.
Causes of pathology
Transmural infarction is most often provoked by atherosclerosis of the coronary arteries (more than 90% of cases). A cholesterol plaque can block the lumen of a vessel on its own or trigger the process of thrombosis. More rare causes:
- heart surgery (bypass surgery, myocardial cauterization);
- hypertensive crisis;
- hypoxia;
- Takayasu's disease;
- systemic lupus erythematosus;
- hypoxia;
- anemia;
- tuberculosis;
- intracardiac thrombus formation in endocarditis;
- closed chest injuries;
- congenital defects in the structure of the coronary vessels.
Features of rehabilitation
Transmural myocardial infarction requires a long recovery. If there are no complications, the rehabilitation period takes 5-6 months. Severe patients recover for more than a year.
Main components of the rehabilitation course:
- exercise stress;
- modification of risk factors;
- diet;
- drug treatment;
- training, work with a psychologist.
Exercise stress
An important component of the rehabilitation process. Deprived of a large part of cardiomyocytes, the heart cannot cope even with light loads without special training. First, the patient is taught the simplest things: stand up, sit, perform lying exercises.
Then the patient is allowed to walk short distances under the supervision of a doctor, go up and down stairs, and increase the complexity of exercise therapy.
The next stage is a long walk along the street, possibly cardio exercises, and light aerobic exercise.
Modification of risk factors
There is a list of factors that increase the likelihood of relapse and complications. Their exclusion improves a person's prognosis. Therefore, rehabilitation usually includes the following components:
- To give up smoking. Cigarettes cause vasospasm and speed up the heart rate. Therefore, people who smoke have a higher chance of dying in the near future.
- Alcohol consumption restrictions. Alcohol increases the likelihood of the formation of atherosclerotic plaques and complicates the functioning of the heart. Therefore, heart attack patients need to minimize or eliminate alcohol consumption.
- Weight loss for obese patients. Obese people are more prone to developing cardiovascular diseases. The greater the weight, the more difficult it is for the heart to provide blood supply to all organs and tissues of the body.
- Blood pressure (BP) control. High blood pressure damages blood vessels. Therefore, it is necessary to ensure that its values do not exceed 140/90 mmHg. Art.
- Controlling sugar levels. Patients with diabetes should monitor glucose concentrations. High sugar content increases the risk of complications.
- Flu prevention. People who have had a myocardial infarction should get an annual flu vaccine. This disease often causes cardiac complications.
Diet, nutritional habits
After a myocardial infarction, it is necessary to control the daily amount of calories, monitor the content of salt and saturated fat. The diet should include a large amount of vegetables, whole grain cereals, herbs, fruits, low-fat dairy products, white meat, and fish.
- pickled dishes;
- pickles;
- smoked meats;
- confectionery products;
- fried food;
- deep-fried products.
Drug treatment
All patients are prescribed medications that prevent blood clots, ease the work of the heart, and prevent the formation of cholesterol plaques. Most of them will have to be taken for life. The standard rehabilitation scheme includes:
- aspirin;
- beta blockers (metoprolol, atenolol);
- ACE inhibitors (captopril, enalapril);
- statins (atorvastatin, rosuvastatin).
Training, work with a psychologist
Understanding the processes occurring in the body helps patients more easily accept the need for changes and disciplinedly follow the doctor’s recommendations. Patients who have undergone training recover faster, adapt, and their lives are happier. Working with a psychologist helps you learn how to manage stress, prevents, and treats depression.
source
Treatment
Surgical method of treatment
Treatment of a heart attack should be carried out immediately after diagnosis. Features of the pathophysiology of extensive and small-focal MI explain different treatment tactics. But in both cases, the main goal of treatment is to restore blood flow in the myocardium as quickly as possible. Treatment of the disease includes medical and surgical methods.
Transmural infarction: definition, diagnosis and patient prognosis
There are several forms of cardiac muscle necrosis, and the most deadly and destructive of them is acute transmural myocardial infarction.
The cause of the development of this pathology is an acute insufficiency of blood flow through the system of coronary arteries, which are responsible for supplying cardiac tissues with oxygen and nutrients.
This deficiency of coronary blood flow can be caused by two phenomena:
- sudden complete cessation of blood flow through the coronary arteries;
- a discrepancy between the oxygen consumption of the heart muscle and its supply through these vessels.
The cause may be atherosclerosis of these vessels, their narrowing, the formation of a single large atherosclerotic plaque, thrombosis, sudden powerful load on the myocardium, spasm of cardiac vessels associated with neurohumoral disorders.
What is the difference from other forms
Based on the location of the lesion in the heart muscle, the following forms of myocardial infarction are distinguished:
- intramural - in the thickness of muscle tissue;
- subepicardial - under the outer membrane;
- subendocardial - under the inner membrane;
- transmural - passes through the entire thickness of the muscle.
The prefix “trans” is translated as “through”. That is, the necrosis zone affects a huge array of myocardium. It passes through the entire muscle from the pericardium to the endocardium.
The seriousness of the pathology is indicated by the following fact: 20% of all registered cases of sudden death are associated precisely with the development of transmural infarction. 20% of patients affected by it die within one month.
The pathology has a clear gender link: out of 100 clinical cases of transmural infarction, 16 occur in women, and 84 in men.
How to identify and suspect
The development of the disease can be suspected based on a number of characteristic symptoms:
- pallor;
- attacks of suffocation;
- heart sinking;
- painful tachycardia;
- acute compressive or prolonged wave-like pain.
Heart pain is very common in most cases. It radiates to various anatomical formations located in the left half of the body: shoulder blade, arm, ear, part of the dentition, and so on.
Key symptoms
The symptoms of transmural myocardial infarction vary depending on the period of development of the pathology. Let's look at those stages of necrosis formation at which, subject to timely medical intervention, it is possible to save not only the patient's life, but also the integrity of his heart muscle.
Prodromal period
The patient begins to worry about warning signs similar to unstable angina:
- increased frequency of pain attacks localized behind the sternum;
- development of pain in response to physical activity that previously did not cause it, or even at rest;
- When nitro drugs are used to relieve pain, the previous dose does not bring the usual relief; more and more drugs are required to achieve the desired effect.
All these manifestations indicate rapidly developing blockage of the coronary arteries. With a further decrease in the volume of blood passing through them, myocardial infarction is likely to develop. Therefore, the clinical protocol for acute coronary syndrome requires mandatory hospitalization of such patients.
The most acute period
If time is lost and sufficient help was not provided in the prodrome, then the most acute period begins - the beginning of necrotic changes in the heart muscle. The largest number of deaths from transmural infarction occurs precisely in the acute period. Although, on the other hand, therapy carried out at this time is most effective, up to complete recovery.
Symptoms are manifested by anginal status - very strong pressing, drilling or dagger-like pain in the chest area with irradiation characteristic of the heart. Its duration is more than half an hour, even taking 3 tablets of nitroglycerin does not bring relief. A number of other symptoms are added:
- anxiety;
- cold sweat;
- fear of dying;
- severe weakness;
- hypotension (more often) or hypertension (less often).
In addition to the standard anginal attack, transmural infarction can manifest itself with atypical syndromes:
- abdominal, with epigastric pain radiating to the back, nausea, belching, flatulence, vomiting, after which there is no relief, tension in the abdominal muscles;
- atypical anginal, with pain in the limbs, lower jaw, throat;
- asthmatic, with an attack of shortness of breath, the development of which is based on pulmonary edema or cardiac asthma;
- arrhythmic, with a predominance of arrhythmia symptoms over pain or without pain at all;
- cerebrovascular, with fainting, vomiting, nausea, dizziness; sometimes with focal cerebral manifestations.
Based on the symptoms, we can suspect a heart attack, but electrocardiography will certainly help determine it. We'll talk about it in the next section.
How to localize transmural infarction using ECG
Most often, transmural infarction develops in the left ventricle, on the anterior, posterior, lateral, inferior walls, and apex. The right ventricle is much less likely to suffer. Below I have placed a table that shows changes in the electrocardiogram with different localization of the lesion, as well as information about the blockage of which particular vessel led to this situation.
| Localization of transmural infarction | Which vessel is blocked? | Characteristic signs of a lesion in standard leads of an electrocardiographic study |
| Front wall | Left coronary artery or its branches | Chest leads V4-V6 |
| Bottom wall | Right coronary artery or circumflex branch of the left | II, III, aVF - ST is elevated with positive T, sometimes large Q |
| Tops | Anterior interventricular artery | II, III, aVF, V1-V6 - ST elevated, T inversion, Q - deep |
| Right ventricle | Right coronary artery | III, right V1-V4 - ST elevated |
| Rear and side | Circumflex branch of the left coronary artery | V5, V6, - deep S, drop in R amplitude; II, III, aVF, V5, V6 - jagged QRS; V1, V2, V3 - reciprocal changes; Reliable transmural myocardial infarction on ECG in III, aVF, V5, V6 - complexes QS |
| Lateral basal | aVL - ST is raised, V1-V2 - high R, the ST segment is lowered. | |
| Posterior basal | Right posterior descending artery or left circumflex artery | Only reciprocal: V1-V2 - amplitude R increased, depth S decreased; V1-V4 - decrease in ST; V1-V4, aVR - positive high T |
| Extensive along the back wall | Right coronary artery, above the origin of branches to the AV and sinus nodes | II, III, aVF - pathological Q, elevated ST, altered T; V6 - deep S. Reciprocal: V1 – V2 - increase in R, decrease in S; V1 – V3 - positive elevated T; V1 – V4 – ST decrease |
The most pronounced symptoms are acute transmural infarction of the anterior wall of the left ventricle myocardium.
If, with an extensive transmural infarction, conduction blocks develop along the posterior wall of the left ventricle, it means that necrosis has spread to the septum between the ventricles.
Forecast: is there a chance to survive
Considering the severity of the lesion, the prognosis for transmural myocardial infarction is very unfavorable. Statistics show that 40% of patients with this pathology die before reaching the hospital.
But the chance of survival remains quite high, and it can be calculated using a special GRACE scale. The patient's risk of death is assessed as high, medium or low, depending on how many points he received based on the calculation results.
The scale takes into account the following criteria:
- age;
- whether there is congestive heart failure;
- whether the patient has previously had myocardial infarction;
- systolic blood pressure level;
- whether there is ST depression on the ECG;
- serum creatinine content;
- whether the content of cardiac-specific enzymes has increased;
- whether the patient underwent PCI in an inpatient setting.
The result represents the likelihood of the subject dying during the upcoming six months from complications of transmural myocardial infarction. This rate varies from less than 1% to 54%.
You can use the scale online using the link here.
Transmural myocardial infarction of any location is a serious challenge not only to the patient’s body, but also to doctors who will fight for his life.
And victory over the disease can only be achieved with complete mutual understanding and mutual assistance from the patient himself, his loved ones, the ambulance service, the clinic and the hospital.
Only the coordinated work of all these departments will give a person a chance of salvation.
The most accurate preliminary and error-free refined diagnosis will allow you to choose the right direction of therapy. Quick, comprehensive treatment and mandatory rehabilitation can return the patient to normal life and minimize the consequences of a heart attack.
If in your life or professional activity you have encountered patients who have had such a difficult ordeal as transmural myocardial infarction, tell us about it. Your valuable experience can be useful to anyone in order to help a person in trouble in time.
I would like to tell you about one case when a patient who was admitted to the inpatient department with a completely, seemingly unrelated diagnosis, was diagnosed with a transmural myocardial infarction after a full examination. The patient, unfortunately, died. However, the case is instructive, showing how different pathologies can enhance each other’s negative impact on the human body.
A 72-year-old female patient was hospitalized with a diagnosis of gastrointestinal bleeding. Her complaints were limited to nausea, weakness and dizziness. A day later, the heart rate was 110 beats/minute, and blood pressure was 90/60 mmHg.
There is a history of coronary artery disease, post-infarction cardiosclerosis of stage 2 NK, against the background of stage 3 hypertension, complicated by a paroxysmal form of atrial fibrillation. Comorbid osteoarthritis acted as a concomitant pathology.
As an outpatient, the patient took Bisoprolol, Losartan, Diclofenac, and Pradaxa.
During examination in the hospital, numerous erosive changes in the gastric mucosa and anemia with a rapidly decreasing hemoglobin level were discovered.
After an ECG, the film revealed acute focal changes in the left ventricle, on its anterior wall.
An immediate troponin test gave a positive result.
I would like to draw your attention to the fact that anemia is a risk factor for cardiovascular disease. It increases the occurrence of the following nosological forms:
- myocardial infarction and its relapses;
- dysfunction of the left ventricle;
- hospital mortality (almost one and a half times);
- complications from the cardiovascular system.
As would be expected, severe posthemorrhagic anemia aggravated the condition, provoked the development of transmural myocardial infarction and, ultimately, led to the death of the patient.
And the basis of all the problems, which significantly aggravated the patient’s condition, was the erroneous prescription of a combination of drugs that caused erosive damage to the gastric mucosa with subsequent gastrointestinal bleeding.
Source: https://cardiograf.com/ibs/nekroz/transmuralnyj-infarkt.html