A disease accompanied by blockage of the branches of the pulmonary arteries. Pulmonary infarction is a serious respiratory disease. Blockage of the pulmonary branches is associated with the formation of a blood clot. More often this disease is the cause of cardiac pathology.
Cardiac pathology includes various lesions of the heart muscles. Mainly arrhythmia, myocardial infarction and diffuse lesions of the heart muscle. What exactly are the disorders that occur in the heart muscle?
The disorders are associated with heart failure. And also against the background of increased blood clotting. In this case, blood clots form in the right heart. These formations are carried by the blood flow into the pulmonary vessels.
Embolism occurs when the veins of the systemic circulation are damaged. Provoking factors are gynecological operations. Also, the risk of embolism is associated with surgical interventions on the abdominal organs.
Various injuries can cause disruption of blood flow. Fractures of tubular bones especially occur. With this pathological condition, a fat embolism can form.
A pulmonary infarction may be accompanied by the development of various complications. Including pneumonia. Which is also a consequence of pulmonary infarction. An inflammatory process occurs in the lungs.
Also, this disease can provoke the development of pleurisy. Pleurisy can be hemorrhagic. Which is also the most serious complication.
During infectious processes, extensive suppuration occurs in the blood clot. In this case, the suppurative process breaks into the pleura. This situation contributes to the development of purulent pleurisy. Which is also the most dangerous to human health.
The size of the infarction matters in the development of the disease. At the same time, large heart attacks lead to even more serious complications. Up to and including death.
These complications carry many consequences. The recovery process is most delayed. Especially if the symptoms are most severe.
Find out more on the website: bolit.info
Consult a specialist!
Symptoms
With a pulmonary infarction, symptoms develop suddenly. In this case, pain develops. Moreover, the larger the heart attack, the stronger the pain. The initial symptoms of the disease are:
- sharp chest pain;
- dyspnea;
- cyanosis;
- hemoptysis;
- cough;
All these manifestations of the disease can provoke the development of collapse. If help is not provided on time. Therefore, it is urgent to provide assistance to the patient. This reduces the risk of fatalities.
At the site of the heart attack, dullness of sound and weakening of breathing are observed. Since the formation of blood clots interferes with the normal functioning of the respiratory system. Collapse is the most life-threatening condition.
A pulmonary infarction is characterized by a rise in temperature. This is due to an inflammatory response. The inflammatory response is often a consequence of pathological disorders.
The disease develops on the second day after blockage of the branches of the pulmonary artery. Painful sensations are sudden. At the same time, they resemble the pain of angina pectoris. It intensifies with coughing and bending of the body.
If the diaphragm is affected, namely the pleura in the diaphragmatic region, then a symptom of an acute abdomen develops. This sign is also appropriate for pulmonary infarction.
In some cases, hemoptysis is possible. The discharge of sputum is streaked. There is a manifestation of “rusty” sputum.
The highest body temperature occurs with infarction pneumonia. In this case, tachycardia and arrhythmia occur. Which is also a significant sign of the disease.
go to top
2 Consequences of the disease
According to many years of research by practicing doctors, pulmonary infarction is somewhat more common in men. The ratio among men and women is 12 to 10. The average age of patients exceeded 50 years. In 44% of the disease, single or multiple lesions are detected.
Lung abscess
What consequences a pulmonary infarction will entail, and how dangerous it is, depends on how much lung tissue is involved in the process. Small infarcts may have minimal consequences. They are often difficult to diagnose and have no symptoms. But large areas of necrosis often become a place for bacteria to accumulate. As a result, a lung abscess can form - a purulent focus with a cavity.
The most unfavorable option is for more aggressive microorganisms to enter the heart attack area. Then gangrene of the lung tissue develops, which is characterized by widespread putrefactive lesions. In this case, the prognosis is extremely unfavorable, because the mortality rate with gangrene of the lung has a very high percentage.
Increased body temperature
In most cases, there are no symptoms with this disease. A pulmonary infarction may be masked by symptoms of another pathology that is present in the body. The manifestations that are present in the body are non-specific for a heart attack. Patients may be concerned about the following complaints:
- Increased body temperature. It may be low if the pulmonary infarction is not complicated by infection. If an abscess or gangrene has formed, the numbers on the thermometer can reach 40 degrees.
- Sweating and chills. These symptoms often accompany infectious complications.
- Chest pain. This symptom is due to the involvement of the pleura covering the lung tissue in the process. It has a large number of nerve endings, so when inhaling or turning the body, the patient may feel sharp and severe pain.
- Cough.
- Dyspnea.
- Hemoptysis.
- General weakness and malaise.
Diagnosing a pulmonary infarction based on complaints is the wrong tactic, since many other ailments have exactly the same manifestations.
Diagnostics
In the diagnosis of pulmonary infarction, anamnesis is collected. Anamnesis consists of collecting the necessary information. Namely, possible causes and concomitant diseases.
A physical examination is also very important. In this case, the presence of weakened breathing, wheezing, and noises is assumed. There is also palpation of the abdomen. On palpation, the liver is enlarged and painful.
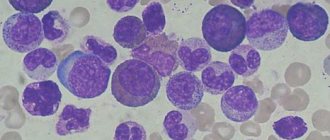
Laboratory diagnostics are used. Mainly a general blood test. As well as a biochemical blood test. The blood picture shows moderate leukocytosis and the presence of total bilirubin.
In diagnosing the disease, consultation with a pulmonologist and cardiologist takes place. Since the disorders affect not only the lungs, but also the cardiovascular system. Therefore, a comprehensive diagnosis is necessary.
Upon consultation with a cardiologist, certain abnormalities are discovered in the cardiovascular system. These violations are characterized as follows:
- systolic murmur;
- fine wheezing
An ECG is also performed. This reveals signs of heart overload. Right bundle branch block may be observed. ECHO provides more informative information.
ECHO studies reveal pathological conditions of the right ventricle. A blood clot may also be detected in the right side of the heart. Which is also a significant indicator.
Ultrasound diagnostics of the lower extremities is very relevant. This makes it possible to identify various disorders of venous outflow. Including the presence of deep vein blood clots.
Lung radiography is also used in diagnosis. This makes it possible to determine pathological conditions in this organ. Namely, expansion of the root of the lung.
go to top
Pathogenesis
It is based on two processes. The first and most common is thrombosis. That is, blockage of the pulmonary artery with a blood clot. Most often it forms far from the localization of the lesion. Limbs as the main place of development. Slightly less heart. For example, after suffering injuries or other conditions.
The second option is atherosclerosis. It itself is divided into two more types. The formation of cholesterol plaques on the walls of the vessel, deposits of fatty compounds that radially envelop the endothelium, create a mechanical obstacle and prevent blood from moving at a normal pace.
Narrowing or stenosis is also a type of atherosclerosis. Accompanied by spontaneous spasm and a change in the diameter of the lumen of the vessel. Other causes, such as inflammation (arteritis) with scarring and fusion of the wall, are less common. Be that as it may, in any case, a pronounced increase in pressure develops at the local level. Because blood has to overcome more resistance. The risk remains during each cycle of heart contraction, that is, continuously, as long as the pathological condition is present.
The deviation involves one vessel or several at once. The further stage of development is accompanied by rupture of the artery. This is usually not a spontaneous or random phenomenon. It is caused by stretching and thinning of tissues. Blood pours abundantly into the intercellular space, possibly entering the chest, which will inevitably provoke inflammation.
If the patient does not die from massive leakage of liquid tissue, many complications arise. The reason is compression of the respiratory structures, blood entering the alveoli (hemorrhagic consolidation of the pulmonary parenchyma), into the chest and other damaging factors. At each stage of therapy, you need to carefully monitor the condition of the victim so as not to miss an important moment and stop the impending threat in time.
Pulmonary infarction does not develop overnight, except in acute cases. Pathology is formed secondarily, as a response to the current disease. Usually we are talking about hypertension, abnormalities in the heart (CHD, other variants), atherosclerosis, cholesterolemia. Symptoms are present in most cases, but they are subtle, weak, and do not motivate the person to go to the hospital.
Prevention
In the prevention of pulmonary infarction, timely treatment of concomitant diseases takes place. Including diseases accompanied by the formation of thrombophlebitis. It is known that thrombophlebitis occurs in a number of cases.
The most common reasons for the formation of thrombophlebitis include lack of necessary physical activity. Long sedentary work. Therapeutic exercises may also be needed.
Some therapeutic measures, such as gymnastics, can prevent the development of thrombophlebitis and its consequences. Therefore, therapeutic exercises are a significant preventive measure.
The disease can develop after surgery. Therefore, it is very important to follow certain rules to prevent surgical complications. Early rise is recommended. Moderate physical activity (as indicated).
In the prevention of the disease, intravenous infusions take place. In this case, the timing of the use of intravenous catheters must be observed. This is necessary to prevent thromboembolism.
In the presence of thrombophlebitis of the lower extremities. Especially after surgery, wearing compression stockings is very important. This allows you to prevent possible complications. This complication is pulmonary infarction.
go to top
Causes
One of the main causes of the disease is pulmonary embolism (PE): it is responsible for 10 to 25% of clinical cases of pulmonary infarction. It has been suggested that there are actually many more of them - but often the pathology is not detected during life due to erroneous diagnosis and is not confirmed after death due to medical ethics (the need to react positively to the refusal of the relatives of the deceased to perform an autopsy). At the moment, it is believed that due to pulmonary embolism, death from pulmonary infarction occurs in 5-30% of patients with this disease .
PE is not only considered a pathology in itself with a high probability of oxygen starvation of the lung tissue, but the risk of fatal cases with a pulmonary infarction caused by it increases even more due to factors such as:
- lack of treatment;
- repeatedly recurrent thrombosis - repeated formation of a blood clot in the same vessel, often in the same place. The cause of relapses is physical and chemical compromise of the inner lining of the vessel;
- thromboembolism observed in the family (hereditary burden of pulmonary embolism);
age over 60 years;- taking hormonal contraceptives;
- obesity;
- pancreatic tumors;
- pulmonary hypertension (increased pressure in the pulmonary artery);
- background (concomitant) diseases that worsen the patient’s general condition;
- improper use of intravenous catheters used for drip infusions (they can provoke thrombus formation at the injection site).
Blood diseases are considered one of the most dangerous background diseases in terms of the occurrence of pulmonary embolism and subsequent pulmonary infarction - in particular:
- sickle cell anemia (red blood cells are shaped like a sickle);
- DIC syndrome (imbalance of the blood coagulation system, which leads to the formation of multiple blood clots).
In addition to PE, most clinical cases of pulmonary infarction develop in patients who suffer from other cardiovascular diseases (particularly chronic ones). First of all, these are heart pathologies such as:
atrial fibrillation (chaotic contraction of individual fibers of the heart muscle);- mitral stenosis (narrowing of the left atrioventricular orifice of the heart);
- coronary heart disease (damage to the heart muscle due to lack of oxygen);
- myocardial infarction as a complication of coronary artery disease (death of the heart muscle);
- cardiomyopathies (damages of various origins, except for blood supply disorders);
- infective endocarditis (infectious inflammation of the inner lining of the heart);
- atrial myxoma (benign tumor);
- heart failure;
- vasculitis (inflammation of blood vessels with their subsequent destruction)
and so on.
In heart pathology, blood clots in most cases form on the inner surface of the right atrium appendage. They can be held at the site of formation for some time until the blood flow tears them off and carries them into the arteries of the pulmonary circulation, thanks to which the lungs are supplied with blood.
Of other causes not related to heart pathology, the following diseases and conditions most often lead to pulmonary embolism, which provokes pulmonary infarction:
- thrombosis of the veins (usually deep veins) of the lower extremities;
- thrombophlebitis of the deep pelvic veins;
- bed rest prescribed in the postpartum or postoperative period for serious illnesses or required due to the specifics of certain conditions (for example, the patient being in a coma);
- immobilization (immobilization) of the upper and lower extremities during fractures.
Please note
Bed rest and immobilization of the limbs for even one week significantly increase the risk of thrombosis, leading to pulmonary infarction.
In the postoperative period, the risk of thrombosis with the development of pulmonary infarction is highest with:
- caesarean section;
- operations on the abdominal organs;
- gynecological interventions;
- surgeries on the chest organs;
- hemorrhoidectomy (removal of hemorrhoids);
- operations for varicose veins of the lower extremities, complicated by thrombosis or thrombophlebitis (inflammation of the vascular wall and the formation of a blood clot in this place).
Important
Particularly dangerous are blood clots that are attached to the inner surface of the vessel with a very small surface (compared to the entire surface area). Such blood clots are called floating (floating). They almost always come off and are carried by the bloodstream into the lobar and segmental vessels of the lung.
In addition to a blood clot (thrombus), the following can serve as an embolus that clogs a vessel:
- fat particles;
- accumulations of tumor cells;
- accumulations of microorganisms or their fragments;
- conglomerates of parasite eggs that have entered the bloodstream;
- gas bubbles.
Fat embolism of the blood vessels of the lungs can occur when:
- erroneous introduction of fat suspensions (suspensions) into the bloodstream;
- fracture of tubular bones - especially with polytrauma (multiple traumatic injuries - for example, in severe road accidents), when several bones break, and the risk of embolization increases significantly.
Tumor embolism can theoretically be caused by cells of any tumor, but in the overwhelming majority of cases it is caused by clusters of cells formed during the disintegration of malignant neoplasms in the terminal stages.
If the place where the embolus came from is unknown, such a pulmonary infarction is called primary; if it is determined, it is called secondary.
Treatment
Anticoagulants are of great importance in the treatment of pulmonary infarction. However, this treatment should be started immediately. This helps prevent possible complications.
The most widely used anticoagulant is heparin. Mostly in a dosage of twenty-five or thirty thousand units. Then dicoumarin, neodicoumarin, and pelentan are used.
However, the use of these drugs is not limited to just one prescription; direct monitoring is important. Monitoring involves daily determination of prothrombin and coagulation. There are certain rules.
I do not reduce prothrombin below fifty percent. Coagulation should occur in sixteen or eighteen seconds. Thanks to this treatment, the risk of repeated embolisms and thromboses is reduced.
Also in the treatment of the disease is the removal of spasms. Papaverine is administered intramuscularly. This eliminates pain.
Caffeine, camphor and cordiamin are administered. These drugs are most necessary for pulmonary infarction. If an inflammatory process is detected, then antibiotics are used.
It is also important to carry out treatment in a hospital setting. This allows you to avoid possible consequences. And also eliminate complications.
go to top
In adults
A lung infarction in an adult can be a consequence of some pathology. Moreover, these pathologies are associated with disorders in the hematopoietic system. The hematopoietic system may be associated with cardiac activity.
Women are more susceptible to pulmonary infarction than men. This is due to various conditions of the female body. It is known that the provoking factors in this case are:
- postpartum period;
- malignant tumors
Malignant tumors can also develop in men. Most often, this pathology causes a lot of complications. Ultimately leading to deaths.
Adults often experience different symptoms. The most common symptom is chest pain. Therefore, it should be distinguished from angina pectoris. Also common symptoms are:
- tachycardia;
- cyanosis;
- hemoptysis;
- arrhythmia;
- hypotension;
- cough;
- pale skin
From the abdominal organs, intestinal paresis is observed. Dyspepsia may also be present. But this phenomenon is not common in this case.
go to top
Myocardial infarction: causes and signs
Pulmonary infarction is a disease caused by a thromboembolic process in the vascular system of the lungs and, in especially severe cases, leads to the instant death of the patient. Hemorrhagic consolidation of the pulmonary parenchyma is a consequence of pulmonary embolism. The main cause of the pathology is blood clots that form in the vessels of the lungs or are brought in from peripheral veins. Inflammatory and sclerotic changes in the pulmonary artery and its branches often result in the development of thrombosis.
The thrombus blocks the lumen of the vessel, ischemia of the lung tissue occurs, the pressure in the affected artery reaches a maximum, which leads to hemorrhage into the lung. Infection of the affected area ends with the development of pneumonia, suppuration, and abscess formation.
Pulmonary infarction often occurs in people with heart diseases: congenital and acquired defects, arrhythmia, coronary heart disease, cardiomyopathy. Cardiac blood clots usually form in the right atrium, break off and travel to the pulmonary arteries. Slow blood flow or stagnation in the pulmonary vessels also leads to thrombosis. The pathology develops quickly, and the affected area falls out of the functioning pattern.
When the first signs of illness appear, the patient must be urgently taken to the hospital. After an X-ray contrast examination of the chest and electrocardiography, he will be prescribed fibrinolytic agents and drugs that improve the rheological properties of blood, which will improve the trophism of the damaged area. When the patient's condition has stabilized, they move on to antibacterial and anti-inflammatory therapy.
Causes
Various diseases can provoke the development of a pulmonary infarction:
- Rheumatism,
- Tumors,
- Sepsis,
- Bone fractures,
- Hypercoagulation,
- Phlebothrombosis and thrombophlebitis,
- Polycythemia,
- Anemia,
- Burns,
- Cardiomyopathy,
- Infectious kidney pathology,
- Endocarditis.
Obstruction of the pulmonary arteries leads to pulmonary ischemia. In this case, the permeability of blood vessels is disrupted, and the ischemic area becomes overfilled with blood. Occlusion of the pulmonary vessels and reflex vasoconstriction lead to overload of the right chambers of the heart. Due to blood stagnation, hypertension occurs in the pulmonary circle.
The affected area acquires a rich red color, becomes dense and rises above the healthy lung tissue. The pleural layers become dull, and hemorrhagic exudate accumulates in the pleural cavity. The risk of developing pathology increases if patients have floating blood clots. Insufficient oxygenation and trophism of the lung tissue lead to its dystrophy, and subsequently to necrosis.
Factors contributing to the development of pathology:
- Long-term hormone therapy
- Early postpartum period,
- Splenectomy,
- Taking medications that increase blood clotting
- Chemotherapy,
- Damage to the vascular wall during venous puncture,
- Overweight,
- Prolonged immobilization.
Symptoms
The symptoms of pulmonary infarction depend on the area of damage to the lung tissue and the general condition of the body. If the size of the lesion is small, clinical signs may be absent, and the disease is detected only with the help of X-ray diagnostics. With an asymptomatic course, radiological changes disappear on their own after 7-10 days. A microinfarction of the lung is detected accidentally during the treatment of its infectious consequences.
- Signs of acute blockage of the pulmonary vessels are the main symptoms of the pathology. The disease is characterized by a sudden onset with the appearance of acute chest pain and inspiratory shortness of breath against a background of general well-being. Pain syndrome is a clinical manifestation of ischemia.
- The cough in patients is dry at first, then becomes wet, and bloody, foamy sputum of a dark brown color is released. Sputum with bloody streaks is a characteristic sign of the hemorrhagic form of the disease. The reason for its appearance is the rupture of a vessel clogged with thrombotic masses and saturation of the lung tissue with blood.
- Shortness of breath is accompanied by a vascular reaction: pale skin, sticky and cold sweat.
- Myocardial ischemia often accompanies pulmonary infarction. This is due to impaired coronary blood flow. Among other symptoms of the pathology are: frequent shallow breathing, thready pulse, chills, fever, pale or gray skin, acrocyanosis.
Patients develop hypotension, cerebral disorders, hepatomegaly, abdominal syndrome, asthma attacks, atrial fibrillation, panic attacks, leukocytosis in the blood, and an increase in ESR. The doctor, examining patients, discovers characteristic percussion, percussion and auscultation signs.
Complications
Pulmonary infarction is a serious disease that leads to dangerous consequences and threatens the patient’s life.
Complications:
- Post-infarction pneumonia develops 10-14 days after a lung infarction. Patients suffer from sore throat and discomfort. They develop a dry or wet cough with a small amount of sputum, and hemoptysis. Chest pain worsens with every breath. During microbiological examination of sputum, atypical pathogens of pneumonia are detected - mycoplasmas, chlamydia, fungi.
- Purulent pleurisy is the result of infection of the pleural cavity. Usually the disease is a complication of pneumonia, pulmonary infarction, or abscess. Patients develop fever, chills, tachycardia, shortness of breath, cyanosis, sweating, chest pain, and cough. The prognosis of purulent pleurisy is always serious. Mortality reaches 20%.
- Post-infarction abscess formation of lung tissue occurs in a relatively short time after pulmonary infarction. As a result of necrosis and infection of the lesion, a cavity is formed in the lung tissue. A lung abscess breaks into the pleural cavity with the development of pleural empyema. With a favorable course of the pathology, the lung tissue becomes scarred.
- Spontaneous pneumothorax develops when air from the alveoli enters the pleural cavity. Patients experience acute chest pain, shortness of breath, tachycardia, and fear of death. Patients take a forced position that brings them relief. The prognosis of the disease is favorable. Relapses are possible.
- Scars on the lung after a heart attack can have different sizes, on which the clinical picture of the pathology depends. With diffuse pneumosclerosis, when there are many scars on the lung, patients experience shortness of breath, weakness, difficulty breathing, and tingling in the chest. If the pathology is not treated, it will develop into cardiopulmonary failure.
- Pulmonary hemorrhage is characterized by the release of dark blood mixed with sputum, clots and food masses. Profuse bleeding can lead to death. When the first signs of bleeding appear, the patient must be immediately hospitalized in a hospital. Blood that constantly enters the respiratory tract should be coughed out. The most dangerous complication of pulmonary hemorrhage is asphyxia. In the hospital, the source of bleeding is determined and appropriate treatment is carried out.
- Rupture of an aortic aneurysm is manifested by severe burning and tearing pain in the chest, a sharp drop in blood pressure and other signs of cardiogenic shock. If patients do not seek medical help in time, they are unlikely to be helped.
- Lung gangrene is a destructive process in the lung tissue caused by exposure to putrefactive bacteria. An early sign of the disease is bad breath. Then patients experience hemoptysis, production of large amounts of sputum, fever, chills, and they suddenly lose weight. The disease is very difficult. If lung gangrene is not treated, sepsis develops and death is possible.
Diagnostics
Before starting treatment for a pulmonary infarction, a specialist must identify the disease that became its direct cause. Diagnosis of pulmonary infarction consists of conducting a thorough examination of the patient, instrumental and laboratory examination.
The radiograph shows a thin wedge-shaped shadow in the middle field, usually on the right. The ischemic area has the shape of a pyramid, the base of which faces the periphery, and the apex faces the root of the lung. The characteristic triangular opacification is located in the middle and basal segments of the lung. Additional diagnostic methods are ECG, CT, MRI.
Treatment
Pulmonary infarction is an emergency condition that requires emergency medical care in the intensive care unit of a hospital.
Treatment of pulmonary infarction is complex and long-term. The patient is prescribed several groups of drugs that dissolve blood clots and eliminate the symptoms of the pathology.
- Treatment begins by administering fibrinolytics to the patient. In the absence of severe arterial hypertension, the following fibrinolytic agents are used - “Streptokinase”, “Urokinase”, “Tissue plasminogen activator”. These medications are contraindicated for persons who suffered a stroke a month ago, as well as those suffering from hemorrhagic diathesis, and pregnant women. In severe cases, they switch from thrombolytic therapy to surgery - thrombectomy.
- Patients with pulmonary infarction are prescribed direct and indirect anticoagulants. Heparin is a drug that does not dissolve a blood clot, but prevents its growth and stops the process of thrombus formation. This medicine reduces spasm of the pulmonary capillaries, alveoli and bronchioles. Heparin therapy lasts ten days. Then they move on to treatment with Dicoumarin, Neodicoumarin, and Phenilin. Anticoagulants prevent further thrombus formation and prevent re-embolization.
- Antiplatelet therapy is carried out to prevent recurrent thrombosis. Patients are prescribed Aspirin, Thrombo ACC, Cardiomagnyl.
- Narcotic analgesics are used for acute pain. They relieve pain, improve blood circulation, and relieve shortness of breath. A 1% Morphine solution is administered intravenously. Non-narcotic analgesics are prescribed when pleural pain appears during breathing and coughing, or when body position changes. A 50% Analgin solution is administered intravenously.
- To relieve reflex vascular spasm, large doses of antispasmodics - Papaverine, Drotaverine - are administered intramuscularly.
- When pulmonary hemorrhage develops, calcium supplements are used.
- To treat shock, vasopressors are used - Dopamine, Dobutomin.
- "Eufillin" is administered intravenously slowly in the presence of bronchospasm.
- After stabilization of the patient's condition, they proceed to antibacterial therapy and standard symptomatic treatment. Antibiotics are prescribed to prevent pneumonia and suppuration. Typically, broad-spectrum drugs are used from the group of fluoroquinolones - Ciprofloxacin, macrolides - Azithromycin, cephalosporins - Ceftriaxone, penicillins - Amoxicillin.
- Intravenous injections of cardiac glycosides - “Strofanthin”, “Korglikon” - will help to ease the work of the heart.
- To improve the rheological properties of blood and accelerate regeneration processes in tissues, Trental, Cavinton, Actovegin are used.
- In case of severe hypertension, intravenous administration of Furosemide is prescribed. The drug ensures blood redistribution and a decrease in its volume in the lungs. Lasix is also used intravenously.
- For hypotension, Prednisolone, Strophanthin and Reopoliglucin are administered intravenously. In this case, all of the above therapeutic measures are prohibited. To combat collapse, Dopamine, Glucose or sodium chloride are administered intravenously.
- In case of pulmonary infarction, a vena cava filter is installed in the inferior vena cava, which will retain blood clots and prevent them from entering the systemic circulation.
In children
Pulmonary infarction in children occurs after infections. Which is pneumonia, typhoid fever. Also associated factors are the development of scarlet fever and influenza.
A feature of the disease in children is the small size of the infarction. At the same time, they do not contribute to the development of pronounced symptoms. But in older children, bloody sputum is observed. It is a sign of disease.
A common symptom in older children is tachycardia. And also shortness of breath. This is the most common symptom in childhood. If these symptoms are present, a diagnosis must be made.
Diagnostics will involve the use of various techniques. Anamnesis collection and ultrasound diagnostics take place. As well as laboratory tests.
Laboratory methods are the most informative. Depending on the age of the child, x-rays are prescribed. An ECG may be ordered. Consultation with a pulmonologist and cardiologist is very important.
go to top
Pulmonary infarction
A pulmonary infarction is similar to a myocardial infarction. They are characterized by such a situation: in a certain area, the blood supply stops, because of this, tissue begins to die.
But there is one defining difference: you cannot die from a pulmonary infarction.
The development of a pulmonary infarction occurs because the lumen of the blood vessels is blocked, and does not allow the blood flow to function normally. This disease develops too quickly, it only takes a day. In addition, the degree of damage may vary.
The reasons for blockage of the lumen of a vessel can be different; they cause all sorts of diseases, thrombophlebitis, thrombosis and many others.
Possible causes and factors of the disease
The first cause of a pulmonary infarction is the appearance of blood clots in the blood vessels. When the lumen of a vessel is blocked by a blood clot, a person begins to have an attack. At the site of the clot, there may be a detached thrombus.
Attacks mainly appear with pulmonary fat embolism, leg thrombosis or thrombophlebitis.
The cause of a blood clot can be surgical intervention, in particular if it was performed on the blood vessels of the extremities. This situation causes a lung infarction and then a heart attack.
Factors that can give impetus to the development of the disease are called:
- Genetic predisposition.
- Chronic diseases.
- Poor circulation.
- Injuries to the walls of blood vessels.
- Changes in blood composition.
- Medicines for blood clotting.
- Excess weight.
- Heart diseases.
- Tumors that put pressure on blood vessels.
- Passive lifestyle.
- Use of contraceptives.
If the lumens of medium-sized or small-sized vessels located in the lungs are clogged, then the patient cannot die from such a disease. But if such a situation occurs in a large blood vessel, then in most cases, the patient dies.
But there are other reasons, these are diseases, vasculitis, anemia, nephrotic syndrome, or completed courses of radiation and chemotherapy procedures. A severe bruise can also cause blockage of a vessel. In this case, the disease will be called traumatic pulmonary infarction.
Signs of illness
Symptoms of pulmonary infarction will appear depending on the location of the lesion, the degree of development and the number of blocked vessels. In addition to these signs, symptoms of other lung and heart diseases will be added.
A pulmonary infarction is easier to detect if a person simultaneously suffers from heart disease.
During a consultation with a doctor, he will conduct a visual examination of the patient and question him about existing symptoms that can confirm the presence of the disease.
And they are:
- Pain under the ribs.
- Cardiopalmus.
- Fever or body chills.
- Panic attacks, shortness of breath.
- Coughing up blood.
Very often, it is the presence of blood when coughing that appears after pain in the hypochondrium. And with a fever, a person becomes covered in cold, sticky sweat.
During pneumonia, a lung infarction that appears manifests itself in severe pain, but there is no shortness of breath or rapid heartbeat. The person does not panic. In some cases, pulmonary infarction does not manifest itself. And it can be diagnosed using x-rays.
An emerging pulmonary infarction exhibits the following symptoms:
- Rapid development of shortness of breath, which has not been observed before.
- Coughing up blood.
- Coughing up blood.
- The appearance of fever.
- Sudden sharp pain under the shoulder blade, which gets worse when coughing.
- Pale skin.
- Blue discoloration of fingertips, nose and lips.
- Weak pulse.
- Increased sweating.
- The appearance of wheezing.
- Low pressure.
- Pain in the liver on palpation.
- Heat.
- Lack of air.
All signs appear depending on the degree of development of the disease (infarction pneumonia) and its type, and there are several of them:
Hemorrhagic
This type of disease occurs due to arterial thrombosis and embolism. In this case, heart attack pneumonia shows the following signs: shortness of breath appears suddenly. And after a short time there is a burning pain in the sternum, which radiates to the shoulder blade or armpit.
As already mentioned, this type occurs due to thrombosis, and this, in turn, is due to infectious diseases, bruises, previous operations on blood vessels, or too long rehabilitation after surgery.
The symptoms of this type of disease are too pronounced, so they cannot be ignored.
The onset of the attack is characterized by the appearance of cold sweat and the appearance of chills. Then pain begins to appear in the area of the shoulder blade or in the armpit. The more advanced the disease, the stronger the pain will be, and then there will be compression in the chest. There may be a cough and shortness of breath, pale skin, and profuse sweat. And if the damage to the blood vessels is too severe, then jaundice will appear.
The cough with such pneumonia is initially dry, and then blood appears. In advanced cases, the blood changes color and becomes dark brown.
When listening, the doctor may hear wheezing and heavy breathing.
Right lung
Almost always, this type of disease occurs when the blood vessels through which blood enters the right lung are blocked. And this also happens due to thrombosis of the pulmonary artery. In addition, a heart attack on the right side may occur due to:
- During the period after childbirth.
- After surgery.
- The resulting fracture of tubular bones.
- Heart failure, chronic.
- Development of a cancerous tumor.
- Stagnation of blood in the lungs.
There are reasons that directly indicate that an attack has begun: pressure on the chest, shortness of breath, foamy cough and high body temperature.
The pain usually appears on the right side and the person may begin to choke.
You can’t ignore these signs, and you shouldn’t try to take any medicine to get rid of them on your own. A person in this situation must be immediately hospitalized so that he can be given an accurate diagnosis and prescribed effective treatment, which should take place in a hospital setting under the supervision of doctors.
Left lung
Pulmonary infarction on the left side also develops due to embolism of blood vessels or thrombosis. All signs of a heart attack on the left side are the same as on the right. Only the pain is felt more on the left side. Signs of this type of heart attack are: shortness of breath, high fever, coughing and coughing up blood. The heart rate also increases and breathing becomes weaker.
This type is characterized by panic attacks, anxiety and lack of coordination. In some cases, diarrhea and vomiting occur. To save a person’s life, or reduce the risk of complications, he must be urgently sent to the hospital. There he will receive qualified assistance in diagnosis and treatment.
Possible consequences of the disease
If a pulmonary infarction is detected and its treatment is started on time, then complications may arise that can be quite serious. This is how the appearance of bacterial pneumonia and pus is observed in the area where the heart attack occurs.
The appearance of pneumonia is considered the most common complication of pulmonary infarction. And all because after a heart attack, the affected area becomes non-viable. During the disease process, blood does not flow into this area, it does not function during breathing, and as a result, infectious diseases arise. The larger the affected area, the more likely pneumonia is to occur.
However, pneumonia is not the only complication; pus may also appear and fill the lungs. As a result, a breakthrough is possible, after which healthy tissues will also fill.
The most severe consequence is called a lung abscess. Inflammation of a large part of the organ occurs, a lot of pus accumulates and the temperature rises greatly.
The occurrence of complications will depend on the area of the lesion and the time of treatment started.
Diagnosis
Upon admission to the clinic, the doctor begins to examine the patient and collects anamnesis. This procedure involves two specialists - a cardiologist and a pulmonologist.
The first procedures involve listening to the chest for fluid and wheezing. After this, the patient’s blood pressure and pulse are measured, and the abdomen is palpated, which may indicate an enlarged liver.
To make a correct diagnosis, the manifestation of all symptoms should be clearly explained, and exactly where the patient experiences pain should be indicated. He must also indicate the nature of the pain, because a heart attack can easily be confused with pulmonary inflammation.
In addition, laboratory and hardware tests are carried out. The latter include:
- X-ray. This diagnostic method is mandatory, because it is considered the main one.
- CT scan. This method is also important because, in combination with x-rays, it confirms or refutes the diagnosis.
Treatment of the disease
During treatment, it is necessary for pulmonary vascular occlusion to disappear, so all therapy is aimed at this. The doctor prescribes medications to the patient that thin the blood and dissolve blood clots.
These means can be:
- Heparin.
- Urokinase.
- Fraxiparine and others.
The course of treatment lasts no more than seven days, at first a large dose is administered, and then it is gradually reduced. During treatment, aspirin may be added to these drugs to prevent thrombosis.
If the pain is severe and the patient cannot tolerate it, then morphine is prescribed.
In parallel with these drugs, the patient is prescribed drugs to prevent complications. It could be ceftriaxone. To prevent fluid from collecting, furosemide is administered intramuscularly.
At the beginning of the attack, when the patient is still at home, he needs to be given a nitroglycerin tablet and call an ambulance. At the hospital, he is given the drug intravenously. Doctors also monitor blood pressure there.
But if the patient has low blood pressure upon admission, then the above drugs are not used, but other means are used.
In addition to medications, surgery is also used.
Prevention
It must be remembered that it is always easier to prevent a disease than to treat it later. Therefore, experts advise regular prophylaxis with medications to prevent the formation of blood clots.
If a person has high blood pressure and too thick blood, thinners should be taken.
If the human body is prone to the formation of blood clots, clotting agents should not be taken. And if an operation was performed, you need to spend several days in bed.
wmedik.ru
Forecast
In case of pulmonary infarction, the prognosis directly depends on the presence of complications. And also the treatment carried out. More precisely, its effectiveness.
A major role is played by the presence of concomitant diseases. Since infectious diseases worsen the prognosis of the disease. This is something to keep in mind!
Only correct treatment therapy and timely diagnosis improve the prognosis. Immediate treatment is also very important. Namely, the use of anticoagulants.
go to top
Exodus
Pulmonary infarction may be characterized by sudden death. This occurs with heart failure. Since the heart in this case has a number of pathological disorders associated with thrombophlebitis.
The presence of relapses, pneumonia during pulmonary infarction leads to an unfavorable outcome. Since the process is often aggravated by suppurative foci. This significantly worsens the picture of the disease.
In the presence of pulmonary edema, the prognosis is also worst. However, treatment must be comprehensive. Only complex therapy will improve the outcome of the disease.
go to top
Consequences and forecasts
In rare cases, the pathology leads to death. The prognosis is influenced by the timeliness of treatment measures and the occurrence of secondary diseases. Complications include the replacement of dead lung cells with connective tissue, which impairs the functioning of the damaged organ. In addition, other negative consequences may appear:
- a lung abscess forms during pneumonia or in the area of necrosis;
- heart attack-pneumonia develops with inflammation of tissue near the lesion, due to stagnation of blood and can provoke the addition of a bacterial pathogen, respiratory failure and the development of adhesions;
- pulmonary failure in chronic form;
- collapse caused by a sharp drop in blood pressure.
A favorable prognosis is observed with timely elimination of cardiopulmonary problems with the help of anticoagulants. In most cases, patients return to a normal rhythm of life. The situation can only get worse due to complications.
Lifespan
With a pulmonary infarction, life expectancy may not be reduced. Especially if the necessary treatment has been carried out. And also there are no complications.
If the disease is aggravated by other concomitant pathologies, then life expectancy may decrease. Especially in the presence of suppurative processes. This process will be quite difficult to stop.
Attention must be paid to cardiac disorders. That's why they take certain medications. To reduce the risk of developing heart failure. This increases the quality of life and its duration!