Possible causes and risk factors
The pathogenesis of thrombophlebitis, a disease that manifests itself when there is a disruption in the process of hematopoiesis and leads to the appearance of thrombotic masses, has now been fully studied, but the factors that provoke the formation of anomalies have not been fully studied.
Doctors list the main causes of blood clots as:
- Vascular pathologies (mainly varicose veins), accompanied by a slowdown in the outflow of biological fluid.
- Surgical interventions.
- Long-term immobilization (for fractures, severe injuries of the musculoskeletal system, paralysis); bed rest prescribed to patients for a long time (for damage to the central nervous system, disorders of the cardiovascular system).
- Oncological diseases. Diseases change the composition of the blood; the emerging tumors deform and compress the veins.
- Allergic reactions, infectious processes that damage the inner surface of the vascular walls.
- Genetic or acquired predisposition to increased venous thrombus formation.
At risk are people over 40 years of age who suffer from physical inactivity, obesity and bad habits.
The appearance of a thrombotic mass under the knee in women is caused by special conditions of the body, accompanied by changes in hormonal levels - pregnancy, menopause, menopause. The disease is also diagnosed in women who have taken oral contraceptives.
The stronger sex is susceptible to the disease at the age of fifty: at this time, most men experience a decrease in testosterone levels.
Doctors include patients who make long journeys or flights into a special category. According to experts, regularly sitting in an uncomfortable position also leads to thrombosis.
Among the indirect factors contributing to the onset of the disease are wearing tight clothing, overeating, hypothermia, and dehydration.
According to statistics, the likelihood of a blood clot forming under the knee reaches 20%. This frequency of the appearance of blood formations in the area under consideration is associated with the hemodynamic conditions of the venous bed - low pressure and slow blood flow.
Thrombosis of the iliofemoral segment
Isolated thrombosis of the common femoral, external and common iliac veins is rarely observed, since they represent a single line, the main route of venous outflow from the lower limb. Therefore, it is advisable to consider the clinical picture of thrombosis of these veins as iliofemoral (iliofemoral) thrombosis.
Thrombosis of these vein segments has common pathogenetic factors, a similar clinical picture and a common treatment strategy.
Thrombosis of this localization can be of an ascending nature (from the deep veins of the leg) and a central path of development (from the pelvic veins). The central path of development is most often observed (in 74% of cases, according to BC Savelyev et al., 1972). In 22.6% of patients, the same authors noted ascending thrombosis from the deep veins of the leg, and in 3.4% of patients, the cause of iliofemoral thrombosis was ascending thrombosis of the great saphenous vein.
According to most authors, acute iliofemoral thrombosis is 2-3 times more common in women, and this statistics relates mainly to the central pathways of thrombosis development. With peripheral routes, the incidence of men and women is approximately the same. The age composition of patients is very different, but it is generally accepted that venous thrombosis occurs extremely rarely in children. With peripheral paths of development, the frequency of left-sided and right-sided thrombosis is approximately the same; with a central origin, left-sided lesions are observed 4.5 times more often than right-sided ones.
Since in ascending thrombosis the block of the iliac veins is preceded by thrombosis of the common femoral vein, we should first dwell on the clinical picture of thrombosis of the common femoral vein, which always has clear clinical symptoms. It is characterized primarily by sudden swelling of the entire limb, as the outlet of the deep vein of the thigh is blocked and most of the main collaterals are turned off. The moment of the appearance of edema of the entire limb in some cases is regarded by the doctor and the patient as the onset of the disease.
When examining the limb, there is cyanosis of the skin, the intensity of which increases towards the periphery.
After a few days, venous stasis may decrease due to the fact that collateral outflow pathways are activated.
In the upper third of the thigh, in the groin area and in the pubic area, an increase in the pattern of saphenous veins is observed. This symptom is important for determining the upper limit of thrombosis. The pain syndrome is more pronounced with primary thrombosis of the common femoral vein, when the disease begins with acute pain in the groin area, then swelling and cyanosis of the limb appear. Palpation reveals sharp pain in the upper third of the thigh and enlarged inguinal lymph nodes.
If thrombosis of the common femoral vein is caused by the spread of the thrombotic process from the mouth of the great saphenous vein, then the clinical picture consists of symptoms of thrombosis of the great saphenous vein and occlusion of the common femoral vein, if it occurs. If the thrombus does not completely obstruct the femoral vein, it can float freely in the lumen of the vein and be dangerous in terms of thromboembolic complications.
With central paths of development of iliofemoral venous thrombosis, thrombosis of the main veins of the pelvis may initially have a hidden course. This is due to the degree of hemodynamic impairment. If a small-diameter thrombus, when spreading from the internal iliac vein, has a parietal character, then no pronounced changes in hemodynamics are observed.
The only manifestation of such thrombosis may be a sudden pulmonary embolism. Widespread thrombosis of the iliofemoral segment leads to a sharp disruption of venous outflow with a corresponding clinical picture. BC Savelyev et al. (1972 and 2001) during the thrombotic process of this localization, two stages are distinguished: the compensation stage, or prodromal stage, and the decompensation stage, or the stage of pronounced clinical manifestations.
The main symptoms of the prodromal stage of the acute iliofemoral segment: increased temperature and pain of various localizations. In some cases, an increase in temperature is the only symptom of latent thrombosis, and antibiotics in most cases do not reduce the temperature. It should be emphasized that an unexplained increase in temperature in a certain category of patients should alert the doctor in this regard. Most authors believe that the increase in temperature is not caused by a microbial factor, but by a hyperergic reaction to damage to the endothelium and absorption of breakdown products of protein substances.
Pain syndrome has its own characteristics. Pain usually appears in the lumbosacral region, in the lower abdomen and in the limb on the affected side; it often begins gradually and is dull, aching in nature. Pain of such localization in the absence of other signs of venous thrombosis often causes diagnostic errors. Pain in the lumbosacral region and in the lower abdomen is caused by several factors: stretching of the walls of thrombosed pelvic veins, hypertension in the main veins of the pelvis and their tributaries, periphlebitis with the involvement of many nerve endings in the inflammatory process. Pain in the lower extremity is caused by venous hypertension below the site of occlusion. The prodromal stage lasts from 1 to 28 days, with an average of 5-7 days.
The stage of pronounced clinical manifestations is characterized by severe pain, swelling and discoloration of the limb.
Pain in the lower extremity is caused by both thrombosis itself and venous hypertension distal to the site of occlusion and can be localized or diffuse. The most pathognomonic symptom of acute iliofemoral thrombosis is swelling of the entire limb, which develops very quickly.
With peripheral pathways of thrombosis development, edema is of an “ascending” nature; with central pathways, edema of the entire limb occurs immediately or is of a “descending” nature, i.e. First, the thigh increases in volume, then the lower leg. Studies have shown that the origin of limb edema in acute iliofemoral thrombosis is due to venous stasis and impaired lymphatic drainage due to damage to the lymphatic collectors. The role of damage to the lymphatic system in the pathogenesis of acute thrombosis of the great veins is unconditional and was discussed above.
Depending on the location and extent of the block of lymphatic collectors, either regional lymphostasis or widespread swelling of the limb, external genitalia, buttocks and anterior abdominal wall on the affected side occurs. These features of damage to the lymphatic system can explain the isolated swelling of the thigh, which sometimes lasts for a long time, and the “descending” nature of the swelling of the limb.
Swelling of the limb can also be observed in other diseases with which iliofemoral venous thrombosis has to be differentiated.
Acute lymphostasis, which can cause misdiagnosis, is usually secondary and develops as a result of previous erysipelas, inguinal lymphadenitis or damage to the inguinal nodes by a tumor process. Acute lymphostasis or lymphedema of the limb, caused by impaired lymph circulation for one reason or another, has its own distinctive features. They are not accompanied by pain, changes in skin color and increased venous pattern, and the swelling is dense.
Edema of the lower extremities in heart failure, as a rule, develops gradually, is bilateral in nature, begins in the distal parts of the extremity, and is not accompanied by pain and increased venous pattern.
Traumatic edema is sometimes classified as acute venous thrombosis. A carefully collected anamnesis will help cast doubt on this diagnosis. A differential diagnosis between iliofemoral thrombosis and a femoral neck fracture will be made possible by symptoms such as shortening of the limb, external rotation of the foot, pain with axial load and load on the greater trochanter, and the symptom of a “stuck heel.” X-ray examination is decisive in making a diagnosis. In addition to the history, intense local swelling of the leg, sharp pain on palpation, and a hematoma in the ankle area, which appears after 2-4 days, help to suspect a spontaneous intermuscular hematoma.
Additional information in differential diagnosis is provided by ultrasound and venographic studies.
Discoloration of the skin of the limb is one of the main symptoms of acute iliofemoral thrombosis. Skin color can vary from pale to pronounced cyanosis. Diffuse cyanosis is explained by dilation of venules and capillaries, as well as increased oxygen utilization due to slower blood flow in the limb. Pale skin color is due to impaired lymphatic drainage. With arteriospasm, which can accompany acute thrombosis, a “marbled” coloration is observed mainly in the distal parts of the limb.
An increased pattern of saphenous veins on the thigh and especially in the groin area is an important symptom of venous iliofemoral thrombosis, but it appears after the swelling of the limb has decreased. It should be remembered that even in healthy people the venous pattern can be pronounced. Therefore, it must be considered in comparison with a healthy limb.
Other symptoms include psoitis observed in some cases, an increase in skin temperature on the affected limb and a general temperature reaction. The general condition of the patient, as a rule, suffers little, and the deterioration of the condition is caused either by the disease against which the thrombosis developed, or by complications of thrombosis.
The stage of pronounced clinical manifestations lasts from one to several months. L.I. Klioner (1969) and BC Savelyev et al. (1972) distinguish three clinical forms depending on the severity of clinical symptoms and the degree of hemodynamic disturbances: mild, moderate and severe forms. We agree with this classification and are of the same opinion in this regard.
The mild form is characterized by mild clinical manifestations due to well-compensated collateral circulation. The phenomena of decompensation of venous circulation develop gradually, swelling reaches a maximum on the second or third day from the beginning of the stage of pronounced clinical manifestations. Venous pressure, measured in the distal parts of the limb, rises no higher than 250-300 mm of water. Art.
In the moderate form, the compensatory capabilities of collateral circulation are much less pronounced, since thrombosis develops very quickly, leaving no time for the formation of venous collaterals. Clinical symptoms manifest themselves, accordingly, more strongly. Significant edema develops quickly and reaches a maximum during the first day from the beginning of the stage of pronounced clinical manifestations. Venous pressure in this form reaches 600-700 mmH2O. Art.
The severe form is caused by total thrombosis of the main veins of the lower limb and pelvis on the affected side.
Along with a sharp disturbance of venous circulation, disorders of arterial blood flow are observed. Patients complain of constant throbbing pain in the limb and buttock, and a sharp feeling of fullness. Movement in the limb is impossible. Skin hyperesthesia is noted on the thigh and lower leg, and sensitivity on the foot is reduced. The foot is cold to the touch. The swelling increases sharply within several hours and does not decrease with an elevated position of the limb. Skin cyanosis is pronounced. The appearance of purple-cyanotic spots with the formation of blisters indicates incipient venous gangrene. Venous pressure in severe forms exceeds 1000 mmH2O. Art.
A severe form of acute venous thrombosis is called “phlegmasia blue” (phlegmasia coerulea dolens). The term was proposed in 1938 by R. Gregoire. The frequency of “blue phlegmasia” in relation to venous thrombosis of the lower extremities and pelvis, according to different authors, varies: from 1.7 (Y. Cranley, 1962) and 8.2% (I.I. Sukharev, 1977). ) up to 22% (S. Hafner et al., 1965). According to literary data (T. Dyula et al. 1969; T. Ghitescu, 1976), the mortality rate for “blue phlegmasia” is 20-26%, and in the case of gangrene of the limb - 40-45%. Moreover, in 6.8% of patients the cause of death is pulmonary embolism; the second most common cause of death is acute renal failure.
It is also necessary to remember about the so-called pseudoembolic form of venous thrombosis.
A feature of this form is pronounced arterial spasm, and therefore the disease occurs as an embolism or thrombosis of the iliac or femoral artery. Erroneous diagnosis is possible in 17.5% of cases (BC Savelyev et al., 1972). Unlike venous thrombosis, arterial thromboembolism is characterized by a sudden onset. The pain is localized mainly in the distal parts of the limb, where anesthesia of the skin and lack of movement in the toes and ankle joint are also noted.
Edema develops late and is limited to the lower leg area. The saphenous veins are poorly filled and collapse when the limb is raised. The skin color is pale or patchy cyanosis is noted.
Symptoms
The main danger of thrombosis is that it occurs in the absence of obvious signs. The popliteal vein affected by pathology may not cause any discomfort to the patient for several years; the main symptoms of the disease appear mainly during a period of critical narrowing of the lumen of the vessel or its complete blockage.
The progression of the anomaly is accompanied by:
- acute pain localized in the popliteal fossa (the depression located behind the knee joint) when bending;
- significant discomfort in the calf muscles after physical activity;
- local increase in skin temperature.
Describing their condition, patients complain of the rapid onset of fatigue and a feeling of heaviness in the lower extremities. When you take a horizontal position and place your legs on an elevation, the unpleasant sensations subside. In some cases, patients note a general deterioration in their condition and signs of intoxication.
Complications and prognosis
In the absence of adequate treatment, blood clot rupture cannot be ruled out. An embolus can enter the pulmonary artery cavity and cause blockage. This condition is life-threatening. A small embolus may not cause significant symptoms, while large clots impair the perfusion of lung tissue, lead to the development of hypoxia, death of a section of the lung and subsequent inflammation.
When the outflow of blood from the lower limb is completely blocked, white or blue phlegmasia develops - conditions that can lead to the development of gangrene and heart failure.
Diagnostic methods
Only a specialist - a phlebologist, a vascular surgeon - can detect the presence of the disease. Diagnosis of vein thrombosis under the knee is carried out in 3 stages.
The primary includes interviewing and examining the patient.
On the second, the doctor uses functional tests. Their list and implementation scheme is in the table below.
| Test | Progress of procedures |
| Moses | Compression of the muscles of the lower extremities, first from the sides, then in the forward-backward direction. The presence of the disease is indicated by severe discomfort during the last of the listed manipulations. |
| Homans | Consecutive bending of the knees and feet of the patient lying on his back. The occurrence of pain in the calves indicates the development of the acute stage of the disease. |
| Ramirez | The test is carried out using a tonometer, the cuff of which is placed on the lower leg in the middle part. Unpleasant sensations that appear when pressure is increased to 150 mm Hg. - a sign of thrombosis. |
| Lowenberg | The implementation scheme is similar, the area of fixation of the product is the thigh. A test in which pain is noted by the patient during an increase in air pressure from 50 mm Hg is positive. |
The third stage of diagnosis is instrumental research. Help to clarify the diagnosis:
- Ultrasound ultrasound of veins The method allows you to detect the location of the blood clot, the size of the clot and the degree of its mobility.
- Phlebography. Makes it possible to assess the general condition of the veins.
- Classic ultrasound used to determine the density of the formation.
Whether an emergency instrumental examination can be prescribed is positive: suspicion of 50% or complete blockage of the vessel is an indication for the immediate use of the technique.
Treatment of deep vein thrombosis n/c
The ultrasound physician often has to decide the question: “In what cases is emergency hospitalization indicated?”
In thrombophlebitis, a fresh clot (from 0 to 7 days) up to 3 cm from the SPS is considered embolic.
With DVT, there is a dangerous fresh thrombus in the ileofemoral and femoropopliteal segment.
Anticoagulant therapy is the basis of treatment for patients with DVT from the popliteal-femoral segment.
They start with the intramuscular administration of heparins, followed by the addition of vitamin K antagonists (Warfarin).
5 days before stopping heparin, begin titrating the dose of Warfarin to the target INR value of 2-3.
The duration of taking anticoagulants is determined taking into account aggravating circumstances.
| Deep vein thrombosis | Anticoagulants | Duration of admission |
| Postoperative | AVK | 3 months |
| Idiopathic | AVK | 6-12 months |
| Oncology | heparins | 3-6 months |
| Thrombophilia | AVK | at least 12 months |
| Recurrent DVT | AVK | for life |
Removing a blood clot from a deep vein is more effective than treatment with anticoagulants alone.
A floating thrombus in the iliofemoral segment is an absolute indication for thrombectomy.
In case of vein occlusion, the issue of thrombectomy is decided personally; it is effective only in the first 5 days.
During thrombectomy, it is advisable to preserve the PBB, because in 40% of cases, headache does not have a direct connection with PCV.
The severity of PTB depends on the preservation of the valve apparatus of the femoral-popliteal segment.
When the patient's condition does not allow thrombectomy, a vena cava filter is placed in the inferior vena cava.
A quarter of patients with a vena cava filter will experience thrombosis of the inferior vena cava within the next 3 years.
Young patients are given removable models and removed after 30 days when the threat of pulmonary embolism is eliminated.
Treatment options
Treatment regimens vary depending on the type of blood clot.
Experts distinguish 3 types of clots. Among them:
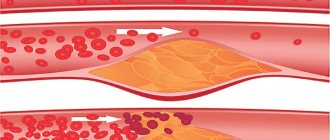
- parietal (not blocking the lumen), located close to the tissues of elastic tubular formations;
- occlusive - more dangerous, capable of causing a cessation of blood flow;
- floating, one end of which is attached to the wall of the vein, the second is free to move.
If a thrombotic mass belonging to category 1 or 2 is detected in a vessel, conservative therapy is prescribed; the third is surgery.
Drug therapy
Treatment of thrombosis is carried out in a hospital, with the patient observing bed rest for 3 to 10 days. Several groups of medications are used to relieve the disease. In the list of prescribed medications:
- Antiplatelet agents, anticoagulants - Curantil, Warfarin, Heparin. The drugs prevent the formation of blood clots and the progression of pathological processes.
- NSAIDs are medical products that reduce discomfort and swelling (Ibuprofen, Diclofenac).
- Angioprotectors used to improve venous microcirculation - Troxevasin, Rutin.
- Antibiotics of the penicillin, fluoroquinol and cephalosporin groups. Prescribed when purulent complications are detected.
It is prohibited to use the above remedies without a doctor’s recommendation.
Local therapy
Treatment methods for a disease identified at an early stage involve applying liniments and gels to the skin of the affected area. Among the most effective drugs are Indovazin, Lyoton, Heparin ointment. Medicines relieve swelling and reduce discomfort.
Traditional methods of treating varicose veins of the legs
Varicose veins in the legs can be treated in the initial stages using traditional methods. The maximum effect will be achieved if you combine traditional methods with the use of venotonic drugs. The most effective components and ingredients in the treatment of varicose veins are:
- Potato. The tubers can be grated raw and applied to sore legs under the knee. The mixture is fixed with a bandage overnight. The course of treatment is until there is a clear improvement in well-being. Instead of potato mass, you can simply use potato juice. It is squeezed out of grated potatoes, bandages are soaked in the juice and wrapped around sore legs. Cover the top of the compress with cling film.
- Lilac (leaves). The plant can be plucked and applied to the area of diseased vessels, securing with a bandage. You can make such compresses every day while the bush is in the spring-summer growth stage.
- Bodyaga. Here, 2 tablespoons of the plant are poured into 0.5 liters of boiling water. Leave the mixture for 2 hours, after which you can soak bandages in the liquid and make medicinal compresses.
- Garlic. A healing ointment is prepared from it. Garlic cloves are crushed into a paste and mixed with butter in a ratio of 1:2. The prepared ointment is applied to the inflamed areas of the legs and secured with a bandage. Cover the top with cling film. The compress should ideally be wrapped in a scarf and left overnight, but you can also apply such a bandage for 3-4 hours. Wash off the ointment with warm water.
- Chestnut. To prepare the product, take 10 grams of crushed chestnut fruit and pour in 100 grams of vodka. The infusion is stored in a dark place for 7 days, shaking occasionally. The finished product is filtered and drunk three times a day before meals, 15–25 drops, washed down with water.
- Green tomato. An application of sliced berries is applied to the diseased veins. Secure the tomato slices with a bandage for the whole day. You can be treated in this way for up to six months or more.
- Apple cider vinegar. It can be rubbed into the skin in the area of inflamed veins on the legs, either pure or diluted. To dilute, mix 0.5 cups of water and 2 tablespoons of vinegar. You can also drink apple cider vinegar by mixing 1 glass of water, 2 tbsp. l. vinegar and 1 tsp. honey. Drink the drug in the morning on an empty stomach. The course of treatment is unlimited.
Important:
It is advisable to use homemade vinegar. Patients with high acidity of gastric juice are prohibited from taking vinegar orally.
- Swamp dry grass. Used to prepare foot baths. 150 grams of dry plant are poured with 10 liters of boiling water and left for an hour. Leave your feet in the prepared broth for up to 20 minutes.
Prevention methods
To prevent the onset of the disease, it is recommended to lead a healthy lifestyle, regularly take walks, alternate work with short rest breaks, visit a massage therapist, and follow a daily routine.
Particular attention should be paid to proper nutrition - the diet should contain a large amount of berries, ginger, vegetables, and fruits. The consumption of fatty and sweet foods and strong coffee should be minimized.
You can avoid disability and the worst-case scenario by undergoing timely preventive medical examinations and visiting a doctor at the slightest problem with the veins. Timely detection of the disease and adequate therapy is the key to maintaining health.
Healing procedures
The disease is treated in a hospital. Depending on how seriously the leg tissue is damaged, conservative therapy or surgery is performed.
Conservative treatment
An important role in the successful treatment of thrombosis of the arteries of the lower extremities with conservative methods is played by the early use of drugs that have a thrombolytic effect. In addition to thrombolytics, anticoagulants and antispastic agents are used. If necessary, thrombolysis therapy is performed.
Thrombolysis is a procedure that dissolves blood clots inside the arteries. To carry it out, special medications are used, which are administered to the patient intravenously by drip.
Reasons for appearance
Thrombosis of the popliteal artery occurs due to a wide range of social and other factors.
- Reaching 40 years of age. The main risk group for the disease is 40-50 year old women, and the risk of blood clots increases over time. Surgical intervention. During surgical manipulations, a protective reaction of the body occurs in the form of increased blood clotting and increased relaxation of muscle tissue. The result of these phenomena is blood stagnation and vein blockage.
- Traumatic injuries to limbs, fractures. Under such circumstances, the body reacts in the same way as during surgery - the rate of blood clotting increases, the muscles relax, hemostasis and popliteal vein embolism are formed. Statistics confirm that more than half of patients who suffer fractures experience thrombosis.
- Varicose veins of the lower extremities.
- Aneurysm (protrusion) of the artery wall.
- Long adynamia, the patient is forced to lie down.
- Cancerous tumors, especially after surgery.
- Hormone therapy, taking contraceptives.
- Pregnancy period, childbirth.
- Inflammation of soft tissues.
- Frequent and long flights.
- Abuse of alcohol, tobacco and products that increase blood viscosity.
Local therapy
Popliteal vein thrombosis involves local treatment. Consists of the following provisions:
- Maintain strict bed rest.
- The use of compresses based on 50% alcohol solutions.
- Fixing the affected leg with elastic bandages.
- Treatment of the affected area with special ointments, gels - Lyoton, Gepatrombit, Indovazin, gel containing Diclofenac, treatment with ointments Rutozidone, Troxevasin.
- Taking anti-inflammatory, thrombolytic drugs, anticoagulants.
- Taking antibiotics if there is an infection.
Symptoms and treatment of a blood clot in the leg behind the knee
Thrombosis of the popliteal vein with varicose veins is very rare. This is due to the anatomical position of the vessel; it is located in the popliteal fossa. Thrombosis is a process where there is a blockage of the lumen of a vein; many risk factors contribute to the initiation of this process.
Popliteal vein thrombosis is a rather difficult diagnosis to diagnose. This is due to the great rarity of occurrence of this type of complication of varicose veins. Therefore, for many doctors, establishing such a diagnosis is quite problematic. The symptoms of the pathology are similar to a large number of diseases of the musculoskeletal system. For example, osteochondrosis and ankylosing spondylitis have similar symptoms. Both of these conditions can impinge on the sciatic nerve, which runs down to the foot. With such disorders, the lower limb begins to hurt in the same places as with thrombosis, which leads to an erroneous diagnosis. Because of this, vein thrombosis is often diagnosed quite late, which can be fatal for the patient.
There are many reasons that cause thrombophlebitis of the popliteal vein. Most often occurs with varicose veins of the lower extremities. Virchow's triad most accurately describes the principle of the formation of blood clots. It consists of a combination of the following features:
- Violation of the integrity of the structures of the venous wall.
- Turbulent circulation.
- Violation of the qualitative and quantitative composition of blood elements.
Varicose veins provoke the occurrence of all three disorders. Dilated veins lead to turbulent blood flow and damage to the vascular wall.
The risk of developing pathology increases significantly in older people, and women are much more likely to suffer from the disorder. This is due to hormonal imbalances during pregnancy and the menopausal period. It is believed that the older a person is, the higher the risk of developing blood clots.
The cause of thrombosis may be surgical interventions that violate the integrity of tissues. As a result of surgical incisions, normal blood circulation is disrupted. Anesthesia promotes muscle relaxation and the release of thromboplastin, which accelerates the process of blood clots. This is complemented by prolonged bed rest, which is accompanied by the occurrence of chronic venous stagnation of blood.
Latest information: Phleboliths in the pelvis, what is it?
Bone fractures lead to long-term casting of the lower limb or installation of a skeletal traction system. As a result of these manipulations, prolonged stagnation of venous blood occurs, which increases the chance of clot formation.
Frequent injuries and compression of blood vessels lead to the development of such signs of Virchow's triad as a violation of the integrity of the vascular wall and the appearance of turbulent blood circulation. The effect of injury is enhanced by wearing clothes that have too tight elements, such as elastic bands, belts and other similar elements.
What's in this article: