What is premature depolarization of the ventricles and atria?
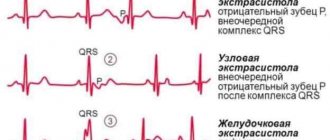
Premature Ventricular Depolarization
Premature ventricular depolarization (PVD) is a condition also known as premature ventricular complex or ventricular premature contraction.
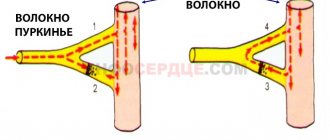
This is a relatively common condition in which the heartbeat is initiated by Purkinje fibers in the ventricles rather than in the sinus node, where the electrical impulse originates. An ECG can detect premature ventricular depolarization and easily identify cardiac arrhythmias. And although this condition is sometimes a sign of reduced oxygenation of the heart muscle, PDs are often natural and can be characteristic of even a generally healthy heart.
Figure 1. Premature ventricular depolarization
PJP may feel like a normal racing heartbeat or a “missed beat” of the heart. In a normal heartbeat, the activity of the ventricles after the atria is clearly coordinated, so the ventricles can pump the maximum amount of blood, both to the lungs and to the rest of the body.
With premature depolarization of the ventricles, they become active ahead of time (contract prematurely), therefore, normal blood circulation is disrupted. However, PJD is usually not dangerous and is asymptomatic in healthy people.
Premature atrial depolarization
Depolarization and repolarization
The section "Basic principles of electrocardiography and disorders" discusses the general concept of "electrical excitation" , which means the propagation of electrical impulses through the atria and ventricles. The exact name for electrical excitation, or activation of the heart, is depolarization . The return of cardiomyocytes to a state of relaxation after excitation (depolarization) is repolarization . These terms emphasize that at rest, the myocardial cells of the atria and ventricles are polarized (their surface is electrically charged). Figure 2-1, A shows the state of polarization of a normal muscle cell of the atria or ventricles
The outside of the cell at rest is positively , and the inside is negatively charged [about -90 mV (millivolts)]. Membrane polarization is caused by the difference in ion concentrations inside and outside the cell.
When the muscle cell of the heart is excited, it depolarizes. As a result, the outer side of the cell in the region of excitation becomes negative, and the inner side becomes positive. There is a difference in electrical voltage on the outer surface of the membrane between the depolarized area in the state of excitation and the unexcited polarized area, see Fig. 2-1, B. Then a small electric current arises, which spreads along the cell until it is completely depolarized, see Fig. 2-1, V.
The direction of depolarization is shown by an arrow, see Fig. 2-1, B. Depolarization and repolarization of individual muscle cells (fibers) occurs in one direction. However, throughout the myocardium, depolarization proceeds from the inner layer (endocardial) to the outermost layer (epicardial), and repolarization occurs in the opposite direction. The mechanism for this difference is not completely clear .
The depolarizing electric current is recorded on the electrocardiogram in the form of the P wave (excitation and depolarization of the atria) and the QRS complex (excitation and depolarization of the ventricles).
After some time, the depolarized cell, completely engulfed in excitation, begins to return to a resting state. This process is called repolarization . A small area on the outside of the cell again acquires a positive charge, see fig. 2-1, G, then the process spreads along the cell until it is completely repolarized. Ventricular repolarization on the electrocardiogram corresponds to the ST segment, T and U waves (atrial repolarization is usually hidden by ventricular potentials).
An electrocardiogram shows the electrical activity of all cells in the atria and ventricles, rather than individual cells. In the heart, depolarization and repolarization are usually synchronized, so on the electrocardiogram these electrical flows can be recorded in the form of certain waves ( P , T , U , QRS complex , ST segment ).
Etiopathogenesis of extrasystole in children
The human heart consists of four chambers. The two upper chambers are called atria, and the lower two are called ventricles.
The atria send blood to the ventricles, and from the ventricles blood flows to the lungs and other organs of the body. The right ventricle sends blood to the lungs, and the left ventricle sends blood to other organs. The heartbeat (or pulse), which is counted during diagnosis, is the result of contraction of the ventricles of the heart.
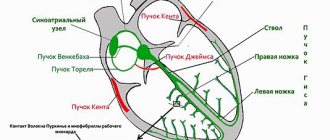
The heartbeat is regulated by the heart's electrical system. The heart's electrical system consists of the sinus node (SA), the atrioventricular node (AV), and special tissue in the ventricles that conduct electrical impulses.
The sinus node is the electrical regulator of the heart's rhythm. This is a small area of cells located in the wall of the right atrium.
The frequency at which the sinus node releases electrical impulses determines the speed at which the heart beats normally. The sinus node helps maintain a normal heartbeat.
At rest, the frequency of electrical impulses emanating from the sinus node is low, so the heart contracts in the lower normal range (60 to 80 beats per minute). During physical exercise or in a state of nervous excitement, the frequency of impulses of the sinus node increases.
People who exercise regularly may have a lower heart rate than normal in old age, but this is not a cause for concern.
Electrical impulses travel from the sinus node through special tissues of the atrium to the atrioventricular node and through the AV node to the ventricles, causing them to contract.
Extrasystoles can be congenital or acquired; etiologically caused by cardiac, extracardiac and combined factors.
Cardiac causes of arrhythmia include congenital and acquired heart defects, primary and secondary cardiomyopathy, rheumatic carditis, infective endocarditis, non-rheumatic carditis and other intracardiac pathology.
It has been proven that extrasystole is more common in children with mitral valve prolapse and other minor structural abnormalities of the heart compared to children without them.
A special etiological group consists of genetically determined diseases, in which arrhythmias (ventricular ES, ventricular tachycardia) are the main clinical manifestation.
, Corrado D. Marcus F.
, 2009; Boqueria L. A
, Revishvili A. Sh
, Neminushchiy N. M
, 2011). In half of the cases, the disease is familial and is a common cause of sudden cardiac death.
ARVD must be excluded in every patient with mono- or polytopic ventricular ES. Currently, the Marcus F criteria are used to diagnose ARVD.
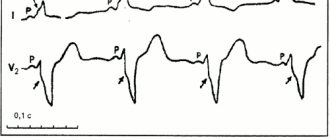
(2010), based on data from electrocardiography, echocardiography, MRI, ventriculography, and histological examination. An important ECG criterion for ARVD is the presence of an epsilon wave (e-wave) in patients with ventricular arrhythmias.
The epsilon wave is a reproducible low-amplitude signal between the end of the QRS and the beginning of T wave in the right precordial leads (Fig. 1).
Extrasystoles can be observed in diseases of the nervous and endocrine systems (diabetes mellitus, thyrotoxicosis, hypothyroidism), acute and chronic infectious processes, intoxication, overdose or inadequate reaction to medications, deficiency of certain microelements, in particular magnesium, potassium, selenium.
To date, there are indications of the role of foci of chronic infection, in particular chronic tonsillitis, in the genesis of extrasystole, but it has not been fully proven.
It has been established that ES can be a manifestation of viscero-visceral reflexes in cholecystitis, diseases of the gastroduodenal zone, gastroesophageal reflux, diaphragmatic hernia, etc.
The appearance of ES after severe emotional and physical overload is explained by an increase in the concentration of catecholamines in the blood. The genesis of extrasystole is also influenced by autonomic dysfunction and psychogenic changes.
What does it represent?
Muscle contraction under the influence of electric current has been known since the first generation of electrical charges and the creation of batteries and electrical elements. A little later it was discovered that nerve tissue can conduct electrical current and cause contraction of the innervated muscle.
Genetic variations in ion channel properties have been incriminated, but no robust genetic profiling has been performed. Data were collected from centers in 22 countries, included people under 60 years of age, and were compared with data from a control group. Information on history of syncope, physical activity level, waveform-averaged electrocardiography, and pharmacological testing was confirmed by electrophysiological testing using multielectrode catheters.
Even before the advent of methods that made it possible to study electrical activity in organs and tissues, scientists came to the conclusion that muscle contraction and the conduction of impulses along nerve fibers are associated with electric current.
Only three types of cells have electrical activity: nerve, muscle and glandular cells.
The primary endpoint was examined over a 30-year follow-up period. Some controversy has arisen from these studies, and doubts have been raised about the validity of these results. In addition, the incidence of arrhythmia was significantly higher in the follow-up period in these individuals.
The more important fact to consider is that since these results were published, more attention has been paid to this “benign” phenomenon. To integrate all of the above, is it or is it not friendly and why is it so important to know? First of all, we must take into account that sudden cardiac death is not at all an unreasonable cause of death; Most of these sudden heart failure cases are caused by ventricular tachyarrhythmias, which occur in 6% to 14% of cases in individuals without structural heart disease, so it is important that any population definition tool be at risk.
Ventricular repolarization syndrome
Where does electric current come from, namely potential difference? For a long time, due to the impossibility of studying the processes occurring inside the cell, and especially in very thin cell membranes, scientists believed that some kind of primitive electrochemical reaction was taking place, like in a car battery.
There is no specific treatment for this person, taking into account that its pathological nature has not been established. Without knowing what exactly causes this phenomenon, it is difficult to declare its benign quality. Early repolarization syndrome: a new electrical disorder associated with sudden cardiac death.
Cardiac repolarization - basic and clinical science. Early repolarization syndrome: an autosomal dominant malignant form in large French families. This followed due to the prevailing view that the nature of these phenomena was largely "benign". Early repolarization changes consistent with Brugada syndrome were interpreted as "innocent" and therefore ignored for decades until the so-called "early repolarization syndrome" was widely and unequivocally considered "normal", "normal variant" or benign early repolarization before .
Cephalopods helped scientists understand the processes occurring in the cell membrane. A species of squid with huge neurons was discovered; they were tens or even hundreds of thousands of times larger than human cells. The squid axons were 1 mm in size, and if you spend a few hours searching, you can find as much as 2 mm!
It was possible to completely immerse giant electrodes from the middle of the last century in such a cage and measure voltage.
Available experimental data suggest that. Steady progress over the past decade has advanced our understanding of the molecular, cellular, and genetic basis of this primary hereditary channelopathy and its arrhythmogenic potential. It should be noted that similar changes may appear in other directions, but to a lesser extent.
Electrophysiological features
In these cases, genetic tests are sometimes useful to determine the primary channelopathy and therefore the most appropriate treatment. Phenotypic expression is highly dependent on or modulated.
Cellular, molecular and genetic considerations
Therefore, identifying high-risk patients is one of the most challenging tasks in clinical cardiology.
For their study of chemical processes and the occurrence of membrane potentials on giant squid axons, Hodgkin and Huxley received the Nobel Prize in Physiology or Medicine.
Where does electricity come from?
The ionic composition of extracellular and intracellular fluid turned out to be different. Inside the cells of excitable tissues there are much more potassium ions and protein ions than outside the cells. Outside the cells there is many times more sodium and chlorine. The osmotic pressure inside and outside the cells is the same, but the charge is different due to the fact that protein anions are polyvalent, and chlorine anions are monovalent.
Treatment, follow-up and clinical recommendations
Electrical heart diseases: genetics, mechanisms, treatment, prevention.
The early pattern of repolarization in the general population is clinically correlated and heritable. Understanding early repolarization. Prevalence of electrocardiographic abnormalities in Western Asian and African athletes. Cardiac adaptation in black athletes: differentiating pathology from physiology. Athlete's heart or hypertrophic cardiomyopathy? Early repolarization in patients with spinal cord injury: prevalence and clinical significance.
Electrical circuit for pulse shortening
Excitation of the cell - depolarization - occurs when potassium ions leave the cell along a concentration gradient, and sodium ions enter the cell. Despite the fact that the cell membrane is a classic semi-permeable membrane, and there is a huge difference in ion concentrations, this transport is energy dependent.
Two of these factors, early repolarization syndrome and Brugada syndrome, are fairly well characterized, allowing correct diagnosis in most patients. The first part of the repolarization of the ventricular myocardium is determined by the Ito current, that is, a fast outward flow of potassium. The proposed mechanism for ventricular fibrillation and ventricular tachycardia storms is that faster I-flow in the epicardium than in the endocardium results in an electrical gradient that forms the substrate for phase 2 re-engagement.
Prevention of Ito flow with quinidine supports this mechanism. A key challenge is identifying individuals at increased risk of sudden cardiac death. The role of electrophysiology studies in provoking ventricular tachycardia or fibrillation has not yet been determined. Radiofrequency ablation of the epicardial substrate in the right ventricle in Brugada syndrome is also under critical evaluation. In medicine, it is defined as any combination of signs and symptoms that indicate a specific disease or disorder with multiple etiologies.
It contains 8 useful medicinal plants that are extremely effective in the treatment and prevention of arrhythmia, heart failure, atherosclerosis, ischemic heart disease, myocardial infarction, and many other diseases. Only natural ingredients are used, no chemicals or hormones!
The electrical activity recorded by the electrocardiogram is a record of action potentials resulting from the movement of ions across the myocardial membrane, causing depolarization, followed by the return of the ions to the ground state, causing repolarization.
Genesis of abnormal action potential
This action potential has five components, designated phases 0-4, 0 depolarization and 1-4 repolarization. We will discuss the pathophysiology, clinical constellation of symptoms, diagnostic methods, and treatment of these conditions. There are 8 types of potassium currents. The ventricular myocardium has actually three layers of muscle: the epicardial, M-cell and endocardial layers. To some extent, M cells resemble Purkinje cells.
The cell membrane has special pumps that use the energy of ATP phosphate bonds to pump ions.
Following depolarization and the occurrence of an action potential, repolarization occurs. Returning the electrical potential of the cell membrane is a much more energy-intensive process. Sodium and potassium pumps pump ions against the concentration gradient; this requires many times more energy than depolarization. If repolarization occurs quickly in a cell, it means that it restores its function faster.
Early repolarization syndrome
In the normal state, there is a uniform genesis of the action potential through three layers.
An anomaly in any layer will result in an aberration in the action potential and the development of an ion gradient between the layers, followed by the development of slow conduction, forming a substrate for phase reentry. Type 1: Early repolarization pattern predominantly in the lateral atrial leads. Type 3: Early pattern of repolarization worldwide in the inferior, lateral, and right precordial leads and is associated with the highest risk of malignant arrhythmia. The genetic basis of early repolarization has not been determined. Recommendations regarding sport participation and family selection have not yet been determined, but hopefully ongoing research will show us the light in the near future.
Repolarization is a physical term. At rest, the cell membrane is polarized; a negative potential accumulates inside the cell relative to the environment outside the cell membrane. The disappearance of polarization is called depolarization, and its restoration is called repolarization.
It is common in Asian and Southeast Asian countries, especially Thailand, the Philippines and Japan, reaching 5-1 in some parts of Asia. LRS appears to be the most common cause of natural death in men under 50 years of age. The reason for this higher prevalence in Asia is unknown. Having a more noticeable transient external current in men may be beneficial.
Higher testosterone levels may also play a significant role in male predominance. Twelve responsible genes have been reported so far. These symptoms often occur during febrile illness, rest or sleep, or with vagotonic conditions, but rarely during exercise.
Thus, without the process of repolarization, myocardial cells would not be able to perform their main task, namely the contraction function.
Doctors pay attention to the condition when the cells of the left ventricle begin to restore their polarization ahead of schedule; this condition is called early ventricular repolarization syndrome.
The syndrome usually appears in adulthood, with a mean age of sudden death of 41 ± 15 years. All authors are not eligible to declare. Report of the American Heart Association Committee on Standardization of Electrocardiographic Nomenclature. Sudden cardiac arrest associated with early repolarization. Experimental hypothermia: changes in the respiratory system and blood in relation to cardiac function.
Who has similar disorders?
Ventricular fibrillation causes sudden death in Southeast Asian immigrants. Characteristics of recurrent ventricular fibrillation associated with the nephrolateral early repolarization role of drug therapy. She had no chest pain and cardiac biomarkers were normal.
Considering that early left ventricular repolarization syndrome is an electrophysiological process, this condition can only be detected on an electrocardiogram.
Early ventricular repolarization syndrome is certain changes in the electrocardiogram in which the ST segment rises and shifts. In addition to these signs, changes in the T and P waves are also possible; the presence of a J wave is characteristic.
Benign early repolarization plus pericarditis
Example 1 Example 2 Features suggestive of pericarditis.
These features are of limited specificity, so it is not always possible to tell the difference between the two conditions. Historically, it has been considered a sign of good health because it is more common among athletes, younger people and at lower heart rates. Scientists at the Masonic Medical Research Laboratory were at the forefront of research in this early repolarization. It has long been ignored as just a harmless abnormality, but in fact it is an indicator that some forms of early repolarization can lead to the development of life-threatening arrhythmias. Review from our reader Victoria Mirnova
I’m not used to trusting any information, but I decided to check and ordered a bag. I noticed changes within a week: the constant pain and tingling in my heart that had tormented me before receded, and after 2 weeks disappeared completely. Try it too, and if anyone is interested, below is the link to the article.
Both can lead to sudden cardiac arrhythmic death. They then transform fibroblasts from the skin biopsy into stem cells and direct the differentiation of the stem cells into heart cells. Muscles are responsible for circulating blood throughout the body and use electrical signals from the heart to control heart rate. When the heart's electrical system does not function as expected, early repolarization may occur.
Young Adult African American Athletes. . At times it was even considered an indicator of good health. During a physical examination, the doctor will listen to the patient's heart to determine if there is an abnormal heart rate. Patients are also offered a detailed description of any symptoms that may be present, as these symptoms may indicate another heart condition.
The figure shows an electrocardiogram with changes characteristic of cardiac repolarization.
Early ventricular repolarization syndrome
Causes
- Heart failure.
- Acute respiratory failure, hypoxia, chronic obstructive pulmonary disease.
- Cervical osteochondrosis.
- Heart defects.
- Cardiac ischemia.
- Overweight, stress, overwork.
- The effect of certain medications (digitalis, procainamide, quinidine).
- Drinking alcohol, coffee, smoking.
- Pregnancy, menopause, premenstrual period, puberty.
- Thyrotoxicosis.
- Anemia.
- Heart disease - heart defects with valve damage, myocardial ischemia, myocarditis, cardiac injury, tachycardia
- General pathologies - electrolyte disturbances, vegetative dystonia, menopause, premenstrual period, hypoxia, hypercapnia, anesthesia, infection, surgery, stress.
- Taking medications, including antiarrhythmics, aminophylline, amitriptyline.
- Drinking alcohol, drugs, smoking.
The process of early repolarization is not yet fully understood. The most popular hypothesis for its origin states that the development of the syndrome is associated either with increased susceptibility to a heart attack in ischemic diseases, or with minor changes in the action potential of cardiomyocytes (heart cells).
According to this hypothesis, the development of early repolarization is associated with the process of potassium leaving the cell.
Another hypothesis about the mechanism of development of SRR indicates a connection between disturbances in the processes of depolarization and repolarization of cells in certain areas of the heart muscle. An example of this mechanism is Brugada syndrome type 1.
The genetic causes of the development of SRGC continue to be studied by scientists. They are based on mutations of certain genes that affect the balance between the flow of some ions into the heart cells and the release of others outside.
- long-term use or overdose of adrenergic agonists;
- hypothermia;
- familial type of hyperlipidemia (congenital elevated levels of low-density lipoproteins and insufficient levels of high-density lipoproteins in the blood), the consequence of which is atherosclerotic heart disease;
— the patient has dysplastic connective tissue disorders in the form of the appearance of additional chords in the cavity of the ventricles of the heart;
— obstructive hypertrophic cardiomyopathy in 12% of cases is associated with manifestations of early repolarization syndrome;
— the patient has a congenital or acquired heart defect.
Recently, studies have begun to appear aimed at identifying the possible genetic nature of this pathology, but so far no reliable data on the inheritance of early repolarization syndrome have been identified.
Causes of premature atrial depolarization
The main causes of PPD are the following factors:
- smoking;
- alcohol consumption;
- stress;
- fatigue;
- poor, restless sleep;
- taking medications that cause cardiac side effects.
Typically, premature atrial depolarization is not dangerous and is not a cause for concern. Often, atrial premature contractions occur due to cardiac injury or a disease related to cardiac function.
Causes of premature ventricular depolarization
The main causes of PJD are:
- acute myocardial infarction;
- valvular heart disease, especially mitral valve prolapse;
- cardiomyopathy (for example, ischemic, dilated, hypertrophic, infiltrative);
- heart contusion (consequence of injury);
- bradycardia;
- tachycardia (excess catecholamines);
Non-cardiological causes of PJD may be:
- electrolyte disturbances (hypokalemia, hypomagnesemia, hypercalcemia);
- taking medications (for example, digoxin, tricyclic antidepressants, aminophylline, amitriptyline, pseudoephedrine, fluoxetine);
- taking drugs such as cocaine, amphetamines;
- consumption of caffeine and alcohol;
- taking anesthetics;
- surgical interventions;
- infectious diseases with severe inflammation;
- stress and insomnia.
Causes
Taking into account the fact that SRGC is a highly conditional disease, the proposed list of possible (!) risk factors should be treated with some skepticism. The reasons themselves may be as follows:
- taking certain medications (adrenergic agonists);
- too much physical activity, especially if it is stimulated by pharmacological drugs;
- cardiovascular diseases of any etiology (CHD - coronary heart disease);
- hereditary factor (familial hyperlipidemia);
- left ventricular hypertrophy;
- age: as we have already said, SRGC is more common in children and adolescents;
- environmental factors, the most likely of which is hypothermia;
- cardiopsychoneurosis;
- electrolyte imbalance.
Definition of extrasystole. Classification of heart rhythm disorders in children
PVCs are divided depending on location into right ventricular (most often in children from the outflow tract) and left ventricular (from the outflow tract, anterior or posterior branch of the left bundle branch).
According to the literature, ventricular extrasystole from the left ventricle often has a benign course, resolving spontaneously with age. PVCs from the right ventricular outflow tract in children are also usually favorable; however, PVCs in this location may be a manifestation of arrhythmogenic right ventricular dysplasia (ARVD) [7,8].
Classifications of the syndrome and theories of its origin
Currently, almost every school of cardiology is studying the phenomenon of left ventricular repolarization, creating its own classifications, studying the causes and prognosis of these disorders.
Why is early ventricular repolarization syndrome detected?
To rule out other conditions, the doctor may order tests to look at the heart muscle, blood flow through the heart, and any potential leaks in the heart valves.
If the abnormal heart rhythm is intermittent, the patient may need to wear a Holter monitor. This portable device allows the medical team to observe the patient's cardiac activity over a longer period of time, and this helps diagnose the condition if an abnormal rhythm occurs while the patient is not in the hospital. Let's consider the main classification options:
- Classification based on the presence or absence of cardiac pathology in people with such changes in the cardiogram.
- Classification based on the number of electrocardiographic signs and leads in which these changes are recorded.
- Classification based on the constancy of electrocardiographic signs in combination with rhythm disturbances and.
- Classification based on the severity of repolarization depending on the number of leads where changes are recorded.
Repolarization on ECG
There are also several theories about the origin of this phenomenon; the following options currently exist:
- The presence of additional pathways for impulse conduction. This leads to the premature appearance of an electrical impulse in.
- Unevenness of repolarization processes in different parts of the left ventricle.
- Increased activity of the sympathetic nervous system.
- Electrolyte disturbances, namely increased levels of potassium and calcium in myocardial cells.
Etiopathogenesis of extrasystole in children
Recently, cardiologists have noted a trend towards an increase in the incidence of early ventricular repolarization syndrome among children.
The phenomenon itself does not cause significant cardiac disorders; children with early repolarization syndrome must undergo a standard blood and urine test, dynamic ECG recording, as well as echocardiography in order to determine the possible cause of the disease and concomitant diseases.
It is mandatory to undergo a preventive ultrasound of the heart and an ECG 2 times. per year and, if necessary, correction of drug treatment by a cardiologist.
It is advisable to prescribe antiarrhythmic drugs only for confirmed cardiac arrhythmias during an ECG study. For preventive purposes, children are recommended to use drugs that contain magnesium.
Extrasystole in children is often asymptomatic, which makes it impossible to accurately determine the time of its occurrence. According to our data, about 70% of cases of arrhythmia are discovered by chance by parents or medical personnel during preventive examinations or in connection with a current or past respiratory infection.
Indeed, the connection between NRS and respiratory infections has been proven, which is due to the possible presence of carditis, autonomic dysfunction with hyperactivity of the trophotropic apparatus in the early period of convalescence, when vagal tone predominates against the background of decreased activity of the sympathoadrenal department.
According to our observations, many patients do not complain and do not know about the existence of ES until the doctor informs them about it. Sometimes the described sensations are accompanied by short-term (1-2 s) acute pain in the area of the apex of the heart.
Manifestations such as dizziness and weakness are observed only with extrasystolic arrhythmia against the background of severe heart damage with hemodynamic disorder.
The issues of treating extrasystole have not been sufficiently developed to date; there is a lot of controversy in them, probably due to different assessments of the degree of organic “interest” of the heart during extrasystole. It is necessary to use all opportunities to make an etiological diagnosis.
The presence of structural changes in the heart, somatic pathology, which could cause arrhythmia, require treatment of the underlying disease.
Children with rare ventricular extrasystoles usually do not require treatment. It is important to dynamically monitor patients at least once a year, and in the presence of clinical symptoms of ES, Holter monitoring is recommended once a year due to evidence of the persistence or transformation of ES into another cardiovascular pathology in subsequent age periods according to the Framingham study.
It is important to explain to the patient that extrasystole is safe, especially when potentially significant arrhythmogenic factors are eliminated: psycho-emotional stress, disruption of the daily routine, bad habits (smoking, alcohol, substance abuse), and taking sympathomimetic drugs.
A healthy lifestyle is of great importance: getting enough sleep, walking in the fresh air, creating a favorable psychological climate in the family and school. Food should contain foods rich in potassium, magnesium (apricots, prunes, baked potatoes, dried fruits), selenium (olive oil, seafood, herring, olives, legumes, nuts, buckwheat and oatmeal, lard) and vitamins.
Extrasystole, especially ventricular, disrupts the correctness of the heart rhythm due to premature ventricular contractions, post-extrasystolic pauses and the associated asynchrony of myocardial excitation.
However, extrasystoles, even frequent ones, as a rule, do not affect or have little effect on hemodynamics if there are no pronounced diffuse or large-focal myocardial lesions. This is associated with the effect of the so-called post-extrasystolic potentiation - an increase in the strength of the contraction following the extrasystole.
In addition to increasing the force of contraction, a compensatory pause (if it is complete) is also important, ensuring an increase in the end-diastolic volume of the ventricles of the heart. In case of organic pathology of the myocardium, the listed compensation mechanisms turn out to be untenable, and ES can cause a decrease in cardiac output and contribute to the development of congestive heart failure.
The prognosis of extrasystole depends on the presence or absence of organic pathology of the heart, the electrophysiological characteristics of extrasystole (frequency, degree of prematurity, localization), as well as on the ability of extrasystole to have a negative effect on blood circulation - the hemodynamic efficiency of extrasystole.
The criteria for a favorable prognosis of the clinical course of ES are: monomorphic ES, disappearing with physical activity, hemodynamically stable (effective), not associated with organic heart pathology.
Features of the course in children and adolescents
The syndrome affects not only adults, but also children. The disease is quite rare, but has a wide age range.
Early repolarization is diagnosed in both infants and older children. Teenagers are also often susceptible to the disease.
External symptoms indicating the syndrome, just like in adults, are absent. Most parents had not even heard of this pathology before the ECG procedure.
If sinus rhythm is maintained, SIRS in children is the age norm and should not be a reason for panic. In healthy children, it goes away without treatment as they grow older.
Sometimes, to eliminate it, it is enough for parents to adjust the child’s lifestyle. It will consist of providing the child with a balanced diet and monitoring compliance with the daily routine. Parents should also reduce the child’s physical and emotional stress and, if possible, reduce the impact of stress factors.
In the case of recently born babies, a complete comprehensive diagnosis of the heart should be carried out to identify possible abnormalities. When it comes to teenagers, the reason for the manifestation of this syndrome often lies in active hormonal changes that pass without consequences as they grow older.
Signs of premature atrial depolarization
- Arrhythmia develops due to increased automatism of the sinus node as a result of the influence of the autonomic nervous system. With sinus tachycardia, the ventricles and atria contract in a coordinated manner, only diastole is shortened.
- Extrasystoles represent a premature contraction of the heart, with the impulse located in various parts of the atrium. The heart rhythm may be normal or rapid.
- Paroxysmal tachycardia is characterized by attacks of increased heart rate, the activation of which is located outside the sinus node.
Types of arrhythmia and reasons for their development
To find out the causes of rhythm disturbances, it is necessary to understand the nature of the normal rhythm of the heart. The latter is provided by a conducting system consisting of a system of successive nodes formed from highly functional cells. These cells provide the ability to create electrical impulses passing along each fiber and bundle of the heart muscle. Such impulses ensure its reduction. The sinus node, located in the upper part of the right atrium, is responsible for the generation of impulses to a greater extent. Heart contraction occurs in several stages:
- Impulses from the sinus node spread to the atria and the atrioventricular node.
- At the atrioventricular node, the impulse slows down, allowing the atria to contract and pump blood into the ventricles.
- Next, the impulse passes through the branches of the His bundle: the right one conducts impulses passing through the Purkinje fibers to the right ventricle, the left one to the left ventricle. As a result, the mechanism of excitation and contraction of the ventricles is triggered.
If all structures of the heart function smoothly, the rhythm will be normal. Rhythm disturbances occur due to pathology of one of the components of the conduction system or due to problems with the conduction of impulses along the muscle fibers of the heart.
There are the following types of arrhythmia:
- Extrasystoles are premature contractions of the heart, the impulse in which does not come from the sinus node.
- Atrial fibrillation, or atrial fibrillation, is a heart rhythm disturbance caused by disordered excitation and contraction of atrial fibers.
- Sinus arrhythmia is caused by an abnormal sinus rhythm, accompanied by alternating deceleration and acceleration.
- Atrial flutter is an increase in the frequency of atrial contractions up to 400 beats per minute, combined with their regular rhythm.
- Supraventricular tachycardia forms within a small area of atrium tissue. Atrial conduction disturbance is observed.
- Ventricular tachycardia is an acceleration of the heart rate coming from the ventricles, due to which they do not have time to fill with blood normally.
- Ventricular fibrillation is a chaotic fluttering of the ventricles, provoked by a flow of impulses from them. This condition makes it impossible for the ventricles to contract and, accordingly, further pumping blood. This is the most dangerous type of rhythm disturbance, as a person falls into a state of clinical death within a few minutes.
- Sinus node dysfunction syndrome is a violation of the formation of an impulse in the sinus node and its transition to the atria. This type of arrhythmia can provoke cardiac arrest.
- The blockade occurs against the background of a slowdown in the conduction of the impulse or its cessation. They can manifest themselves in both the ventricles and atria.
The causes of arrhythmia include:
- Organic organ damage: congenital or acquired defects, myocardial infarction, etc.
- Violation of the water-salt balance caused by intoxication or loss of potassium (magnesium, sodium) by the body.
- Thyroid diseases: due to increased thyroid function, the synthesis of hormones increases. It increases metabolism in the body, which increases heart rate. When the thyroid gland produces insufficient hormones, the rhythm weakens.
- Diabetes mellitus increases the risk of developing cardiac ischemia. With a sharp drop in sugar levels, the rhythm of its contractions is disrupted.
- Hypertension provokes thickening of the wall of the left ventricle, thereby reducing its conductivity.
- Consumption of caffeine, nicotine and narcotic substances.
Symptoms and diagnosis
The diagnosis is made based on the patient’s complaints, examination and research data. The symptoms of the disease are varied and complaints may be absent or have the following signs:
- heartbeat.
- pain, discomfort, feeling of heaviness in the left half of the chest.
- general weakness, dizziness, fear, agitation.
- nausea, vomiting.
- increased sweating.
- sensation of fluttering in the region of the heart.
- after an attack - copious urination due to relaxation of the bladder sphincter.
- pale skin, swelling of the neck veins.
- on examination - tachycardia, blood pressure is reduced or normal, increased breathing.
To clarify the diagnosis, an ECG study is performed, which records changes:
- sinus rhythm, shortening of the interval between cardiac complexes, tachycardia.
- the ventricular complex is not changed, the P wave may be absent, negative, biphasic. An incomplete compensatory pause is observed.
- ST segment depression develops against the background of tachycardia.
Clinical manifestations of pathology can be divided into two groups.
First group
The first group includes those patients in whom this syndrome leads to complications - fainting and cardiac arrest. Fainting is a short-term loss of consciousness and muscle tone, which is characterized by a sudden onset and spontaneous recovery.
It develops due to deterioration of blood supply to the brain. In case of SRGC, the most common cause of fainting is a violation of the rhythm of contractions of the ventricles of the heart.
Cardiac arrest is the sudden cessation of blood circulation due to ineffective or absent heartbeats. In SRGC, cardiac arrest is caused by ventricular fibrillation.
Ventricular fibrillation is the most dangerous heart rhythm disorder, which is characterized by rapid, irregular and uncoordinated contractions of ventricular cardiomyocytes. Within a few seconds of the onset of ventricular fibrillation, the patient usually loses consciousness, then his pulse and breathing disappear.
Without the necessary assistance, a person most often dies.
Second group
Many large-scale experimental studies have been conducted to determine specific clinical symptoms characteristic exclusively of early repolarization syndrome, but they have not been successful. Changes in ECG indicators are recorded under equal conditions not only in patients with cardiac pathologies, but also among healthy young people.
Symptoms of premature atrial depolarization
The main symptoms of premature atrial depolarization are the following conditions:
- a feeling of intense shocks occurring in the heart (this condition may be a consequence of contractions of the ventricle after a pause);
- moderate hemodynamic disturbances, for example, heartbeat more active than usual;
- dyspnea;
- weakness;
- dizziness.
Often there are no symptoms at all, and PPD is diagnosed after deciphering the ECG or by palpating the pulse and detecting the so-called “loss” of one beat.
Symptoms of premature ventricular depolarization
Sometimes there are no symptoms at all. In a number of other cases, the following symptoms may be present:
- temporary increase in the force of heart contraction;
- feeling of strong tremors;
- fainting, nausea;
- feeling of heart fluttering;
- chest pain;
- sweating;
- labored breathing;
- pulse more than 100 beats per minute at rest.
Can it be avoided?
Considering that this syndrome is concomitant in many cardiac patients, its occurrence can be avoided using the same methods as all other diseases of the cardiovascular system.
Despite the insufficient study of this pathology, we can say with confidence that early stimulation of the cell membrane over a long period of time will definitely not lead to anything good, so prevention of this condition is necessary.
Prevention of cardiovascular diseases is based on a healthy lifestyle (this means not only giving up smoking and alcohol abuse, but also combating excess weight and physical inactivity). Heart diseases often occur after prolonged psycho-emotional stress, so you need to avoid any situations that can lead to stress.
To prevent atherosclerotic vascular damage and arterial hypertension, it is necessary to limit the consumption of animal fats and table salt, and eat sea fish more often. Quit smoking completely, eat more plant foods, especially those rich in fats.
To summarize, we can say that early ventricular repolarization syndrome is a condition that has not yet been sufficiently studied. Detection of corresponding changes in the electrocardiogram indicates the need to change lifestyle to prevent the occurrence of cardiovascular diseases. The frequency of examinations and consultations should be clarified with a cardiologist.
Sergey, 28 years old. He has been playing volleyball for about 10 years, training twice every day for two hours. He undergoes an annual medical examination; no previous diseases have been identified. During the last medical examination, the ECG revealed early left ventricular repolarization syndrome. A young man, concerned about his health, came to see a cardiologist without any complaints about his health.
The cardiologist advised me to reconsider my diet and reduce the effectiveness of my workouts for a while. A month later, Sergei came for a follow-up appointment; there were no changes in his state of health or on the ECG. Now the athlete needs to undergo an ECG twice a year and be examined by a cardiologist at the same frequency.
Brief information: Early left ventricular repolarization syndrome in athletes is a very common phenomenon; according to some authors, about 50% of athletes in professional sports have such changes.
Cases of cardiac arrest with such changes and the occurrence of arrhythmias have been described. Therefore, athletes need especially careful monitoring of their heart condition.
Do you still think that it is impossible to get rid of HEART DISEASES!?
- Do you often experience discomfort in the heart area (pain, tingling, squeezing)?
- You may suddenly feel weak and tired...
- I constantly feel high blood pressure...
- There is nothing to say about shortness of breath after the slightest physical exertion...
- And you have been taking a bunch of medications for a long time, going on a diet and watching your weight...
But judging by the fact that you are reading these lines, victory is not on your side. That is why we recommend reading the story of Olga Markovich, who found an effective remedy for cardiovascular diseases.
What should you do to persuade yourself to see a doctor? The question is not as idle as it might seem. What factors should force a person who is always in a hurry to throw away important things, change his meeting schedule, refuse to watch a football match or go shopping with friends nearby? The reasons can be very different. Unbearable pain, concern about the health of children, or any other threatening symptoms (note for clarity, often far-fetched) that can force us to abandon our usual way of life. In this case, we are ready not only to spend several hours visiting a doctor, but also to begin treatment.
But what to do if a person is faced with something incomprehensible? There are no signs of the disease, the symptoms seem insignificant, and we are familiar with heart pathologies only from the stories of my grandmother. You say this doesn’t happen? It turns out that not everything is so simple. Early ventricular repolarization syndrome is a rather interesting phenomenon. It can only be noticed on an ECG, and all treatment consists of an unobtrusive recommendation from a cardiologist to quit smoking. But any heart disease, no matter how harmless it may seem, can always turn into big problems. Therefore, we decided that early repolarization syndrome deserves a separate detailed discussion.
Diagnostics
The symptoms of the condition are varied and occur both asymptomatically and with complaints of a feeling of cardiac arrest, pulsation, palpitations, and weakness. Other signs may be a manifestation of the underlying disease that led to the arrhythmia.
When analyzing your medical history, you should take into account the presence of structural heart damage, bad habits, and medication use. During the examination, pulsation of the neck veins and a decrease in the sonority of heart sounds are observed.
The ECG reveals not only extrasystole and tachycardia, but also heart disease, which causes premature depolarization of the ventricles. A deformed and wide ventricular complex and a compensatory pause are recorded. The atrial complex does not depend on the ventricular complex; extrasystoles can be single and polytopic, mono- and polymorphic.
In our medical center, to clarify the diagnosis, in addition to an ECG study, a specialist can prescribe other types of diagnostic measures:
- Holter monitoring ECG.
- Ultrasound of the heart.
- electrophysiological study.
Since the disease may not manifest itself, it is recommended that everyone undergo a preventive examination with a mandatory ECG.
- Electrocardiography is recommended [2, 9].
(Strength of recommendation – 1; Strength of evidence – A)
- Consultation with a geneticist is recommended [11,12].
(Strength of recommendation – 2; Strength of evidence – C)
Symptoms
Each type of rhythm disorder is characterized by certain symptoms. During extrasystoles, a person practically does not feel any discomfort. Sometimes a strong shock may be felt coming from the heart.
With atrial fibrillation, symptoms such as chest pain, shortness of breath, weakness, darkening of the eyes and characteristic bubbling in the heart area are observed. Atrial fibrillation can manifest itself in the form of attacks that last several minutes, hours, days, or be constant.
Symptoms of sinus arrhythmia are as follows: increased (slow) pulse, extremely rarely, pain in the left side of the chest, fainting, darkening of the eyes, shortness of breath.
With atrial flutter, blood pressure rapidly drops, the heart rate increases, and dizziness and weakness are felt. There is also an increase in pulse in the neck veins.
As for supraventricular tachycardia, some people who have a similar heart rhythm disorder do not feel any symptoms at all. However, most often such arrhythmia is manifested by increased heart rate, shallow breathing, profuse sweating, pressure in the left side of the chest, throat spasm, frequent urination and dizziness.
With unstable ventricular tachycardia, symptoms such as palpitations, dizziness, and fainting are observed. With persistent arrhythmia of this type, there is a weakening of the pulse in the neck veins, impaired consciousness, and an increase in heart rate up to 200 beats per minute.
Treatment
In the absence of heart disease and symptoms, treatment is usually not required. It is recommended to give up bad habits that cause arrhythmia, correct electrolyte imbalances, and replace medications. If extrasystole is poorly tolerated, sedative therapy and correction of imbalances in the functioning of the autonomic nervous system will be useful.
Children with PVCs usually do not require emergency treatment.
The decision to initiate therapy for the treatment of frequent PVCs in children depends on age, the presence of symptoms of the disease, the presence of concomitant cardiac pathology, and the hemodynamic influences of PVCs.
Given the benign course of idiopathic PVCs, in most cases no treatment is required [2,9].
The decision to prescribe therapy, select a drug, or determine the indications for RFA of the PVC substrate should be strictly individual, with an assessment and comparison of the benefits of therapy and the risks of possible complications.
Choice of treatment tactics for children with PVCs
- It is recommended to conduct a comprehensive examination of asymptomatic patients with frequent PVCs or accelerated idioventricular rhythm, who have normal myocardial contractility. Drug therapy and RFA are not recommended [9].
(Strength of recommendation – 1; certainty of evidence – C)
- For children with frequent PVCs, which caused the development of arrhythmogenic myocardial dysfunction, AAT or RFA is recommended [9].
- It is recommended to prescribe β-blockers in asymptomatic patients with frequent or polymorphic PVCs, and if they are ineffective, the use of calcium channel blockers may be justified [2,9].
- In the group of children with rare PVCs and their good tolerance, only a comprehensive examination is recommended.
- It is recommended to consider antiarrhythmic therapy with b-blockers or RFA of the arrhythmia substrate if the patient has symptoms of the disease that correlate with frequent ventricular ectopy or accelerated idioventricular rhythm [9,13].
- If a child has frequent or polymorphic PVCs, in case of ineffectiveness of b-blockers or calcium channel blockers, the use of class I or III antiarrhythmic drugs is recommended.
- Conservative (drug) therapy is based on the correction of the main pathophysiological mechanisms of the development of PVCs and includes the correction of metabolic disorders, effects on the neurovegetative basis of arrhythmia and the specific electrophysiological mechanism of arrhythmia.
- The goal of drug therapy for PVCs is to prevent the development of arrhythmogenic myocardial dysfunction and restore sinus rhythm.
- The selection of antiarrhythmic drugs is carried out strictly under the control of ECG and Holter monitoring, taking into account saturation doses and the circadian nature of the arrhythmia. It is advisable to calculate the maximum therapeutic effect of the drug taking into account what periods of the day the PVC is most pronounced. The exception is long-acting drugs and Amiodarone. The maintenance dose of the antiarrhythmic drug is determined individually. If the duration of the QT interval increases by more than 25% of the original, class III drugs are discontinued.
For the treatment of many forms of ventricular arrhythmias, β-blockers are the first-line drugs. Considering that these are the safest antiarrhythmic drugs, it is reasonable to start treatment with them, and if they are ineffective, it is necessary to sequentially select drugs from other classes.
Calcium channel blockers are effective drugs for the treatment of ventricular arrhythmias, although they are generally not recommended in children younger than 12 months due to the risk of severe hemodynamic complications [2,9,14,15,16].
- Conservative, antiarrhythmic therapy is recommended as a treatment method in patients with frequent or polymorphic extrasystole, including when extrasystole caused the development of myocardial dysfunction [2, 9].
(Strength of recommendation – 1; Strength of evidence – B)
The surgical method of treating ventricular extrasystole includes radiofrequency catheter ablation of the focus of ventricular ectopy.
Radiofrequency ablation of the PVC lesion
- RFA of the PVC focus is recommended if the patient has arrhythmogenic myocardial dysfunction caused by PVCs [9, 13].
Severe physical activity is contraindicated for all persons suffering from early repolarization syndrome. Correction of eating behavior involves the inclusion in the diet of foods containing potassium, magnesium and B vitamins (greens, raw vegetables and fruits, sea fish, soy and nuts).
In most cases, early ventricular repolarization syndrome does not require drug correction, but if the patient has reliable signs of concomitant cardiac pathology (coronary syndrome, various forms of arrhythmia), then specific drug therapy is recommended.
Numerous randomized studies have proven the effectiveness of energotropic therapy drugs in relieving signs of early repolarization syndrome in both children and adults. Of course, drugs in this group are not the drugs of choice for this pathology, but their use improves the trophism of the heart muscle and prevents possible complications from the heart.
Among the energy-tropic drugs, the most effective in this situation are: Kudesan in a daily dose of 2 mg per 1 kg of weight, Carnitine 500 mg 2 times. per day, vitamin B complex, Neurovitan 1 tablet per day.
Among antiarrhythmic drugs, it is advisable to prescribe a group of drugs that slow down the repolarization process - Novocainamide at a dose of 0.25 mg every 6 hours, Quinidine sulfate 200 mg 3 times a day, Ethmozin 100 mg 3 times a day.
Treatment methods for premature atrial depolarization
If there are any noticeable changes in heart rhythm accompanied by the symptoms described above, you should consult a doctor. Premature atrial depolarization often does not require treatment, but medications such as beta blockers or antiarrhythmic drugs are prescribed if there is discomfort or feeling unwell.
These drugs usually suppress premature contractions and help normalize the electrical activity of the heart.
Treatment methods for premature ventricular depolarization
Premature ventricular depolarization requires a little more attention from both the patient and the doctor. If PJD is accompanied by symptoms such as fainting and attacks of nausea, if the patient feels pain in the heart, catheter ablation or installation of a pacemaker is necessary.
This treatment method, such as a pacemaker, is used when it comes to an irreparable abnormality in the electrical activity of the heart.
In the absence of heart disease or other cardiac dysfunction, premature ventricular depolarization does not need to be treated. Auxiliary treatment methods are:
- oxygen therapy;
- restoration of electrolyte balance;
- prevention of ischemia or heart attack.
There are several factors that need to be considered before starting treatment. These include:
- hypoxia;
- toxic drugs;
- correct electrolyte balance.
Early diagnosis and proper treatment of coronary heart disease are mandatory for successful restoration of the electrical activity of the heart.
Medicines used to treat premature ventricular depolarization are:
- propafenone, amiodarone;
- beta-blockers: bisoprolol, atenolol, metoprolol and others;
- omega-3 fatty acids, verapamil, diltiazem, panangin, diphenylhydantoin.
Prevention
In order to prevent disturbances in the electrical activity of the heart, physical activity, control of body weight, and blood sugar levels are recommended.
The following products are recommended:
- nuts, natural oils;
- foods rich in fiber and vitamins;
- fatty fish;
- dairy products.
Treatment methods
The treatment tactics for patients depend on the opinion of the cardiologist. If the patient does not have cardiac abnormalities and, against the background of a detected repolarization failure, he maintains a normal sinus rhythm, then no special treatment is performed.
Antiarrhythmic drugs may be prescribed as prophylaxis.
To prevent complications due to early depolarization syndrome, patients should follow the following recommendations:
- Avoid drinks containing alcohol, cigarettes, and drugs.
- Optimize and balance physical activity.
- Control your emotional state.
- Eat foods that contain elements essential for the coordinated functioning of the heart and blood vessels. High levels of phosphorus, potassium and magnesium are present in seasonal vegetables, fruits, red fish, nuts and dried fruits.
If the patient has other cardiovascular pathologies, treatment of the disease will be medicinal.
The table below provides examples of the main groups of drugs prescribed for SRGC and their names:
Prevention and follow-up
5.1 Prevention
In patients with cardiac pathology such as congenital heart disease, including after surgical correction of congenital heart disease, cardiomyopathies, taking into account the potential for the development of ventricular tachycardia, regular dynamic monitoring is necessary (with mandatory ECG, Holter monitoring and, if indicated, a stress test).
5.2 Management of patients with ventricular extrasystole
All patients with ventricular extrasystole require observation by a pediatric cardiologist.
For children with rare PVCs, in the absence of evidence of organic heart disease, dynamic monitoring is carried out once a year and includes an ECG and 24-hour ECG monitoring.
Primary hospitalization in a specialized cardiology department is associated with diagnosing the cause of newly detected frequent ventricular extrasystole and carrying out etiotropic treatment. The duration of hospitalization is determined by the underlying disease.
In the presence of frequent PVCs in patients with the presence/absence of cardiac pathology, outpatient monitoring includes an ECG, 24-hour ECG monitoring and ultrasound examination of the heart at least once every 6 months.
If PVCs progress during follow-up and/or symptoms associated with the presence of frequent PVCs (fatigue, dizziness, fainting) appear, an unscheduled examination is performed in a hospital setting.
Hospitalization is carried out in a specialized cardiology department of a city/regional/republican children's hospital. Purpose of hospitalization: to determine the presence of indications for prescribing antiarrhythmic therapy and treatment of chronic heart failure, in the event of the formation of arrhythmogenic myocardial dysfunction, to determine the presence of indications for endoEPI and radiofrequency catheter ablation of the arrhythmogenic focus.
The duration of hospitalization is determined by the severity of the patient's condition, but should not exceed 14 days.
Prescribing a new drug with class I-IV antiarrhythmic effects is possible after assessing the 24-hour heart rate profile after eliminating the previous one due to the risk of worsening the proarrhythmic effect.
With long-term administration of Amiodarone, it is recommended to evaluate the size, structure (ultrasound) and hormonal function of the thyroid gland once every 6 months.
In case of persistent drug remission of PVCs, a planned discontinuation of therapy is carried out and in the absence of extrasystole (not earlier than a year after complete discontinuation of therapy), before removal from the dispensary register, a control examination is carried out (with the obligatory ECG, ECHO-CG, stress test, Holter monitoring ).
In the absence of ventricular ectopic activity, removal from the dispensary register with recommendations for an ECG after intercurrent illnesses and during prescribed age periods.