To determine the presence of a heart attack, its location and the stage of destruction of the heart muscle, the most reliable and accessible method is an ECG. The first signs appear after the third hour from the onset of the attack, increase in the first day and remain after the formation of the scar. To make a diagnosis, the depth of myocardial destruction and the extent of the process are taken into account, since the severity of the patient’s condition and the risk of complications depend on this.
What does a cardiogram show during a heart attack?
Electrocardiography (ECG) is a test performed first when a myocardial infarction is suspected. Based on the recorded cardiogram, several conclusions can be drawn:
1. The area of the dead zone located in the thickness of the heart muscle is indicated by a change in the QRS complex . Usually this part increases or a pathologically high Q wave .
2. About the place around the formed necrosis, which is affected by the displacement of the ST segment .
3. About the ischemic zone, which is located even further from the point of injury. An electrocardiogram records a violation of the myocardial restoration processes in the form of changes in the T wave .
The concept of ST segment elevation: above without atrial repolarization, below with atrial repolarization without QRS
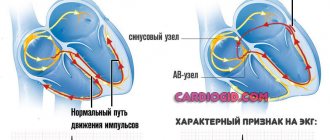
During an ECG, each lead is recorded on the film with a new line, which helps to accurately determine the location of the cardiac lesion. In total, the electrocardiogram consists of 12 graphic lines and 5 teeth - P, Q, R, S, T. Each tooth is distinguished by its width, height, depth and goes in its own direction.
projection of ECG leads
projection of ECG leads
The dynamics of the development of a heart attack on the ECG become visible in the first minutes after the development of the disease. On the film, changes are displayed depending on the shape of the infarction, its location and stage of progression. They can be barely noticeable (with small focal lesions) or have a clear “classical” form, known to all literate people.
Consequences
Unlike extensive forms of heart attack, small lesions do not often cause serious complications in the first year after the attack. The list of consequences of necrosis is as follows:
- Failures in the heartbeat are provoked by a violation of the conduction system.
- Heart failure is caused by a weakening of the strength and regularity of myocardial contractions.
- Post-infarction angina manifests itself as acute pain within 2 weeks after the attack and significantly increases the likelihood of a recurrent heart attack.
Over time, left ventricular failure and cardiosclerosis may develop. To avoid consequences, it is recommended to call an ambulance immediately when the first signs of a heart attack are detected and undergo a course of therapy in a hospital. At the clinic, a medical history is created for the patient, where diagnostic results, complaints and stages of treatment completed will be recorded. After discharge, the person will be given a conclusion and recommendations for a speedy recovery.
ECG picture depending on the stage of infarction
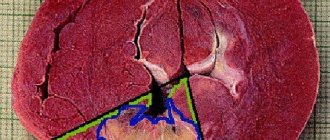
Zones of myocardial ischemia on the ECG
When the blood supply to any part of the heart muscle is cut off, muscle cells in that area die. At the edges of the myocardial ischemia zone, the cells of the conduction system do not die, but their performance is impaired. After the blood supply is restored, the functioning of the damaged tissues usually returns to normal. That is, this is the area that can be saved with early endovascular intervention. These functions are displayed depending on the stage and strength of MI development. They are divided into:
- acute;
- spicy;
- subacute;
- cicatricial
There are only two types of lesions: small-focal and large-focal infarction (a severe version of large-focal infarction is transmural infarction). Large-focal MI is called a “Q-forming infarction.”
Typical dynamics of the stages of infarction on the ECG
1. The most acute stage lasts 3 - 72 hours. During this time, the formation of necrosis and the Q wave may occur. Elevation of the ST segment outside the isoline is observed. The most acute stage can be recognized by the formation of a monophasic curve (cat's back).
ST segment elevation on ECG
2. The acute stage lasts 14-20 days. It is characterized by a clear localization of the ischemic zone and existing damage. In case of AMI, the ST segment comes close to the isoline and covers the T wave.
3. The subacute phase can last up to three months. The damaged area is replaced by connective tissue. The patient's condition is stabilized. When repeating the ECG, ST elevation to the isoline is recorded.
4. The scar stage is the stage of formation of a strong connective tissue scar. In other words, this is a scar that will not disappear for the rest of your life. When deciphering the ECG tape, the ST segment does not go beyond the isoline. During scarring, the amplitude of the T wave should not exceed 5 mm, and it is also important that its height does not reach the middle of Q and R in the same lead. An old scar of unknown date is recorded on the ECG tape in the form of a scar.
MI can be large-focal or small-focal. This takes into account how extensive the area of damage to the heart muscle is.
transmural Q infarction ECG - stages of development
How can you determine the location of a heart attack on an electrocardiogram?
After myocardial infarction, the location of necrosis can be found in different parts of the heart muscle. It can be located in the area:
• anterior septum;
• anterior wall of the left ventricle;
• back wall;
• from the side;
• lower part;
• combined arrangement.
The right ventricle is not subjected to heavy loads. Therefore, myocardial infarction in this part of the heart is less common. In this case, the description of the ECG result is different:
• an increase in the ST segment and the appearance of a Q wave;
• inhibition of the T wave;
• slight increase in ST wave in the thoracic area;
• In lead V2 there is a decrease in ST.
According to statistics, left ventricular infarction is more common. This is explained by the fact that the walls in this part of the heart are most thickened. The entire load falls on the left ventricle and requires more blood circulation.
ECG signs of anterior wall infarction
Electrocardiographic signs of LAD occlusion in anterior infarction: D1=first diagonal artery, S1=first septal artery, LAD=anterior interventricular/anterior descending artery, STD=ST depression, STE=ST elevation, RBBB=right bundle branch block.
ECG algorithm for identifying the localization of lesions in the LAD
With ST elevation in leads V1-V6 LAD=anterior interventricular artery, RBBB=right bundle branch block, D1=1st diagonal artery, S1=1st septal artery, STD=ST depression, STE-ST elevation, E = sum
Clinical example
The ECG shows ST segment elevation in leads V2, V3, I, aVL and ST depression in the inferior leads, suggesting occlusion of the anterior descending artery, which was confirmed by coronary angiography (Figure B).
Diagnosis of inferior wall infarction
How to determine the location of infarction with ST elevation in the inferior leads
If we detect ST elevation in the “lower” leads II, III, aVF, we look at lead V4R: if V4R is present, we suspect occlusion of the anterior interventricular artery and proceed to the algorithm for identifying it. If V4R is absent, we diagnose a lesion of the right coronary or circumflex artery: ST elevation in I - OA lesion, ST depression in I - RCA lesion, on the isoline - compare ST elevation in II and III, if II > III - OA lesion, vice versa - defeat of the RCA.
Also, by changes in ST in lead V4R, it is possible to differentiate between lesions of the OA, the proximal third of the RCA and the distal third of the RCA:
Clinical example
Infarction of the inferior wall: we see ST segment elevation in the inferior leads, with elevation in lead III > II. We also see depression in leads I and aVL. This picture suggests occlusion of the right coronary artery, which was revealed by selective coronary angiography (Figure B)
Infarction according to the “depth” of the lesion
• transmural;
• subendocardial;
• intramural.
For each form, the characteristic signs are determined by the state of the zones of necrosis and damage. With transmural MI, signs of macrofocal necrosis appear. The entire thickness of the walls from the endocardium to the pericardium is affected.
Subendocardial infarction also occurs very extensively and can be large-focal. But during the development of a heart attack, diagnosis is difficult due to the blurring of the boundaries of the affected area. Even with myocardial hypertrophy, activity in subendocardial fibers increases and with the development of MI the indicators do not decrease. The diagnosis of subendocardial infarction is confirmed if signs of the disease do not disappear within two days.
The intramural form of MI is less common in medical practice. To identify this type, the patient is observed for two weeks. It happens that the patient suffers an attack on his feet. This type of pathology refers to small focal necrosis. The diagnosis can be confirmed or refuted only after a thorough analysis of the signs of pathology development.
A heart attack can also be:
1. Circular, which is characterized by damage to the apex of the heart. Circular infarction develops in an arcuate shape and passes through the posterior wall to the anterior, lateral or lower parts. A left ventricular infarction occurs with irreversible consequences.
2. Septal, arising between the ventricular septum. In the process, the heart muscle completely dies due to lack of blood supply.
Topical diagnosis includes 5 types of localization of left ventricular infarction, which cannot be hidden. The table below explains them in more detail.
Types of localization Indicators Leads
Anteroseptal V1-4 II, III, AVF
Posterior diaphragmatic II, III, AVF I, AVF
Posterolateral I, AVL, V5 VI
Posterobasal with extension to the basal sections. missing V1, V5
Septal V1, V2, QS missing
In case of right ventricular infarction, changes can only be recorded in other leads V3R - V4R.
Key symptoms
The symptoms of transmural myocardial infarction vary depending on the period of development of the pathology. Let's look at those stages of necrosis formation at which, subject to timely medical intervention, it is possible to save not only the patient's life, but also the integrity of his heart muscle.
Prodromal period
The patient begins to worry about warning signs similar to unstable angina:
- increased frequency of pain attacks localized behind the sternum;
- development of pain in response to physical activity that previously did not cause it, or even at rest;
- When nitro drugs are used to relieve pain, the previous dose does not bring the usual relief; more and more drugs are required to achieve the desired effect.
All these manifestations indicate rapidly developing blockage of the coronary arteries. With a further decrease in the volume of blood passing through them, myocardial infarction is likely to develop. Therefore, the clinical protocol for acute coronary syndrome requires mandatory hospitalization of such patients.
The most acute period
If time is lost and sufficient help was not provided in the prodrome, then the most acute period begins - the beginning of necrotic changes in the heart muscle. The largest number of deaths from transmural infarction occurs precisely in the acute period. Although, on the other hand, therapy carried out at this time is most effective, up to complete recovery.
Symptoms are manifested by anginal status - very strong pressing, drilling or dagger-like pain in the chest area with irradiation characteristic of the heart. Its duration is more than half an hour, even taking 3 tablets of nitroglycerin does not bring relief. A number of other symptoms are added:
- anxiety;
- cold sweat;
- fear of dying;
- severe weakness;
- hypotension (more often) or hypertension (less often).
In addition to the standard anginal attack, transmural infarction can manifest itself with atypical syndromes:
- abdominal, with epigastric pain radiating to the back, nausea, belching, flatulence, vomiting, after which there is no relief, tension in the abdominal muscles;
- atypical anginal, with pain in the limbs, lower jaw, throat;
- asthmatic, with an attack of shortness of breath, the development of which is based on pulmonary edema or cardiac asthma;
- arrhythmic, with a predominance of arrhythmia symptoms over pain or without pain at all;
- cerebrovascular, with fainting, vomiting, nausea, dizziness; sometimes with focal cerebral manifestations.
Based on the symptoms, we can suspect a heart attack, but electrocardiography will certainly help determine it. We'll talk about it in the next section.
ECG - signs depending on the size of the lesion
A large-focal MI in a photocardiogram will show a pathological Q wave. For example, the occurrence of a Q-myocardial infarction in part of the anterior wall of the left ventricle usually occurs due to blockage of the anterior artery. Signs of the development of a heart attack on the ECG with this pathology look something like this:
• Q wave outside the R wave line;
• R is equal to Q;
• T—negative wave;
• upward push of the ST segment.
Large focal MI in patients with bundle branch block is very difficult to determine. To avoid making a mistake in making a diagnosis, scientists have identified several signs that may indicate the development of a heart attack.
The interpretation of the electrocardiogram reflects:
• manifestation on the film of the cardiogram of the Q wave in 2 or more leads (VL, I, v5, v6);
• identification of Cabrera's sign in leads v3-v5;
• ST shift to two adjacent leads;
• decrease of the R wave from v1 to v4.
Identification of even one indicator from the above list increases the risk of developing MI by 90%.
Small focal MI is characterized by a weak clinical picture. The condition occurs against the background of cardiac ischemia with minor muscle necrosis. A heart attack suffered on the legs, the time of ECG diagnostics, reflects changes in the ST segment and T wave.
It could be:
• absence of any QRS changes;
• decrease in the R wave depending on previous results;
• location of the ST segment below the isoline;
• the appearance of a patholic T wave.
Thus, infarctions are divided into Q-infarctions (large-focal) and non-Q-infarctions (small-focal).
Additional studies for heart attack
The interpretation of the cardiogram may sometimes not correspond to the ongoing clinical picture. It can be difficult to recognize a possible MI, and changes on the ECG tape may be caused by other diseases. Example: An ECG pattern simulating a large-focal infarction occurs with pulmonary embolism. The disease threatens human life and changes in the electrocardiogram should be taken extremely seriously.
Laboratory diagnosis of heart attack
To make a correct diagnosis, doctors conduct additional research methods. During the development of necrosis, different types of proteins are found in the blood. Laboratory diagnostics in this case involves taking a general blood test. Its results determine the presence of inflammatory processes. Biochemistry (biological markers) is presented as:
1. Counting the number of myoglobin.
2. Creatine phosphokinase (CPK) measurements.
3. Determination of lactate dehydrogenase activity.
4. Testing for troponin T.
For many years, medicine has used blood tests for ALT, AST, and LDH to diagnose MI. Now doctors complement the diagnosis with a study of the gas and electrolyte composition of the blood and general clinical studies. Only the results of laboratory and instrumental research methods confirm the development of myocardial infarction.
Causes
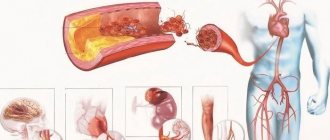
Blockage of the circumflex branch of the left coronary artery or the right posterior descending artery directly leads to disruption of blood flow in the myocardium. The reasons for this condition may be:
- thrombus, arteriosclerotic plaque, fat embolus;
- ligation or dissection of arteries during cardiac surgery;
- spasm of coronary vessels.
Risk factors include: diabetes, hypertension, smoking, rheumatism, obesity, alcoholism.
In such patients, as a rule, fat metabolism is impaired, hypercholestrinemia and increased coagulability are observed in the blood. Most often, heart attacks occur in men over 40 years of age with a sedentary lifestyle and high stress load.
We recommend reading the article about complications of myocardial infarction. From it you will learn about the stages of the disease and the classification of complications, early and late complications, treatment methods and preventive measures.
And here is more information about myocardial infarction in diabetes mellitus.